Synergistic Action of Gefitinib and GSK41364A Simultaneously Loaded in Ratiometrically-Engineered Polymeric Nanoparticles for Glioblastoma Multiforme


Abstract
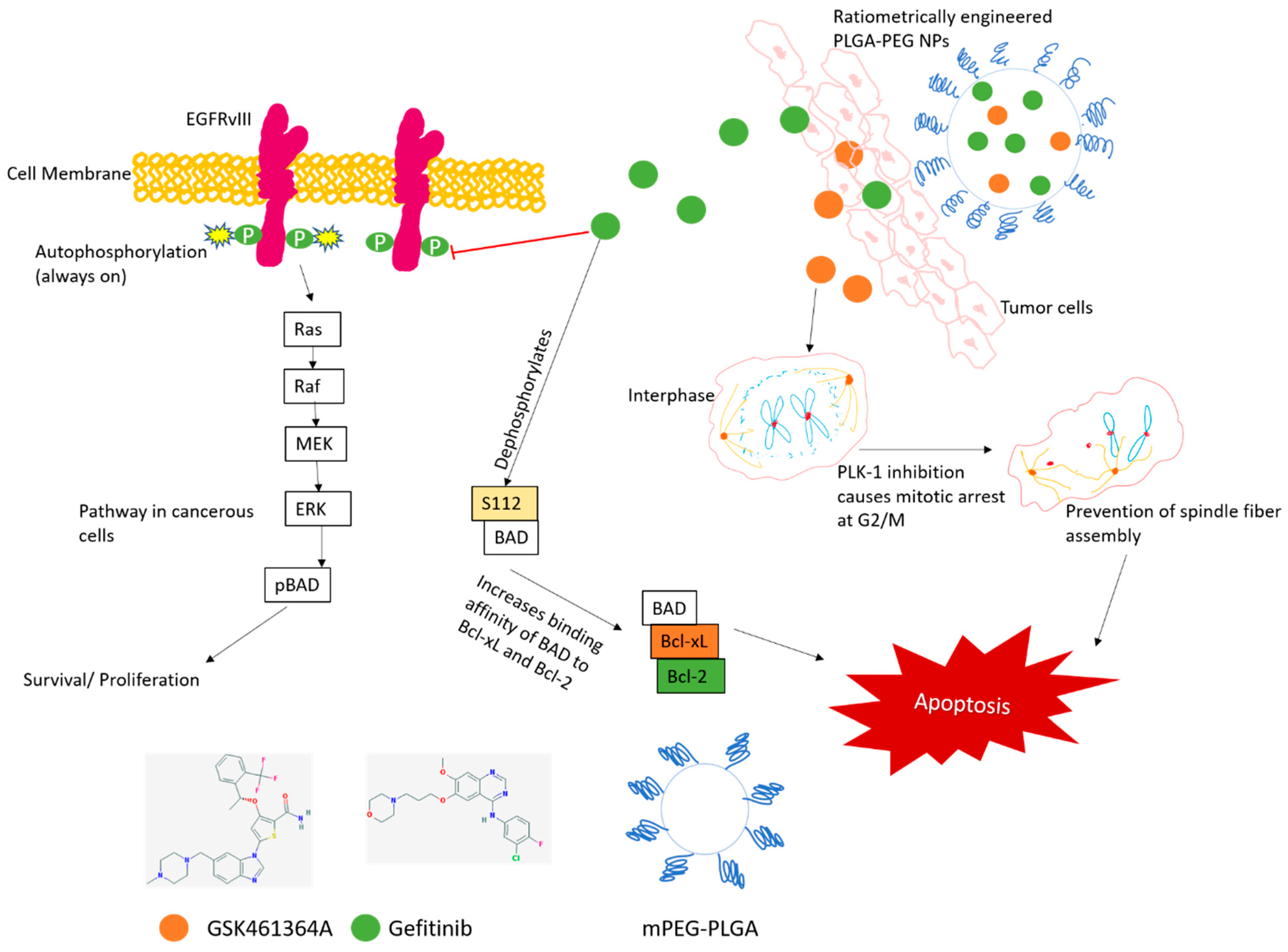
:1. Introduction
2. Experimental Section
2.1. Ratiometric Synthesis and Characterization of Co-Loaded PLGA-PEG Nanoparticles
2.1.1. Characterization of Co-Encapsulated Nanocarriers
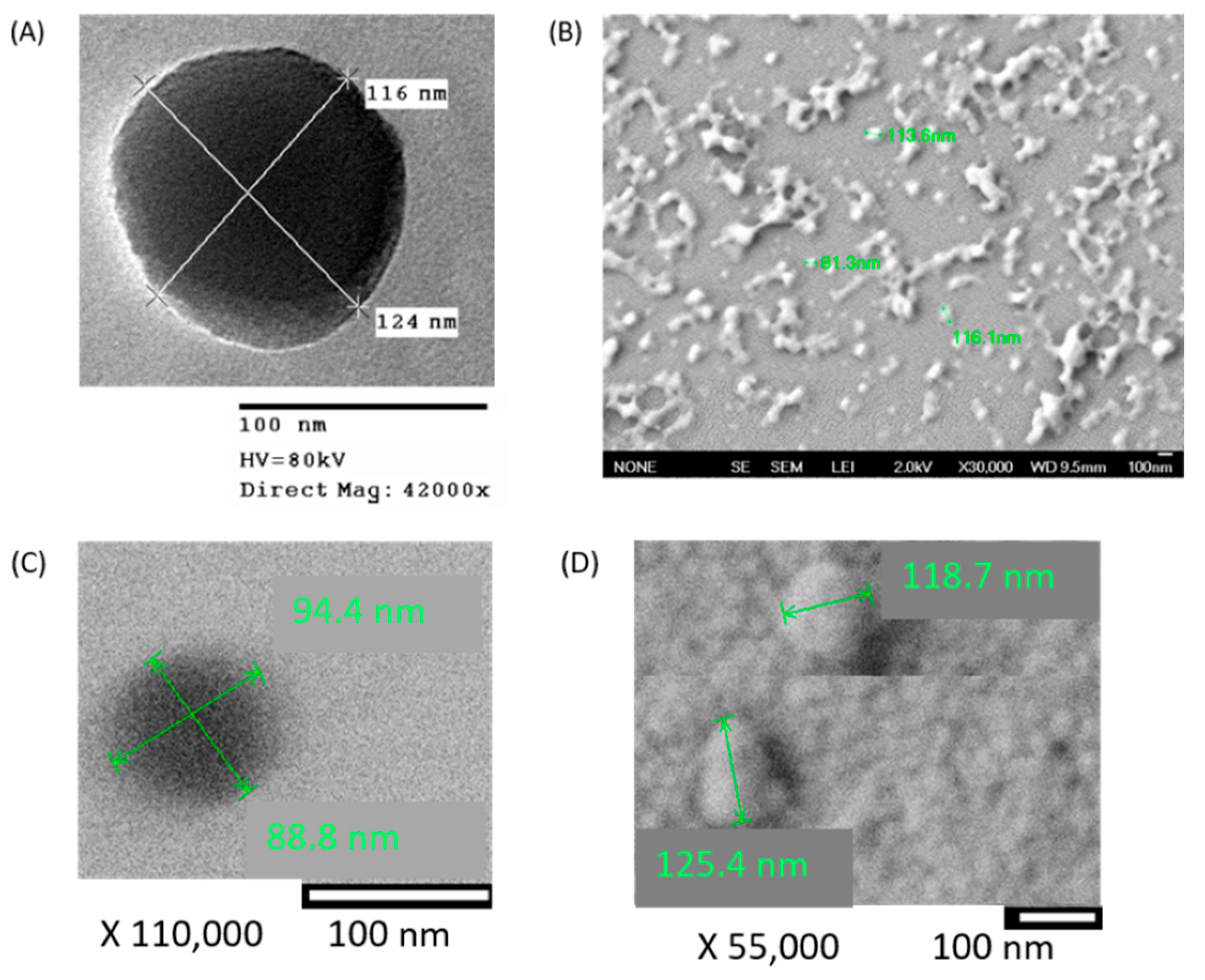
2.1.2. Morphological Characterization
2.1.3. Determination of Encapsulation Efficiency
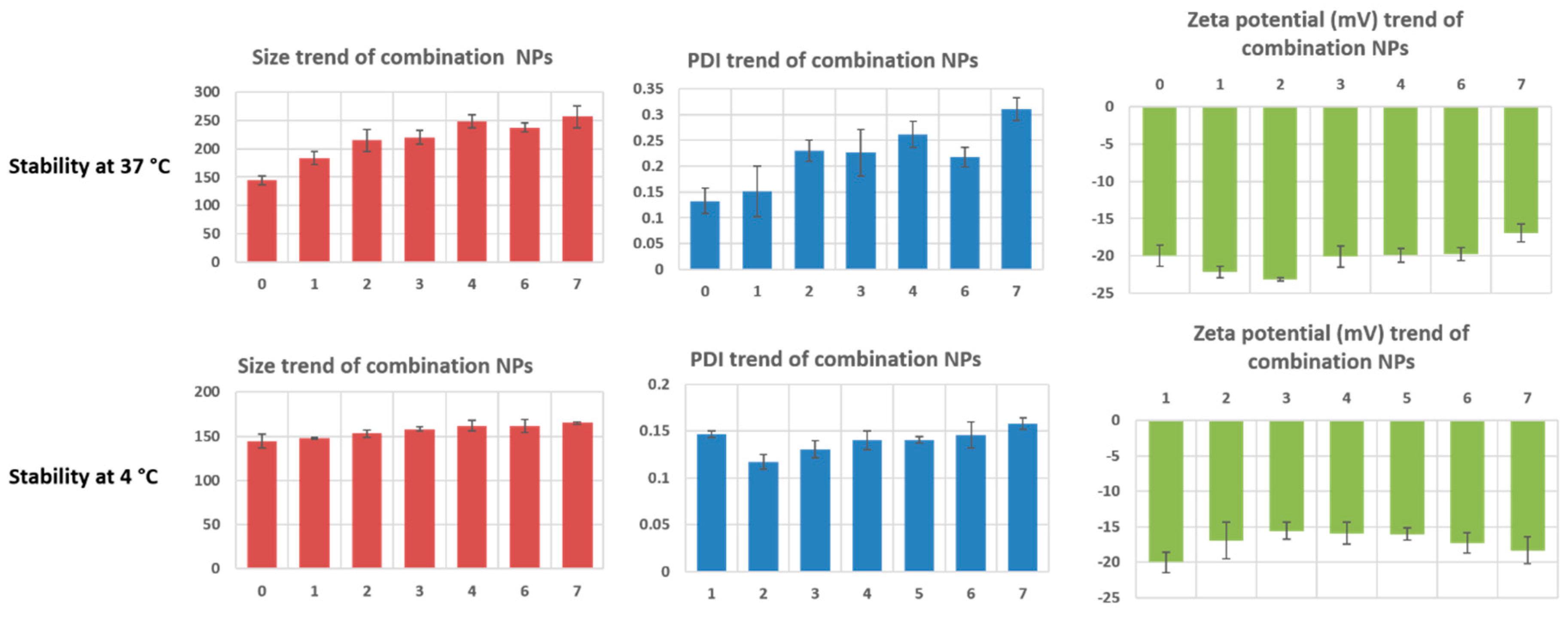
2.2. In Vitro Stability of Co-Loaded PLGA-PEG Nanoparticles
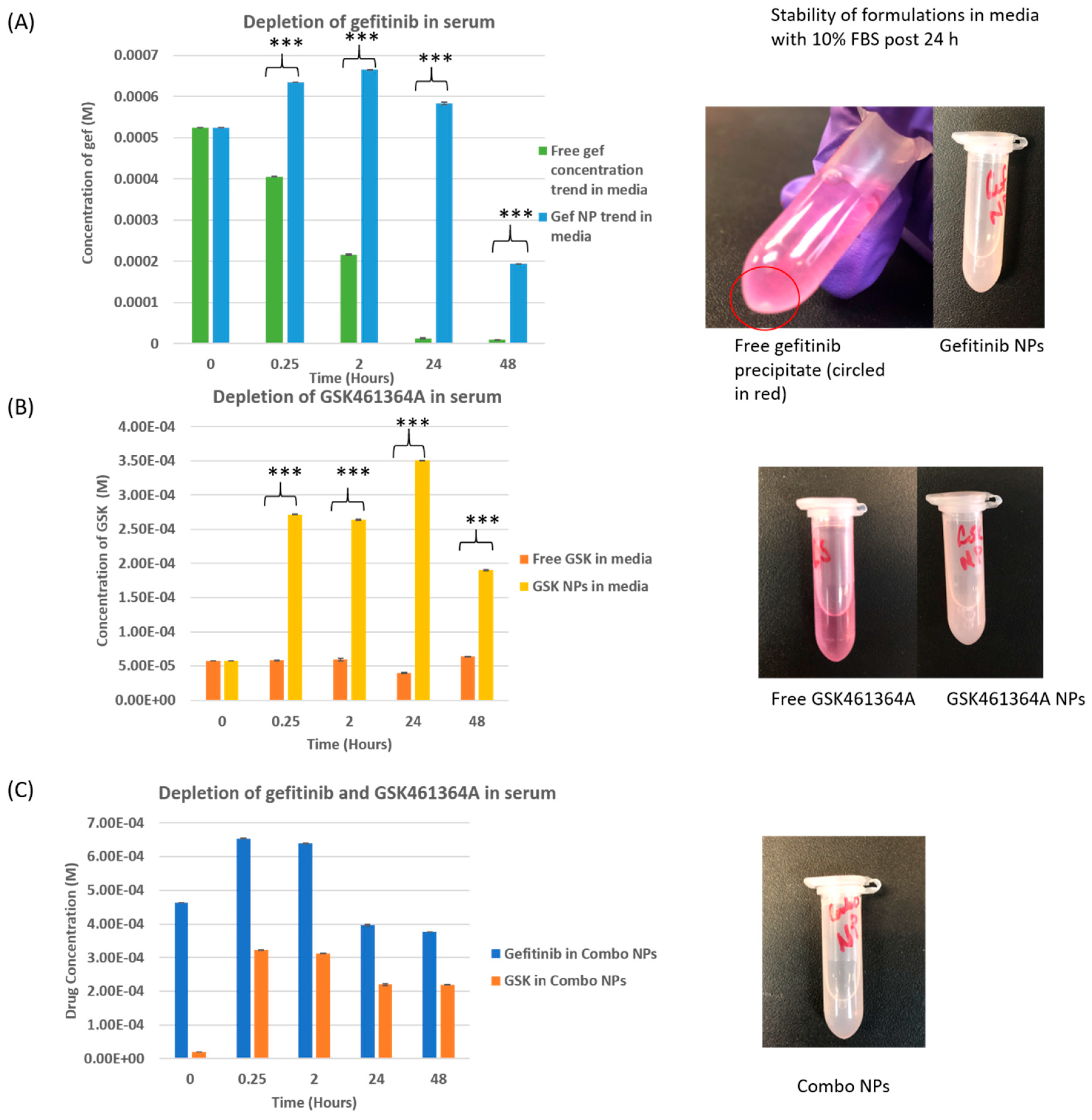
2.3. Stability of Free vs. Nano Drug in Media Containing Fetal Bovine Serum
2.4. Measurement of In Vitro Drug Release from the Combination Nanoparticles
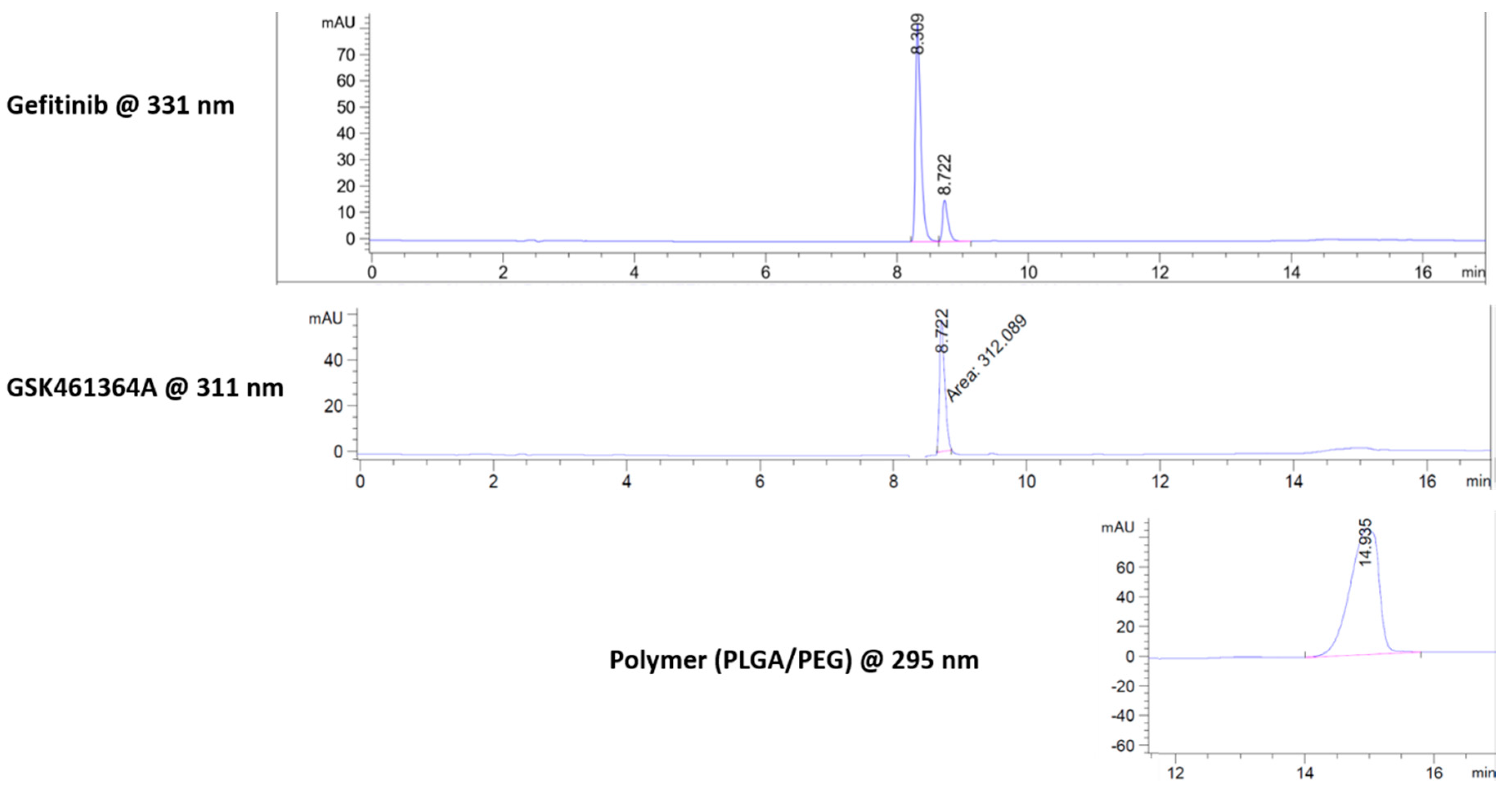
2.4.1. Peak Separation Using Reverse Phase HPLC
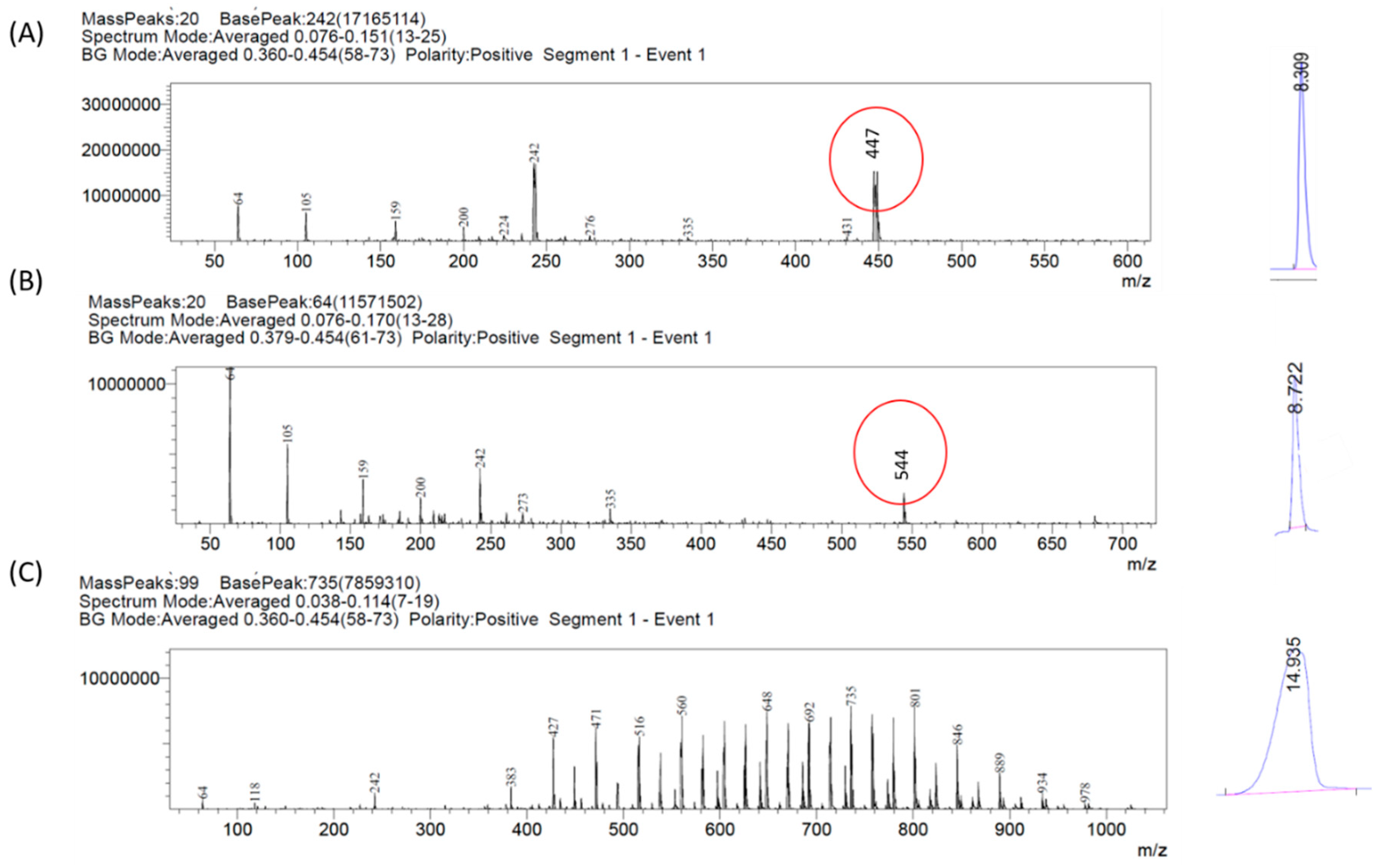
2.4.2. Peak Confirmation Using Mass Spectrometer
2.5. EC50 Determination of Gefitinib and GSK461364A
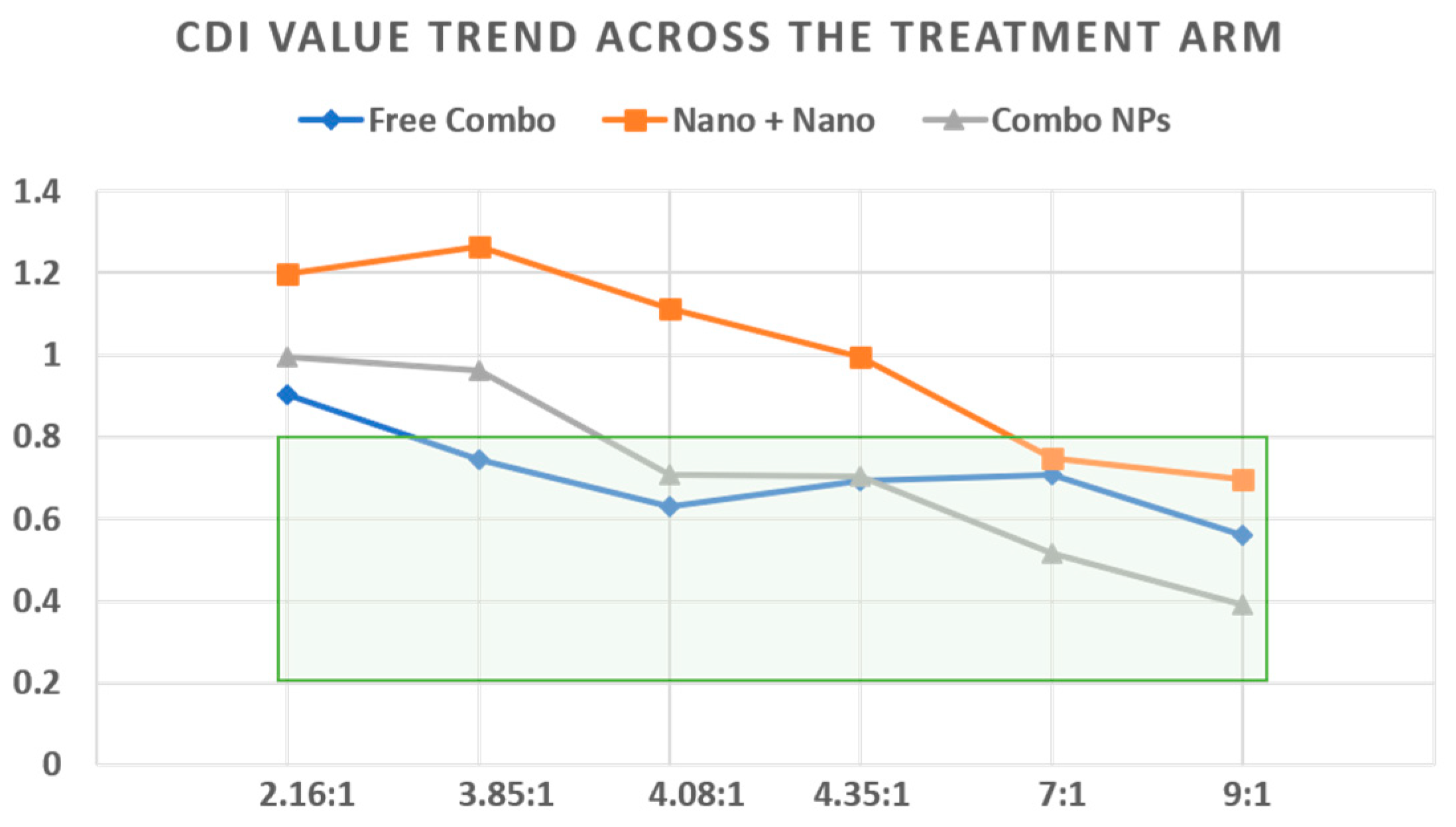
2.6. Estimation of the Drug Concentrations in the Ratiometric Study from the Free Drug Combination- Cytotoxicity Study
2.7. Measurement of Cytotoxicity-Evaluation of the Treatment for Synergy in Monolayer Cultures of U87-MG
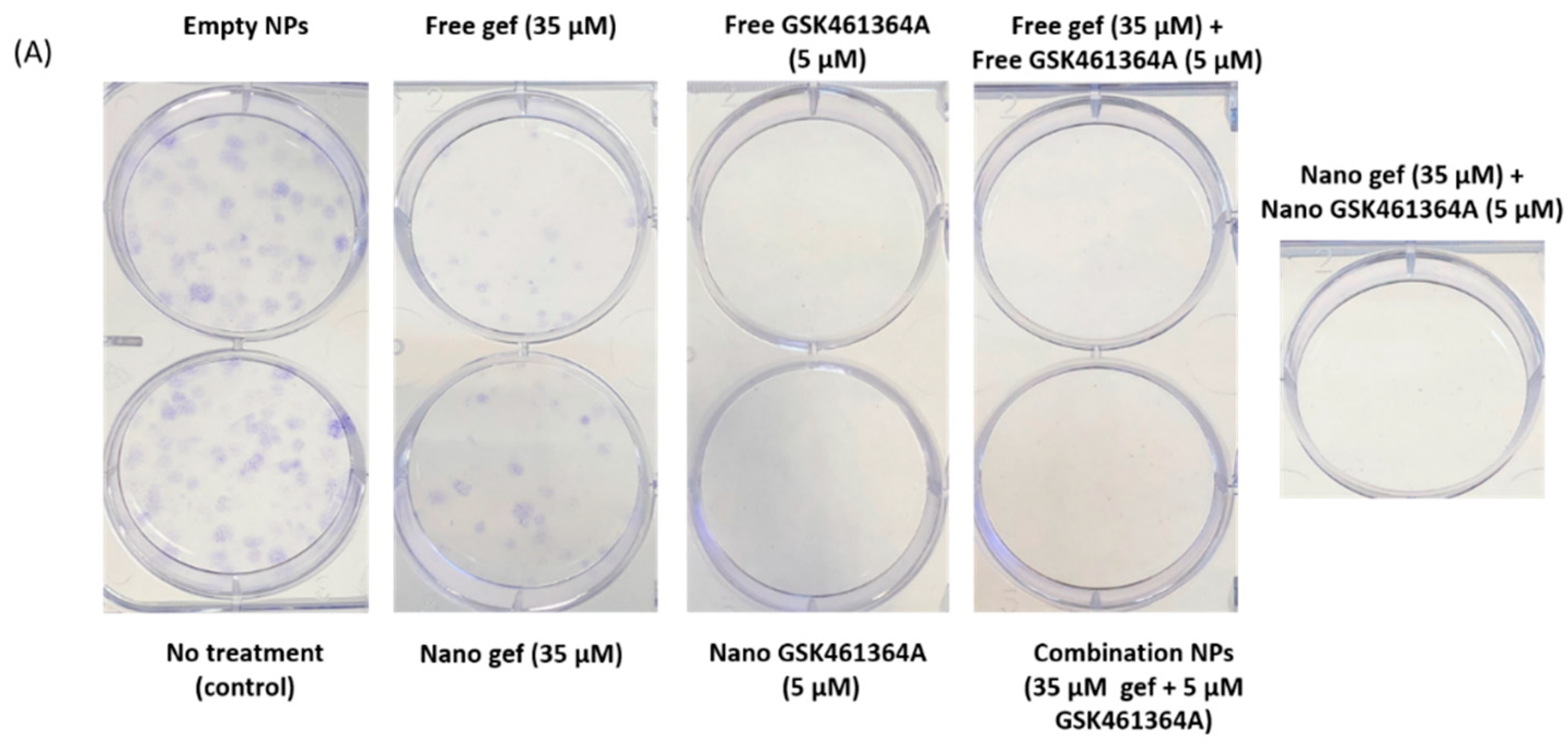
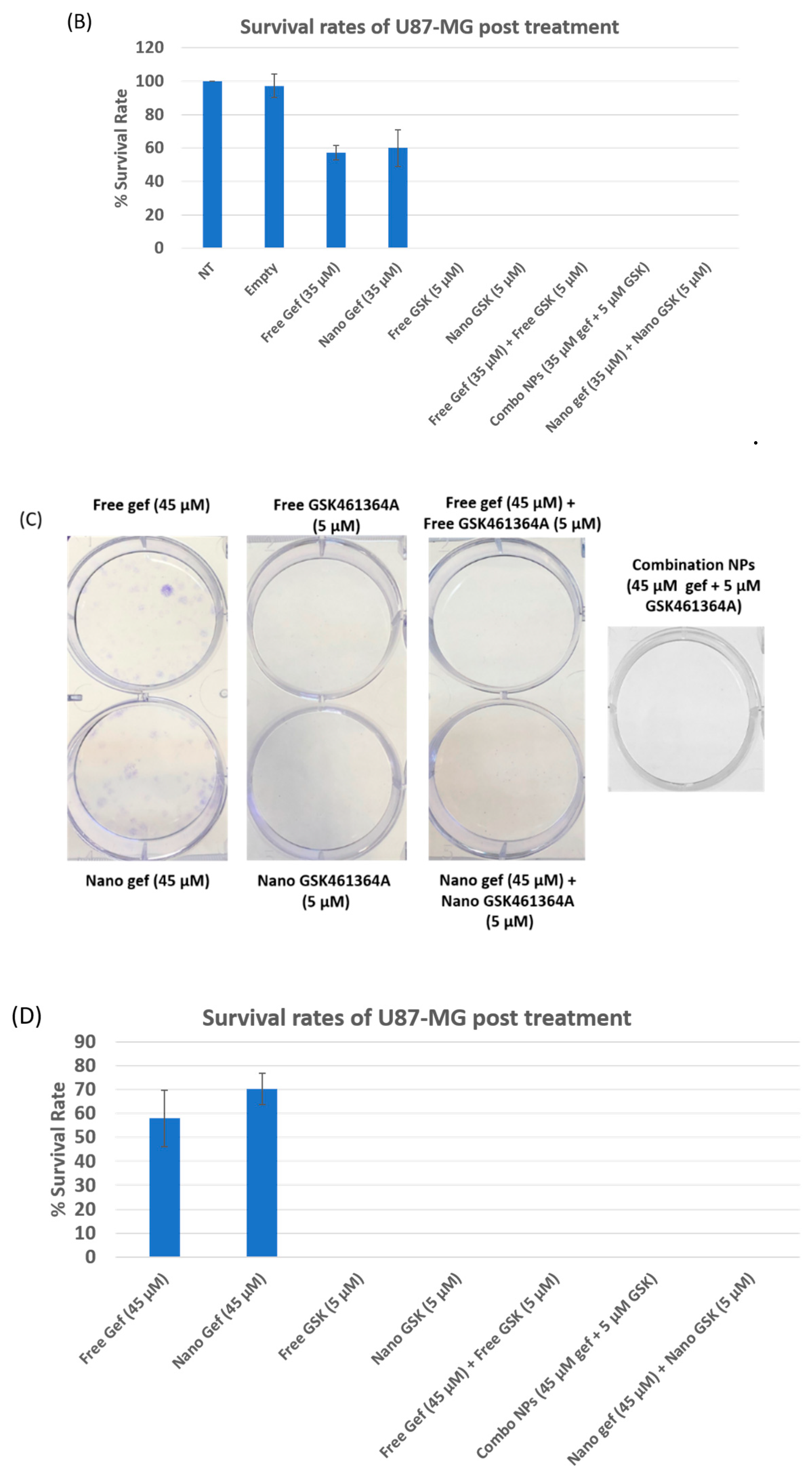
2.8. Clonogenic Assay
3. Results
3.1. Synthesis Optimization and Characterization of Dual Drug Loaded PLGA-PEG NPs
Morphological Characterization
3.2. In Vitro Stability Study
3.3. Stability of Free vs. Nano Drug in Media Containing Fetal Bovine Serum
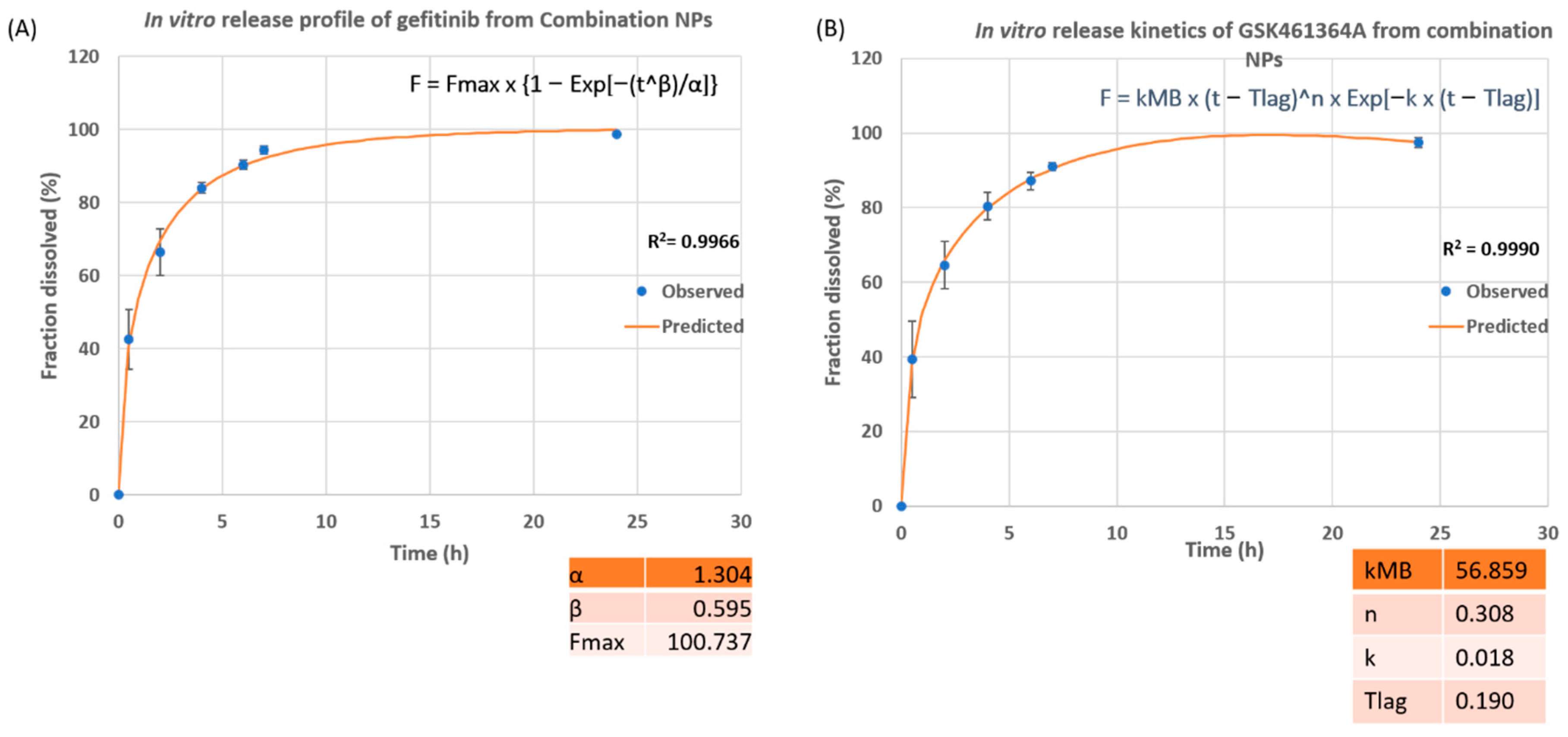
3.4. Measurement of In Vitro Drug Release from the Combination Nanoparticles
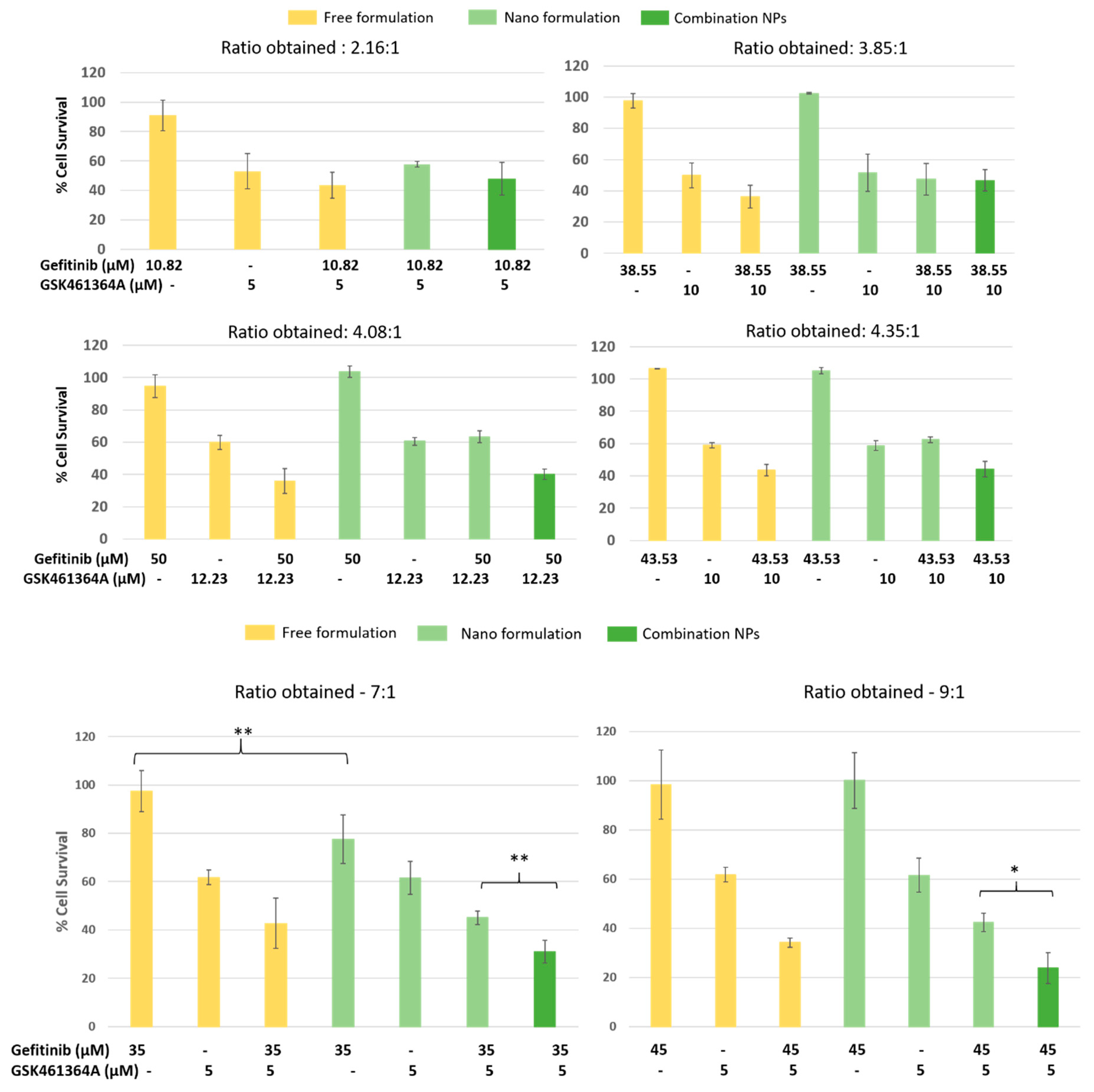
3.5. Measurement of Cytotoxicity -Evaluation of the Treatment for Synergy in Monolayer Cultures of U87-MG
3.6. Clonogenic Assay
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Scott, C.B.; Scarantino, C.; Urtasun, R.; Movsas, B.; Jones, C.U.; Simpson, J.R.; Fischbach, A.J.; Curran, W.J. Validation and Predictive Power of Radiation Therapy Oncology Group (RTOG) Recursive Partitioning Analysis Classes for Malignant Glioma Patients: A Report Using RTOG 90-06. Int. J. Radiat. Oncol. Biol. Phys. 1998, 40, 51–55. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Gittleman, H.; Farah, P.; Ondracek, A.; Chen, Y.; Wolinsky, Y.; Stroup, N.E.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2006–2010. Neuro Oncol. 2013, 15 (Suppl. 2), iv1–iv62. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Bauchet, L.; Davis, F.G.; Deltour, I.; Fisher, J.L.; Langer, C.E.; Pekmezci, M.; Schwartzbaum, J.A.; Turner, M.C.; Walsh, K.M.; et al. The epidemiology of glioma in adults: A “state of the science” review. Neuro Oncol. 2014, 16, 896–913. [Google Scholar] [CrossRef] [PubMed]
- Kamb, A.; Wee, S.; Lengauer, C. Why is cancer drug discovery so difficult? Nat. Rev. Drug Discov. 2007, 6, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Kesari, S.; Ram, Z.; Investigators, E.F.T. Tumor-treating fields plus chemotherapy versus chemotherapy alone for glioblastoma at first recurrence: A post hoc analysis of the EF-14 trial. CNS Oncol. 2017, 6, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Taillibert, S.; Kanner, A.; Read, W.; Steinberg, D.M.; Lhermitte, B.; Toms, S.; Idbaih, A.; Ahluwalia, M.S.; Karen Fink, K.; et al. Effect of Tumor-Treating Fields Plus Maintenance Temozolomide vs. Maintenance Temozolomide Alone on Survival in Patients with Glioblastoma: A Randomized Clinical Trial. JAMA 2017, 318, 2306–2316. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Wong, E.T.; Kanner, A.A.; Steinberg, D.; Engelhard, H.; Heidecke, V.; Kirson, E.D.; Taillibert, S.; Liebermann, F.; Dbalý, V.; et al. NovoTTF-100A versus physician’s choice chemotherapy in recurrent glioblastoma: A randomised phase III trial of a novel treatment modality. Eur. J. Cancer 2012, 48, 2192–2202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koshy, M.; Villano, J.L.; Dolecek, T.A.; Howard, A.; Mahmood, U.; Chmura, S.J.; Weichselbaum, R.R.; McCarthy, B.J. Improved survival time trends for glioblastoma using the SEER 17 population-based registries. J. Neurooncol. 2012, 107, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Velpurisiva, P.; Gad, A.; Piel, B.; Jadia, R.; Rai, P. Nanoparticle Design Strategies for Effective Cancer Immunotherapy. J. Biomed. 2017, 2, 64–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campanella, F.; Fabbro, F.; Ius, T.; Shallice, T.; Skrap, M. Acute effects of surgery on emotion and personality of brain tumor patients: Surgery impact, histological aspects, and recovery. Neuro Oncol. 2015, 17, 1121–1131. [Google Scholar] [CrossRef] [PubMed]
- Nieder, C.; Grosu, A.L.; Astner, S.; Molls, M. Treatment of unresectable glioblastoma multiforme. Anticancer Res. 2005, 25, 4605–4610. [Google Scholar] [PubMed]
- Fazeny-Dörner, B.; Wenzel, C.; Veitl, M.; Piribauer, M.; Rössler, K.; Dieckmann, K.; Ungersböck, K.; Marosi, C. Survival and prognostic factors of patients with unresectable glioblastoma multiforme. Anticancer Drugs 2003, 14, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Hatanpaa, K.J.; Burma, S.; Zhao, D.; Habib, A.A. Epidermal growth factor receptor in glioma: Signal transduction, neuropathology, imaging, and radioresistance. Neoplasia 2010, 12, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Schulte, A.; Liffers, K.; Kathagen, A.; Riethdorf, S.; Zapf, S.; Merlo, A.; Kolbe, K.; Manfred, W.; Lamszus, K. Erlotinib resistance in EGFR-amplified glioblastoma cells is associated with upregulation of EGFRvIII and PI3Kp110delta. Neuro Oncol. 2013, 15, 1289–1301. [Google Scholar] [CrossRef] [PubMed]
- Yano, S.; Kondo, K.; Yamaguchi, M.; Richmond, G.; Hutchison, M.; Wakeling, A.; Averbuch, S.; Wadsworth, P. Distribution and function of EGFR in human tissue and the effect of EGFR tyrosine kinase inhibition. Anticancer Res. 2003, 23, 3639–3650. [Google Scholar] [PubMed]
- Kaur, J.; Tikoo, K. p300/CBP dependent hyperacetylation of histone potentiates anticancer activity of gefitinib nanoparticles. Biochim. Biophys. Acta 2013, 1833, 1028–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakeling, A.E.; Guy, S.P.; Woodburn, J.R.; Ashton, S.E.; Curry, B.J.; Barker, A.J.; Gibson, K.H. ZD1839 (Iressa): An orally active inhibitor of epidermal growth factor signaling with potential for cancer therapy. Cancer Res. 2002, 62, 5749–5754. [Google Scholar] [PubMed]
- Ward, W.H.; Cook, P.N.; Slater, A.M.; Davies, D.H.; Holdgate, G.A.; Green, L.R. Epidermal growth factor receptor tyrosine kinase. Investigation of catalytic mechanism, structure-based searching and discovery of a potent inhibitor. Biochem. Pharmacol. 1994, 48, 659–666. [Google Scholar] [CrossRef]
- Chang, C.-Y.; Shen, C.-C.; Su, H.-L.; Chen, C.-J. Gefitinib induces apoptosis in human glioma cells by targeting Bad phosphorylation. J. Neurooncol. 2011, 105, 507–522. [Google Scholar] [CrossRef] [PubMed]
- Barr, F.A.; Sillje, H.H.; Nigg, E.A. Polo-like kinases and the orchestration of cell division. Nat. Rev. Mol. Cell Biol. 2004, 5, 429–440. [Google Scholar] [CrossRef] [PubMed]
- Pezuk, J.A.; Brassesco, M.; Morales, A.G.; De Oliveira, J.C.; Queiroz, R.G.D.P.; Machado, H.R.; Carlotti, C.G.; Neder, L.; Scrideli, C.A.; Tone, L.G. Polo-like kinase 1 inhibition causes decreased proliferation by cell cycle arrest, leading to cell death in glioblastoma. Cancer Gene Ther. 2013, 20, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Olmos, D.; Barker, D.; Sharma, R.; Brunetto, A.T.; Yap, T.A.; Taegtmeyer, A.B.; Barriuso, J.; Medani, H.; Degenhardt, Y.Y.; Allred, A.J.; et al. Phase I study of GSK461364, a specific and competitive Polo-like kinase 1 inhibitor, in patients with advanced solid malignancies. Clin. Cancer Res. 2011, 17, 3420–3430. [Google Scholar] [CrossRef] [PubMed]
- Tandle, A.T.; Kramp, T.; Kil, W.J.; Halthore, A.; Gehlhaus, K.; Shankavaram, U.; Tofilon, P.J.; Caplenb, N.J.; Camphausen, K. Inhibition of polo-like kinase 1 in glioblastoma multiforme induces mitotic catastrophe and enhances radiosensitisation. Eur. J. Cancer 2013, 49, 3020–3028. [Google Scholar] [CrossRef] [PubMed]
- Mignani, S.; Bryszewska, M.; Klajnert-Maculewicz, B.; Zablocka, M.; Majoral, J.P. Advances in combination therapies based on nanoparticles for efficacious cancer treatment: an analytical report. Biomacromolecules 2015, 16, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Miles, D.; von Minckwitz, G.; Seidman, A.D. Combination versus sequential single-agent therapy in metastatic breast cancer. Oncologist 2002, 7 (Suppl. 6), 13–19. [Google Scholar] [CrossRef] [PubMed]
- Spring, B.; Mai, Z.; Rai, P.; Chang, S.; Hasan, T. Theranostic nanocells for simultaneous imaging and photodynamic therapy of pancreatic cancer. In Optical Methods for Tumor Treatment and Detection: Mechanisms and Techniques in Photodynamic Therapy XIX; International Society for Optics and Photonics: Bellingham, WA, USA, 2010. [Google Scholar]
- Zheng, L.Z.; Rai, P.; Mai, Z.; Spring, B.Q.; Hasan, T. Simultaneous Targeting of EGFR and MET Pathways Using Nanotechnology Improves the Treatment Outcomes of Photodynamic Therapy for Pancreatic Cancer; AACR: Philadelphia, PA, USA, 2010. [Google Scholar]
- Mayer, L.D.; Harasym, T.O.; Tardi, P.G.; Shew, C.R.; Johnstone, S.A.; Ramsay, E.C.; Bally, M.B.; Janoff, A.S. Ratiometric dosing of anticancer drug combinations: controlling drug ratios after systemic administration regulates therapeutic activity in tumor-bearing mice. Mol. Cancer Ther. 2006, 5, 1854–1863. [Google Scholar] [CrossRef] [PubMed]
- Herrlinger, U.; Tzaridis, T.; Mack, F.; Steinbach, J.; Schlegel, U.; Sabel, M.; Hau, P.; Kortman, R.-D.; Krex, D.; Grauer, O.; et al. ACTR-58. Phase III trial of CCNU/temozolomide (TMZ) combination therapy vs. standard TMZ therapy for newly diagnosed MGMT-methylated glioblastoma patients: The CeTeg/NOA-09 trial. Neuro-Oncology 2017, 19 (Suppl. 6), vi13–vi14. [Google Scholar] [CrossRef]
- Van Leeuwen, R.W.F.; Brundel, D.H.S.; Neef, C.; van Gelder, T.; Mathijssen, R.H.J.; Burger, D.M.; Jansman, F.G.A. Prevalence of potential drug-drug interactions in cancer patients treated with oral anticancer drugs. Br. J. Cancer 2013, 108, 1071–1078. [Google Scholar] [CrossRef] [PubMed]
- Suri, S.S.; Fenniri, H.; Singh, B. Nanotechnology-based drug delivery systems. J. Occup. Med. Toxicol. 2007, 2, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moghimi, S.M.; Porter, C.; Muir, I.; Illum, L.; Davis, S. Non-phagocytic uptake of intravenously injected microspheres in rat spleen: Influence of particle size and hydrophilic coating. Biochem. Biophys. Res. Commun. 1991, 177, 861–866. [Google Scholar] [CrossRef]
- Hu, K.; Shi, Y.; Jiang, W.; Han, J.; Huang, S.; Jiang, X. Lactoferrin conjugated PEG-PLGA nanoparticles for brain delivery: Preparation, characterization and efficacy in Parkinson’s disease. Int. J. Pharm. 2011, 415, 273–283. [Google Scholar] [CrossRef] [PubMed]
- Sosnovik, D.E.; Nahrendorf, M.; Weissleder, R. Magnetic nanoparticles for MR imaging: Agents, techniques and cardiovascular applications. Basic Res. Cardiol. 2008, 103, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Valdivia, J.U.; Ibarra, M.G.; Fernández, R.P.; Viloria, A.; Higuera, T.; Laborda, A.; García, A.; García de Jalón, J.A.; Gutiérrez, M.; Romero, M.S.; et al. Research study on renal targeted chemotherapy with magnetic harpoons and intravenous administration of ferro-carbon nanoparticles. Arch. Esp. Urol. 2007, 60, 5–14. [Google Scholar]
- Senapati, S.; Mahanta, A.K.; Kumar, S.; Maiti, P. Controlled drug delivery vehicles for cancer treatment and their performance. Signal Transduct. Target. Ther. 2018, 3, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velpurisiva, P.; Piel, B.P.; Lepine, J.; Rai, P. GSK461364A, a Polo-Like Kinase-1 Inhibitor Encapsulated in Polymeric Nanoparticles for the Treatment of Glioblastoma Multiforme (GBM). Bioengineering (Basel) 2018, 5, 83. [Google Scholar] [CrossRef] [PubMed]
- Saraiva, C.; Praça, C.; Ferreira, R.; Santos, T.; Ferreira, L.; Bernardino, L. Nanoparticle-mediated brain drug delivery: Overcoming blood-brain barrier to treat neurodegenerative diseases. J. Control. Release 2016, 235, 34–47. [Google Scholar] [CrossRef] [PubMed]
- Law, M.E.; Templeton, K.L.; Kitange, G.; Smith, J.; Misra, A.; Feuerstein, B.G.; Jenkins, R.B. Molecular cytogenetic analysis of chromosomes 1 and 19 in glioma cell lines. Cancer Genet. Cytogenet. 2005, 160, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Mishra, P.; Nayak, B.; Dey, R. PEGylation in anti-cancer therapy: An overview. Asian J. Pharm. Sci. 2016, 11, 337–348. [Google Scholar] [CrossRef] [Green Version]
- Fessi, H.; Puisieux, F.; Devissaguet, J.; Ammoury, N.; Benita, S. Nanocapsule formation by interfacial polymer deposition following solvent displacement. Int. J. Pharm. 1989, 55, R1–R4. [Google Scholar] [CrossRef]
- Zhang, Y.; Huo, M.; Zhou, J.; Zou, A.; Li, W.; Yao, C.; Xie, S. DDSolver: An add-in program for modeling and comparison of drug dissolution profiles. AAPS J. 2010, 12, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Yang, X. Clonogenic Assay; Nature Protocols: London, UK, 2006. [Google Scholar]
- Moore, T.L.; Hirsch, V.; Urban, D.; Jud, C.; Balog, S.; Lattuada, M.; Rodriguez-Lorenzo, L.; Rothen-Rutishauser, B.; Petri-Fink, A. Nanoparticle colloidal stability in cell culture media and impact on cellular interactions. Chem. Soc. Rev. 2015, 44, 6287–6305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gref, R.; Luck, M.; Quellec, P.; Marchand, M.; Dellacherie, É.; Harnisch, S.; Blunk, T.; Müller, R. ‘Stealth’ corona-core nanoparticles surface modified by polyethylene glycol (PEG): Influences of the corona (PEG chain length and surface density) and of the core composition on phagocytic uptake and plasma protein adsorption. Colloids Surf B Biointerfaces 2000, 18, 301–313. [Google Scholar] [CrossRef]
- Owens, D.E., 3rd; Peppas, N.A. Opsonization, biodistribution, and pharmacokinetics of polymeric nanoparticles. Int. J. Pharm. 2006, 307, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Zambito, Y.; Pedreschi, E.; di Colo, G. Is dialysis a reliable method for studying drug release from nanoparticulate systems?—A case study. Int. J. Pharm. 2012, 434, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Costa, P.; Lobo, J.M.S. Evaluation of mathematical models describing drug release from estradiol transdermal systems. Drug Dev. Ind. Pharm. 2003, 29, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Ramteke, K.H.; Dighe, P.A.; Kharat, A.R.; Patil, S.V. Mathematical models of drug dissolution: A review. Sch. Acad. J. Pharm. 2014, 3, 388–396. [Google Scholar]
- Franken, N.A.; Rodermond, H.M.; Stap, J.; Haveman, J.; Van Bree, C. Clonogenic assay of cells in vitro. Nat. Protoc. 2006, 1, 2315–2319. [Google Scholar] [CrossRef] [PubMed]
- Aryal, S.; Hu, C.M.; Zhang, L. Polymeric nanoparticles with precise ratiometric control over drug loading for combination therapy. Mol. Pharm. 2011, 8, 1401–1407. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Tao, R.; Ding, D.; Kong, D.; Fan, A.; Wang, Z.; Zhao, Y. Ratiometric co-delivery of multiple chemodrugs in a single nanocarrier. Eur. J. Pharm. Sci. 2017, 107, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Miao, L.; Guo, S.; Zhang, J.; Kim, W.Y.; Huang, L. Nanoparticles with Precise Ratiometric Co-Loading and Co-Delivery of Gemcitabine Monophosphate and Cisplatin for Treatment of Bladder Cancer. Adv. Funct. Mater. 2014, 24, 6601–6611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lammers, T.; Subr, V.; Ulbrich, K.; Peschke, P.; Huber, P.E.; Hennink, W.E.; Storm, G. Simultaneous delivery of doxorubicin and gemcitabine to tumors in vivo using prototypic polymeric drug carriers. Biomaterials 2009, 30, 3466–3475. [Google Scholar] [CrossRef] [PubMed]
- Bae, Y.; Diezi, T.A.; Zhao, A.; Kwon, G.S. Mixed polymeric micelles for combination cancer chemotherapy through the concurrent delivery of multiple chemotherapeutic agents. J. Control. Release 2007, 122, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, S.; Eavarone, D.; Capila, I.; Zhao, G.; Watson, N.; Kiziltepe, T.; Sasisekharan, R. Temporal targeting of tumour cells and neovasculature with a nanoscale delivery system. Nature 2005, 436, 568–572. [Google Scholar] [CrossRef] [PubMed]
- Jain, K. Use of nanoparticles for drug delivery in glioblastoma multiforme. Expert Rev. Neurother. 2007, 7, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Premkumar, D.R.; Arnold, B.; Pollack, I.F. Cooperative inhibitory effect of ZD1839 (Iressa) in combination with 17-AAG on glioma cell growth. Mol. Carcinog. 2006, 45, 288–301. [Google Scholar] [CrossRef] [PubMed]
- Ohno, S.; Nishi, T.; Kojima, Y.; Haraoka, J.; Ito, H.; Mizuguchi, J. Combined stimulation with interferon alpha and retinoic acid synergistically inhibits proliferation of the glioblastoma cell line GB12. Neurol. Res. 2002, 24, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Mu, L.; Wang, T.; Chen, Y.; Tang, X.; Yuan, Y.; Zhao, Y. Beta-Elemene enhances the efficacy of gefitinib on glioblastoma multiforme cells through the inhibition of the EGFR signaling pathway. Int. J. Oncol. 2016, 49, 1427–1436. [Google Scholar] [CrossRef] [PubMed]
- Lam, F.C.; Morton, S.W.; Wyckoff, J.; Han, T.L.; Hwang, M.K.; Maffa, A.; Balkanska-Sinclair, E.; Yaffe, M.B.; Floyd, S.R.; Hammond, P.T. Enhanced efficacy of combined temozolomide and bromodomain inhibitor therapy for gliomas using targeted nanoparticles. Nat. Commun. 2018, 9, 1991. [Google Scholar] [CrossRef] [PubMed]
- Rich, J.N.; Reardon, D.A.; Peery, T.; Dowell, J.M.; Quinn, J.A.; Penne, K.L.; Wikstrand, C.J.; Van Duyn, L.B.; Dancey, J.E.; McLendon, R.E.; et al. Phase II trial of gefitinib in recurrent glioblastoma. J. Clin. Oncol. 2004, 22, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Du, C.; Qi, Y.; Zhang, Y.; Wang, Y.; Zhao, X.; Min, H.; Han, X.; Lang, J.; Qin, H.; Shi, Q.; et al. Epidermal Growth Factor Receptor-Targeting Peptide Nanoparticles Simultaneously Deliver Gemcitabine and Olaparib to Treat Pancreatic Cancer with Breast Cancer 2 (BRCA2) Mutation. ACS Nano 2018, 12, 10785–10796. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Xu, L.; Liang, C.; Wang, C.; Peng, R.; Liu, Z. Photothermal therapy with immune-adjuvant nanoparticles together with checkpoint blockade for effective cancer immunotherapy. Nat. Commun. 2016, 7, 13193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Schwerbrock, N.M.; Rogers, A.B.; Kim, W.Y.; Huang, L. Codelivery of VEGF siRNA and gemcitabine monophosphate in a single nanoparticle formulation for effective treatment of NSCLC. Mol. Ther. 2013, 21, 1559–1569. [Google Scholar] [CrossRef] [PubMed]
- Rai, P.; Chang, S.K.; Mai, Z.; Neuman, D.; Hasan, T. Nanotechnology-based combination therapy improves treatment response in cancer models. In Photodynamic Therapy: Back to the Future; International Society for Optics and Photonics: Bellingham, WA, USA, 2009. [Google Scholar]
- McGinnity, D.F.; Riley, R.J. Predicting drug pharmacokinetics in humans from in vitro metabolism studies. Biochem. Soc. Trans. 2001, 29 Pt 2, 135–139. [Google Scholar] [CrossRef]
- Di Maio, M.; Chiodini, P.; Georgoulias, V.; Hatzidaki, D.; Takeda, K.; Wachters, F.M.; Gebbia, V.; Smit, E.F.; Morabito, A.; Gallo, C.; et al. Meta-analysis of single-agent chemotherapy compared with combination chemotherapy as second-line treatment of advanced non-small-cell lung cancer. J. Clin. Oncol. 2009, 27, 1836–1843. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nanoparticle Type | Mean Hydrodynamic Size (nm) | PDI | Zeta Potential (mV) | Molar Ratio of Gefitinib: GSK461364A | % Encapsulation Efficiency | |
|---|---|---|---|---|---|---|
| PLGA-PEG (empty NPs) | 127.0 ± 0.3464 | 0.097 ± 0.005 | −35.5 ± 5.90 | N/A | N/A | |
| Gef NPs | 116.8 ± 1.62 | 0.120 ± 0.6576 | −23.4 ± 0.707 | N/A | 68.34 ± 6.438 | |
| GSK461364A NPs | 120.5 ± 2.483 | 0.115 ± 0.004 | −25.6 ± 0.451 | N/A | 56.29 ± 4.319 [37] | |
| Combo NPs | 101.29 ± 2.412 | 0.102 ± 0.034 | −24.65 ± 1.943 | 1:1 | 26 ± 8.98 gefitinib | 35 ± 5.34 GSK461364A |
| Final Polymer Concentration (mg/mL) | Mean Hydrodynamic Size (nm) | PDI | Average Zeta Potential (mV) | % Encapsulation Efficiency | |
|---|---|---|---|---|---|
| Gefitinib | GSK461364A | ||||
| 2.5 | Synthesis Unsuccessful | ||||
| 5 | 408.25 ± 48.98 | 0.239 | −24.5 ± 0.458 | 6.65 ± 4.45 | None |
| 10 | 101.29 ± 2.412 | 0.133 | −29.6 ± 0.777 | 70.11± 6.33 | 65.74 ± 10.85 |
| Molar Ratio of Gefitinib:GSK461364A | (2.16–3):1 | (3.6–4.35):1 | 7:1 | 9:1 |
| Encapsulated gefitinib (µM) | 1146.88 | 1959.26 | 1294.79 | 590.51 |
| Encapsulated GSK461364A (µM) | 386.28 | 508.18 | 184.27 | 66.38 |
| Size (nm) | 160 ± 21.385 | 141.04 ± 25.156 | 142.8 ± 14.153 | 129.75 ± 22.69 |
| PDI | 0.15 ± 0.0487 | 0.146 ± 0.052 | 0.168 ± 0.044 | 0.154 ± 0.045 |
| Zeta potential (mV) | −20.44 ± 3.069 | −20.867 ± 4.055 | −19.78 ± 2.252 | −20.25 ± 7.848 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velpurisiva, P.; Rai, P. Synergistic Action of Gefitinib and GSK41364A Simultaneously Loaded in Ratiometrically-Engineered Polymeric Nanoparticles for Glioblastoma Multiforme. J. Clin. Med. 2019, 8, 367. https://doi.org/10.3390/jcm8030367
Velpurisiva P, Rai P. Synergistic Action of Gefitinib and GSK41364A Simultaneously Loaded in Ratiometrically-Engineered Polymeric Nanoparticles for Glioblastoma Multiforme. Journal of Clinical Medicine. 2019; 8(3):367. https://doi.org/10.3390/jcm8030367
Chicago/Turabian StyleVelpurisiva, Praveena, and Prakash Rai. 2019. "Synergistic Action of Gefitinib and GSK41364A Simultaneously Loaded in Ratiometrically-Engineered Polymeric Nanoparticles for Glioblastoma Multiforme" Journal of Clinical Medicine 8, no. 3: 367. https://doi.org/10.3390/jcm8030367