The Prognosis of Blunt Bowel and Mesenteric Injury—The Pitfall in the Contemporary Image Survey

Abstract
:1. Introduction
2. Experimental Section
2.1. Materials and Methods
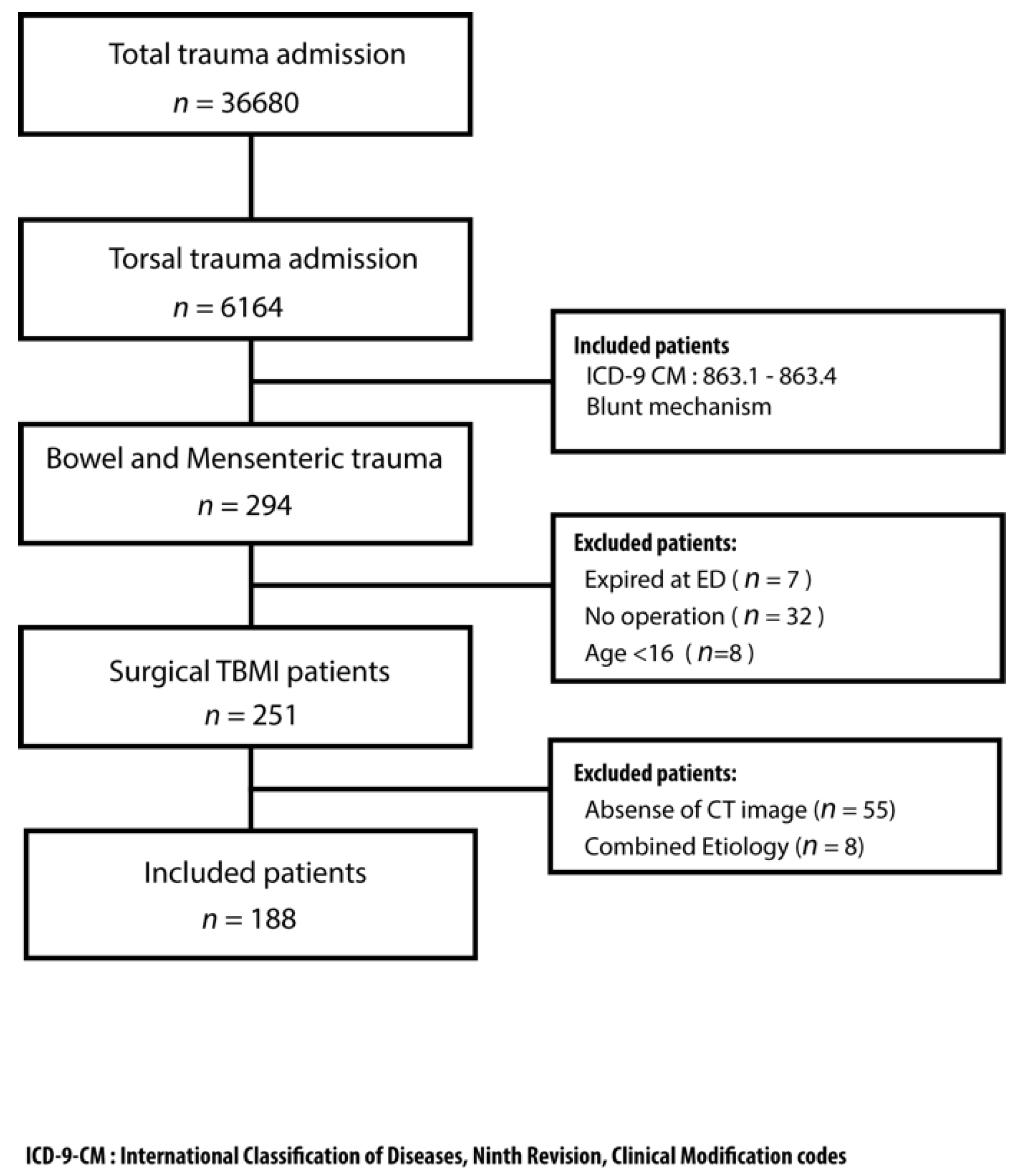
2.2. Study Population
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Fakhry, S.M.; Watts, D.D.; Luchette, F.A. EAST Multi-Institutional Hollow Viscus Injury Research Group Current diagnostic approaches lack sensitivity in the diagnosis of perforated blunt small bowel injury: Analysis from 275,557 trauma admissions from the EAST multi-institutional HVI trial. J. Trauma 2003, 54, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Butela, S.T.; Federle, M.P.; Chang, P.J.; Thaete, F.L.; Peterson, M.S.; Dorvault, C.J.; Hari, A.K.; Soni, S.; Branstetter, B.F.; Paisley, K.J.; et al. Performance of CT in detection of bowel injury. AJR Am. J. Roentgenol. 2001, 176, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Zingg, T.; Agri, F.; Bourgeat, M.; Yersin, B.; Romain, B.; Schmidt, S.; Keller, N.; Demartines, N. Avoiding delayed diagnosis of significant blunt bowel and mesenteric injuries: Can a scoring tool make the difference? A 7-year retrospective cohort study. Injury 2018, 49, 33–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bekker, W.; Kong, V.Y.; Laing, G.L.; Bruce, J.L.; Manchev, V.; Clarke, D.L. The spectrum and outcome of blunt trauma related enteric hollow visceral injury. Ann. R. Coll. Surg. Engl. 2018, 100, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Fakhry, S.M.; Brownstein, M.; Watts, D.D.; Baker, C.C.; Oller, D. Relatively short diagnostic delays (<8 hours) produce morbidity and mortality in blunt small bowel injury: An analysis of time to operative intervention in 198 patients from a multicenter experience. J. Trauma 2000, 48, 408–415. [Google Scholar] [PubMed]
- Malinoski, D.J.; Patel, M.S.; Yakar, D.O.; Green, D.; Qureshi, F.; Inaba, K.; Brown, C.V.R.; Salim, A. A diagnostic delay of 5 hours increases the risk of death after blunt hollow viscus injury. J. Trauma 2010, 69, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Petrosoniak, A.; Engels, P.T.; Hamilton, P.; Tien, H.C. Detection of significant bowel and mesenteric injuries in blunt abdominal trauma with 64-slice computed tomography. J. Trauma Acute Care Surg. 2013, 74, 1081–1086. [Google Scholar] [CrossRef] [PubMed]
- Drasin, T.E.; Anderson, S.W.; Asandra, A.; Rhea, J.T.; Soto, J.A. MDCT evaluation of blunt abdominal trauma: Clinical significance of free intraperitoneal fluid in males with absence of identifiable injury. Am. J. Roentgenol. 2008, 191, 1821–1826. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Fulcher, A.S.; Wang, D.B.; Turner, M.A.; Ha, J.D.; McCulloch, M.; Kennedy, R.M.; Malhotra, A.K.; Halvorsen, R.A. Frequency and importance of small amount of isolated pelvic free fluid detected with multidetector CT in male patients with blunt trauma. Radiology 2010, 256, 799–805. [Google Scholar] [CrossRef]
- Bates, D.D.B.; Wasserman, M.; Malek, A.; Gorantla, V.; Anderson, S.W.; Soto, J.A.; LeBedis, C.A. Multidetector CT of Surgically Proven Blunt Bowel and Mesenteric Injury. Radiographics 2017, 37, 613–625. [Google Scholar] [CrossRef] [Green Version]
- Morrison, J.E.; Wisner, D.H.; Bodai, B.I. Complications after negative laparotomy for trauma: Long-term follow-up in a health maintenance organization. J. Trauma 1996, 41, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Gonser-Hafertepen, L.N.; Davis, J.W.; Bilello, J.F.; Ballow, S.L.; Sue, L.P.; Cagle, K.M.; Venugopal, C.; Hafertepen, S.C.; Kaups, K.L. Isolated free fluid on abdominal computed tomography in blunt trauma: Watch and wait or operate? J. Am. Coll. Surg. 2014, 219, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Chereau, N.; Wagner, M.; Trésallet, C.; Lucidarme, O.; Raux, M.; Menegaux, F. CT scan and Diagnostic Peritoneal Lavage: Towards a better diagnosis in the area of nonoperative management of blunt abdominal trauma. Injury 2016, 47, 2006–2011. [Google Scholar] [CrossRef] [PubMed]
- Young, K.; Benson, M.; Higgins, A.; Dove, J.; Hunsinger, M.; Shabahang, M.; Blansfield, J.; Torres, D.; Widom, K.; Wild, J. In the Modern Era of CT, Do Blunt Trauma Patients with Markers for Blunt Bowel or Mesenteric Injury Still Require Exploratory Laparotomy? Am. Surg. 2017, 83, 722–727. [Google Scholar] [PubMed]
- Harmston, C.; Ward, J.B.M.; Patel, A. Clinical outcomes and effect of delayed intervention in patients with hollow viscus injury due to blunt abdominal trauma: A systematic review. Eur. J. Trauma Emerg. Surg. 2018, 44, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Atri, M.; Hanson, J.M.; Grinblat, L.; Brofman, N.; Chughtai, T.; Tomlinson, G. Surgically important bowel and/or mesenteric injury in blunt trauma: Accuracy of multidetector CT for evaluation. Radiology 2008, 249, 524–533. [Google Scholar] [CrossRef] [PubMed]
- Brody, J.M.; Leighton, D.B.; Murphy, B.L.; Abbott, G.F.; Vaccaro, J.P.; Jagminas, L.; Cioffi, W.G. CT of blunt trauma bowel and mesenteric injury: Typical findings and pitfalls in diagnosis. Radiographics 2000, 20, 1525–1536. [Google Scholar] [CrossRef] [PubMed]
- Molinelli, V.; Iosca, S.; Duka, E.; De Marchi, G.; Lucchina, N.; Bracchi, E.; Carcano, G.; Novario, R.; Fugazzola, C. Ability of specific and nonspecific signs of multidetector computed tomography (MDCT) in the diagnosis of blunt surgically important bowel and mesenteric injuries. Radiol. Med. 2018, 123, 891–903. [Google Scholar] [CrossRef] [PubMed]
- Livingston, D.H.; Lavery, R.F.; Passannante, M.R.; Skurnick, J.H.; Fabian, T.C.; Fry, D.E.; Malangoni, M.A. Admission or observation is not necessary after a negative abdominal computed tomographic scan in patients with suspected blunt abdominal trauma: Results of a prospective, multi-institutional trial. J. Trauma 1998, 44, 273–282. [Google Scholar] [CrossRef] [PubMed]
- McNutt, M.K.; Chinapuvvula, N.R.; Beckmann, N.M.; Camp, E.A.; Pommerening, M.J.; Laney, R.W.; West, O.C.; Gill, B.S.; Kozar, R.A.; Cotton, B.A.; et al. Early surgical intervention for blunt bowel injury. J. Trauma Acute Care Surg. 2015, 78, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Sharma, O.P.; Oswanski, M.F.; Singer, D.; Kenney, B. The role of computed tomography in diagnosis of blunt intestinal and mesenteric trauma (BIMT). J. Emerg. Med. 2004, 27, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Lannes, F.; Scemama, U.; Maignan, A.; Boyer, L.; Beyer-Berjot, L.; Berdah, S.V.; Chaumoître, K.; Leone, M.; Bège, T. Value of early repeated abdominal CT in selective non-operative management for blunt bowel and mesenteric injury. Eur. Radiol. 2019, 54, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Romano, S.; Scaglione, M.; Tortora, G.; Martino, A.; Di Pietto, F.; Romano, L.; Grassi, R. MDCT in blunt intestinal trauma. Eur. J. Radiol. 2006, 59, 359–366. [Google Scholar] [CrossRef] [PubMed]
- LeBedis, C.A.; Anderson, S.W.; Bates, D.D.B.; Khalil, R.; Matherly, D.; Wing, H.; Burke, P.A.; Soto, J.A. CT imaging signs of surgically proven bowel trauma. Emerg. Radiol. 2016, 23, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Joseph, D.K.; Kunac, A.; Kinler, R.L.; Staff, I.; Butler, K.L. Diagnosing blunt hollow viscus injury: Is computed tomography the answer? Am. J. Surg. 2013, 205, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, A.K.; Fabian, T.C.; Katsis, S.B.; Gavant, M.L.; Croce, M.A. Blunt bowel and mesenteric injuries: The role of screening computed tomography. J. Trauma 2000, 48, 991–1000. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | |
|---|---|
| Total Numbers | 188 |
| Age (Mean ± SD) | 45.3 ± 18.3 |
| Male Gender (n, %) | 146 (77.7%) |
| ISS (Mean ± SD) | 17.2 ± 11.2 |
| RTS (Mean ± SD) | 7.078 ± 1.394 |
| TRISS (Mean ± SD) | 0.871 ± 0.240 |
| CT Characters | |
| Bowel Wall Discontinuity (n, %) | 5 (2.7%) |
| Extraluminal Air (n, %) | 82 (43.6%) |
| Bowel Wall Thickening (n, %) | 43 (22.9%) |
| Abnormal Bowel Wall Enhancement (n, %) | 23 (12.2 %) |
| Mesenteric Extravasation (n, %) | 27 (14.4%) |
| Mesenteric Vascular Bleeding (n, %) | 4 (2.1%) |
| Mesenteric Infiltration (n, %) | 44 (23.4%) |
| Mesenteric Pseudoaneurysm (n, %) | 23 (12.2%) |
| Intraperitoneal and Retroperitoneal Free Fluid (n, %) | 134 (71.3%) |
| Abdominal Wall Injury (n, %) | 14 (7.4%) |
| Surgical timing | |
| Early Operation, <24 h (n, %) | 161 (85.6%) |
| Deferred Operation, >24 h (n, %) | 27 (14.4%) |
| Surgical finding | |
| Mesenteric Injury | 58 (30.9%) |
| Bowel Injury | 125 (66.5%) |
| Combined Injury | 5 (2.6%) |
| ICULOS (days, Mean ± SD) | 6.5 ± 8.5 |
| HLOS (days, Mean ± SD) | 17.3 ± 15.6 |
| Mortality (n, %) | 21 (11.2%) |
| Characteristics | Early Diagnosis n = 161 | Deferred Diagnosis n = 27 | p Value |
|---|---|---|---|
| Age | 26.1 ± 17.4 | 40.4 ± 22.5 | 0.224 |
| ISS | 17.2 ± 11.2 | 17.6 ± 10.5 | 0.718 |
| AIS abdomen | 2.9 ± 0.7 | 3.0 ± 0.6 | 0.437 |
| RTS | 7.03 ± 1.46 | 7.35 ± 0.89 | 0.129 |
| TRISS | 0.86 ± 0.25 | 0.92 ± 0.17 | 0.289 |
| Bowel Wall Discontinuity | 4 (2.5%) | 1 (3.7%) | 0.569 |
| Extraluminal Air | 70 (43.5%) | 12 (44.4%) | 0.466 |
| Bowel Wall Thickening | 36 (22.4%) | 7 (25.9%) | 0.535 |
| Abnormal Bowel Wall Enhancement | 22 (13.7%) | 1 (0.5%) | 0.072 |
| Mesenteric Extravasation | 27 (16.8%) | 0 (0%) | 0.008 * |
| Mesenteric Vascular Bleeding | 3 (1.9%) | 1 (3.7%) | 0.489 |
| Mesenteric Infiltration | 40 (24.8%) | 4 (14.8%) | 0.142 |
| Mesenteric Pseudoaneurysm | 23 (14.3%) | 0 (0%) | 0.017 * |
| Intraperitoneal and Retroperitoneal Fluid | 116 (72.0%) | 18 (66.7%) | 0.453 |
| Abdominal Wall Injury | 11 (6.8%) | 3 (11.1%) | 0.366 |
| TAE | 5 (3.1%) | 4 (14.8%) | 0.026 * |
| Mesentery Injury | 53 (32.9%) | 5 (18.5%) | 0.133 |
| Bowel Injury | 103 (64.0%) | 22 (81.5%) | 0.075 |
| Combined Injury | 5 (3.1%) | 0 (0%) | |
| Necessity for 2nd Operation | 88 (54.7%) | 15 (55.6%) | 1.000 |
| Bowel Resection | 42 (26.1%) | 8 (29.6%) | 0.814 |
| Stoma Creation | 4 (2.5%) | 2 (7.4%) | 0.207 |
| Intrabdominal Infection | 17 (10.6%) | 7 (25.9%) | 0.054 |
| ICU LOS | 6.37 ± 8.4 | 7.04 ± 8.8 | 0.718 |
| HLOS | 17.1 ± 15.4 | 18.3 ± 16.6 | 0.724 |
| Mortality | 18/161 (11.2%) | 3/27 (11.1%) | 1.000 |
| Characteristics | Survival n = 167 | Deceased n = 21 | p Value |
|---|---|---|---|
| Age | 44.38 ± 17.59 | 53.33 ± 21.13 | 0.060 |
| ISS | 15.65 ± 10.43 | 29.33 ± 10.07 | <0.001 * |
| RTS | 7.29 ± 1.10 | 5.43 ± 2.24 | 0.001 * |
| TRISS | 0.91 ± 1.86 | 0.56 ± 0.37 | <0.001 * |
| AIS abdomen | 2.90 ± 0.65 | 3.29 ± 0.90 | 0.069 |
| Bowel Wall Discontinuity | 5 (3.0%) | 0 (0%) | 1.000 |
| Extraluminal Air | 75 (44.9%) | 7 (33.3%) | 0.358 |
| Bowel Wall Thickening | 38 (22.8%) | 5 (23.8%) | 1.000 |
| Abnormal Bowel Wall Enhancement | 1 (4.8%) | 2 (13.2%) | 0.479 |
| Mesenteric Extravasation | 23 (13.8%) | 4 (19.0%) | 0.512 |
| Mesenteric Vascular Bleeding | 3 (1.8%) | 1 (4.8%) | 0.380 |
| Mesenteric Infiltration | 37 (22.2%) | 7 (33.3%) | 0.277 |
| Mesenteric Pseudoaneurysm | 19 (11.4%) | 4 (19.0%) | 0.297 |
| Intraperitoneal and Retroperitoneal Fluid | 119 (71.3%) | 15 (71.4%) | 1.000 |
| Abdominal Wall Injury | 11 (6.6%) | 3 (14.3%) | 0.194 |
| Transcatheter Arterial Embolization | 6 (3.6%) | 3 (14.3%) | 0.065 |
| Early Operation | 143 (85.6%) | 18 (85.7%) | 1.000 |
| Intraabdominal Infection | 19 (11.4%) | 5 (23.8%) | 0.155 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, C.-H.; Hsieh, F.-J.; Chen, C.-C.; Cheng, C.-T.; Ooyang, C.-H.; Hsieh, C.-H.; Yang, S.-J.; Fu, C.-Y. The Prognosis of Blunt Bowel and Mesenteric Injury—The Pitfall in the Contemporary Image Survey. J. Clin. Med. 2019, 8, 1300. https://doi.org/10.3390/jcm8091300
Liao C-H, Hsieh F-J, Chen C-C, Cheng C-T, Ooyang C-H, Hsieh C-H, Yang S-J, Fu C-Y. The Prognosis of Blunt Bowel and Mesenteric Injury—The Pitfall in the Contemporary Image Survey. Journal of Clinical Medicine. 2019; 8(9):1300. https://doi.org/10.3390/jcm8091300
Chicago/Turabian StyleLiao, Chien-Hung, Feng-Jen Hsieh, Chih-Chi Chen, Chi-Tung Cheng, Chun-Hsiang Ooyang, Chi-Hsun Hsieh, Shang-Ju Yang, and Chih-Yuan Fu. 2019. "The Prognosis of Blunt Bowel and Mesenteric Injury—The Pitfall in the Contemporary Image Survey" Journal of Clinical Medicine 8, no. 9: 1300. https://doi.org/10.3390/jcm8091300