A Lesion-Based Convolutional Neural Network Improves Endoscopic Detection and Depth Prediction of Early Gastric Cancer

 , , , ,
, , , ,
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Data Preparation (Endoscopic Image Collection)
2.3. Convolutional Neural Network and Training
2.4. Evaluation
2.5. Statistical Analysis
3. Results
3.1. Baseline Clinicopathological Characteristics of the Subjects
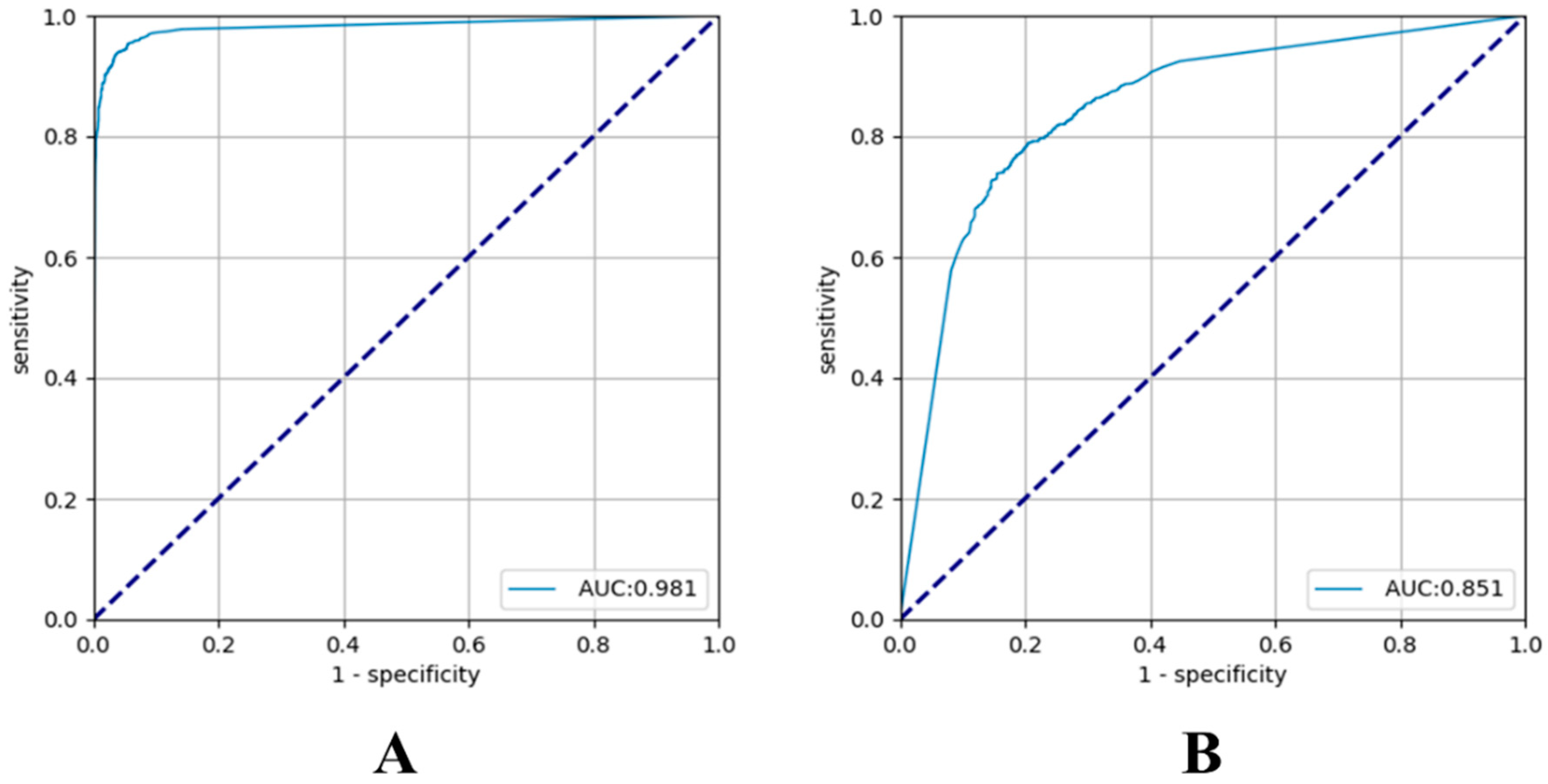
3.2. Diagnostic Performance Using the VGG-16
3.3. Localization Ability of the Activated Regions
3.4. Factors Associated with the Accuracy of Tumor Detection by AI
3.5. Factors Associated with the Accuracy of T-Staging by AI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Wang, J.; Yu, J.C.; Kang, W.M.; Ma, Z.Q. Treatment strategy for early gastric cancer. Surg. Oncol. 2012, 21, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Goto, O.; Fujishiro, M.; Kodashima, S.; Ono, S.; Omata, M. Outcomes of endoscopic submucosal dissection for early gastric cancer with special reference to validation for curability criteria. Endoscopy 2009, 41, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, K. The Most Important Prognostic Factors for Gastric Cancer Patients: A Study Using Univariate and Multivariate Analyses. Scand. J. Gastroenterol. 1987, 22 (Suppl. 133), 63–68. [Google Scholar] [CrossRef]
- Mocellin, S.; Marchet, A.; Nitti, D. EUS for the staging of gastric cancer: A meta-analysis. Gastrointest. Endosc. 2011, 73, 1122–1134. [Google Scholar] [CrossRef] [PubMed]
- Yanai, H.; Matsumoto, Y.; Harada, T.; Nishiaki, M.; Tokiyama, H.; Shigemitsu, T.; Tada, M.; Okita, K. Endoscopic ultrasonography and endoscopy for staging depth of invasion in early gastric cancer: A pilot study. Gastrointest. Endosc. 1997, 46, 212–216. [Google Scholar] [CrossRef]
- Choi, J.; Kim, S.G.; Im, J.P.; Kim, J.S.; Jung, H.C.; Song, I.S. Comparison of endoscopic ultrasonography and conventional endoscopy for prediction of depth of tumor invasion in early gastric cancer. Endoscopy 2010, 42, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Pei, Q.; Wang, L.; Pan, J.; Ling, T.; Lv, Y.; Zou, X. Endoscopic ultrasonography for staging depth of invasion in early gastric cancer: A meta-analysis. J. Gastroenterol. Hepatol. 2015, 30, 1566–1573. [Google Scholar] [CrossRef]
- Schmidt-Erfurth, U.; Sadeghipour, A.; Gerendas, B.S.; Waldstein, S.M.; Bogunovic, H. Artificial intelligence in retina. Prog. Retin. Eye Res. 2018, 67, 1–29. [Google Scholar] [CrossRef]
- Alagappan, M.; Brown, J.R.G.; Mori, Y.; Berzin, T.M. Artificial intelligence in gastrointestinal endoscopy: The future is almost here. World J. Gastrointest. Endosc. 2018, 10, 239–249. [Google Scholar] [CrossRef]
- Hirasawa, T.; Aoyama, K.; Tanimoto, T.; Ishihara, S.; Shichijo, S.; Ozawa, T.; Ohnishi, T.; Fujishiro, M.; Matsuo, K.; Fujisaki, J.; et al. Application of artificial intelligence using a convolutional neural network for detecting gastric cancer in endoscopic images. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2018, 21, 653–660. [Google Scholar]
- Horie, Y.; Yoshio, T.; Aoyama, K.; Yoshimizu, S.; Horiuchi, Y.; Ishiyama, A.; Hirasawa, T.; Tsuchida, T.; Ozawa, T.; Ishihara, S.; et al. Diagnostic outcomes of esophageal cancer by artificial intelligence using convolutional neural networks. Gastrointest. Endosc. 2019, 89, 25–32. [Google Scholar] [CrossRef]
- Urban, G.; Tripathi, P.; Alkayali, T.; Mittal, M.; Jalali, F.; Karnes, W.; Baldi, P. Deep Learning Localizes and Identifies Polyps in Real Time with 96% Accuracy in Screening Colonoscopy. Gastroenterology 2018, 155, 1069–1078.e8. [Google Scholar] [CrossRef]
- Stone, M. Cross-validatory choice and assessment of statistical predictions. J. R. Stat. Soc. Ser. B 1974, 36, 111–147. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M. Imagenet large scale visual recognition challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-CAM: Visual Explanations from Deep Networks via Gradient-Based Localization; ICCV: Venice, Italy, 2017; pp. 618–626. Available online: http://openaccess.thecvf.com/content_iccv_2017/html/Selvaraju_Grad-AM_Visual_Explanations_ICCV_2017_paper.html (accessed on 22 August 2019).
- De Boer, P.-T.; Kroese, D.P.; Mannor, S.; Rubinstein, R.Y. A tutorial on the cross-entropy method. Ann. Oper. Res. 2005, 134, 19–67. [Google Scholar] [CrossRef]
- Zeiler, M.D.; Fergus, R. Proceedings of the Visualizing and Understanding Convolutional Networks; ECCV: Zurich, Switzerland, 2014; pp. 818–833. [Google Scholar]
- Simonyan, K.; Vedaldi, A.; Zisserman, A. Deep inside convolutional networks: Visualising image classification models and saliency maps. arXiv 2013, arXiv:1312.6034. [Google Scholar]
- Kim, T.Y.; Yi, N.H.; Hwang, J.W.; Kim, J.H.; Kim, G.H.; Kang, M.S. Morphologic pattern analysis of submucosal deformities identified by endoscopic ultrasonography for predicting the depth of invasion in early gastric cancer. Surg. Endosc. 2018, 33, 2169–2180. [Google Scholar] [CrossRef]
- Han, Y.; Sun, S.; Guo, J.; Ge, N.; Wang, S.; Liu, X.; Wang, G.; Hu, J.; Wang, S. Is endoscopic ultrasonography useful for endoscopic submucosal dissection? Endosc. Ultrasound 2016, 5, 284–290. [Google Scholar]
- Kim, J.; Kim, S.G.; Chung, H.; Lim, J.H.; Choi, J.M.; Park, J.Y.; Yang, H.J.; Han, S.J.; Oh, S.; Kim, M.S.; et al. Clinical efficacy of endoscopic ultrasonography for decision of treatment strategy of gastric cancer. Surg. Endosc. 2018, 32, 3789–3797. [Google Scholar] [CrossRef]
- Choi, J.; Kim, S.G.; Im, J.P.; Kim, J.S.; Jung, H.C.; Song, I.S. Endoscopic prediction of tumor invasion depth in early gastric cancer. Gastrointest. Endosc. 2011, 73, 917–927. [Google Scholar] [CrossRef]
- Tsujii, Y.; Kato, M.; Inoue, T.; Yoshii, S.; Nagai, K.; Fujinaga, T.; Maekawa, A.; Hayashi, Y.; Akasaka, T.; Shinzaki, S.; et al. Integrated diagnostic strategy for the invasion depth of early gastric cancer by conventional endoscopy and EUS. Gastrointest. Endosc. 2015, 82, 452–459. [Google Scholar] [CrossRef]
- Zhu, Y.; Wang, Q.C.; Xu, M.D.; Zhang, Z.; Chen, J.; Zhong, Y.S.; Zhang, Y.Q.; Chen, W.F.; Yao, L.Q.; Zhou, P.H.; et al. Application of convolutional neural network in the diagnosis of the invasion depth of gastric cancer based on conventional endoscopy. Gastrointest. Endosc. 2019, 89, 806–815. [Google Scholar] [CrossRef]
- Kim, J.H.; Song, K.S.; Youn, Y.H.; Lee, Y.C.; Cheon, J.H.; Song, S.Y.; Chung, J.B. Clinicopathologic factors influence accurate endosonographic assessment for early gastric cancer. Gastrointest. Endosc. 2007, 66, 901–908. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the CVPR, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Age (years, mean ± SD) | 62.6 ± 12.2 |
| Male (n, %) | 536 (67.2) |
| Tumor size (mm, mean ± SD) | 23.7 ± 15.1 |
| Location of lesion (n, %) | - |
| Upper one-third | 74 (9.3) |
| Middle one-third | 118 (14.7) |
| Lower one-third | 608 (76) |
| Gross type (n, %) | - |
| Elevated | 171 (21.4) |
| Flat | 285 (35.6) |
| Depressed | 344 (43) |
| Lymphovascular invasion (n, %) | 82 (10.3) |
| Perineural invasion (n, %) | 14 (1.8) |
| T-stage (n, %) | - |
| Mucosa (T1a) | 428 (53.5) |
| Submucosa (T1b) | 372 (46.5) |
| WHO classification (n, %) | - |
| Well-differentiated | 321 (40.1) |
| Moderately-differentiated | 268 (33.5) |
| Poorly-differentiated | 103 (12.9) |
| Signet ring cell carcinoma | 108 (13.5) |
| Japanese classification (n, %) | - |
| Differentiated | 589 (73.6) |
| Undifferentiated | 211 (26.4) |
| Lauren classification (n, %) | - |
| Intestinal | 606 (77.3) |
| Diffuse | 156 (19.9) |
| Mixed | 22 (2.8) |
| Variables | Accurate | Inaccurate | p-Value | Odds Ratio (95% CI) | p-Value |
|---|---|---|---|---|---|
| Gross type (n, %) | - | - | 0.038 | - | - |
| Elevated | 169 (21.7) | 2 (10.5) | - | - | - |
| Flat | 271 (34.9) | 12 (63.2) | - | - | - |
| Depressed | 337 (43.4) | 5 (26.3) | - | - | - |
| T-stage (n, %) | - | - | 0.001 | - | 0.019 |
| Mucosa (T1a) | 406 (52.3) | 17 (89.5) | - | ref | - |
| Submucosa (T1b) | 371 (47.7) | 2 (10.5) | - | 5.891 (1.326–26.171) | - |
| Size (n, %) | - | - | 0.002 | - | 0.006 |
| 1–13 mm | 162 (21.7) | 11 (57.9) | - | ref | - |
| ≥14 mm | 608 (78.3) | 8 (42.1) | - | 3.660 (1.427–9.384) | - |
| Location of lesion (n, %) | - | - | 0.780 | - | - |
| Upper one-third | 72 (9.3) | 2 (10.5) | - | - | - |
| Mid one-third | 115 (14.8) | 3 (15.8) | - | - | - |
| Lower one-third | 590 (75.9) | 14 (73.7) | - | - | - |
| Japanese classification (n, %) | - | - | 0.296 | - | - |
| Differentiated | 575 (74) | 12 (63.2) | - | - | - |
| Undifferentiated | 202 (26) | 7 (36.8) | - | - | - |
| Variables | Accurate | Inaccurate | p-Value | Odds Ratio (95% CI) | p-Value |
|---|---|---|---|---|---|
| Japanese classification (n, %) | - | - | 0.001 | - | 0.033 |
| Differentiated | 446 (76.8) | 132 (65.0) | - | ref | - |
| Undifferentiated | 135 (23.2) | 71 (35.0) | - | 0.491 (0.255–0.945) | - |
| Gross type (n, %) | - | - | 0.442 | - | - |
| Elevated | 127 (21.9) | 41 (20.2) | - | - | - |
| Flat | 212 (36.5) | 67 (33.0) | - | - | - |
| Depressed | 242 (41.6) | 95 (46.8) | - | - | - |
| T-stage (n, %) | - | - | 0.235 | - | - |
| Mucosa (T1a) | 320 (55.1) | 102 (50.3) | - | - | - |
| Submucosa (T1b) | 261 (44.9) | 101 (49.7) | - | - | - |
| Size (n, %) | - | - | 0.329 | - | - |
| 1–13 mm | 137 (23.7) | 44 (21.8) | - | - | - |
| ≥14 mm | 442 (76.3) | 158 (78.2) | - | - | - |
| Variables | Accurate | Inaccurate | p-Value | Odds Ratio (95% CI) | p-Value |
|---|---|---|---|---|---|
| T-stage (n, %) | - | - | 0.015 | - | 0.015 |
| Mucosa (T1a) | 97 (71.9) | 39 (54.9) | - | ref | - |
| Submucosa (T1b) | 38 (28.1) | 32 (45.1) | - | 0.477 (0.262–0.869) | - |
| Gross type (n, %) | - | - | 0.152 | - | - |
| Elevated | 15 (11.1) | 7 (9.9) | - | - | - |
| Flat | 55 (40.7) | 20 (28.1) | - | - | - |
| Depressed | 65 (48.2) | 44 (62.0) | - | - | - |
| Size (n, %) | - | - | 0.444 | - | - |
| 1–13 mm | 24 (17.9) | 14 (19.7) | - | - | - |
| ≥ 14 mm | 110 (82.1) | 57 (80.3) | - | - | - |
| WHO classification (n, %) | - | - | 0.296 | - | - |
| APD | 60 (44.4) | 38 (53.5) | - | - | - |
| SRC | 75 (55.6) | 33 (46.5) | - | - | - |
| Variables | T1a | T1b | p-Value |
|---|---|---|---|
| Gross type (n, %) | - | - | 0.003 |
| Elevated | 8 (5.8) | 14 (19.2) | - |
| Flat | 57 (41.3) | 19 (26.0) | - |
| Depressed | 73 (52.9) | 40 (54.8) | - |
| Sex (n, %) | - | - | 0.012 |
| Male | 60 (43.5) | 45 (61.6) | - |
| Female | 78 (56.5) | 28 (38.4) | - |
| Size (n, %) | - | - | 0.003 |
| 1–13 mm | 33 (24.1) | 6 (8.2) | - |
| ≥14 mm | 104 (75.9) | 67 (91.8) | - |
| Location of lesion (n, %) | - | - | 0.276 |
| Upper one-third | 5 (3.6) | 5 (6.8) | - |
| Mid one-third | 27 (19.6) | 19 (26.0) | - |
| Lower one-third | 106 (76.8) | 49 (67.1) | - |
| WHO classification (n, %) | - | - | <0.001 |
| APD | 53 (38.4) | 50 (68.5) | - |
| SRC | 85 (61.6) | 23 (31.5) | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, H.J.; Kim, S.; Kim, J.-H.; Keum, J.-S.; Oh, S.-I.; Jo, J.; Chun, J.; Youn, Y.H.; Park, H.; Kwon, I.G.; et al. A Lesion-Based Convolutional Neural Network Improves Endoscopic Detection and Depth Prediction of Early Gastric Cancer. J. Clin. Med. 2019, 8, 1310. https://doi.org/10.3390/jcm8091310
Yoon HJ, Kim S, Kim J-H, Keum J-S, Oh S-I, Jo J, Chun J, Youn YH, Park H, Kwon IG, et al. A Lesion-Based Convolutional Neural Network Improves Endoscopic Detection and Depth Prediction of Early Gastric Cancer. Journal of Clinical Medicine. 2019; 8(9):1310. https://doi.org/10.3390/jcm8091310
Chicago/Turabian StyleYoon, Hong Jin, Seunghyup Kim, Jie-Hyun Kim, Ji-Soo Keum, Sang-Il Oh, Junik Jo, Jaeyoung Chun, Young Hoon Youn, Hyojin Park, In Gyu Kwon, and et al. 2019. "A Lesion-Based Convolutional Neural Network Improves Endoscopic Detection and Depth Prediction of Early Gastric Cancer" Journal of Clinical Medicine 8, no. 9: 1310. https://doi.org/10.3390/jcm8091310
APA StyleYoon, H. J., Kim, S., Kim, J.-H., Keum, J.-S., Oh, S.-I., Jo, J., Chun, J., Youn, Y. H., Park, H., Kwon, I. G., Choi, S. H., & Noh, S. H. (2019). A Lesion-Based Convolutional Neural Network Improves Endoscopic Detection and Depth Prediction of Early Gastric Cancer. Journal of Clinical Medicine, 8(9), 1310. https://doi.org/10.3390/jcm8091310