
Cranial MRI beyond the Neonatal Period and Neurodevelopmental Outcomes in Neonatal Encephalopathy Due to Perinatal Asphyxia: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources and Search Strategy
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Synthesis of Results
3. Results
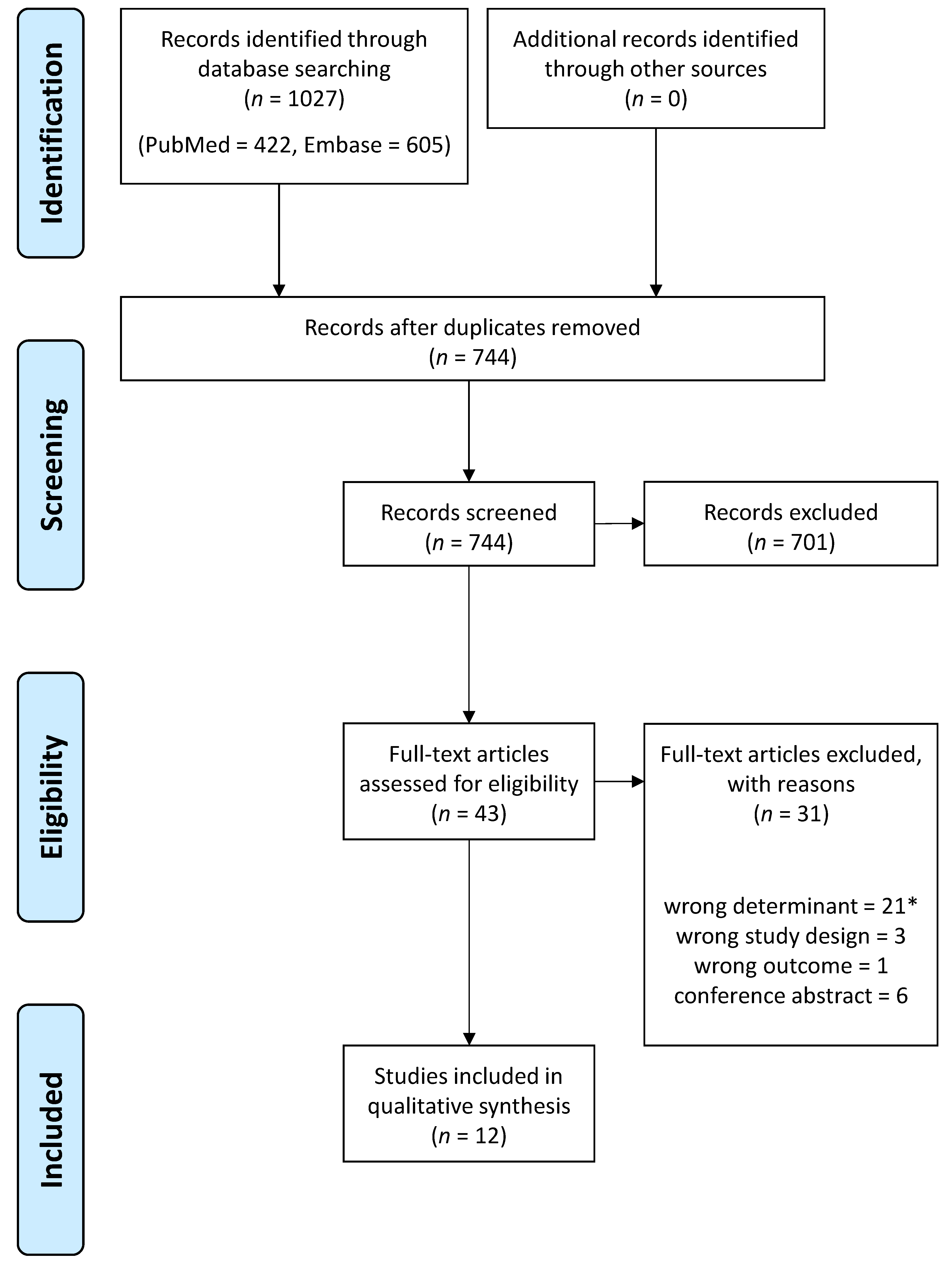
3.1. Article Search
3.2. Study Characteristics
3.3. MRI at 2–18 Months
3.3.1. Composite Adverse Outcomes
3.3.2. Motor Outcomes
3.3.3. Cognitive Outcomes
3.3.4. Epilepsy
3.3.5. Audiovisual Impairment
3.4. MRI at 18–24 Months
3.5. Neonatal MRI versus Later MRI
3.6. Therapeutic Hypothermia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy
Appendix A.1. PubMed
- (Brain Hypoxia-Ischemia*[Title/Abstract] OR Brain Ischemia Hypoxia[Title/Abstract] OR Brain Hypoxia-Ischaemia*[Title/Abstract] OR Brain Ischaemia Hypoxia[Title/Abstract] OR Ischemic-Hypoxic Encephalopath*[Title/Abstract] OR Cerebral Hypoxia Ischemia*[Title/Abstract] OR Cerebral Hypoxia Ischaemia*[Title/Abstract] OR Cerebral Ischemia Hypoxia*[Title/Abstract] OR Cerebral Ischaemia Hypoxia*[Title/Abstract] OR Brain Anoxia-Ischemia*[Title/Abstract] OR Brain Ischemia Anoxia*[Title/Abstract] OR Cerebral Ischemia Anoxia*[Title/Abstract] OR “Asphyxia Neonatorum”[Mesh] OR “Asphyxia”[MeSH Terms] OR asphyx*[Title/Abstract] OR “hypoxia ischemia, brain”[MeSH Terms] OR hypoxic-ischemic encephalopathy[Title/Abstract] OR hypoxic-ischaemic encephalopathy[Title/Abstract]) AND (“Magnetic Resonance Imaging”[MeSH Terms] OR “magnetic resonance imag*”[Title/Abstract] OR MRI[Title/Abstract]) AND (“Infant, Newborn”[Mesh] OR “Infant”[MeSH Terms] OR infant*[Title/Abstract] OR newborn*[Title/Abstract] OR baby[Title/Abstract] OR neonat*[Title/Abstract] OR babies[Title/Abstract]) AND (Serial* OR follow-up OR repeat* OR late mri OR evolution* OR transformation* OR evolv*)
Appendix A.2. Embase
- (‘Infant’/exp OR ‘infant*’:ti,ab,kw OR ‘newborn*’:ti,ab,kw OR ‘baby’:ti,ab,kw OR ‘neonat*’:ti,ab,kw OR ‘babies’:ti,ab,kw) AND (‘Brain Hypoxia-Ischemia*’:ti,ab,kw OR ‘Brain Ischemia Hypoxia’:ti,ab,kw OR ‘Brain Hypoxia-Ischaemia*’:ti,ab,kw OR ‘Brain Ischaemia Hypoxia’:ti,ab,kw OR ‘Ischemic-Hypoxic Encephalopath*’:ti,ab,kw OR ‘Cerebral Hypoxia Ischemia*’:ti,ab,kw OR ‘Cerebral Hypoxia Ischaemia*’:ti,ab,kw OR ‘Cerebral Ischemia Hypoxia*’:ti,ab,kw OR ‘Cerebral Ischaemia Hypoxia*’:ti,ab,kw OR ‘Brain Anoxia-Ischemia*’:ti,ab,kw OR ‘Brain Ischemia Anoxia*’:ti,ab,kw OR ‘Cerebral Ischemia Anoxia*’:ti,ab,kw OR ‘asphyxia’/exp OR ‘asphyx*’:ti,ab,kw OR ‘hypoxic-ischemic encephalopathy’:ti,ab,kw OR ‘hypoxic-ischaemic encephalopathy’:ti,ab,kw OR ‘hypoxic ischaemic’:ti,ab,kw OR ‘hypoxic ischemic’:ti,ab,kw) AND (‘nuclear magnetic resonance’/exp OR ‘magnetic resonance imag*’:ti,ab,kw OR ‘MRI’:ti,ab,kw) AND (‘serial*’:ti,ab,kw OR ‘follow-up’:ti,ab,kw OR ‘repeat*’:ti,ab,kw OR ‘late MRI’:ti,ab,kw OR ‘evolution*’:ti,ab,kw OR ‘transformation*’:ti,ab,kw OR ‘evolv*’:ti,ab,kw)
Appendix B

{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | Overall Quality | |
|---|---|---|---|---|---|---|---|
| Parmentier, 2023 [10] | LR | LR | LR | MR | LR | LR | High |
| Jose, 2013 [19] | MR | LR | LR | MR | MR | LR | High |
| Spring in ‘t Veld, 2016 [20] | MR | LR | LR | MR | HR | LR | Moderate |
| Mulkey, 2012 [21] | MR | LR | LR | HR | HR | MR | Moderate |
| Belet, 2004 [22] | MR | LR | LR | LR | HR | LR | Moderate |
| Tekgul. 2003 [23] | MR | LR | LR | MR | HR | HR | Moderate |
| Krägeloh-Mann, 2002 [16] | MR | LR | LR | MR | HR | HR | Moderate |
| Byrne, 1990 [25] | MR | LR | MR | MR | HR | HR | Moderate |
| Millet, 1998 [18] | HR | LR | LR | MR | HR | HR | Low |
| Fujii, 1993 [17] | HR | LR | LR | HR | HR | MR | Low |
| Rutherford, 1996 [26] | HR | LR | LR | MR | HR | HR | Low |
| Steinlin, 1991 [24] | MR | MR | MR | HR | HR | HR | Low |
References
- Lee, A.C.C.; Kozuki, N.; Blencowe, H.; Vos, T.; Bahalim, A.; Darmstadt, G.L.; Niermeyer, S.; Ellis, M.; Robertson, N.J.; Cousens, S.; et al. Intrapartum-related neonatal encephalopathy incidence and impairment at regional and global levels for 2010 with trends from 1990. Pediatr. Res. 2013, 74, 50–72. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, S.E.; Berg, M.; Hunt, R.; Tarnow-Mordi, W.O.; Inder, T.E.; Davis, P.G. Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst. Rev. 2013, CD003311. [Google Scholar] [CrossRef] [PubMed]
- Grossmann, K.R.; Westblad, M.E.; Blennow, M.; Lindstrom, K. Outcome at early school age and adolescence after hypothermia-treated hypoxic-ischaemic encephalopathy: An observational, population-based study. Arch. Dis. Child-Fetal 2023, 108, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Annink, K.V.; de Vries, L.S.; Groenendaal, F.; Eijsermans, R.; Mocking, M.; van Schooneveld, M.M.J.; Dudink, J.; van Straaten, H.L.M.; Benders, M.; Lequin, M.; et al. Mammillary body atrophy and other MRI correlates of school-age outcome following neonatal hypoxic-ischemic encephalopathy. Sci. Rep. 2021, 11, 5017. [Google Scholar] [CrossRef] [PubMed]
- Wisnowski, J.L.; Wintermark, P.; Bonifacio, S.L.; Smyser, C.D.; Barkovich, A.J.; Edwards, A.D.; de Vries, L.S.; Inder, T.E.; Chau, V.; Newborn Brain Society, G.; et al. Neuroimaging in the term newborn with neonatal encephalopathy. Semin. Fetal Neonatal Med. 2021, 26, 101304. [Google Scholar] [CrossRef] [PubMed]
- Bednarek, N.; Mathur, A.; Inder, T.; Wilkinson, J.; Neil, J.; Shimony, J. Impact of therapeutic hypothermia on MRI diffusion changes in neonatal encephalopathy. Neurology 2012, 78, 1420–1427. [Google Scholar] [CrossRef] [PubMed]
- Weeke, L.C.; Groenendaal, F.; Mudigonda, K.; Blennow, M.; Lequin, M.H.; Meiners, L.C.; van Haastert, I.C.; Benders, M.J.; Hallberg, B.; de Vries, L.S. A Novel Magnetic Resonance Imaging Score Predicts Neurodevelopmental Outcome after Perinatal Asphyxia and Therapeutic Hypothermia. J. Pediatr. 2018, 192, 33–40.e2. [Google Scholar] [CrossRef]
- Cheong, J.L.; Coleman, L.; Hunt, R.W.; Lee, K.J.; Doyle, L.W.; Inder, T.E.; Jacobs, S.E.; Infant Cooling Evaluation, C. Prognostic utility of magnetic resonance imaging in neonatal hypoxic-ischemic encephalopathy: Substudy of a randomized trial. Arch. Pediatr. Adolesc. Med. 2012, 166, 634–640. [Google Scholar] [CrossRef]
- de Vries, L.S.; Groenendaal, F. Patterns of neonatal hypoxic-ischaemic brain injury. Neuroradiology 2010, 52, 555–566. [Google Scholar] [CrossRef]
- Parmentier, C.E.J.; Lequin, M.H.; Alderliesten, T.; Swanenburg de Veye, H.F.N.; van der Aa, N.E.; Dudink, J.; Benders, M.; Harteman, J.C.; Koopman-Esseboom, C.; Groenendaal, F.; et al. Additional Value of 3-Month Cranial Magnetic Resonance Imaging in Infants with Neonatal Encephalopathy following Perinatal Asphyxia. J. Pediatr. 2023, 258, 113402. [Google Scholar] [CrossRef]
- Rutherford, M.A.; Pennock, J.M.; Schwieso, J.E.; Cowan, F.M.; Dubowitz, L.M.S. Hypoxic-Ischemic Encephalopathy—Early Magnetic-Resonance-Imaging Findings and Their Evolution. Neuropediatrics 1995, 26, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Welker, K.M.; Patton, A. Assessment of normal myelination with magnetic resonance imaging. Semin. Neurol. 2012, 32, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Riley, R.D.; Moons, K.G.M.; Snell, K.I.E.; Ensor, J.; Hooft, L.; Altman, D.G.; Hayden, J.; Collins, G.S.; Debray, T.P.A. A guide to systematic review and meta-analysis of prognostic factor studies. BMJ 2019, 364, k4597. [Google Scholar] [CrossRef] [PubMed]
- Hayden, J.A.; Cote, P.; Bombardier, C. Evaluation of the quality of prognosis studies in systematic reviews. Ann. Intern. Med. 2006, 144, 427–437. [Google Scholar] [CrossRef]
- Krageloh-Mann, I.; Helber, A.; Mader, I.; Staudt, M.; Wolff, M.; Groenendaal, F.; DeVries, L. Bilateral lesions of thalamus and basal ganglia: Origin and outcome. Dev. Med. Child. Neurol. 2002, 44, 477–484. [Google Scholar] [CrossRef]
- Fujii, Y.; Konishi, Y.; Kuriyama, M.; Maeda, M.; Saito, M.; Ishii, Y.; Sudo, M. MRI assessment of myelination patterns in high-risk infants. Pediatr. Neurol. 1993, 9, 194–197. [Google Scholar] [CrossRef]
- Millet, V.; Bartoli, J.M.; Lacroze, V.; Raybaud, C.; Unal, D.; Girard, N. Predictive significance of magnetic resonance imaging at 4 months of adjusted age in infants after a perinatal neurologic insult. Biol. Neonate 1998, 73, 207–219. [Google Scholar] [CrossRef]
- Jose, A.; Matthai, J.; Paul, S. Correlation of EEG, CT, and MRI Brain with Neurological Outcome at 12 Months in Term Newborns with Hypoxic Ischemic Encephalopathy. J. Clin. Neonatol. 2013, 2, 125–130. [Google Scholar] [CrossRef]
- Spring In ‘‘t Veld, L.G.; de Vries, L.S.; Alderliesten, T.; Benders, M.J.; Groenendaal, F. Serial 1- and 2-Dimensional Cerebral MRI Measurements in Full-Term Infants after Perinatal Asphyxia. Neonatology 2016, 110, 27–32. [Google Scholar] [CrossRef]
- Mulkey, S.B.; Yap, V.L.; Swearingen, C.J.; Riggins, M.S.; Kaiser, J.R.; Schaefer, G.B. Quantitative cranial magnetic resonance imaging in neonatal hypoxic-ischemic encephalopathy. Pediatr. Neurol. 2012, 47, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Belet, N.; Belet, U.; Incesu, L.; Uysal, S.; Ozinal, S.; Keskin, T.; Sunter, A.T.; Kucukoduk, S. Hypoxic-ischemic encephalopathy: Correlation of serial MRI and outcome. Pediatr. Neurol. 2004, 31, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Tekgul, H.; Serdaroglu, G.; Yalman, O.; Tutuncuoglu, S. Prognostic correlative values of the late-infancy MRI pattern in term infants with perinatal asphyxia. Pediatr. Neurol. 2004, 31, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Steinlin, M.; Dirr, R.; Martin, E.; Boesch, C.; Largo, R.H.; Fanconi, S.; Boltshauser, E. MRI following severe perinatal asphyxia: Preliminary experience. Pediatr. Neurol. 1991, 7, 164–170. [Google Scholar] [CrossRef]
- Byrne, P.; Welch, R.; Johnson, M.A.; Darrah, J.; Piper, M. Serial magnetic resonance imaging in neonatal hypoxic-ischemic encephalopathy. J. Pediatr. 1990, 117, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, M.; Pennock, J.; Schwieso, J.; Cowan, F.; Dubowitz, L. Hypoxic-ischaemic encephalopathy: Early and late magnetic resonance imaging findings in relation to outcome. Arch. Dis. Child. Fetal Neonatal Ed. 1996, 75, F145–F151. [Google Scholar] [CrossRef] [PubMed]
- Krageloh-Mann, I.; Hagberg, G.; Meisner, C.; Schelp, B.; Haas, G.; Eegolofsson, K.E.; Selbmann, H.K.; Hagberg, B.; Michaelis, R. Bilateral Spastic Cerebral-Palsy—A Comparative-Study between South-West Germany and Western Sweden.1. Clinical-Patterns and Disabilities. Dev. Med. Child Neurol. 1993, 35, 1037–1047. [Google Scholar] [CrossRef]
- Largo, R.H.; Molinari, L.; Weber, M.; Comenale Pinto, L.; Duc, G. Early development of locomotion: Significance of prematurity, cerebral palsy and sex. Dev. Med. Child. Neurol. 1985, 27, 183–191. [Google Scholar] [CrossRef]
- Largo, R.H.; Molinari, L.; Comenale Pinto, L.; Weber, M.; Duc, G. Language development of term and preterm children during the first five years of life. Dev. Med. Child. Neurol. 1986, 28, 333–350. [Google Scholar] [CrossRef]
- Barkovich, A.J.; Hajnal, B.L.; Vigneron, D.; Sola, A.; Partridge, J.C.; Allen, F.; Ferriero, D.M. Prediction of neuromotor outcome in perinatal asphyxia: Evaluation of MR scoring systems. AJNR Am. J. Neuroradiol. 1998, 19, 143–149. [Google Scholar]
- Barkovich, M.J.; Xu, D.; Desikan, R.S.; Williams, C.; Barkovich, A.J. Pediatric neuro MRI: Tricks to minimize sedation. Pediatr. Radiol. 2018, 48, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.L.; Gano, D.; Rogers, E.E.; Xu, D.; Cox, S.; James Barkovich, A.; Li, Y.; Ferriero, D.M.; Glass, H.C. Long-term cognitive outcomes in term newborns with watershed injury caused by neonatal encephalopathy. Pediatr. Res. 2021, 92, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Perez, A.; Ritter, S.; Brotschi, B.; Werner, H.; Caflisch, J.; Martin, E.; Latal, B. Long-term neurodevelopmental outcome with hypoxic-ischemic encephalopathy. J. Pediatr. 2013, 163, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.M.; Walsh, B.H.; Boylan, G.B.; Murray, D.M. Mild hypoxic ischaemic encephalopathy and long term neurodevelopmental outcome—A systematic review. Early Hum. Dev. 2018, 120, 80–87. [Google Scholar] [CrossRef]
- Molloy, E.J.; El-Dib, M.; Juul, S.E.; Benders, M.; Gonzalez, F.; Bearer, C.; Wu, Y.W.; Robertson, N.J.; Hurley, T.; Branagan, A.; et al. Neuroprotective therapies in the NICU in term infants: Present and future. Pediatr. Res. 2023, 93, 1819–1827. [Google Scholar] [CrossRef]
- Tusor, N.; Wusthoff, C.; Smee, N.; Merchant, N.; Arichi, T.; Allsop, J.M.; Cowan, F.M.; Azzopardi, D.; Edwards, A.D.; Counsell, S.J. Prediction of neurodevelopmental outcome after hypoxic-ischemic encephalopathy treated with hypothermia by diffusion tensor imaging analyzed using tract-based spatial statistics. Pediatr. Res. 2012, 72, 63–69. [Google Scholar] [CrossRef]
| Author, Year of Publication | Design | Total No./No. Term PA | GA (w) | Age at Later MRI | Age at Follow-Up | Neurodevelopmental Test | Definition of (Composite) Adverse Outcome | Study Quality |
|---|---|---|---|---|---|---|---|---|
| Parmentier, 2023 [10] | R | 63/63 | ≥36.0 | 2–4 mo (all) 18–24 mo (subset) | 18–24 mo (all) 5.5 y (subset) | 18–24 mo: Bayley-III-NL or GMDS 5.5 y: M-ABC, WPPSI-III-NL | CP, epilepsy, hearing/visual impairment, or neurodevelopmental delay | H |
| Jose, 2013 [19] | P | 31/31 | ≥37.0 | 10–12 weeks | 12 mo | Neurological examination, DDST II | Abnormal neurological exam and/or untestable DDST II | H |
| Spring in ‘t Veld, 2016 [20] | R | 29/29 | ≥36.0 | 3 mo | ≥18 mo | GMDS | CP or neurodevelopmental delay | M |
| Mulkey, 2012 [21] | R | 16/16 | ≥36.0 | 2–18 mo | Median 556 (range 255–1556) days | Neurological examination | Epilepsy, CP, and neurodevelopmental delay | M |
| Belet, 2004 [22] | P | 24/24 | >37.0 | 4 mo 3.5–4 years | 3.5–4 y | Neurological examination, Bayley Scales, and DDST (edition not described) | CP, developmental delay, and epilepsy | M |
| Tekgul, 2003 [23] | R | 65/65 1 | ≥37.0 | 4–12 mo | 2 y | Neurological examination, DDST II | Moderate–severe neurologic abnormalities (causing functional impairment or requiring full-time special assistance) or difficult-to-control post-neonatal seizures | M |
| Kragelöh-Mann, 2002 [16] | R | 17/9 | ≥34.0 | ≥12 mo Subset with PA: 12–18 mo n = 3 18–24 mo n = 2 >24 mo n = 4 | 18 mo–17 y | CP-recorded according to Krägeloh-Mann et al. [27] motor and cognitive development based on milestones by Largo et al. [28,29], and school results if available | Mild motor impairment: walk independently between 18 mo and 5 y, or sit between 10 mo and 2 y; severe motor impairment: unable to walk at 5 y, unable to sit at 2 y, or no head control at 1 y Mild cognitive impairment: developmental milestones < 10th centile and delay < 1 y; severe cognitive impairment: delay > 1 y or not following with eyes/establishing visual contact at age 1 y | M |
| Byrne, 1990 [25] | P | 15/15 | ≥37.0 | 4 mo 8 mo | 18 mo | Neurologic examination of the Collaborative Perinatal Project | CP | M |
| Millet, 1998 [18] | P | 60/15 | ≥25.0 | 3–6 mo CA | 2–5 y | Neurological examination with Amiel–Tison assessment, Bayley Scales, parental interview, and full ophthalmologic and audiologic assessment if screening was abnormal | CP, cognitive impairment (dysphasia/delayed expressive language, ADHD, and lack of visuospatial processing or spatialization), visual disability (strabismus or blindness), developmental delay, and seizures | L |
| Rutherford, 1996 [26] | U | 16/16 | ≥37.0 | 12–24 mo 2 | 12–24 mo | Neurological examination and GMDS | Signs of central motor deficit with or without developmental delay | L |
| Fujii, 1993 [17] | U | 39/U | ≥24.0 | 2–12 mo CA | 18 mo CA | Japanese Edition of DDST and Enjoji Developmental Scale | Neurodevelopmental delay and/or CP | L |
| Steinlin, 1991 [24] | U | 30/30 3 | ≥28.0 | 1–2 mo n = 1 2–18 mo n = 13 18–24 mo n = 2 >24 mo n = 5 | 3–6 mo (n = 7) 6–12 mo (n = 8) 2 y (n = 9) 2–3 y (n = 1) | Neurological examination, GMDS, and Snijders–Oomen nonverbal intelligence test | No definition for adverse outcome. Outcome was described for each infant, including (signs of) CP, neurodevelopmental delay, visual abnormalities, and epilepsy | L |
| Author, Year of Publication | Later MRI Strength, Sequences | Later MRI Assessment | Association between Later MRI and Neurodevelopmental Outcomes |
|---|---|---|---|
| Parmentier, 2023 [10] | 1.5 (n = 27) or 3.0 T (n = 36); T1, T2 | Biometrics: 1D and 2D measurements Qualitative: new injury score including WM, DGM and cerebellum sub-score | Biometrics: smaller DGM surface area (p < 0.001) and frontal horn depth (p < 0.001) on 3-month MRI associated with composite adverse outcomes at 18–24 months; smaller brain width (p = 0.027) associated with composite adverse outcomes at 5.5 years. Qualitative score: WM and DGM sub-scores for 3-month MRI associated with adverse 18–24 month outcomes. Infants with adverse outcomes at 5.5 years had higher DGM sub-scores for later MRI (p = 0.042). Sensitivity, specificity, PPV, and NPV of the 3-month MRI scoring model for composite adverse outcomes at 18–24 months were 65%, 95%, 88%, and 83%. |
| Jose, 2013 [19] | 1.5 T; T1, T2, DWI, SWI | Qualitative: categorization of injury according to Barkovich [30] | Normal later MRI associated with normal outcomes (p < 0.001); abnormal signal in cortex and basal nuclei associated with adverse outcomes (p = 0.002). Sensitivity, specificity, PPV, and NPV of later MRI for abnormal outcomes were respectively 82%, 93%, 60%, and 100%. |
| Spring in ‘t Veld, 2016 [20] | 1.5 or 3.0 T; T1, T2 | Biometrics: 1D and 2D measurements | Smaller cerebellar width (p = 0.025) on 3-month MRI and smaller difference in BG width (p = 0.014), thalamic width (p = 0.012), and BG surface (p = 0.028) between neonatal and 3-month MRI associated with composite adverse outcomes at ≥18 months. |
| Mulkey, 2012 [21] | 1.5 T; T1 | Biometrics: volumetrics of whole brain and corpus callosum | Infants with whole brain volumes < 99% CI boundary of the volume estimation model on later MRI had an OR of 33 to have epilepsy, CP, and neurodevelopmental delay (95% CI 2.32–469.03, p = 0.008); infants with whole brain volumes > 99% CI boundary of the volume estimation model had an OR of 15 to have a normal outcome (95% CI 1.21–185.46, p = 0.029). |
| Belet, 2004 [22] | Field strength NA; T1, T2, PD | Qualitative: categorization by pattern of injury | Four-month MRI associated with epilepsy (p = 0.033), CP (p < 0.001), and composite adverse outcomes (p < 0.001). Sensitivity, specificity, PPV, and NPV for neurological outcomes were, respectively, 86.7%, 100%, 100%, and 81.8%. * |
| Tekgul, 2003 [23] | 1.5 T; T1, T2 | Qualitative: categorization by pattern of injury | Infants with only focal cortical involvement (p = 0.045) or myelination delay (p = 0.019) more frequently had a favorable outcome compared with the other injury patterns. Infants with only myelination delay were less likely to demonstrate a motor deficit (p = 0.016). * |
| Kragelöh-Mann, 2002 [16] | 0.5 or 1.5 T; T1, T2, TSE, FLAIR (subset) | Qualitative: classification of degree of DGM injury | Overall group: severity of DGM injury on MRI ≥ 12 months correlated with motor (p = 0.001) and cognitive development (p < 0.001). Subgroup with asphyxia and MRI at 2–18 months (n = 3): an infant with mild DGM injury had mild motor and cognitive impairment at 15 months. Two infants with severe DGM injury had severe motor and cognitive impairment at, respectively, 27 and 99 months of age. |
| Byrne, 1990 [25] | 1.5 T; T1, T2, IR | Qualitative: assessment of ventricular size, myelination, structural abnormalities, and extracerebral space | Four-month MRI abnormalities were not significantly associated with CP (p = 0.580); 8-month MRI abnormalities were significantly associated with CP: PPV of 80%, NPV of 100%, sensitivity of 100%, and specificity of 67%, p = 0.015. * |
| Millet, 1998 [18] | 1.0 T; T1, T2, PD | Qualitative: assessment of myelination, corpus callosum size, ventricular and subarachnoid space sizes, and morphology of WM/cortex | Subgroup of term infants with perinatal asphyxia (n = 15): diffuse brain injury on later MRI associated with composite abnormal outcomes: PPV of 100%, NPV of 90%, sensitivity of 83%, and specificity of 100%, p = 0.002. * |
| Rutherford, 1996 [26] | 1.0 T; T1, T2, IR, FLAIR (subset) | Qualitative: adapted scoring system for later MRI with separate DGM injury score | Significant correlation between the optimality score for neurological function and the injury score for later MRI (p = 0.0012) and the separate DGM injury score for later MRI (p = 0.0002). |
| Fujii, 1993 [17] | 0.35 or 1.5 T; T1, T2 | Qualitative: assessment of myelination | Overall group: infants with an abnormal outcome (n = 11) more often showed delayed myelination on MRI ≥ 2 months (n = 9, 82%) than infants with a normal outcome (2/13, 15%), p = 0.001. A subgroup analysis for term infants with perinatal asphyxia was not possible. * |
| Steinlin, 1991 [24] | 2.35 T; T1, T2 | Qualitative: assessment of gross morphology, myelination, bleeding, and ventricular size | Diffuse MRI lesions on later MRI were not significantly associated with severe motor abnormalities (p = 0.070) or the composite of mild and severe motor abnormalities (p = 0.192) at follow-up. Numbers were too small to analyze MRI in relation to epilepsy or audiovisual impairment. * |
| Author, Year of Publication | Neonatal MRI Protocol | Age Neonatal MRI | Association between Neonatal MRI Findings and Neurodevelopmental Outcomes | Neonatal versus Later MRI |
|---|---|---|---|---|
| Parmentier, 2023 [10] | T1, T2, DWI, 1H-MRS of BGT, SWI (subset) | <14 days | Biometrics: neonatal MRI not associated with outcome. | Neonatal MRI had better sensitivity and NPV; 3-month MRI had better specificity and PPV. |
| Spring in ‘t Veld, 2016 [20] | T1, T2 | ≤7 days | Qualitative score: total neonatal injury score and neonatal DGM injury sub-score associated with 18–24 month outcomes. Sensitivity, specificity, PPV, and NPV were 67%, 93%, 83%, and 84% for the neonatal DGM sub-score. Infants with adverse 5.5-year outcomes had higher neonatal total (p = 0.045) and DGM sub-scores (p = 0.002) and lower cerebellum injury scores (p = 0.003). | Both neonatal and 3-month MRI biometrics were associated with outcomes. |
| Mulkey, 2012 [21] | T1, DWI | ≤7 days | Infants with an adverse outcome had larger BG and thalamic width (both p < 0.001) and BG surface area (p = 0.007) on neonatal MRIs compared with infants with a favorable outcome. The cerebellar width on neonatal MRIs was larger in the favorable outcome group (p = 0.028). | Both neonatal and later MRI findings were associated with outcomes. |
| Belet, 2004 [22] | T1, T2 | 5–19 days | BG injury on neonatal MRI associated with CP (p = 0.019) and the presence of CP, epilepsy, and delayed neurodevelopment (p = 0.027). Acute brain injury volume in the corpus callosum was associated with epilepsy (OR 24.1, p < 0.030). Whole brain acute injury volume was not associated with unfavorable neurodevelopmental outcomes. | Neonatal MRI had better sensitivity and NPV; 4-month and 4-year MRI had better specificity and PPV. |
| Byrne, 1990 [25] | T1, T2, IR | Not further specified | No significant association between abnormal neonatal MRI (n = 3 infants) and outcome was demonstrated. | Only 8-month MRI was associated with outcomes. |
| Rutherford, 1996 [26] | T1, T2, IR, FLAIR (subset) | ≤4 weeks | Significant correlation between the optimality score for neurological function and the neonatal DGM injury score (p = 0.0004) and the neonatal MRI injury score (p = 0.0034). There was a significant correlation between the neonatal and later DGM injury scores (p = 0.0005) and MRI injury scores (p = 0.0001). | Both neonatal and later MRI findings were associated with outcomes. |
| Fujii, 1993 [17] | T1, T2 | <2 months | No significant association between MRI findings <2 months and neurologic outcome among overall study population (no subgroup analysis for term infants with perinatal asphyxia). | Only myelination on later MRI was correlated with neurologic outcomes. |
| Steinlin, 1991 [24] | T1, T2 | ≤4 days (early) 2–4 weeks (intermediate) | No significant association between abnormal early (n = 6 infants) or intermediate MRI (n = 11 infants) and outcome was demonstrated. | For the overall group with later MRI at 2–75 months, only later MRI was associated with CP (p = 0.031). Neonatal, intermediate, and later MRI at 2–24 months were not associated with outcomes. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parmentier, C.E.J.; Kropman, T.; Groenendaal, F.; Lequin, M.H.; de Vries, L.S.; Benders, M.J.N.L.; Alderliesten, T. Cranial MRI beyond the Neonatal Period and Neurodevelopmental Outcomes in Neonatal Encephalopathy Due to Perinatal Asphyxia: A Systematic Review. J. Clin. Med. 2023, 12, 7526. https://doi.org/10.3390/jcm12247526
Parmentier CEJ, Kropman T, Groenendaal F, Lequin MH, de Vries LS, Benders MJNL, Alderliesten T. Cranial MRI beyond the Neonatal Period and Neurodevelopmental Outcomes in Neonatal Encephalopathy Due to Perinatal Asphyxia: A Systematic Review. Journal of Clinical Medicine. 2023; 12(24):7526. https://doi.org/10.3390/jcm12247526
Chicago/Turabian StyleParmentier, Corline E. J., Tobias Kropman, Floris Groenendaal, Maarten H. Lequin, Linda S. de Vries, Manon J. N. L. Benders, and Thomas Alderliesten. 2023. "Cranial MRI beyond the Neonatal Period and Neurodevelopmental Outcomes in Neonatal Encephalopathy Due to Perinatal Asphyxia: A Systematic Review" Journal of Clinical Medicine 12, no. 24: 7526. https://doi.org/10.3390/jcm12247526