Evaluation of the Intraoperative Perfusion Index for Correlation with Acute Postoperative Pain in Patients Undergoing Laparoscopic Colorectal Cancer Surgery

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Intervention
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Argoff, C.E. Recent management advances in acute postoperative pain. Pain Pract. 2014, 14, 477–487. [Google Scholar] [CrossRef] [PubMed]
- Buvanendran, A.; Fiala, J.; Patel, K.A.; Golden, A.D.; Moric, M.; Kroin, J.S. The Incidence and Severity of Postoperative Pain following Inpatient Surgery. Pain Med. 2015, 16, 2277–2283. [Google Scholar] [CrossRef] [PubMed]
- Pogatzki-Zahn, E.M.; Segelcke, D.; Schug, S.A. Postoperative pain-from mechanisms to treatment. Pain Rep. 2017, 2, e588. [Google Scholar] [CrossRef] [PubMed]
- Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology 2012, 116, 248–273. [CrossRef] [PubMed]
- Thapa, P.; Euasobhon, P. Chronic postsurgical pain: current evidence for prevention and management. Korean J. Pain 2018, 31, 155–173. [Google Scholar] [CrossRef] [PubMed]
- Lavand’Homme, P. The progression from acute to chronic pain. Curr. Opin. Anaesthesiol. 2011, 24, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Loeser, J.D.; Treede, R.D. The Kyoto protocol of IASP Basic Pain Terminology. Pain 2008, 137, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Korhonen, I.; Yli-Hankala, A. Photoplethysmography and nociception. Acta. Anaesthesiol. Scand. 2009, 53, 975–985. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Sun, K.; Zhu, Z.; Zhou, C.; Wu, Y.; Zhang, F.; Yan, M. Oximetry-derived perfusion index as an early indicator of CT-guided thoracic sympathetic blockade in palmar hyperhidrosis. Clin. Radiol. 2013, 68, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Tapar, H.; Suren, M.; Karaman, S.; Dogru, S.; Karaman, T.; Sahin, A.; Altıparmak, F. Evaluation of the perfusion index according to the visual analog scale in postoperative patients. Saudi Med. J. 2018, 39, 1006–1010. [Google Scholar] [CrossRef]
- Lee, J.Y.; Kim, H.C.; Huh, J.W.; Sim, W.S.; Lim, H.Y.; Lee, E.K.; Park, H.G.; Bang, Y.J. Incidence and risk factors for rectal pain after laparoscopic rectal cancer surgery. J. Int. Med. Res. 2017, 45, 781–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hjermstad, M.J.; Fayers, P.M.; Haugen, D.F.; Caraceni, A.; Hanks, G.W.; Loge, J.H.; Fainsinger, R.; Aass, N.; Kaasa, S. Studies Comparing Numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for Assessment of Pain Intensity in Adults: A Systematic Literature Review. J. Pain Symptom Manage. 2011, 41, 1073–1093. [Google Scholar] [CrossRef] [PubMed]
- Lovich-Sapola, J.; Smith, C.E.; Brandt, C.P. Postoperative pain control. Surg. Clin. North Am. 2015, 95, 301–318. [Google Scholar] [CrossRef] [PubMed]
- Rawal, N. Current issues in postoperative pain management. Eur. J. Anaesthesiol. 2016, 33, 160–171. [Google Scholar] [CrossRef] [PubMed]
- Meijer, F.S.; Martini, C.H.; Broens, S.; Boon, M.; Niesters, M.; Aarts, L.; Olofsen, E.; van Velzen, M.; Dahan, A. Nociception-guided versus Standard Care during Remifentanil-Propofol Anesthesia: A Randomized Controlled Trial. Anesthesiology 2019, 130, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Ledowski, T. Objective monitoring of nociception: a review of current commercial solutions. Br. J. Anaesth. 2019, 123, e312–e321. [Google Scholar] [CrossRef] [PubMed]
- Julien-Marsollier, F.; Rachdi, K.; Caballero, M.J.; Ayanmanesh, F.; Vacher, T.; Hörlin, A.L.; Skhiri, A.; Brasher, C.; Michelet, D.; Dahmani, S. Evaluation of the analgesia nociception index for monitoring intraoperative analgesia in children. Br. J. Anaesth. 2018, 121, 462–468. [Google Scholar] [CrossRef] [Green Version]
- Mowafi, H.A.; Ismail, S.A.; Shafi, M.A.; Al-Ghamdi, A.A. The Efficacy of Perfusion Index as an Indicator for Intravascular Injection of Epinephrine-Containing Epidural Test Dose in Propofol-Anesthetized Adults. Anesth. Analg. 2009, 108, 549–553. [Google Scholar] [CrossRef]
- Ovadia-Blechman, Z.; Meilin, A.; Rabin, N.; Eldar, M.; Castel, D. Noninvasive monitoring of peripheral microcirculatory hemodynamics under varying degrees of hypoxia. Respir. Physiol. Neurobiol. 2015, 216, 23–27. [Google Scholar] [CrossRef]
- Ginosar, Y.; Weiniger, C.F.; Meroz, Y.; Kurz, V.; Bdolah-Abram, T.; Babchenko, A.; Nitzan, M.; Davidson, E.M. Pulse oximeter perfusion index as an early indicator of sympathectomy after epidural anesthesia. Acta Anaesthesiol. Scand. 2009, 53, 1018–1026. [Google Scholar] [CrossRef]
- Chu, C.L.; Huang, Y.Y.; Chen, Y.H.; Lai, L.P.; Yeh, H.M. An observational study: The utility of perfusion index as a discharge criterion for pain assessment in the postanesthesia care unit. PLOS ONE 2018, 13, e0197630. [Google Scholar] [CrossRef]
- Chung, K.; Kim, K.H.; Kim, E.D. Perfusion index as a reliable parameter of vasomotor disturbance in complex regional pain syndrome. Br. J. Anaesth. 2018, 121, 1133–1137. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Kim, E.D.; Na Kim, Y.; Kim, J.S.; Sim, W.S.; Lee, H.J.; Park, H.J.; Park, H.J. Correlation of Perfusion Index Change and Analgesic Efficacy in Transforaminal Block for Lumbosacral Radicular Pain. J. Clin. Med. 2019, 8, 51. [Google Scholar] [CrossRef]
- Şahin, Ö.F.; Kılıç, E.T.; Aksoy, Y.; Kaydu, A.; Gökçek, E. The importance of perfusion index monitoring in evaluating the efficacy of stellate ganglion blockage treatment in Raynaud’s disease. Libyan J. Med. 2018, 13, 1422666. [Google Scholar] [CrossRef]
- Abdelnasser, A.; Abdelhamid, B.; Elsonbaty, A.; Hasanin, A.; Rady, A. Predicting successful supraclavicular brachial plexus block using pulse oximeter perfusion index. Br. J. Anaesth. 2017, 119, 276–280. [Google Scholar] [CrossRef] [Green Version]
- Galvin, E.M.; Niehof, S.; Verbrugge, S.J.; Maissan, I.; Jahn, A.; Klein, J.; Van Bommel, J. Peripheral Flow Index Is a Reliable and Early Indicator of Regional Block Success. Anesth. Analg. 2006, 103, 239–243. [Google Scholar] [CrossRef]
- Hasanin, A.; Mohamed, S.A.R.; El-Adawy, A. Evaluation of perfusion index as a tool for pain assessment in critically ill patients. J. Clin. Monit. Comput. 2017, 31, 961–965. [Google Scholar] [CrossRef]
- Touj, S.; Houle, S.; Ramla, D.; Jeffrey-Gauthier, R.; Hotta, H.; Bronchti, G.; Martinoli, M.G.; Piché, M. Sympathetic regulation and anterior cingulate cortex volume are altered in a rat model of chronic back pain. Neurosci. 2017, 352, 9–18. [Google Scholar] [CrossRef]
- Wu, C.L.; Raja, S.N. Treatment of acute postoperative pain. Lancet 2011, 377, 2215–2225. [Google Scholar] [CrossRef]
- Saxena, A.K.; Chilkoti, G.T.; Chopra, A.K.; Banerjee, B.D.; Sharma, T. Chronic persistent post-surgical pain following staging laparotomy for carcinoma of ovary and its relationship to signal transduction genes. Korean J. Pain 2016, 29, 239–248. [Google Scholar] [CrossRef]
- Lee, M.G.; Kim, H.J.; Lee, K.H.; Choi, Y.S. The influence of genotype polymorphism on morphine analgesic effect for postoperative pain in children. Korean J. Pain 2016, 29, 34–39. [Google Scholar] [CrossRef]


{kind=link}
| All Patients (n = 98) | Group N (n = 50) | Group P (n = 48) | p-Value | |
|---|---|---|---|---|
| Age (years) | 62.9 ± 12.8 | 65.3 ± 13.2 | 60.5 ± 11.9 | 0.064 |
| Sex (Male/Female) | 50/48 | 25/25 | 25/23 | 0.997 |
| Body mass index (kg/m2) | 24.0 ± 3.2 | 23.8 ± 3.2 | 24.3 ± 3.1 | 0.436 |
| ASA status: I/II/III | 39/52/7 | 19/27/4 | 20/25/3 | 0.952 |
| Diagnosis | 0.098 | |||
| Colon cancer | 69 (70.4%) | 32 (64.0%) | 37 (77.1%) | |
| Rectal cancer | 29 (29.6%) | 18 (36.0%) | 11 (22.9%) | |
| Presence of DM | 16 (16.3%) | 8 (16.0%) | 8 (16.7%) | 1.000 |
| Preoperative CRT | 10 (10.2%) | 3 (6.0%) | 7 (14.6%) | 0.195 |
| Surgery type | ||||
| Colectomy | 54 (55.1%) | 27 (54.0%) | 27 (56.3%) | 0.599 |
| Low anterior resection | 44 (44.9%) | 23 (46.0%) | 21 (43.7%) | |
| Pathological stage | ||||
| I | 26 (26.5%) | 14 (28.0%) | 12 (25.0%) | 0.673 |
| II | 19 (19.4%) | 7 (14.0%) | 12 (25.0%) | |
| III | 11 (11.2%) | 6 (12.0%) | 5 (10.4%) | |
| IV | 42 (42.9%) | 23 (46.0%) | 19 (39.6%) | |
| Mean tumor size > 4 cm | 57 (58.2%) | 26 (52.0%) | 31 (64.6%) | 0.290 |
| Operation time (min) | 144.4 ± 58.4 | 137.7 ± 43.8 | 151.3 ± 70.3 | 0.259 |
| Anesthesia time (min) | 190.7 ± 60.2 | 185.3 ± 45.1 | 196.3 ± 72.8 | 0.374 |
| Intraoperative fentanyl (µg) | 59.3 ± 23.9 | 54.4 ± 22.8 | 64.3 ± 24.7 * | 0.039 |
| Preoperative pain (VAS) | 0.1 ± 0.6 | 0.0 ± 0.4 | 0.2 ± 0.7 | 0.379 |
| Postoperative pain at PACU | ||||
| Admission | 6.4 ± 1.8 | 4.9 ± 1.2 | 7.8 ± 1.0 * | <0.001 |
| Discharge | 2.9 ± 0.8 | 2.7 ± 0.6 | 3.0 ± 0.9 * | 0.026 |
| Rescue fentanyl at PACU (µg) | 53.8 ± 31.2 | 42.6 ± 26.7 | 65.5 ± 31.4 * | <0.001 |
| Group N (n = 50) | Group P (n = 48) | p-Value | |
|---|---|---|---|
| PI change ratio | |||
| T2 | 0.98 ± 1.7 | 1.02 ± 1.8 | 0.909 |
| T3 | 0.00 ± 1.0 | −0.12 ± 1.3 | 0.635 |
| T4 | −0.36 ± 0.62 | −0.40 ± 0.5 | 0.729 |
| BIS change ratio | |||
| T2 | −0.60 ± 0.1 | −0.55 ± 0.2 | 0.123 |
| T3 | −0.43 ± 0.1 | −0.36 ± 0.3 | 0.181 |
| T4 | −0.13 ± 0.1 | −0.13 ± 0.1 | 0.786 |
| Parameter | Estimate | SE | 95% Confidence Limits | p-Value | |
|---|---|---|---|---|---|
| PI values | |||||
| Intercept | 5.1413 | 0.4850 | 4.1906 | 6.0919 | <0.0001 |
| Time | −0.8938 | 0.1457 | −1.1793 | −0.6082 | <0.0001 |
| Group | 0.5059 | 0.8001 | −1.0623 | 2.0741 | 0.5272 |
| Time, group | −0.0544 | 0.2184 | −0.4824 | 0.3737 | 0.8034 |
| BIS values | |||||
| Intercept | 70.7969 | 1.4266 | 68.0009 | 73.5929 | <0.0001 |
| Time | −1.3688 | 0.6316 | −2.6066 | −0.1309 | 0.0302 |
| Group | 0.4888 | 2.0224 | −3.4750 | 4.4527 | 0.8090 |
| Time, group | −1.1491 | 0.9412 | −2.9938 | 0.6956 | 0.2221 |
| Group N (n = 50) | Group P (n = 48) | |
|---|---|---|
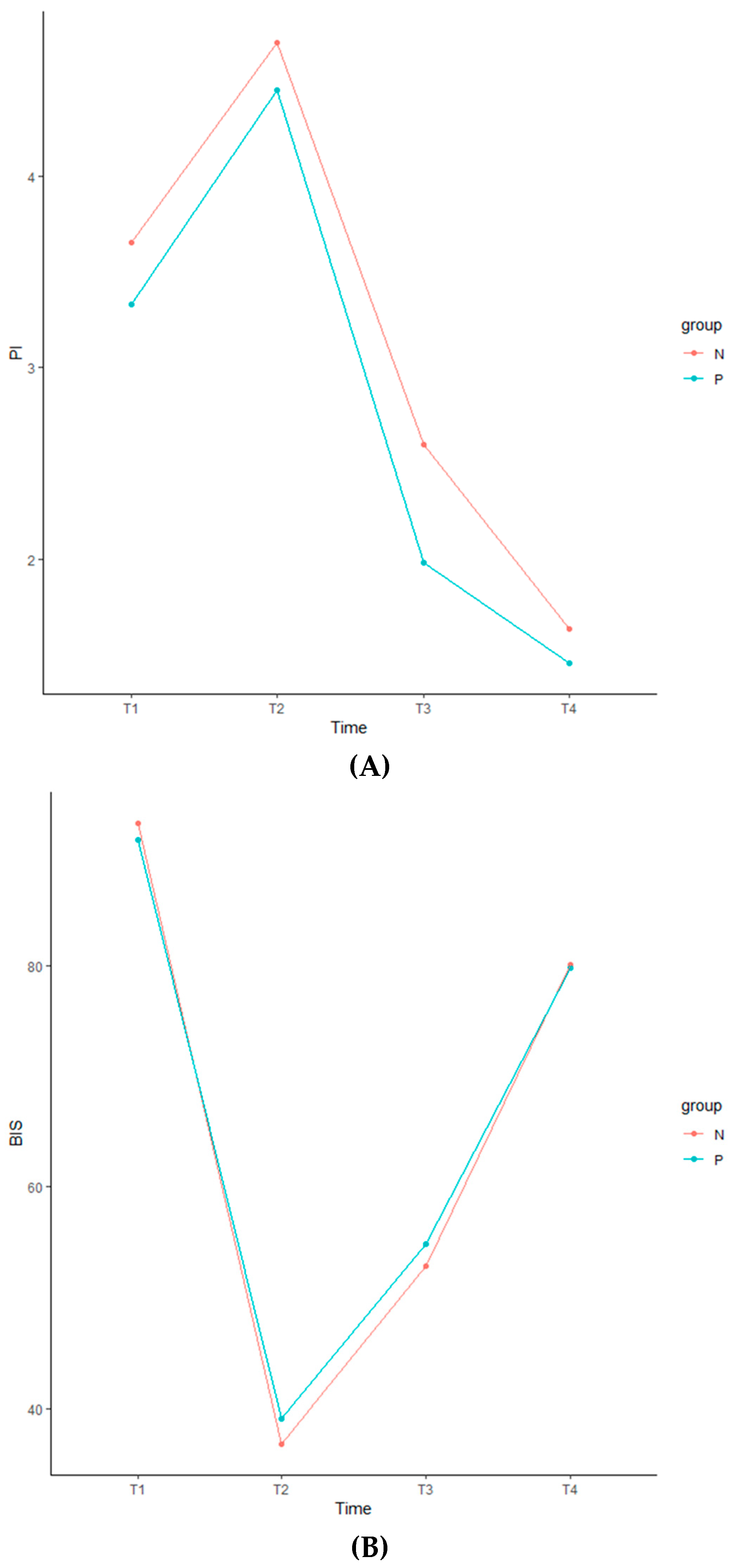
| PI values | ||
| T1 | 3.65 ± 2.7 | 3.33 ± 2.3 |
| T2 | 4.69 ± 2.3 | 4.45 ± 2.1 |
| T3 | 2.60 ± 2.1 | 1.98 ± 1.8 |
| T4 | 1.64 ± 1.3 | 1.46 ± 1.1 |
| BIS values | ||
| T1 | 92.84 ± 5.1 | 91.29 ± 11.9 |
| T2 | 36.78 ± 8.5 | 39.04 ± 10.4 |
| T3 | 52.84 ± 10.6 | 54.79 ± 10.9 |
| T4 | 80.04 ± 9.5 | 79.73 ± 13.4 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, J.H.; Park, H.J.; Sim, W.S.; Park, J.H.; Jung, K.H.; Oh, M.S.; Seon, H.J.; Lee, J.Y. Evaluation of the Intraoperative Perfusion Index for Correlation with Acute Postoperative Pain in Patients Undergoing Laparoscopic Colorectal Cancer Surgery. J. Clin. Med. 2019, 8, 1299. https://doi.org/10.3390/jcm8091299
Kwon JH, Park HJ, Sim WS, Park JH, Jung KH, Oh MS, Seon HJ, Lee JY. Evaluation of the Intraoperative Perfusion Index for Correlation with Acute Postoperative Pain in Patients Undergoing Laparoscopic Colorectal Cancer Surgery. Journal of Clinical Medicine. 2019; 8(9):1299. https://doi.org/10.3390/jcm8091299
Chicago/Turabian StyleKwon, Ji Hye, Hue Jung Park, Woo Seog Sim, Joo Hyun Park, Kang Ha Jung, Min Seok Oh, Heui Jin Seon, and Jin Young Lee. 2019. "Evaluation of the Intraoperative Perfusion Index for Correlation with Acute Postoperative Pain in Patients Undergoing Laparoscopic Colorectal Cancer Surgery" Journal of Clinical Medicine 8, no. 9: 1299. https://doi.org/10.3390/jcm8091299