Quality Assurance of Non-Invasive Prenatal Screening (NIPS) for Fetal Aneuploidy Using Positive Predictive Values as Outcome Measures

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
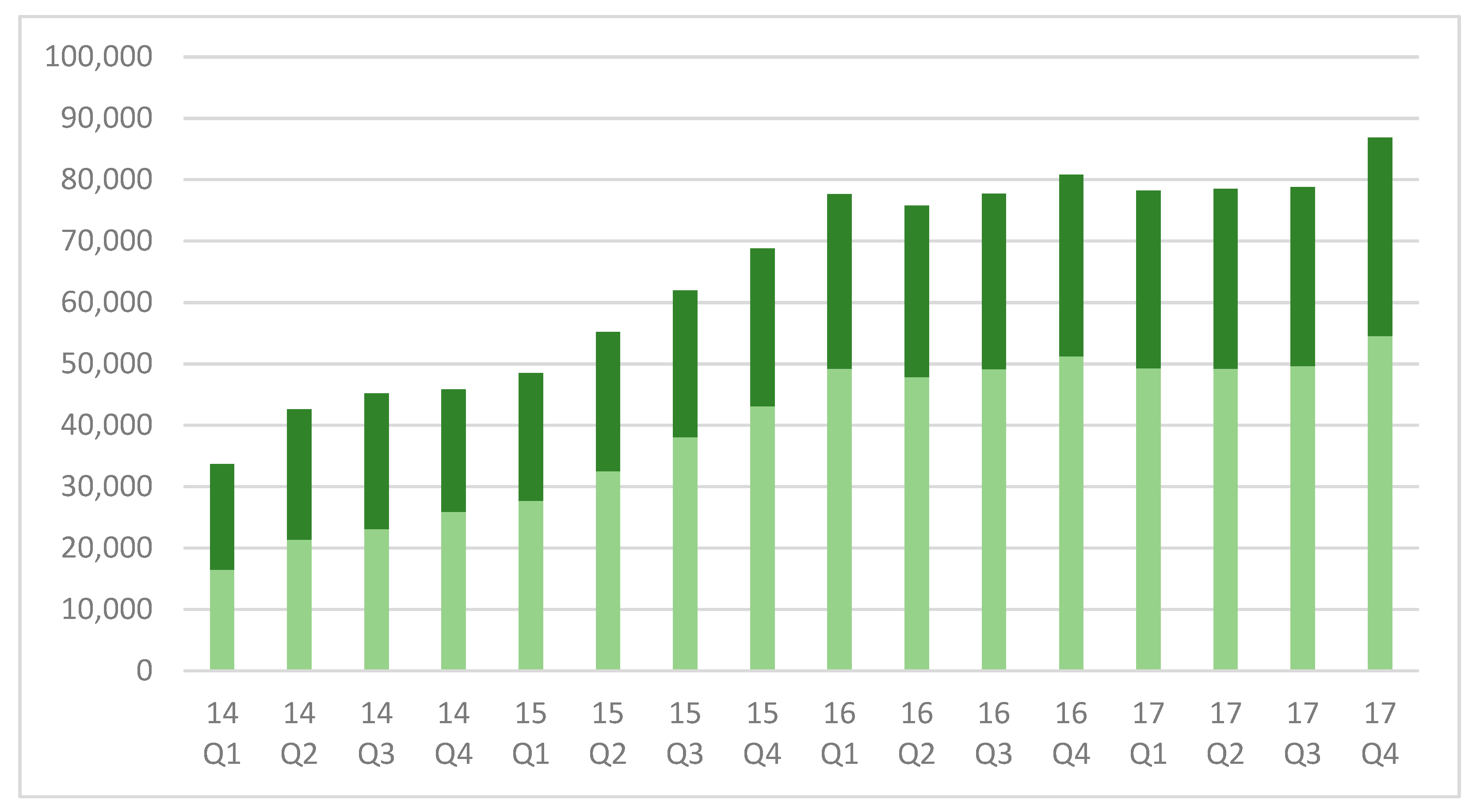
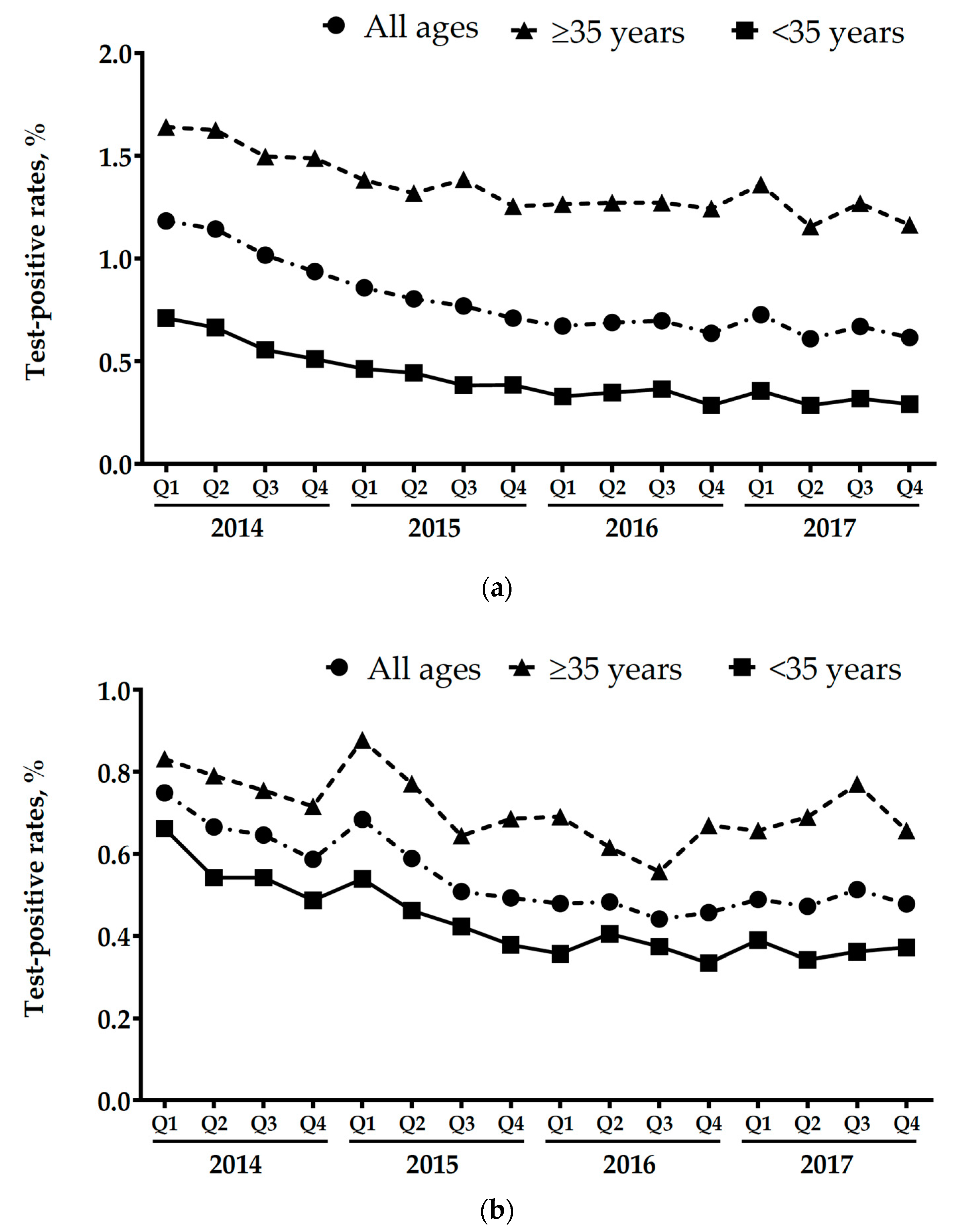
3.1. Changes in The Referral Population and Positive Test Rates
3.2. Overall Test Performance
3.3. Non-Inferiority Analysis
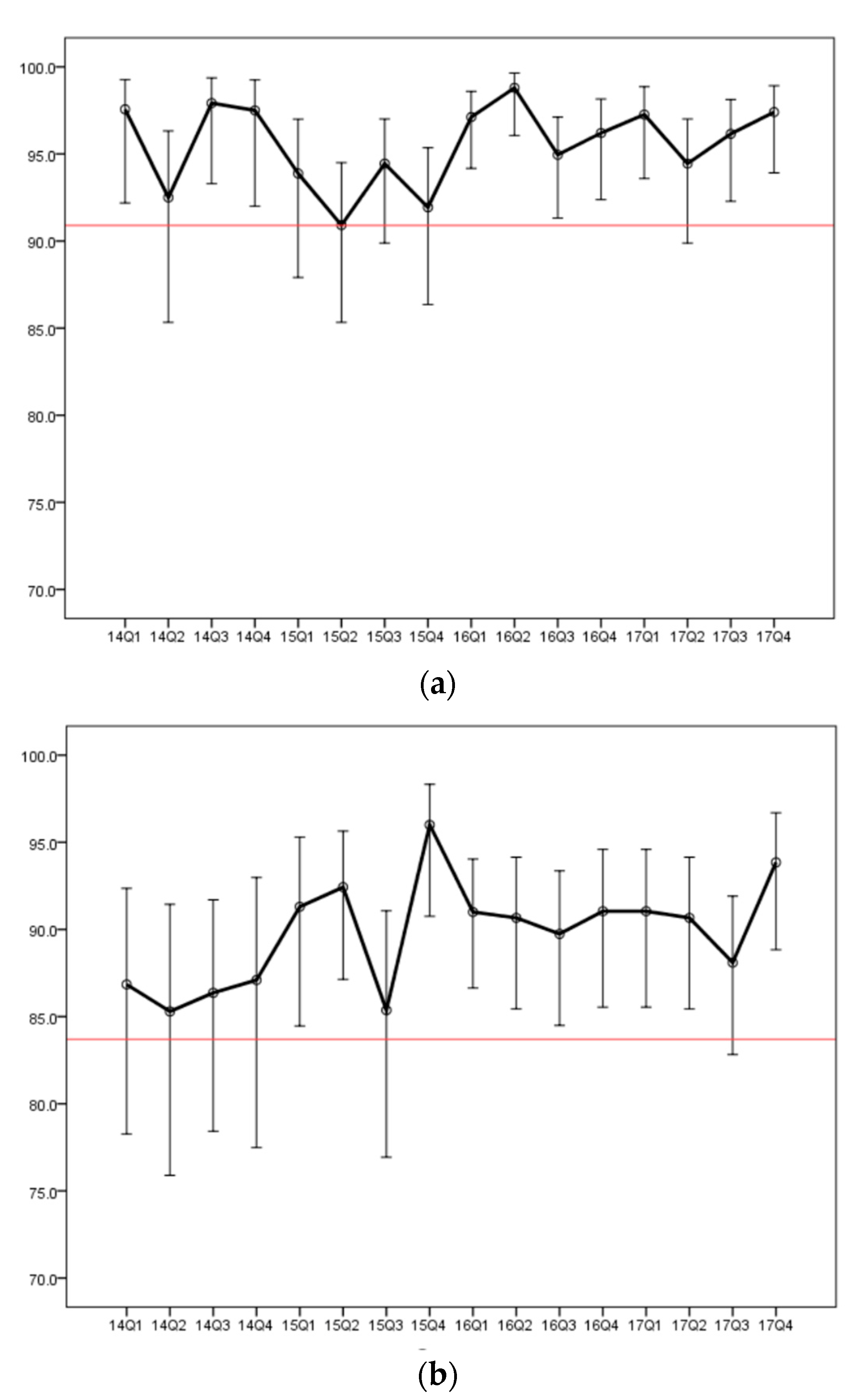
3.4. Trends in Positive Predictive Values
3.5. False-Negative Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cuckle, H.; Benn, P.; Pergament, E. Cell-free DNA screening for fetal aneuploidy as a clinical service. Clin. Biochem. 2015, 48, 932–941. [Google Scholar] [CrossRef] [PubMed]
- Gil, M.M.; Accurti, V.; Santacruz, B.; Plana, M.N.; Nicolaides, K.H. Analysis of cell-free DNA in maternal blood in screening for aneuploidies: updated meta-analysis. Ultrasound Obstet. Gynecol. 2017, 50, 302–314. [Google Scholar] [CrossRef] [PubMed]
- Santorum, M.; Wright, D.; Syngelaki, A.; Karagioti, N.; Nicolaides, K.H. Accuracy of first-trimester combined test in screening for trisomies 21, 18 and 13. Ultrasound Obstet. Gynecol. 2017, 49, 714–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Standards for Certification, Laboratory Requirements; Federal Register: Baltimore, MD, USA, 2007.
- College of American Pathologists. Laboratory General Checklist. 2018. Available online: http://www.cap.org (accessed on 5 May 2019).
- Skotko, B.G.; Allyse, M.A.; Bajaj, K.; Best, R.G.; Klugman, S.; Leach, M.; Meredith, S.; Michie, M.; Gregg, A.R. Adherence of cell-free DNA noninvasive prenatal screens to ACMG recommendations. Genet. Med. 2019, 1. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, B.; Hill, M.; Gemelos, G.; Demko, Z.; Banjevic, M.; Baner, J.; Ryan, A.; Sigurjonsson, S.; Chopra, N.; Dodd, M.; et al. Noninvasive prenatal aneuploidy testing of chromosomes 13, 18, 21, X, and Y, using targeted sequencing of polymorphic loci. Prenat. Diagn. 2012, 32, 1233–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pergament, E.; Cuckle, H.; Zimmermann, B.; Banjevic, M.; Sigurjonsson, S.; Ryan, A.; Hall, M.P.; Dodd, M.; Lacroute, P.; Stosic, M.; et al. Single-nucleotide polymorphism-based noninvasive prenatal screening in a high-risk and low-risk cohort. Obstet. Gynecol. 2014, 124, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Ryan, A.; Hunkapiller, N.; Banjevic, M.; Vankayalapati, N.; Fong, N.; Jinnett, K.N.; Demko, Z.; Zimmermann, B.; Sigurjonsson, S.; Gross, S.J.; et al. Validation of an Enhanced Version of a Single-Nucleotide Polymorphism-Based Noninvasive Prenatal Test for Detection of Fetal Aneuploidies. Fetal Diagn. Ther. 2016, 40, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Ravi, H.; McNeill, G.; Goel, S.; Meltzer, S.D.; Hunkapiller, N.; Ryan, A.; Levy, B.; Demko, Z.P. Validation of a SNP-based non-invasive prenatal test to detect the fetal 22q11.2 deletion in maternal plasma samples. PLoS ONE 2018, 13, e0193476. [Google Scholar] [CrossRef] [PubMed]
- Wapner, R.J.; Babiarz, J.E.; Levy, B.; Stosic, M.; Zimmermann, B.; Sigurjonsson, S.; Wayham, N.; Ryan, A.; Banjevic, M.; Lacroute, P.; et al. Expanding the scope of noninvasive prenatal testing: detection of fetal microdeletion syndromes. Am. J. Obstet. Gynecol. 2015, 212, 332 e1–332 e9. [Google Scholar] [CrossRef]
- Martin, K.; Iyengar, S.; Kalyan, A.; Lan, C.; Simon, A.L.; Stosic, M.; Kobara, K.; Ravi, H.; Truong, T.; Ryan, A.; et al. Clinical experience with a single-nucleotide polymorphism-based non-invasive prenatal test for five clinically significant microdeletions. Clin. Genet. 2018, 93, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Dar, P.; Curnow, K.J.; Gross, S.J.; Hall, M.P.; Stosic, M.; Demko, Z.; Zimmermann, B.; Hill, M.; Sigurjonsson, S.; Ryan, A.; et al. Clinical experience and follow-up with large scale single-nucleotide polymorphism-based noninvasive prenatal aneuploidy testing. Am. J. Obstet. Gynecol. 2014, 211, 527.e1–527.e17. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.; Nowacki, A.S. Understanding equivalence and noninferiority testing. J. Gen. Intern. Med. 2011, 26, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Taylor, T.H.; Gitlin, S.A.; Patrick, J.L.; Crain, J.L.; Wilson, J.M.; Griffin, D.K. The origin, mechanisms, incidence and clinical consequences of chromosomal mosaicism in humans. Hum. Reprod. Update. 2014, 20, 571–581. [Google Scholar] [CrossRef] [PubMed]
- Norton, M.E.; Jacobsson, B.; Swamy, G.K.; Laurent, L.C.; Ranzini, A.C.; Brar, H.; Tomlinson, M.W.; Pereira, L.; Spitz, J.L.; Hollemon, D.; et al. Cell-free DNA analysis for noninvasive examination of trisomy. N. Engl. J. Med. 2015, 372, 1589–1597. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Gao, Y.; Jiang, F.; Fu, M.; Yuan, Y.; Guo, Y.; Zhu, Z.; Lin, M.; Liu, Q.; Tian, Z.; et al. Non-invasive prenatal testing for trisomies 21, 18 and 13: clinical experience from 146,958 pregnancies. Ultrasound Obstet. Gynecol. 2015, 45, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Futch, T.; Spinosa, J.; Bhatt, S.; de Feo, E.; Rava, R.P.; Sehnert, A.J. Initial clinical laboratory experience in noninvasive prenatal testing for fetal aneuploidy from maternal plasma DNA samples. Prenat. Diagn. 2013, 33, 569–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snyder, H.L.; Curnow, K.J.; Bhatt, S.; Bianchi, D.W. Follow-up of multiple aneuploidies and single monosomies detected by noninvasive prenatal testing: implications for management and counseling. Prenat. Diagn. 2016, 36, 203–209. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Test | All Positive (%) | Follow-Up Solicited | Confirmation by Genetics | Confirmation by Genetics, Ultrasound, or Loss | |||||
|---|---|---|---|---|---|---|---|---|---|
| Follow-up Received | Abn Confirmed | PPV% (95% CI) | Follow-up Received | Abn Confirmed | PPV% (95% CI) | ||||
| All referrals (1,035,844) | T21 | 7802 (0.75) | 2347 | 884 | 837 | 94.7 (93.0–96.0) | 1,083 | 1036 | 95.7 (94.3–96.7) |
| T18 | 2205 (0.21) | 845 | 333 | 304 | 91.3 (87.8–93.9) | 476 | 447 | 93.9 (91.4–95.7) | |
| T13 | 1207 (0.12) | 344 | 118 | 80 | 67.8 (58.9–75.6) | 186 | 148 | 79.6 (73.2–84.7) | |
| MX | 2017 (0.19) | 535 | 120 | 93 | 77.5 (69.2–84.1) | 299 | 272 | 91.0 (87.2–93.7) | |
| All | 13,231 (1.28) | 4071 | 1455 | 1314 | 90.3 (88.7–91.7) | 2,044 | 1903 | 93.1 (91.9–94.1) | |
| Referrals from women <35 (628,242) | T21 | 2388 (0.38) | 711 | 271 | 248 | 91.5 (87.6–94.3) | 339 | 316 | 93.2 (90.0–95.4) |
| T18 | 666 (0.11) | 256 | 105 | 92 | 87.6 (80.0–92.6) | 152 | 139 | 91.4 (85.9–94.9) | |
| T13 | 540 (0.09) | 149 | 46 | 27 | 58.7 (44.3–71.7) | 84 | 65 | 77.4 (67.4–85.0) | |
| MX | 1361 (0.22) | 372 | 76 | 59 | 77.6 (58.2–77.4) | 212 | 195 | 92.0 (87.5–94.9) | |
| All | 4955 (0.79) | 1488 | 498 | 426 | 85.5 (82.2–88.4) | 787 | 715 | 90.9 (88.6–92.7) | |
| T21 | 5414 (1.33) | 1636 | 613 | 589 | 96.1 (94.2–97.4) | 744 | 720 | 96.8 (95.3–97.8) | |
| Referrals from women ≥35 (407,602) | T18 | 1539 (0.38) | 589 | 228 | 212 | 93.0 (88.9–95.6) | 324 | 308 | 95.1 (92.1–96.9) |
| T13 | 667 (0.16) | 195 | 72 | 53 | 73.6 (62.4–82.4) | 102 | 83 | 81.4 (72.7–87.7) | |
| MX | 656 (0.16) | 163 | 44 | 34 | 77.3 (63.0–87.2) | 87 | 77 | 88.5 (80.1–93.6) | |
| All | 8,276 (2.03) | 2583 | 957 | 888 | 92.8 (91.0–94.3) | 1257 | 1188 | 94.5 (93.1–95.6) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
DiNonno, W.; Demko, Z.; Martin, K.; Billings, P.; Egbert, M.; Zneimer, S.; Keen-Kim, D.; Benn, P. Quality Assurance of Non-Invasive Prenatal Screening (NIPS) for Fetal Aneuploidy Using Positive Predictive Values as Outcome Measures. J. Clin. Med. 2019, 8, 1311. https://doi.org/10.3390/jcm8091311
DiNonno W, Demko Z, Martin K, Billings P, Egbert M, Zneimer S, Keen-Kim D, Benn P. Quality Assurance of Non-Invasive Prenatal Screening (NIPS) for Fetal Aneuploidy Using Positive Predictive Values as Outcome Measures. Journal of Clinical Medicine. 2019; 8(9):1311. https://doi.org/10.3390/jcm8091311
Chicago/Turabian StyleDiNonno, Wendy, Zachary Demko, Kimberly Martin, Paul Billings, Melissa Egbert, Susan Zneimer, Dianne Keen-Kim, and Peter Benn. 2019. "Quality Assurance of Non-Invasive Prenatal Screening (NIPS) for Fetal Aneuploidy Using Positive Predictive Values as Outcome Measures" Journal of Clinical Medicine 8, no. 9: 1311. https://doi.org/10.3390/jcm8091311
APA StyleDiNonno, W., Demko, Z., Martin, K., Billings, P., Egbert, M., Zneimer, S., Keen-Kim, D., & Benn, P. (2019). Quality Assurance of Non-Invasive Prenatal Screening (NIPS) for Fetal Aneuploidy Using Positive Predictive Values as Outcome Measures. Journal of Clinical Medicine, 8(9), 1311. https://doi.org/10.3390/jcm8091311