A Randomized Comparison between 4, 6 and 8 mL of Local Anesthetic for Ultrasound-Guided Stellate Ganglion Block

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
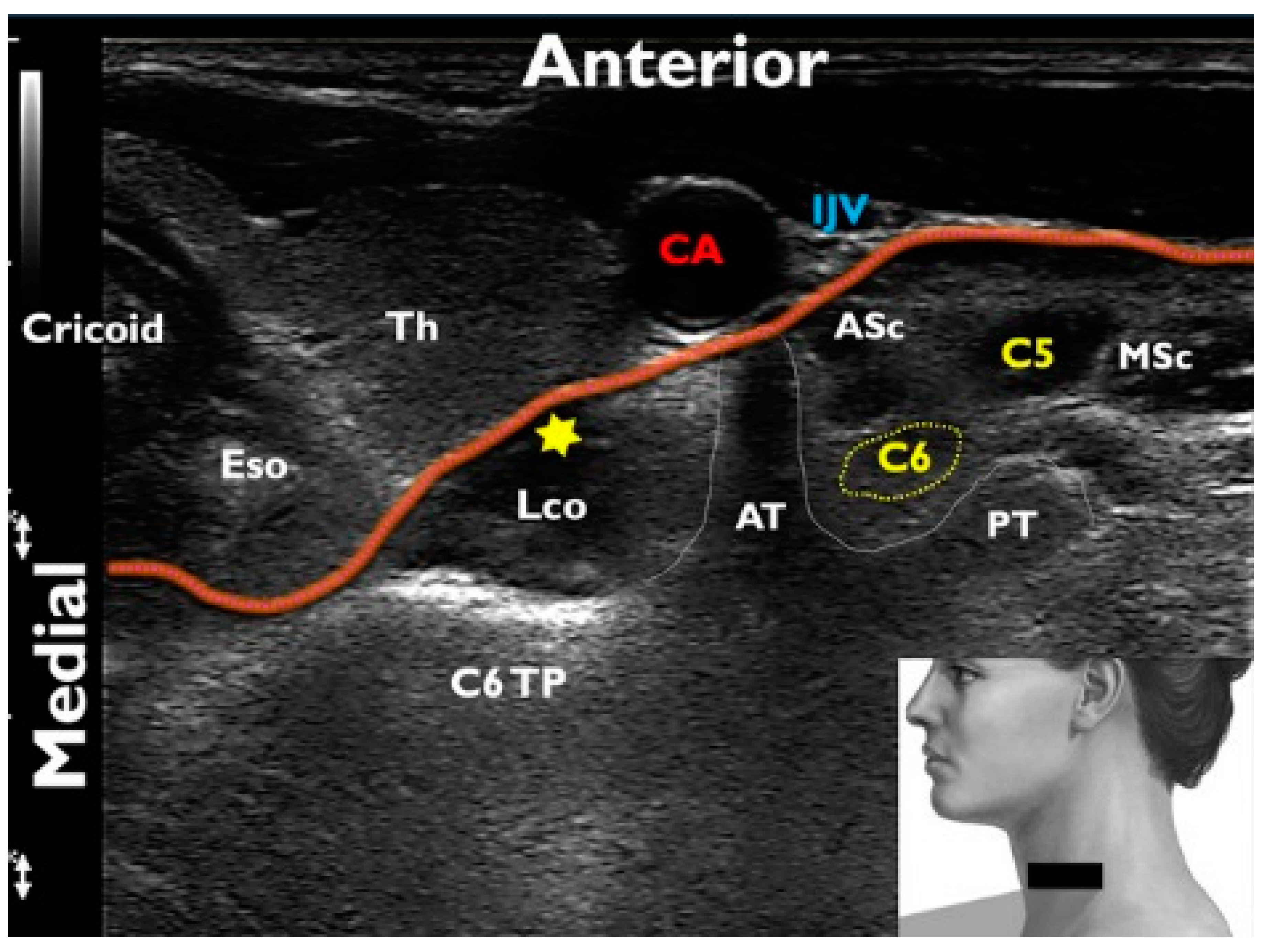
2.1. Stellate Ganglion Block
2.2. Statistical Analyses
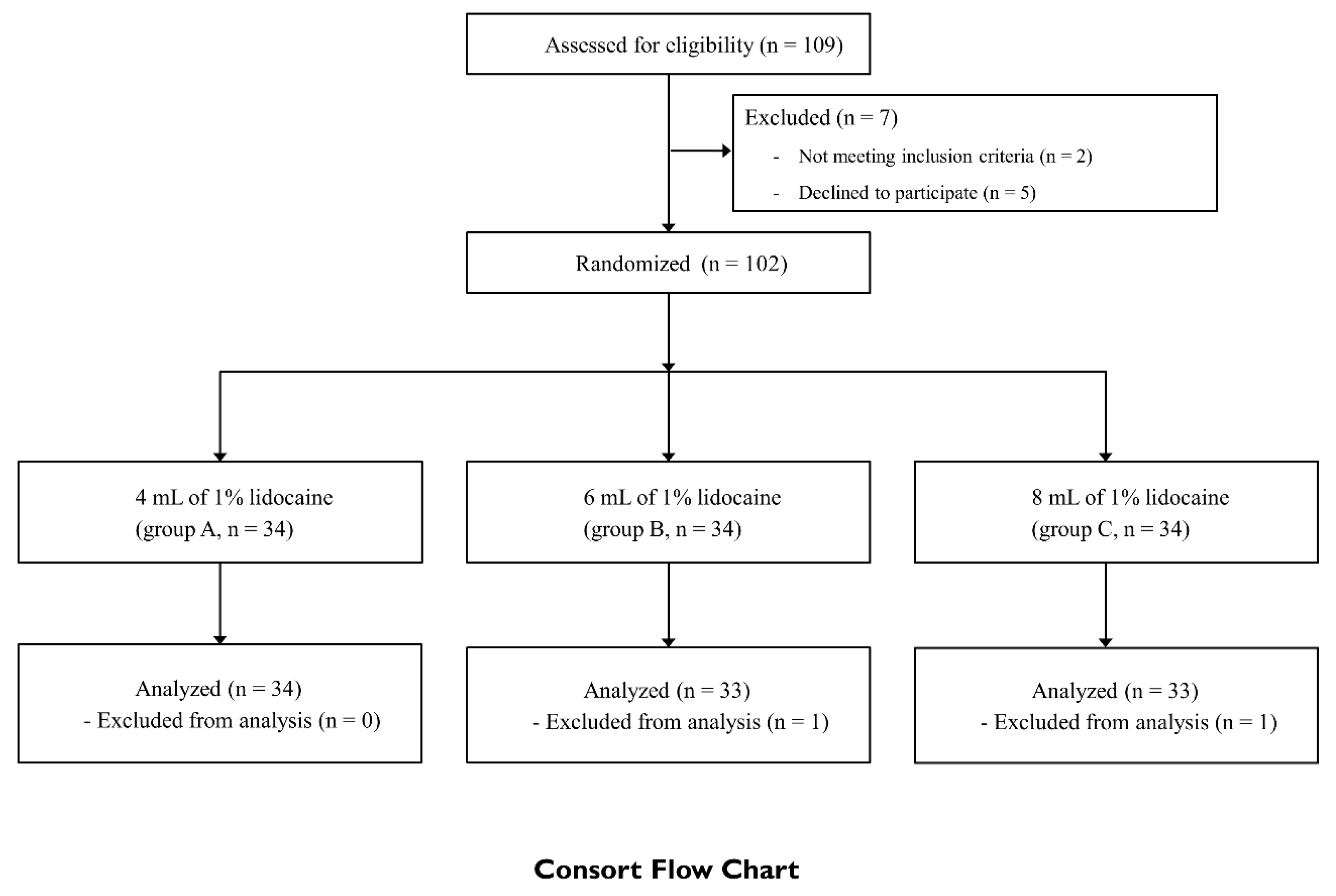
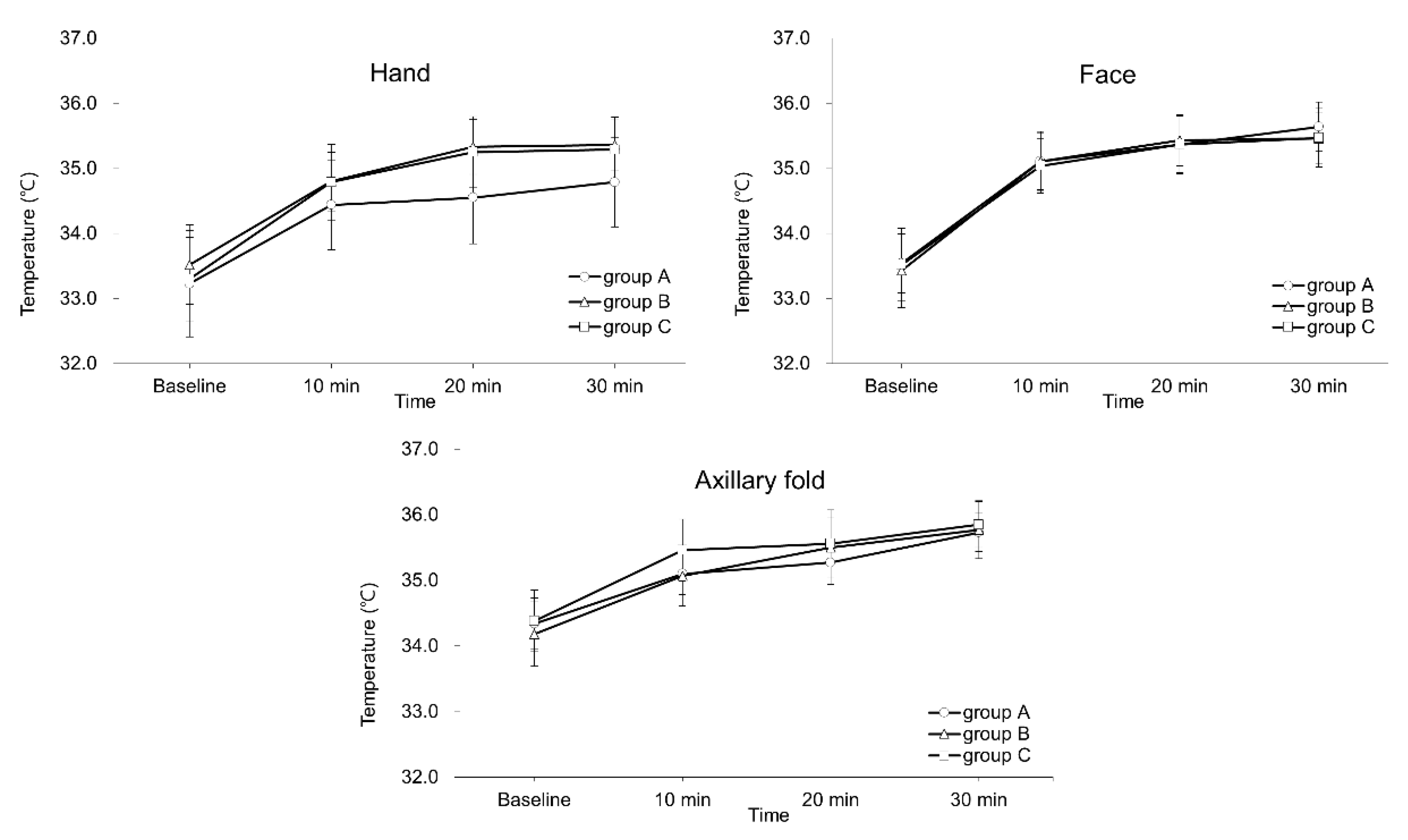
3. Results
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Salvaggio, I.; Adducci, E.; Dell’Aquila, L.; Rinaldi, S.; Marini, M.; Zappia, L.; Mascaro, A. Facial pain: A possible therapy with stellate ganglion block. Pain Med. Malden Mass. 2008, 9, 958–962. [Google Scholar] [CrossRef] [PubMed]
- Elias, M. Cervical sympathetic and stellate ganglion blocks. Pain Phys. 2000, 3, 294–304. [Google Scholar]
- Yoo, S.D.; Jung, S.S.; Kim, H.S.; Yun, D.H.; Kim, D.H.; Chon, J.; Hong, D.W. Efficacy of ultrasonography guided stellate ganglion blockade in the stroke patients with complex regional pain syndrome. Ann. Rehabil. Med. 2012, 36, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Makharita, M.Y.; Amr, Y.M.; El-Bayoumy, Y. Effect of early stellate ganglion blockade for facial pain from acute herpes zoster and incidence of postherpetic neuralgia. Pain Phys. 2012, 15, 467–474. [Google Scholar]
- McDonnell, J.G.; Finnerty, O.; Laffey, J.G. Stellate ganglion blockade for analgesia following upper limb surgery. Anaesthesia 2011, 66, 611–614. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Min, Y.S.; Chun, S.M.; Seo, K.S. Effects of stellate ganglion block on breast cancer-related lymphedema: Comparison of various injectates. Pain Phys. 2015, 18, 93–99. [Google Scholar]
- Jeon, Y.; Kim, D. The effect of stellate ganglion block on the atypical facial pain. J. Dent. Anesth. Pain Med. 2015, 15, 35–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soneji, N.; Peng, P.W. Ultrasound-guided pain interventions - a review of techniques for peripheral nerves. Korean J. Pain 2013, 26, 111–124. [Google Scholar] [CrossRef] [PubMed]
- Huntoon, M.A. The vertebral artery is unlikely to be the sole source of vascular complications occurring during stellate ganglion block. Pain Pract. 2010, 10, 25–30. [Google Scholar] [CrossRef]
- Honma, M.; Murakami, G.; Sato, T.J.; Namiki, A. Spread of injectate during C6 stellate ganglion block and fascial arrangement in the prevertebral region: An experimental study using donated cadavers. Reg. Anesth. Pain Med. 2000, 25, 573–583. [Google Scholar] [CrossRef]
- Nishiyama, T.; Matsukawa, T.; Yamashita, K. Comparison between neurotropin and mepivacaine for stellate ganglion injection. J. Anesth. 2006, 20, 240–242. [Google Scholar] [CrossRef] [PubMed]
- Stevens, R.A.; Stotz, A.; Kao, T.C.; Powar, M.; Burgess, S.; Kleinman, B. The relative increase in skin temperature after stellate ganglion block is predictive of a complete sympathectomy of the hand. Reg. Anesth. Pain Med. 1998, 23, 266–270. [Google Scholar] [PubMed]
- Goel, V.; Patwardhan, A.M.; Ibrahim, M.; Howe, C.L.; Schultz, D.M.; Shankar, H. Complications associated with stellate ganglion nerve block: A systematic review. Reg. Anesth. Pain Med. 2019, 44, 669–678. [Google Scholar] [CrossRef] [PubMed]
- Kapral, S.; Krafft, P.; Gosch, M.; Fleischmann, D.; Weinstabl, C. Ultrasound imaging for stellate ganglion block: Direct visualization of puncture site and local anesthetic spread. A pilot study. Reg. Anesth. 1995, 20, 323–328. [Google Scholar] [PubMed]
- Lee, M.H.; Kim, K.Y.; Song, J.H.; Jung, H.J.; Lim, H.K.; Lee, D.I.; Cha, Y.D. Minimal volume of local anesthetic required for an ultrasound-guided SGB. Pain Med. Malden Mass. 2012, 13, 1381–1388. [Google Scholar] [CrossRef] [PubMed]
- Yeo, J.; Jeon, Y. Effects of stellate ganglion block on sedation as assessed by bispectral index in normal healthy volunteers. Pain Phys. 2015, 18, 173–178. [Google Scholar]
- Jung, G.; Kim, B.S.; Shin, K.B.; Park, K.B.; Kim, S.Y.; Song, S.O. The optimal volume of 0.2% ropivacaine required for an ultrasound-guided stellate ganglion block. Korean J. Anesth. 2011, 60, 179–184. [Google Scholar] [CrossRef] [Green Version]
- Groves, T. Enhancing the quality and transparency of health research. BMJ 2008, 337, a718. [Google Scholar] [CrossRef]
- Minville, V.; Gendre, A.; Hirsch, J.; Silva, S.; Bourdet, B.; Barbero, C.; Fourcade, O.; Samii, K.; Bouaziz, H. The efficacy of skin temperature for block assessment after infraclavicular brachial plexus block. Anesth. Analg. 2009, 108, 1034–1036. [Google Scholar] [CrossRef]
- Putterman, A.M. Margin reflex distance (MRD) 1, 2, and 3. Ophthalmic Plast. Reconstr. Surg. 2012, 28, 308–311. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brittain, E.; Lin, D. A comparison of intent-to-treat and per-protocol results in antibiotic non-inferiority trials. Stat. Med. 2005, 24, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Benzon, H.T.; Cheng, S.C.; Avram, M.J.; Molloy, R.E. Sign of complete sympathetic blockade: Sweat test or sympathogalvanic response? Anesth. Analg. 1985, 64, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Ash, C.J.; Shealy, C.N.; Young, P.A.; Van Beaumont, W. Thermography and the sensory dermatome. Skelet. Radiol. 1986, 15, 40–46. [Google Scholar] [CrossRef]
- Hogan, Q.H.; Erickson, S.J. MR imaging of the stellate ganglion: Normal appearance. AJR. Am. J. Roentgenol. 1992, 158, 655–659. [Google Scholar] [CrossRef] [PubMed]
- Chung, I.H.; Oh, C.S.; Koh, K.S.; Kim, H.J.; Paik, H.C.; Lee, D.Y. Anatomic variations of the T2 nerve root (including the nerve of Kuntz) and their implications for sympathectomy. J. Thorac. Cardiovasc. Surg. 2002, 123, 498–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, E.; Yoshimura, T.; Omura, Y.; Sakaguchi, M.; Nishio, Y.; Maegawa, H.; Hisatomi, A.; Fujimoto, K.; Takeda, J.; Kashiwagi, A. Higher arterial stiffness, greater peripheral vascular resistance and lower blood flow in lower-leg arteries are associated with long-term hyperglycaemia in type 2 diabetic patients with normal ankle-brachial index. Diabetes Metab. Res. Rev. 2009, 25, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Arosio, E.; De Marchi, S.; Rigoni, A.; Prior, M.; Lechi, A. Effects of smoking on cardiopulmonary baroreceptor activation and peripheral vascular resistance. Eur. J. Clin. Investig. 2006, 36, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, K.C.; Guller, U.; Steele, S.M.; Klein, S.M.; Greengrass, R.A.; Pietrobon, R. Influence of obesity on surgical regional anesthesia in the ambulatory setting: An analysis of 9,038 blocks. Anesthesiology 2005, 102, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Sherman, R.A.; Woerman, A.L.; Karstetter, K.W. Comparative effectiveness of videothermography, contact thermography, and infrared beam thermography for scanning relative skin temperature. J. Rehabil. Res. Dev. 1996, 33, 377–386. [Google Scholar] [PubMed]
- Fernández-Cuevas, I.; Bouzas Marins, J.C.; Arnáiz Lastras, J.; Gómez Carmona, P.M.; Piñonosa Cano, S.; García-Concepción, M.Á.; Sillero-Quintana, M. Classification of factors influencing the use of infrared thermography in humans: A review. Infrared Phys. Technol. 2015, 71, 28–55. [Google Scholar] [CrossRef]
- Kim, M.K.; Yi, M.S.; Park, P.G.; Kang, H.; Lee, J.S.; Shin, H.Y. Effect of Stellate Ganglion Block on the Regional Hemodynamics of the Upper Extremity: A Randomized Controlled Trial. Anesth. Analg. 2018, 126, 1705–1711. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 100) | Group A (n = 34) | Group B (n = 33) | Group C (n = 33) | |
|---|---|---|---|---|
| Sex, n (%) | ||||
| Female | 68 (68.0%) | 22 (64.7%) | 21 (63.6%) | 25 (75.8%) |
| Male | 32 (32.0%) | 12 (35.3%) | 12 (36.4%) | 8 (24.2%) |
| Age, years | 51.3 ± 13.8 | 50.7 ± 16.1 | 50.2 ± 12.8 | 52.9 ± 12.4 |
| Body mass index, kg/m2 | 24.1 ± 3.9 | 24.1 ± 3.6 | 24.6 ± 4.5 | 23.7 ± 3.6 |
| Smoking, n (%) | 11 (11.0%) | 5 (14.7%) | 2 (6.1%) | 4 (12.1%) |
| Diabetes Mellitus, n (%) | 13 (13.0%) | 3 (8.8%) | 6 (18.2%) | 4 (12.1%) |
| Diagnosis, n (%) | ||||
| Face | 40 (40.0%) | 15 (44.1%) | 14 (42.4%) | 11 (33.3%) |
| TN | 6 | 7 | 2 | |
| AFP | 2 | 4 | 3 | |
| PHN | 2 | 1 | 1 | |
| Upper limb | 60 (60.0%) | 19 (55.9%) | 19 (57.6%) | 22 (66.7%) |
| CRPS | 5 | 8 | 4 | |
| PHN | 0 | 0 | 2 | |
| PTPS | 3 | 3 | 4 | |
| Other peripheral neuropathy * | 1 | 0 | 3 | |
| Duration of pain, months | 57.1 ± 55.1 | 51.7 ± 48.1 | 67.0 ± 48.2 | 52.3 ± 67.2 |
| Psychiatric comorbidity, n (%) | 40 (40.0%) | 11 (32.4%) | 14 (42.4%) | 15 (45.5%) |
| Laterality, n (%) | ||||
| Right | 48 (48.0%) | 15 (44.1%) | 19 (57.6%) | 14 (42.4%) |
| Left | 52 (52.0%) | 19 (55.9%) | 14 (42.4%) | 19 (57.6%) |
| Pre-NRS pain score | 6.0 [3.3–8.0] | 5.0 [4.0–7.3] | 5.0 [3.0–8.0] | 7.0 [5.0–8.0] |
| Mean Relative * Temperature Increase (°C) | Success Rate Ψ N (%) | 95% Confidence Intervals for the Difference of the Means | |
|---|---|---|---|
| Hand | |||
| Group A | 1.24 ± 0.84 | 15/19 (44.1%) | A versus B: −0.76 to 0.24 |
| Group B | 1.50 ± 0.68 | 15/18 (45.5%) | B versus C: −0.63 to 0.38 |
| Group C | 1.62 ± 1.02 | 18/15 (54.5%) | A versus C: −0.89 to 0.11 |
| Face | |||
| Group A | 1.77 ± 0.97 | 19/15 (55.8%) | A versus B: −0.14 to 1.04 |
| Group B | 1.25 ± 0.83 | 13/20 (39.3%) | B versus C: −0.89 to 0.17 |
| Group C | 1.61 ± 0.91 | 16/17 (48.5%) | A versus C: −0.37 to 0.68 |
| Axillary fold | |||
| Group A | 1.00 ± 0.73 | 8/26 (23.5%) | A versus B: −0.52 to 0.42 |
| Group B | 1.04 ± 0.80 | 12/21 (36.3%) | B versus C: −0.54 to 0.40 |
| Group C | 1.12 ± 0.89 | 11/22 (33.3%) | A versus C: −0.59 to 0.36 |
| Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| B (95% CI) | p-Value | B (95% CI) | p-Value | |
| Male Age | −0.25 (−0.91, 0.42) −0.01 (−0.03, 0.01) | 0.461 0.443 | 0.02 (−0.77, 0.81) −0.01 (−0.03, 0.01) | 0.958 0.288 |
| Body mass index, kg/m2 | −0.10 (−0.18, −0.02) | 0.013 | −0.10 (−0.18, −0.02) | 0.013 |
| Smoking DM Duration of pain | −0.81 (−1.79, 0.16) −0.72 (−1.63, 0.19) 0.001 (−0.004, 0.01) | 0.102 0.119 0.667 | −0.73 (−0.17, −0.02) −0.40 (−1.37, 0.57) | 0.135 0.417 |
| Location of pain | ||||
| Upper extremity | −0.07 (−0.70, 0.57) | 0.839 | ||
| Laterality (Right) | −0.21 (−0.83, 0.41) | 0.505 | ||
| Psychiatric comorbidity | −0.46 (−1.09, 0.17) | 0.148 | −0.32 (−0.98, 0.33) | 0.332 |
| Pre-NRS score Group | −0.03 (−0.15, 0.09) 0.22 (−0.16, 0.60) | 0.631 0.253 | ||
| Group | Group A (n = 34) | Group B (n = 33) | Group C (n = 33) | p-Value |
|---|---|---|---|---|
| Ptosis | 32 (94.1%) | 33 (100.0%) | 33 (100.0%) | 0.220 |
| Marginal reflex distance | 0.445 | |||
| None | 2 (5.9%) | 0 (0.0%) | 0 (0.0%) | |
| Mild | 20 (58.8%) | 20 (60.6%) | 21 (63.6%) | |
| Moderate | 12 (35.3%) | 9 (27.3%) | 10 (30.3%) | |
| Severe | 0 (0.0%) | 4 (12.1%) | 2 (6.1%) | |
| Hoarseness Dysphagia NRS reduction (%) | 4 (11.8%) 1 (2.9%) 6.5 [0.0‒30.0] | 5 (15.2%) 1 (3.0%) 20.0 [0.0‒30.5] | 5 (15.2%) 2 (6.1%) 22.0 [0.0‒50.0] | 0.878 0.844 0.371 |
| Other adverse effects * | 0 (0.0%) | 0 (0.0%) | 3 (9.1%) | 0.034 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, Y.; Lee, C.-s.; Kim, Y.-C.; Moon, J.Y.; Finlayson, R.J. A Randomized Comparison between 4, 6 and 8 mL of Local Anesthetic for Ultrasound-Guided Stellate Ganglion Block. J. Clin. Med. 2019, 8, 1314. https://doi.org/10.3390/jcm8091314
Yoo Y, Lee C-s, Kim Y-C, Moon JY, Finlayson RJ. A Randomized Comparison between 4, 6 and 8 mL of Local Anesthetic for Ultrasound-Guided Stellate Ganglion Block. Journal of Clinical Medicine. 2019; 8(9):1314. https://doi.org/10.3390/jcm8091314
Chicago/Turabian StyleYoo, Yongjae, Chang-soon Lee, Yong-Chul Kim, Jee Youn Moon, and Roderick J. Finlayson. 2019. "A Randomized Comparison between 4, 6 and 8 mL of Local Anesthetic for Ultrasound-Guided Stellate Ganglion Block" Journal of Clinical Medicine 8, no. 9: 1314. https://doi.org/10.3390/jcm8091314
APA StyleYoo, Y., Lee, C.-s., Kim, Y.-C., Moon, J. Y., & Finlayson, R. J. (2019). A Randomized Comparison between 4, 6 and 8 mL of Local Anesthetic for Ultrasound-Guided Stellate Ganglion Block. Journal of Clinical Medicine, 8(9), 1314. https://doi.org/10.3390/jcm8091314