Nodal Metastases in Acinic Cell Carcinoma of the Parotid Gland

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Pathology
2.2. Statistical Methods
3. Results
3.1. Patients’ Clinical Data
3.2. Recurrence and Survival
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Seifert, G.; Sobin, L.H. Histological typing of salivary gland tumours. In World Health Organization International Histological Classification of Tumours, 2nd ed.; Springer: New York, NY, USA, 1991. [Google Scholar]
- Hoffman, H.T.; Karnell, L.H.; Robinson, R.A.; Pinkston, J.A.; Menck, H.R. National Cancer Data Base report on cancer of the head and neck: Acinic cell carcinoma. Head Neck 1999, 21, 297–309. [Google Scholar] [CrossRef]
- Vander Poorten, V.; Bradley, P.J.; Takes, R.P.; Rinaldo, A.; Woolgar, J.A.; Ferlito, A. Diagnosis and management of parotid carcinoma with a special focus on recent advances in molecular biology. Head Neck 2012, 34, 429–440. [Google Scholar] [CrossRef] [PubMed]
- Spiro, R.H. Salivary neoplasms: Overview of a 35-year experience with 2807 patients. Head Neck 1986, 8, 177–184. [Google Scholar] [CrossRef]
- Erovic, B.M.; Schopper, C.; Pammer, J.; Vormittag, L.; Maleki, A.; Brunner, M.; Heiduschka, G.; Grasl, M.C.; Thurnher, D. Multimodal treatment of patients with minor salivary gland cancer in the case of recurrent disease. Head Neck 2010, 32, 1167–1172. [Google Scholar] [CrossRef] [PubMed]
- Haymerle, G.; Schneider, S.; Harris, L.; Häupl, T.; Schopper, C.; Pammer, J.; Grasl, M.C.; Erovic, B.M. Minor salivary gland carcinoma: A review of 35 cases. Eur. Arch. Otorhinolaryngol. 2016, 273, 2717–2726. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.; Kloimstein, P.; Pammer, J.; Brannath, W.; Grasl, M.C.; Erovic, B.M. New diagnostic markers in salivary gland tumors. Eur. Arch. Otorhinolaryngol. 2014, 271, 1999–2007. [Google Scholar] [CrossRef] [PubMed]
- Xiao, C.C.; Zhan, K.Y.; White-Gilbertson, S.J.; Day, T.A. Predictors of nodal metastasis in parotid malignancies: A National Cancer Data Base Study of 22,653 Patients. Otolaryngol. Head Neck Surg. 2016, 154, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Scherl, C.; Kato, M.G.; Erkul, E.; Graboyes, E.M.; Nguyen, S.A.; Chi, A.C.; Morgan, P.F.; Day, T.A. Outcomes and prognostic factors for parotid acinic cell Carcinoma: A National Cancer Database study of 2362 cases. Oral. Oncol. 2018, 82, 53–60. [Google Scholar] [CrossRef]
- Ellis, G.L.; Corio, R.L. Acinic cell adenocarcinoma. A clinicopathologic analysis of 294 cases. Cancer 1983, 52, 542–549. [Google Scholar] [CrossRef]
- Erovic, B.M.; Shah, M.D.; Bruch, G.; Johnston, M.; Kim, J.; O’Sullivan, B.; Perez-Ordonez, B.; Weinreb, I.; Atenafu, E.G.; de Almeida, J.; et al. Outcome analysis of 215 patients with parotid gland tumors: A retrospective cohort analysis. J. Otolaryngol. Head Neck Surg. 2015, 44, 43. [Google Scholar] [CrossRef]
- Armstrong, J.G.; Harrison, L.B.; Thaler, H.T.; Friedlander-Klar, H.; Fass, D.E.; Zelefsky, M.J.; Shah, J.P.; Strong, E.W.; Spiro, R.H. The indications for elective treatment of the neck in cancer of the major salivary glands. Cancer 1992, 69, 615–619. [Google Scholar] [CrossRef]
- Kawata, R.; Koutetsu, L.; Yoshimura, K.; Nishikawa, S.; Takenaka, H. Indication for elective neck dissection for N0 carcinoma of the parotid gland: A single institution’s 20-year experience. Acta Otolaryngol. 2010, 130, 286–292. [Google Scholar] [CrossRef]
- Eneroth, C.M.; Hamberger, C.A. Principles of treatment of different types of parotid tumors. Laryngoscope 1974, 84, 1732–1740. [Google Scholar] [CrossRef]
- Ali, S.; Palmer, F.L.; DiLorenzo, M.; Shah, J.P.; Patel, S.G.; Ganly, I. Treatment of the neck in carcinoma of the parotid gland. Ann. Surg. Oncol. 2014, 21, 3042–3048. [Google Scholar] [CrossRef]
- Stenner, M.; Molls, C.; Luers, J.C.; Beutner, D.; Klussmann, J.P.; Huettenbrink, K.B. Occurrence of lymph node metastasis in early-stage parotid gland cancer. Eur. Arch. Otorhinolaryngol. 2012, 269, 643–648. [Google Scholar] [CrossRef]
- Medina, J.E. Neck dissection in the treatment of cancer of major salivary glands. Otolaryngol. Clin. N. Am. 1998, 31, 815–822. [Google Scholar] [CrossRef]
- Zbaren, P.; Schupbach, J.; Nuyens, M.; Stauffer, E. Elective neck dissection versus observation in primary parotid carcinoma. Otolaryngol. Head Neck Surg. 2005, 132, 387–391. [Google Scholar] [CrossRef]
- Colevas, A.D.; Yom, S.S.; Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Brizel, D.M.; Burtness, B.; Busse, P.M.; Caudell, J.J.; et al. NCCN Guidelines Insights: Head and Neck Cancers, Version 1.2018. J. Natl. Compr. Cancer Netw. 2018, 16, 479–490. [Google Scholar] [CrossRef]
- Mc Guirt, W.F. Management of occult metastatic disease from salivary gland neoplasms. Arch. Otolaryngol. Head Neck Surg. 1989, 115, 322–325. [Google Scholar] [CrossRef]
- Kelley, D.; Spiro, R. Management of the neck in parotid carcinoma. Am. J. Surg. 1996, 172, 695–697. [Google Scholar] [CrossRef]
- Gomez, D.R.; Katabi, N.; Zhung, J.; Wolden, S.L.; Zelefsky, M.J.; Kraus, D.H.; Shah, J.P.; Wong, R.J.; Ghossein, R.A.; Lee, N.Y. Clinical and pathologic prognostic features in acinic cell carcinoma of the parotid gland. Cancer 2009, 115, 2128–2137. [Google Scholar] [CrossRef]
- Eneroth, C.M.; Jakobsson, P.A.; Blanck, C. Acinic cell carcinoma of the parotid gland. Cancer 1966, 19, 1761–1772. [Google Scholar] [CrossRef]
- Spiro, R.H.; Huvos, A.G.; Strong, E.W. Acinic cell carcinoma of salivary origin. A clinicopathologic study of 67 cases. Cancer 1978, 41, 924–935. [Google Scholar] [CrossRef]
- Lin, W.N.; Huang, H.C.; Wu, C.C.; Liao, C.T.; Chen, I.H.; Kan, C.J.; Huang, S.F. Analysis of acinic cell carcinoma of the parotid gland—15 years experience. Acta Otolaryngol. 2010, 130, 1406–1410. [Google Scholar] [CrossRef]
- Amit, M.; Na’ara, S.; Trejo-Leider, L.; Ramer, N.; Burstein, D.; Yue, M.; Miles, B.; Yang, X.; Lei, D.; Bjoerndal, K.; et al. Defining the surgical margins of adenoid cystic carcinoma and their impact on outcome: An international collaborative study. Head Neck 2017, 39, 1008–1014. [Google Scholar] [CrossRef]



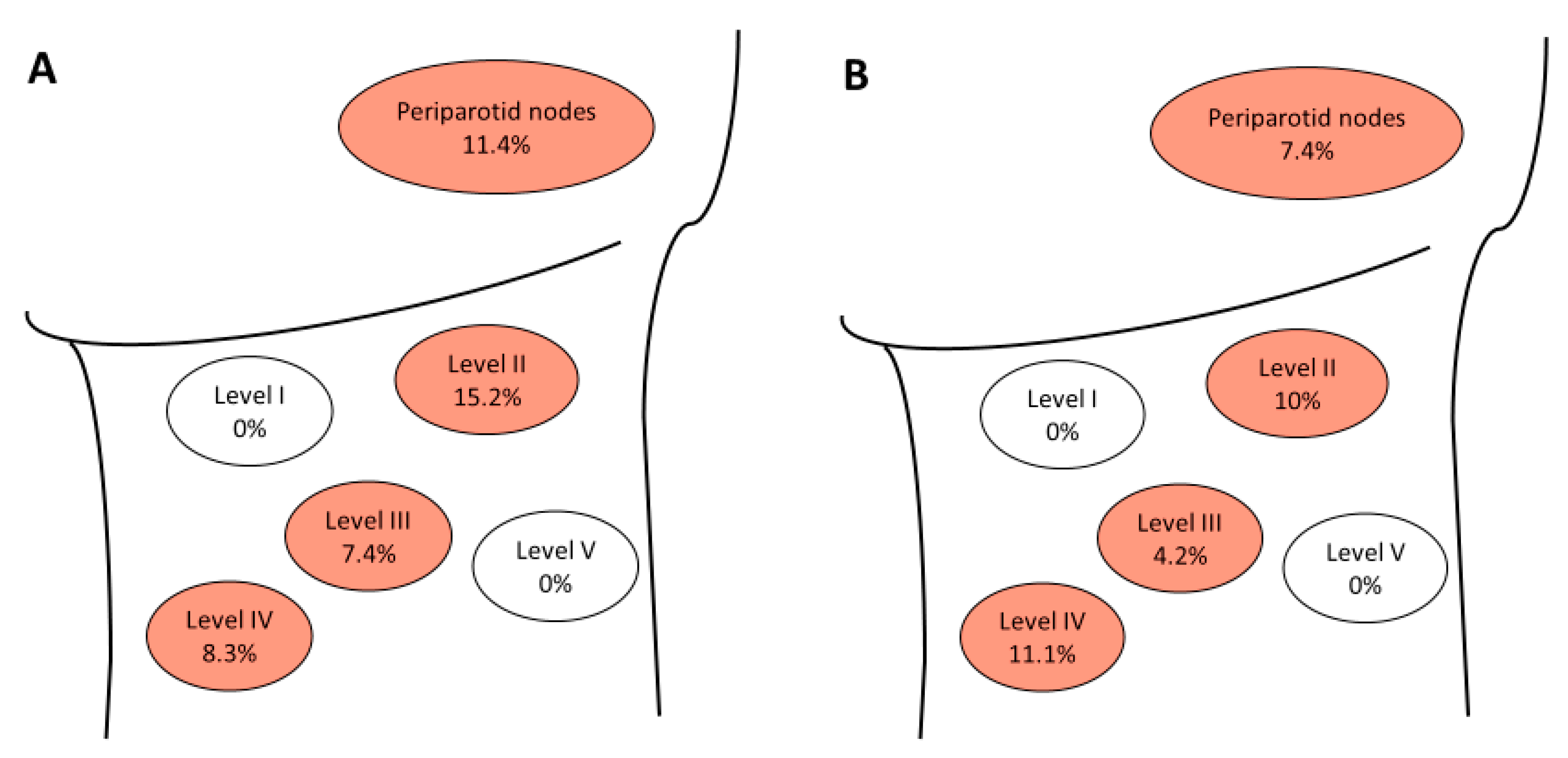{kind=link}
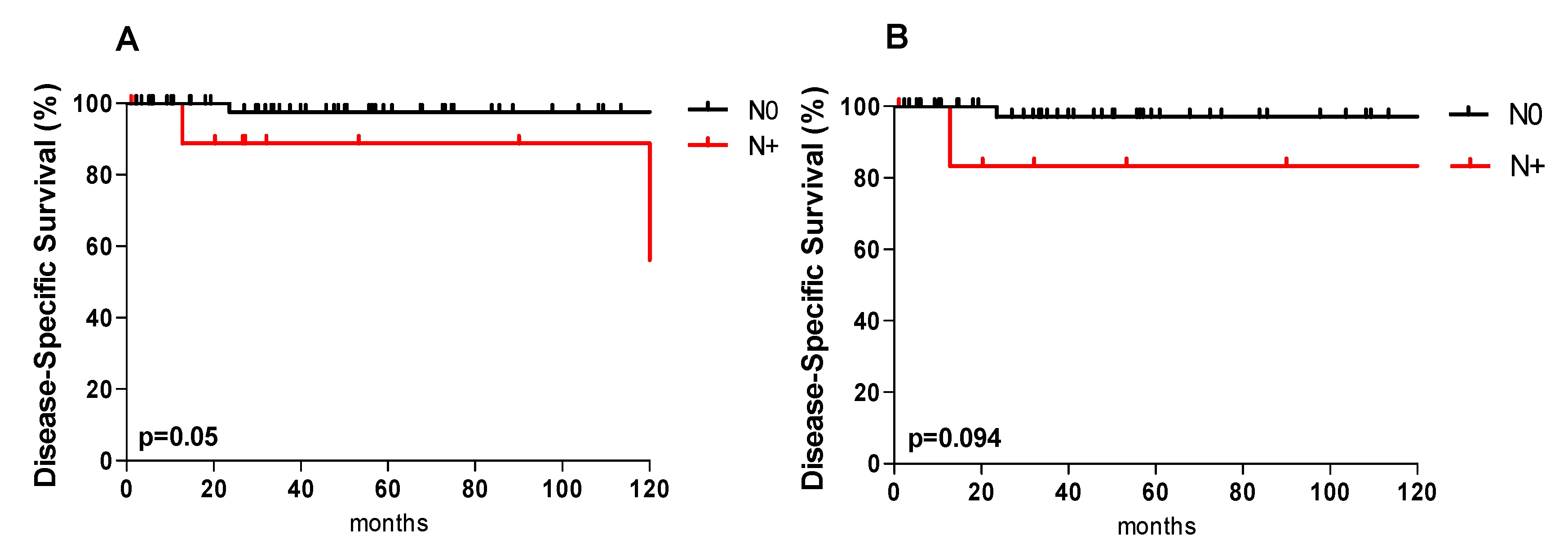{kind=link}
| Clinical Variables | Nr. | |
|---|---|---|
| Age, years (mean ± SD) | 49.4 ± 17.1 | |
| Sex | ||
| Male | 32 (48.5%) | |
| Female | 34 (51.5%) | |
| pT classification | ||
| T1 | 30 (45.5%) | |
| T2 | 25 (37.9%) | |
| T3 | 9 (13.6%) | |
| T4 | 2 (3%) | |
| N classification | ||
| N0 | 54 (81.8%) | |
| N+ | 12 (18.2%) | |
| Staging | ||
| I | 27(40.9%) | |
| II | 19 (28.8%) | |
| III | 12 (18.2%) | |
| IV | 4 (6.1%) | |
| n.a. | 4 (6%) | |
| Tumor Grading | ||
| Low-grade (G1) | 53 (80.3%) | |
| Intermediate-grade (G2) | 3 (4.5%) | |
| High-grade (G3) | 6 (9.1%) | |
| n.a. | 4 (6.1%) | |
| Perineural Invasion | ||
| negative (PNI 0) | 53 (80.3%) | |
| positive (PNI 1) | 4 (6.1%) | |
| n.a. | 9 (13.6%) | |
| Lymphovascular Invasion | ||
| negative (LVI 0) | 51 (77.3%) | |
| positive (LVI 1) | 7 (10.6%) | |
| n.a. | 8 (12.1%) | |
| Extraparotid Extension | ||
| negative | 54 (81.8%) | |
| positive | 4 (6.1%) | |
| n.a. | 8 (12.1%) | |
| Periparotid lymph node involvement | ||
| negative | 45 (68.2%) | |
| positive | 5 (7.6%) | |
| n.a. | 16 (24.2%) | |
| Variables | Total | N Classification | ||||
|---|---|---|---|---|---|---|
| N+ | Occult N | N0 | pa | |||
| pT classification | ||||||
| pT1–pT2 | 55 | 8 (14.5%) | 4 (7.3%) | 47 (85.5%) | ||
| pT3–pT4 | 11 | 4 (36.4%) | 2 (18.2%) | 7 (63.6%) | 0.087 | |
| Tumor Grading | ||||||
| G1 | 53 | 9 (17%) | 4 (7.3%) | 44 (83%) | ||
| G2-G3 | 9 | 2 (22.2%) | 1 (11.1%) | 7 (77.8%) | ||
| n.a. | 4 | 1 (25%) | 1 (25%) | 3 (75%) | 0.871 | |
| PNI | ||||||
| negative | 53 | 8 (15.1%) | 3 (5.7%) | 45 (84.9%) | ||
| positive | 4 | 1 (25%) | 1 (25%) | 3 (75%) | ||
| n.a. | 9 | 3 (33.3%) | 2 (22.2%) | 6 (66.7%) | 0.396 | |
| LVI | ||||||
| negative | 51 | 8 (15.7%) | 3 (5.9%) | 43 (84.3%) | ||
| positive | 7 | 1 (14.3%) | 1 (14.3%) | 6 (85.7%) | ||
| n.a. | 8 | 3 (37.5%) | 2 (25%) | 5 (62.5%) | 0.318 | |
| Extraparotid extension | ||||||
| negative | 54 | 8 (14.8%) | 3 (5.6%) | 47(85.2%) | ||
| positive | 4 | 2 (50%) | 1 (25%) | 2 (50%) | ||
| n.a. | 8 | 2 (25%) | 2 (25%) | 6 (75%) | 0.184 | |
| Variables | Recurrence | pa | ||
|---|---|---|---|---|
| YES | NO | |||
| Nr. (%) | Nr. (%) | |||
| pT classification | ||||
| pT1–pT2 | 5 (71.4%) | 50 (84.7%) | ||
| pT3–pT4 | 2 (28.6%) | 9 (15.3%) | 0.371 | |
| Occult metastasis | ||||
| yes | 0 | 6 (10.2%) | ||
| no | 7 (100%) | 53 (89.8%) | 0.376 | |
| N classification | ||||
| N0 | 1 (14.3%) | 24 (40.7%) | ||
| pN+ | 2 (28.6%) | 10 (16.9%) | ||
| no ND | 4 (57.1%) | 25 (42.4%) | 0.382 | |
| Neck dissection | ||||
| yes | 3 (42.9%) | 32 (54.2%) | ||
| no | 4 (57.1%) | 27 (45.8%) | 0.568 | |
| Grading | ||||
| G1 | 3 (42.9%) | 50 (84.7%) | ||
| G2–G3 | 4 (57.1%) | 5 (8.5%) | ||
| n.a. | 0 | 4 (6.8%) | 0.002 | |
| Margin status | ||||
| negative (R0) | 3 (42.9%) | 44 (74.6%) | ||
| positive (R1) | 4 (57.1%) | 12 (20.3%) | ||
| n.a. | 0 | 3 (5.1%) | 0.094 | |
| PNI | ||||
| negative | 3 (42.9%) | 50 (84.7%) | ||
| positive | 2 (28.6%) | 2 (3.4%) | ||
| n.a. | 2 (28.6%) | 7 (11.9%) | 0.010 | |
| LVI | ||||
| negative | 3 (42.9%) | 48 (81.4%) | ||
| positive | 2 (28.6%) | 5 (8.5%) | ||
| n.a. | 2 (28.6%) | 6 (10.1%) | 0.070 | |
| Extraparotid extension | ||||
| negative | 6 (85.7%) | 48 (81.4%) | ||
| positive | 1 (14.3%) | 3 (5.1%) | ||
| n.a. | 0 | 8 (13.6%) | 0.399 | |
| Periparotid lymph node involvement | ||||
| negative | 5 (71.4%) | 40 (67.8%) | ||
| positive | 1 (14.3%) | 4 (6.8%) | ||
| n.a. | 1 (14.3%) | 15 (25.4%) | 0.671 | |
| PORT | ||||
| yes | 6 (85.7%) | 32 (54.2%) | ||
| no | 1 (14.3%) | 27 (45.8%) | 0.111 | |
| Variables | Overall Survival | Disease-Specific Survival | Disease-Free Survival | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 y | 5 y | pa | 1 y | 5 y | pa | 1 y | 5 y | pa | ||
| pT classification | ||||||||||
| pT1–pT2 | 98.2 | 91.3 | 100 | 95.3 | 91.9 | 91.7 | ||||
| pT3–pT4 | 100 | 100 | 0.126 | 100 | 100 | 0.505 | 100 | 75.0 | 0.329 | |
| N classification | ||||||||||
| N0 | 100 | 95.4 | 100 | 97.6 | 93.8 | 91.3 | ||||
| N+ | 91.7 | 81.5 | 0.109 | 100 | 88.9 | 0.050 | 90 | 67.5 | 0.182 | |
| Margin status | ||||||||||
| negative (R0) | 97.9 | 93.0 | 100 | 97.6 | 95.5 | 92.6 | ||||
| positive (R1) | 100 | 90.9 | 0.244 | 100 | 90.9 | 0.406 | 85.1 | 70.9 | 0.210 | |
| Grading | ||||||||||
| G1 | 98.1 | 95.9 | 100 | 100 | 95.7 | 93 | ||||
| G2–G3 | 100 | 68.6 | 0.148 | 100 | 68.6 | 0.007 | 72.9 | 48.6 | 0.002 | |
| PNI | ||||||||||
| no | 98.1 | 95.9 | 100 | 100 | 95.9 | 93.3 | ||||
| yes | 100 | 66.7 | 0.063 | 100 | 66.7 | 0.001 | 66.7 | 0 | 0.001 | |
| LVI | ||||||||||
| no | 100 | 97.7 | 100 | 100 | 97.9 | 92.3 | ||||
| yes | 85.7 | 64.3 | 0.004 | 100 | 75.0 | 0.002 | 75.0 | 50.0 | 0.002 | |
| PORT | ||||||||||
| no | 96.4 | 91.6 | 100 | 100 | 100 | 100 | ||||
| yes | 100 | 93.7 | 0.832 | 100 | 93.7 | 0.180 | 88.4 | 81.0 | 0.038 | |
| END | ||||||||||
| no | 100 | 91.5 | 100 | 95.5 | 92.3 | 87.2 | ||||
| yes | 96.6 | 96.6 | 0.795 | 100 | 100 | 0.307 | 96.2 | 96.2 | 0.312 | |
| Variables | Grading | pa,b | ||
|---|---|---|---|---|
| G1 | G2–G3 | |||
| Nr. (%) | Nr. (%) | |||
| pT classification | ||||
| pT1–pT2 | 45 (84.9%) | 6 (66.7%) | ||
| pT3–pT4 | 8 (15.1%) | 3 (33.3%) | 0.185 a | |
| N classification | ||||
| N0 | 23 (43.4%) | 1 (11.1%) | ||
| pN+ | 9 (17%) | 2 (22.2%) | ||
| no ND | 21 (39.6%) | 6 (66.7%) | 0.175 a | |
| Neck dissection | ||||
| yes | 31 (58.5%) | 3 (33.3%) | ||
| no | 22 (41.5%) | 6 (66.7%) | 0.161 a | |
| Margin status | ||||
| negative (R0) | 40 (75.5%) | 3 (33.3%) | ||
| positive (R1) | 11 (20.8%) | 5 (55.6%) | ||
| n.a. | 2 (3.7%) | 1 (11.1%) | 0.040 a | |
| PORT | ||||
| yes | 28 (52.8%) | 8 (88.9%) | ||
| no | 25 (47.2%) | 1 (11.1%) | 0.043 a | |
| Overall Survival | ||||
| 1 year | 98.1 | 100 | ||
| 5 year | 95.9 | 68.6 | 0.148 b | |
| Disease-specific survival | ||||
| 1 year | 100 | 100 | ||
| 5 year | 100 | 68.6 | 0.007 b | |
| Disease-free survival | ||||
| 1 year | 95.7 | 72.9 | ||
| 5 year | 93 | 48.6 | 0.002 b | |
| PNI | ||||
| negative | 49 (92.5%) | 3 (33.3%) | ||
| positive | 0 (0%) | 4 (44.5%) | ||
| n.a. | 4 (7.5%) | 2 (22.2%) | 0.001 a | |
| LVI | ||||
| negative | 44 (83.1%) | 5 (55.6%) | ||
| positive | 5 (9.4%) | 2 (22.2%) | ||
| n.a. | 4 (7.5%) | 2 (22.2%) | 0.169 a | |
| Extraparotid extension | ||||
| negative | 45 (84.9%) | 8 (88.9%) | ||
| positive | 3 (5.7%) | 1 (11.1%) | ||
| n.a. | 5 (9.4%) | 0 (0%) | 0.544 a | |
| Periparotid lymph node involvement | ||||
| negative | 35 (66.1%) | 9 (100%) | ||
| positive | 5 (9.4%) | 0 (0%) | ||
| n.a. | 13 (24.5%) | 0 (0%) | 0.116 a | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grasl, S.; Janik, S.; Grasl, M.C.; Pammer, J.; Formanek, M.; Weinreb, I.; Perez-Ordonez, B.; Hope, A.; Hosni, A.; de Almeida, J.R.; et al. Nodal Metastases in Acinic Cell Carcinoma of the Parotid Gland. J. Clin. Med. 2019, 8, 1315. https://doi.org/10.3390/jcm8091315
Grasl S, Janik S, Grasl MC, Pammer J, Formanek M, Weinreb I, Perez-Ordonez B, Hope A, Hosni A, de Almeida JR, et al. Nodal Metastases in Acinic Cell Carcinoma of the Parotid Gland. Journal of Clinical Medicine. 2019; 8(9):1315. https://doi.org/10.3390/jcm8091315
Chicago/Turabian StyleGrasl, Stefan, Stefan Janik, Matthaeus C. Grasl, Johannes Pammer, Michael Formanek, Ilan Weinreb, Bayardo Perez-Ordonez, Andrew Hope, Ali Hosni, John R. de Almeida, and et al. 2019. "Nodal Metastases in Acinic Cell Carcinoma of the Parotid Gland" Journal of Clinical Medicine 8, no. 9: 1315. https://doi.org/10.3390/jcm8091315
APA StyleGrasl, S., Janik, S., Grasl, M. C., Pammer, J., Formanek, M., Weinreb, I., Perez-Ordonez, B., Hope, A., Hosni, A., de Almeida, J. R., Irish, J., Gilbert, R., Goldstein, D. P., & Erovic, B. M. (2019). Nodal Metastases in Acinic Cell Carcinoma of the Parotid Gland. Journal of Clinical Medicine, 8(9), 1315. https://doi.org/10.3390/jcm8091315