Motor and Postural Patterns Concomitant with General Movements Are Associated with Cerebral Palsy at Term and Fidgety Age in Preterm Infants

 and
and
Abstract
:1. Introduction
- (a)
- Which type of GM trajectories were associated with cerebral palsy in preterm infants?
- (b)
- Which concomitant motor and postural patterns, with or without GMs, were associated with cerebral palsy at three key ages (preterm, term, and fidgety age)?
- (c)
- Which concomitant motor and postural patterns were longitudinally considered to increase the association of GMs to cerebral palsy?
2. Methods
2.1. Study Design
2.2. Video Recordings
2.3. Evaluation of Spontaneous Motor Repertoire
2.4. Statistical Methods
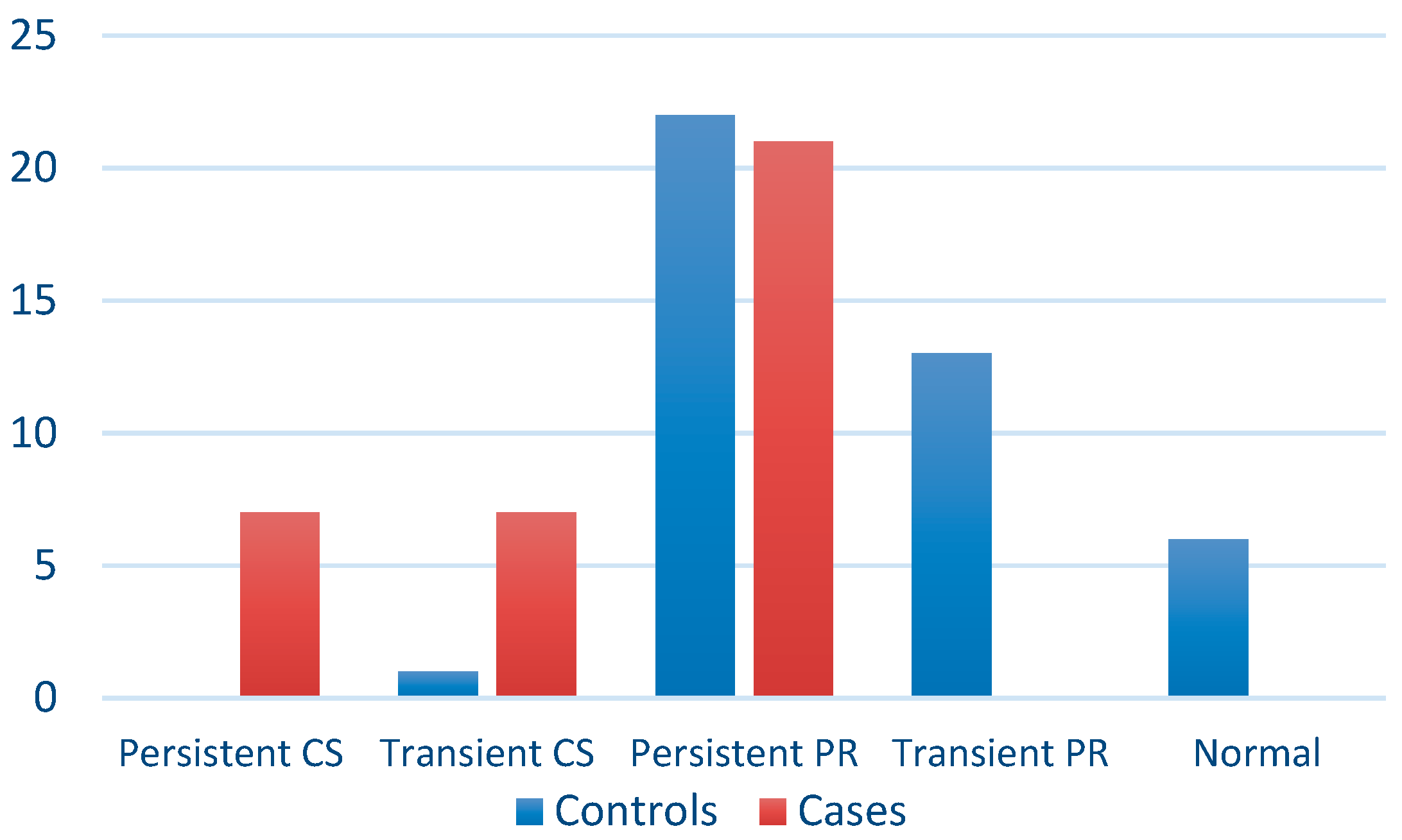
- Normal trajectory, when normal GMs were present at both preterm and term age (N-N);
- Transient poor repertoire trajectory, when poor repertoire GMs were present at either preterm or term age (PR-N or N-PR);
- Persistent poor repertoire trajectory, when poor repertoire was present at both preterm and term age (PR-PR);
- Transient cramped-synchronized trajectory, when cramped-synchronized was present at either preterm or term age (CS-PR or PR-CS);
- Persistent cramped-synchronized trajectory, when cramped-synchronized was present at both preterm and term age (CS-CS).
- N-N, F+
- PR-N, F+ or N-PR, F+
- PR-N, F− or N-PR, F−
- PR-PR, F+
- PR-PR, F−
- CS-PR, F+ or PR-CS, F+
- CS-PR, F− or PR-CS, F−
- CS-CS, F−
3. Results
3.1. GM Trajectories Associated with Cerebral Palsy in Preterm Infants
3.2. Concomitant Motor and Postural Patterns Associated with Cerebral Palsy Regardless of GMs in Preterm Infants
- (a)
- At preterm age, only two patterns were associated with cerebral palsy: open hand posture and absence of signs pointing to loss of balance.
- (b)
- At term age, the following seven patterns were associated with cerebral palsy: tremors, movements towards midline in upper limbs (few or absent), movements towards midline in lower limbs (absent), open hand posture, monotonous/stereotyped limbs movements, head posture on a side, and pathological head movements.
- (c)
- At fidgety age, all concomitant motor and postural patterns were associated with cerebral palsy.
3.3. Concomitant Motor and Postural Patterns That, along with GMs, were Associated with Cerebral Palsy at the Three Key Ages
3.4. Concomitant Motor and Postural Pattern Trajectories Associated with Cerebral Palsy
4. Discussion
Limitations
5. Conclusions
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Age | Model | −2 Log-Likelihood | ΔLL | Degrees of Freedom | Δdf | p |
|---|---|---|---|---|---|---|
| Preterm age | GMs | 82.577 | - | 2 | - | <0.001 |
| GMs + LB | 76.245 | 6.332 | 3 | 1 | 0.012 | |
| GMs + T | 82.102 | 0.474 | 3 | 1 | 0.491 | |
| GMs + MTM-UL | 79.827 | 2.749 | 3 | 1 | 0.097 | |
| GMs + MTM-LL | 82.216 | 0.361 | 3 | 1 | 0.548 | |
| GMs + OHP | 74.523 | 8.054 | 3 | 1 | 0.005 | |
| GMs + FS | 79.720 | 2.857 | 3 | 1 | 0.091 | |
| GMs + MSLM | 80.562 | 2.015 | 3 | 1 | 0.156 | |
| GMs + ATN | 81.437 | 1.140 | 3 | 1 | 0.286 | |
| GMs + HPS | 80.216 | 2.361 | 3 | 1 | 0.124 | |
| GMs + PHM | 82.556 | 0.021 | 3 | 1 | 0.885 | |
| GMs + ASY | 82.556 | 0.021 | 3 | 1 | 0.885 | |
| Term age | GMs | 78.878 | - | 2 | - | <0.001 |
| GMs + LB | 76.318 | 2.005 | 3 | 1 | 0.157 | |
| GMs + T | 73.680 | 4.642 | 3 | 1 | 0.031 | |
| GMs + MTM-UL | 73.027 | 5.295 | 4 | 1 | 0.071 | |
| GMs + MTM-LL | 73.681 | 4.642 | 4 | 1 | 0.098 | |
| GMs + OHP | 66.528 | 11.794 | 3 | 1 | 0.001 | |
| GMs + FS | 76.732 | 1.590 | 3 | 1 | 0.207 | |
| GMs + MSLM | 63.337 | 14.985 | 3 | 1 | <0.001 | |
| GMs + ATN | 75.938 | 2.384 | 3 | 1 | 0.123 | |
| GMs + HPS | 77.795 | 0.527 | 3 | 1 | 0.468 | |
| GMs + PHM | 76.668 | 1.654 | 3 | 1 | 0.198 | |
| GMs + ASY | 77.956 | 0.366 | 3 | 1 | 0.545 | |
| Fidgety age | GMs | 59.968 | - | 1 | - | <0.001 |
| GMs + LB | 49.048 | 10.920 | 2 | 1 | 0.001 | |
| GMs + T | 55.225 | 4.743 | 2 | 1 | 0.029 | |
| GMs + MTM-UL | 52.257 | 7.712 | 4 | 1 | 0.052 | |
| GMs + MTM-LL | 45.225 | 14.743 | 4 | 1 | 0.002 | |
| GMs + OHP | 58.950 | 1.018 | 2 | 1 | 0.313 | |
| GMs + FS | 53.952 | 6.016 | 2 | 1 | 0.014 | |
| GMs + MSLM | 34.729 | 25.239 | 2 | 1 | <0.001 | |
| GMs + ATN | 51.601 | 8.367 | 2 | 1 | 0.004 | |
| GMs + HPS | 58.945 | 1.024 | 2 | 1 | 0.312 | |
| GMs + PHM | 57.004 | 2.964 | 2 | 1 | 0.085 | |
| GMs + ASY | 53.578 | 6.390 | 2 | 1 | 0.011 |
| Age | Model | −2 Log-Likelihood | ΔLL | Degrees of Freedom | Δdf | p |
|---|---|---|---|---|---|---|
| Preterm age | GMs | 82.577 | - | 1 | - | <0.001 |
| GMs + OHP | 74.523 | 8.054 | 2 | 1 | 0.005 | |
| GMs + LB + OHP | 68.626 | 5.897 | 3 | 1 | 0.015 | |
| Term age | GMs | 81.066 | - | 1 | - | <0.001 |
| GMs + MSLM | 66.049 | 15.017 | 2 | 1 | <0.001 | |
| GMs + MSLM + OHP | 54.566 | 11.483 | 3 | 1 | 0.001 | |
| Fidgety age | GMs | 48.715 | - | 1 | - | <0.001 |
| GMs + MSLM | 34.729 | 13.986 | 2 | 1 | <0.001 |
References
- McIntyre, S. The continually changing epidemiology of cerebral palsy. Acta Paediatr. 2018, 107, 374–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novak, I.; Morgan, C.; Adde, L.; Blackman, J.; Boyd, R.N.; Brunstrom-Hernandez, J.; Cioni, G.; Damiano, D.; Darrah, J.; Eliasson, A.-C.; et al. Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment. JAMA Pediatr. 2017, 171, 897–907. [Google Scholar] [CrossRef] [PubMed]
- Dargassies, S.S.-A. Neurodevelopmental Symptoms during the First Year of Life. Dev. Med. Child Neurol. 1972, 14, 235–246. [Google Scholar] [CrossRef] [PubMed]
- Yuge, M.; Marschik, P.B.; Nakajima, Y.; Yamori, Y.; Kanda, T.; Hirota, H.; Yoshida, N.; Einspieler, C. Movements and postures of infants aged 3 to 5 months: To what extent is their optimality related to perinatal events and to the neurological outcome? Early Hum. Dev. 2011, 87, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Cioni, G.; Ferrari, F.; Prechtl, H.F.R. Posture and spontaneous motility in fullterm infants. Early Hum. Dev. 1989, 18, 247–262. [Google Scholar] [CrossRef]
- Prechtl, H.F.R. Qualitative changes of spontaneous movements in fetus and preterm infant are a marker of neurological dysfunction. Early Hum. Dev. 1990, 23, 151–158. [Google Scholar] [CrossRef]
- Ferrari, F.; Cioni, G.; Prechtl, H.F.R. Qualitative changes of general movements in preterm infants with brain lesions. Early Hum. Dev. 1990, 23, 193–231. [Google Scholar] [CrossRef]
- Prechtl, H.F.; Einspieler, C.; Cioni, G.; Bos, A.F.; Ferrari, F.; Sontheimer, D. An early marker for neurological deficits after perinatal brain lesions. Lancet 1997, 349, 1361–1363. [Google Scholar] [CrossRef]
- Einspieler, C.; Prechtl, H.F.R. Prechtl’s assessment of general movements: A diagnostic tool for the functional assessment of the young nervous system. Ment. Retard. Dev. Disabil. Res. Rev. 2005, 11, 61–67. [Google Scholar] [CrossRef]
- Einspieler, C.; Prechtl, H.R.F.; Bos, A.; Ferrari, F.; Cioni, G. Prechtl’s Method on the Qualitative Assessment of General Movements in Preterm, Term and Young Infants; Wiley: New York, NY, USA, 2008; ISBN 978-1-898683-62-9. [Google Scholar]
- Bosanquet, M.; Copeland, L.; Ware, R.; Boyd, R. A systematic review of tests to predict cerebral palsy in young children. Dev. Med. Child Neurol. 2013, 55, 418–426. [Google Scholar] [CrossRef]
- Kwong, A.K.L.; Fitzgerald, T.L.; Doyle, L.W.; Cheong, J.L.Y.; Spittle, A.J. Predictive validity of spontaneous early infant movement for later cerebral palsy: A systematic review. Dev. Med. Child Neurol. 2018, 60, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Cioni, G.; Bos, A.F.; Einspieler, C.; Ferrari, F.; Martijn, A.; Paolicelli, P.B.; Rapisardi, G.; Roversi, M.F.; Prechtl, H.F.R. Early Neurological Signs in Preterm Infants with Unilateral Intraparenchymal Echodensity. Neuropediatrics 2000, 31, 240–251. [Google Scholar] [CrossRef] [PubMed]
- Guzzetta, A.; Mercuri, E.; Rapisardi, G.; Ferrari, F.; Roversi, M.F.; Cowan, F.; Rutherford, M.; Paolicelli, P.B.; Einspieler, C.; Boldrini, A.; et al. General Movements Detect Early Signs of Hemiplegia in Term Infants with Neonatal Cerebral Infarction. Neuropediatrics 2003, 34, 61–66. [Google Scholar] [PubMed]
- Guzzetta, A.; Pizzardi, A.; Belmonti, V.; Boldrini, A.; Carotenuto, M.; D’acunto, G.; Ferrari, F.; Fiori, S.; Gallo, C.; Ghirri, P.; et al. Hand movements at 3 months predict later hemiplegia in term infants with neonatal cerebral infarction. Dev. Med. Child Neurol. 2010, 52, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, F.; Todeschini, A.; Guidotti, I.; Martinez-Biarge, M.; Roversi, M.F.; Berardi, A.; Ranzi, A.; Cowan, F.M.; Rutherford, M.A. General Movements in Full-Term Infants with Perinatal Asphyxia Are Related to Basal Ganglia and Thalamic Lesions. J. Pediatr. 2011, 158, 904–911. [Google Scholar] [CrossRef] [PubMed]
- De Vries, L.S.; Groenendaal, F. Neuroimaging in the preterm infant. Ment. Retard. Dev. Disabil. Res. Rev. 2002, 8, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Volpe, J.J. Brain injury in premature infants: A complex amalgam of destructive and developmental disturbances. Lancet Neurol. 2009, 8, 110–124. [Google Scholar] [CrossRef]
- Amiel-Tison, C. Neurological evaluation of the maturity of newborn infants. Arch. Dis. Child. 1968, 43, 89–93. [Google Scholar] [CrossRef]
- Drillien, C.M. Abnormal neurologic signs in the first year of life in low-birthweight infants: Possible prognostic significance. Dev. Med. Child Neurol. 1972, 14, 575–584. [Google Scholar] [CrossRef]
- Allen, M.C.; Alexander, G.R. Using gross motor milestones to identify very preterm infants at risk for cerebral palsy. Dev. Med. Child Neurol. 1992, 34, 226–232. [Google Scholar] [CrossRef]
- Ferrari, F.; Gallo, C.; Pugliese, M.; Guidotti, I.; Gavioli, S.; Coccolini, E.; Zagni, P.; Casa, E.D.; Rossi, C.; Lugli, L.; et al. Preterm birth and developmental problems in the preschool age. Part I: Minor motor problems. J. Matern. Fetal Neonatal Med. 2012, 25, 2154–2159. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, M.; Rossi, C.; Guidotti, I.; Gallo, C.; Casa, E.D.; Bertoncelli, N.; Coccolini, E.; Ferrari, F. Preterm birth and developmental problems in infancy and preschool age Part II: Cognitive, neuropsychological and behavioural outcomes. J. Matern. Fetal Neonatal Med. 2013, 26, 1653–1657. [Google Scholar] [CrossRef] [PubMed]
- Bruggink, J.L.; Einspieler, C.; Butcher, P.R.; Van Braeckel, K.N.; Prechtl, H.F.; Bos, A.F. The quality of the early motor repertoire in preterm infants predicts minor neurologic dysfunction at school age. J. Pediatr. 2008, 153, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Bruggink, J.L.; Einspieler, C.; Butcher, P.R.; Stremmelaar, E.F.; Prechtl, H.F.; Bos, A.F. Quantitative aspects of the early motor repertoire in preterm infants: Do they predict minor neurological dysfunction at school age? Early Hum. Dev. 2009, 85, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, F.; Bertoncelli, N.; Roversi, M.F.; Cattani, S.; Ori, L.; Ranzi, A. Motor and postural behavior in low-risk preterm infants from 30–33 to 46–54 weeks’ postmenstrual age: An observational study. Prenat. Neonatal Med. 2001, 6, 166–183. [Google Scholar]
- Van Dyk, J.; Church, P.; Dell, S.; To, T.; Luther, M.; Shah, V. Prediction of long-term neurodevelopmental outcome in preterm infants using trajectories of general movement assessments. J. Perinatol. Off. J. Calif. Perinat. Assoc. 2018, 38, 1398–1406. [Google Scholar] [CrossRef] [PubMed]
- Manacero, S.A.; Marschik, P.B.; Nunes, M.L.; Einspieler, C. Is it possible to predict the infant’s neurodevelopmental outcome at 14 months of age by means of a single preterm assessment of General Movements? Early Hum. Dev. 2012, 88, 39–43. [Google Scholar] [CrossRef]
- Bos, A.F.; van Asperen, R.M.; de Leeuw, D.M.; Prechtl, H.F.R. The influence of septicaemia on spontaneous motility in preterm infants. Early Hum. Dev. 1997, 50, 61–70. [Google Scholar] [CrossRef]
- Hitzert, M.M.; Roescher, A.M.; Bos, A.F. The quality of general movements after treatment with low-dose dexamethasone in preterm infants at risk of bronchopulmonary dysplasia. Neonatology 2014, 106, 222–228. [Google Scholar] [CrossRef]
- Bos, A.F.; Martijn, A.; van Asperen, R.M.; Hadders-Algra, M.; Okken, A.; Prechtl, H.F. Qualitative assessment of general movements in high-risk preterm infants with chronic lung disease requiring dexamethasone therapy. J. Pediatr. 1998, 132, 300–306. [Google Scholar] [CrossRef]
- Bruggink, J.L.; Cioni, G.; Einspieler, C.; Maathuis, C.G.; Pascale, R.; Bos, A.F. Early motor repertoire is related to level of self-mobility in children with cerebral palsy at school age. Dev. Med. Child Neurol. 2009, 51, 878–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crowle, C.; Walker, K.; Galea, C.; Novak, I.; Badawi, N. General movement trajectories and neurodevelopment at 3months of age following neonatal surgery. Early Hum. Dev. 2017, 111, 42–48. [Google Scholar] [CrossRef] [PubMed]
- De Vries, N.K.S.; Bos, A.F. The quality of general movements in the first ten days of life in preterm infants. Early Hum. Dev. 2010, 86, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Garcia, J.M.; Gherpelli, J.L.D.; Leone, C.R. The role of spontaneous general movement assessment in the neurological outcome of cerebral lesions in preterm infants. J. Pediatr. 2004, 80, 296–304. [Google Scholar] [CrossRef]
- Nakajima, Y.; Einspieler, C.; Marschik, P.B.; Bos, A.F.; Prechtl, H.F. Does a detailed assessment of poor repertoire general movements help to identify those infants who will develop normally? Early Hum. Dev. 2006, 82, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Olsen, J.E.; Brown, N.C.; Eeles, A.L.; Lee, K.J.; Anderson, P.J.; Cheong, J.L.Y.; Doyle, L.W.; Spittle, A.J. Trajectories of general movements from birth to term-equivalent age in infants born <30 weeks’ gestation. Early Hum. Dev. 2015, 91, 683–688. [Google Scholar]
- Roze, E.; Meijer, L.; Van Braeckel, K.N.; Ruiter, S.A.; Bruggink, J.L.; Bos, A.F. Developmental trajectories from birth to school age in healthy term-born children. Pediatrics 2010, 126, e1134–e1142. [Google Scholar] [CrossRef]
- Ferrari, F.; Cioni, G.; Einspieler, C.; Roversi, M.F.; Bos, A.F.; Paolicelli, P.B.; Ranzi, A.; Prechtl, H.F.R. Cramped Synchronized General Movements in Preterm Infants as an Early Marker for Cerebral Palsy. Arch. Pediatr. Adolesc. Med. 2002, 156, 460–467. [Google Scholar] [CrossRef]
- Back, S.A. Brain Injury in the Preterm Infant: New Horizons for Pathogenesis and Prevention. Pediatr. Neurol. 2015, 53, 185–192. [Google Scholar] [CrossRef] [Green Version]
- Hamrick, S.E.; Miller, S.P.; Leonard, C.; Glidden, D.V.; Goldstein, R.; Ramaswamy, V.; Piecuch, R.; Ferriero, D.M. Trends in severe brain injury and neurodevelopmental outcome in premature newborn infants: The role of cystic periventricular leukomalacia. J. Pediatr. 2004, 145, 593–599. [Google Scholar] [CrossRef]


| Patterns | Definition | Score |
|---|---|---|
| Signs pointing to loss of balance | Presence of at least one minor and one major sign. Major signs are sudden abduction-extension of the four limbs, burst of tremors, abrupt rolling to the side, abrupt limb movements and/or head rotation at lifting of hips, burst of fast movements at three or four limbs lifting, side-to-side oscillation of lower limbs. Minor signs are finger spreading, abrupt abduction-extension of arms. | 0. Absent 1. Present |
| Tremors | Involuntary, rhythmical oscillatory movement of equal amplitude around a fixed axis. | 0. Absent 1. Some 2. Many |
| Movements towards midline in upper limbs | Antigravity movements in which a part of upper limbs moves towards or exceeds the midline (ideally considered as a line from the vertex to the lower extremities in supine position) resulting in contacts between two body parts. We distinguished simple contacts (many or some) from manipulation. | 0. Manipulation 1. Many contacts 2. Some contacts 3. Absent |
| Movements towards midline in lower limbs | Antigravity movements in which a part of lower limbs moves towards or exceeds the midline (ideally considered as a line from the vertex to the lower extremities in supine position) resulting in contacts between two body parts. We distinguished simple contacts (many or some) from manipulation. | 0. Manipulation 1. Many contacts 2. Some contacts 3. Absent |
| Open hand posture | Open hand posture mainly maintained throughout the observation. | 0. Absent 1. Present |
| Finger spreading | Abrupt unilateral or bilateral full or partial extension of fingers. | 0. Absent 1. Present |
| Monotonous/stereotyped limbs movements | Repetition of the same limbs’ movements over time. Examples are:
| 0. Absent 1. Present |
| Asymmetric tonic neck posture | Face turned to one side with extended arm and leg on the same side and flexed arm and leg on the opposite side. | 0. Absent 1. Occasional 2. Frequent/dominant |
| Head posture on a side | Head posture mainly maintained throughout most of the observation. | 0. Absent 1. Present |
| Pathological head movements | Repetitive side-to-side head movements, and/or neck hyperextension. | 0. Absent 1. Present |
| Asymmetries | Lack of equality in posture or movements between the two body sides. | 0. Absent 1. Present |
| Patterns | Trajectory | Description |
|---|---|---|
| Signs pointing to loss of balance | Low risk | Signs pointing to loss of balance disappearing before fidgety age |
| High risk | Patterns pointing to loss of balance still present at fidgety age | |
| Tremors | Low risk | Tremors disappearing before fidgety age |
| High risk | Tremors still present at fidgety age | |
| Movements towards midline in upper limbs | Low risk | Manipulation appears at fidgety age. When there is no manipulation at fidgety age, many contacts on the midline must be present starting from term age |
| High risk | Occasional movements towards midline at term age and no manipulation at fidgety age | |
| Movements towards midline in lower limbs | Low risk | Manipulation appearing at fidgety age. When there is no manipulation at fidgety age, many contacts on the midline must be present starting from term age |
| High risk | Occasional movement towards midline at term age and no manipulation at fidgety age | |
| Open hand posture | Low risk | Open hand posture disappearing before term age |
| High risk | Open hand posture still present at term and/or fidgety age | |
| Finger spreading | Low risk | Finger spreading disappearing before fidgety age |
| High risk | Finger spreading still present at fidgety age | |
| Monotonous/stereotyped limbs movements | Low risk | Monotonous or stereotyped limbs movements disappearing before term age |
| High risk | Monotonous or stereotyped limbs movements still present at term and/or fidgety age | |
| Asymmetric tonic neck (ATN) posture | Low risk | ATN posture disappearing or becoming occasional at fidgety age |
| High risk | ATN posture frequent or dominant at fidgety age | |
| Head posture on a side | Low risk | Head-on-midline posture predominant at fidgety age |
| High risk | Head posture on a side predominant at fidgety age | |
| Pathological head movements | Low risk | Normal head movements present from term age |
| High risk | Side-to-side head movements or neck hyperextension present at term and/or fidgety age | |
| Asymmetries | Low risk | Asymmetric postures and movements disappearing before fidgety age |
| High risk | Asymmetric postures and movements present at fidgety age |
| Clinical Characteristics | Cases N = 37 | Controls N = 42 | p | |
|---|---|---|---|---|
| Infant Characteristics at Birth | ||||
| Male/female ratio | 16:21 | 14:28 | 0.368 | |
| Birth gestational age in weeks (mean ± SD 1) | 28.4 ± 3 | 28.7 ± 2 | 0.395 | |
| Birth weight (mean ± SD) | 1148 ± 499 | 1065 ± 240 | 0.694 | |
| Birth head circumference (mean ± SD) | 26 ± 3 | 26 ± 2 | 0.579 | |
| Birth weight for gestational age | Number of SGA2infants (%) | 2 (5.4%) | 10 (23.8%) | 0.080 |
| Number of AGA3infants (%) | 29 (78.4%) | 26 (61.9%) | ||
| Number of LGA4infants (%) | 6 (16.2%) | 6 (14.3%) | ||
| Apgar score | Number of infants with 1-min Apgar score < 7 (%) | 27 (73.0%) | 19 (45.2%) | 0.005 |
| Number of infants with 5-min Apgar score < 7 (%) | 12 (32.4%) | 8 (19.0%) | 0.122 | |
| US cerebral lesions | ||||
| Number of IVH 5 1 (%) | 2 (5.4%) | 1 (2.4%) | <0.001 | |
| Number of IVH 2 (%) | 10 (27.0%) | 1 (2.4%) | ||
| Number of IVH 3 (%) | 8 (21.6%) | 0 (0.0%) | ||
| Number of IVH 4 (%) | 4 (10.8%) | 0 (0.0%) | ||
| Number of PVL 6 1 (%) | 8 (21.6%) | 12 (28.6%) | 0.001 | |
| Number of PVL 2 (%) | 4 (10.8%) | 5 (11.9%) | ||
| Number of PVL 3 (%) | 8 (21.6%) | 0 (0.0%) | ||
| Number of PVL 4 (%) | 4 (10.8%) | 0 (0.0%) | ||
| Trajectories | Group | OR | 95% CI | p | |||
|---|---|---|---|---|---|---|---|
| Control N = 42 | Case N = 42 | ||||||
| n | % | n | % | ||||
| Normal GMs and F+ | 6 | 14.3 | 0 | 0 | Ref. | - | - |
| Transient PR and F+ | 14 | 33.3 | 0 | 0 | 2.23 | 0.04–125.22 | 0.6962 |
| Persistent PR and F+ | 16 | 38.1 | 5 | 13.5 | 4.33 | 0.21–90.05 | 0.3435 |
| Transient CS and F+ | 1 | 2.4 | 0 | 0 | 4.33 | 0.03–560.31 | 0.5545 |
| Persistent PR and F− | 5 | 11.9 | 16 | 43.2 | 39.00 | 0.67–2257.11 | 0.0768 |
| Transient CS and F− | 0 | 0 | 7 | 18.9 | 195.00 | 3.37–11,285.55 | 0.0109 |
| Persistent CS and F− | 0 | 0 | 7 | 18.9 | 195.00 | 10.65–3569.68 | 0.0004 |
| Trajectories | Group | OR | 95% CI | p | |||
|---|---|---|---|---|---|---|---|
| Control | Case | ||||||
| n/N | % | n/N | % | ||||
| Low risk | 37 | 88.1 | 5 | 13.5 | - | - | - |
| High risk | 5 | 11.9 | 30 | 81.1 | 44.40 | 11.74–167.85 | <0.001 |
| Patterns | Odds Ratio (95% CI) | |||
|---|---|---|---|---|
| Preterm Age | Term Age | Fidgety Age | ||
| LB | 0.23 (0.09–0.62) | 0.59 (0.23–1.48) | 20.90 (1.15–379.98) * | |
| T | 0.80 (0.25–2.55) | 5.19 (1.87–14.43) | 46.84 (2.67–822.91) * | |
| MTM-UL | Many | - | - | 13.89 (2.90–66.62) |
| Some | - | 5.20 (1.66–16.26) | 16.67 (3.84–72.33) | |
| Absent | 2.56 (0.77–8.53) | 12.00 (1.84–78.37) | 22.22 (3.72–132.75) | |
| MTM-LL | Many | - | - | 14.88 (1.75–126.50) |
| Some | - | 2.22 (0.52–9.54) | 27.20 (2.71–272.83) | |
| Absent | 1.04 (0.42–2.55) | 6.06 (1.37–26.76) | 59.50 (5.95–595.04) | |
| OHP | 3.83 (1.49–9.89) | 7.81 (2.51–24.30) | 9.57 (1.12–81.93) | |
| FS | 0.34 (0.10–1.11) | 0.49 (0.15–1.66) | 17.54 (0.95–322.99) | |
| MSLM | 3.25 (0.77–13.68) | 12.50 (4.14–37.74) | 175.71 (20.52–1504.80) | |
| ATN | 1.85 (0.53–6.45) | 2.44 (0.93–6.39) | 10.85 (3.47–33.98) | |
| HPS | 1.88 (0.57–6.12) | 2.67 (1.07–6.64) | 6.43 (1.29–32.05) | |
| PHM | 5.29 (0.56–49.71) | 15.19 (1.84–125.53) | 5.50 (1.40–21.64) | |
| ASY | 2.49 (0.22–28.62) | 1.14 (0.07–18.87) | 7.04 (1.82–27.28) | |
| Age | Pattern | OR | 95% CI | |
| Preterm age | GMs | Normal | reference | reference |
| PR | 15.60 | 0.87–280.15 | ||
| CS | 323.00 | 5.75–18131.35 | ||
| LB | Absent | reference | reference | |
| Present | 0.23 | 0.09–0.62 | ||
| OHP | Absent | reference | reference | |
| Present | 3.83 | 1.49–9.89 | ||
| Term age | GMs | Normal | reference | reference |
| PR | 33.00 | 1.87–581.28 | ||
| CS | 178.20 | 7.87–4037.41 | ||
| MSLM | Absent | reference | reference | |
| Present | 12.50 | 4.14–37.74 | ||
| OHP | Absent | reference | reference | |
| Present | 7.81 | 2.51–24.30 | ||
| Fidgety age | GMs | F + | reference | reference |
| F − | 47.36 | 12.57–178.51 | ||
| MSLM | Absent | reference | reference | |
| Present | 175.71 | 20.52–1504.80 | ||
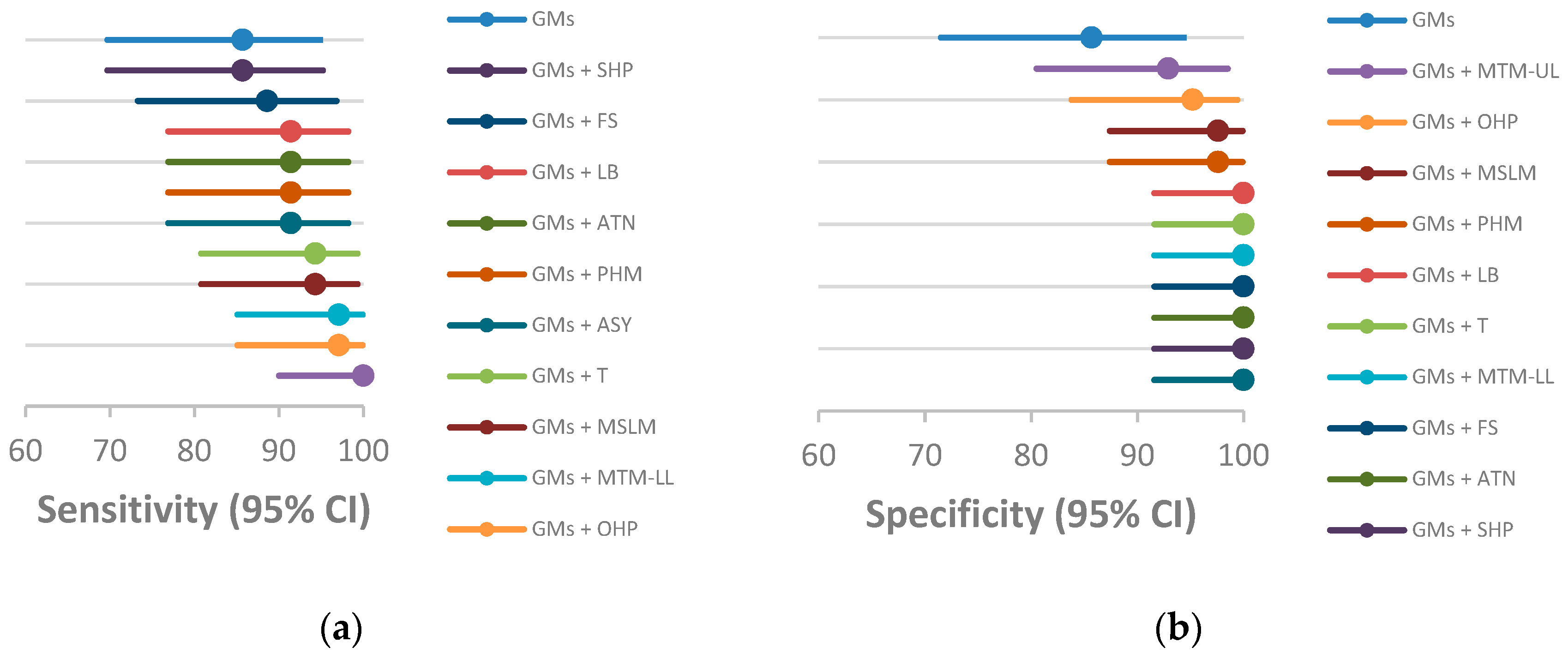
| Sensitivity % (95% CI) | Specificity % (95% CI) | |
|---|---|---|
| GMs trajectories | 85.7 (69.7–95.2) | 85.7 (71.5–94.6) |
| GMs trajectories + LB trajectories | 91.4 (76.9–98.2) | 100 (91.6–100 *) |
| GMs trajectories + T trajectories | 94.3 (80.8–99.3) | 100 (91.6–100*) |
| GMs trajectories + MTM–UL trajectories | 100 (90.0–100 *) | 92.9 (80.5–98.5) |
| GMs trajectories + MTM–LL trajectories | 97.1 (85.1–99.9) | 100 (91.6–100 *) |
| GMs trajectories + OHP trajectories | 97.1 (85.1–99.9) | 95.2 (83.8–99.4) |
| GMs trajectories + FS trajectories | 88.6 (73.3–96.8) | 100 (91.6–100 *) |
| GMs trajectories + MSLM trajectories | 94.3 (80.8–99.3) | 97.6 (87.4–99.9) |
| GMs trajectories + ATN trajectories | 91.4 (76.9–98.2) | 100 (91.6–100 *) |
| GMs trajectories + HPS trajectories | 85.7 (69.7–95.2) | 100 (91.6–100 *) |
| GMs trajectories + PHM trajectories | 91.4 (76.9–98.2) | 97.6 (87.4–99.9) |
| GMs trajectories + ASY trajectories | 91.4 (76.9–98.2) | 100 (91.6–100 *) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrari, F.; Plessi, C.; Lucaccioni, L.; Bertoncelli, N.; Bedetti, L.; Ori, L.; Berardi, A.; Della Casa, E.; Iughetti, L.; D’Amico, R. Motor and Postural Patterns Concomitant with General Movements Are Associated with Cerebral Palsy at Term and Fidgety Age in Preterm Infants. J. Clin. Med. 2019, 8, 1189. https://doi.org/10.3390/jcm8081189
Ferrari F, Plessi C, Lucaccioni L, Bertoncelli N, Bedetti L, Ori L, Berardi A, Della Casa E, Iughetti L, D’Amico R. Motor and Postural Patterns Concomitant with General Movements Are Associated with Cerebral Palsy at Term and Fidgety Age in Preterm Infants. Journal of Clinical Medicine. 2019; 8(8):1189. https://doi.org/10.3390/jcm8081189
Chicago/Turabian StyleFerrari, Fabrizio, Carlotta Plessi, Laura Lucaccioni, Natascia Bertoncelli, Luca Bedetti, Luca Ori, Alberto Berardi, Elisa Della Casa, Lorenzo Iughetti, and Roberto D’Amico. 2019. "Motor and Postural Patterns Concomitant with General Movements Are Associated with Cerebral Palsy at Term and Fidgety Age in Preterm Infants" Journal of Clinical Medicine 8, no. 8: 1189. https://doi.org/10.3390/jcm8081189