CD19+ CD24hi CD38hi Regulatory B Cells and Memory B Cells in Periodontitis: Association with Pro-Inflammatory and Anti-Inflammatory Cytokines

 ,
, 
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Patient Grouping and Selection Criteria
- Patients with any systemic diseases according to the criteria of Modified Cornell Medical Index [8].
- Patients were receiving antibiotics or non-steroidal anti-inflammatory for at least three months before sample collection.
- Patients subjected to previous periodontal therapy during at least six months.
- Patients suffering from any systemic or local inflammatory disease other than gingivitis or periodontitis.
- Smokers.
- Pregnant and lactating women.
2.3. Sample Collection
2.4. Serum Cytokine Measurements
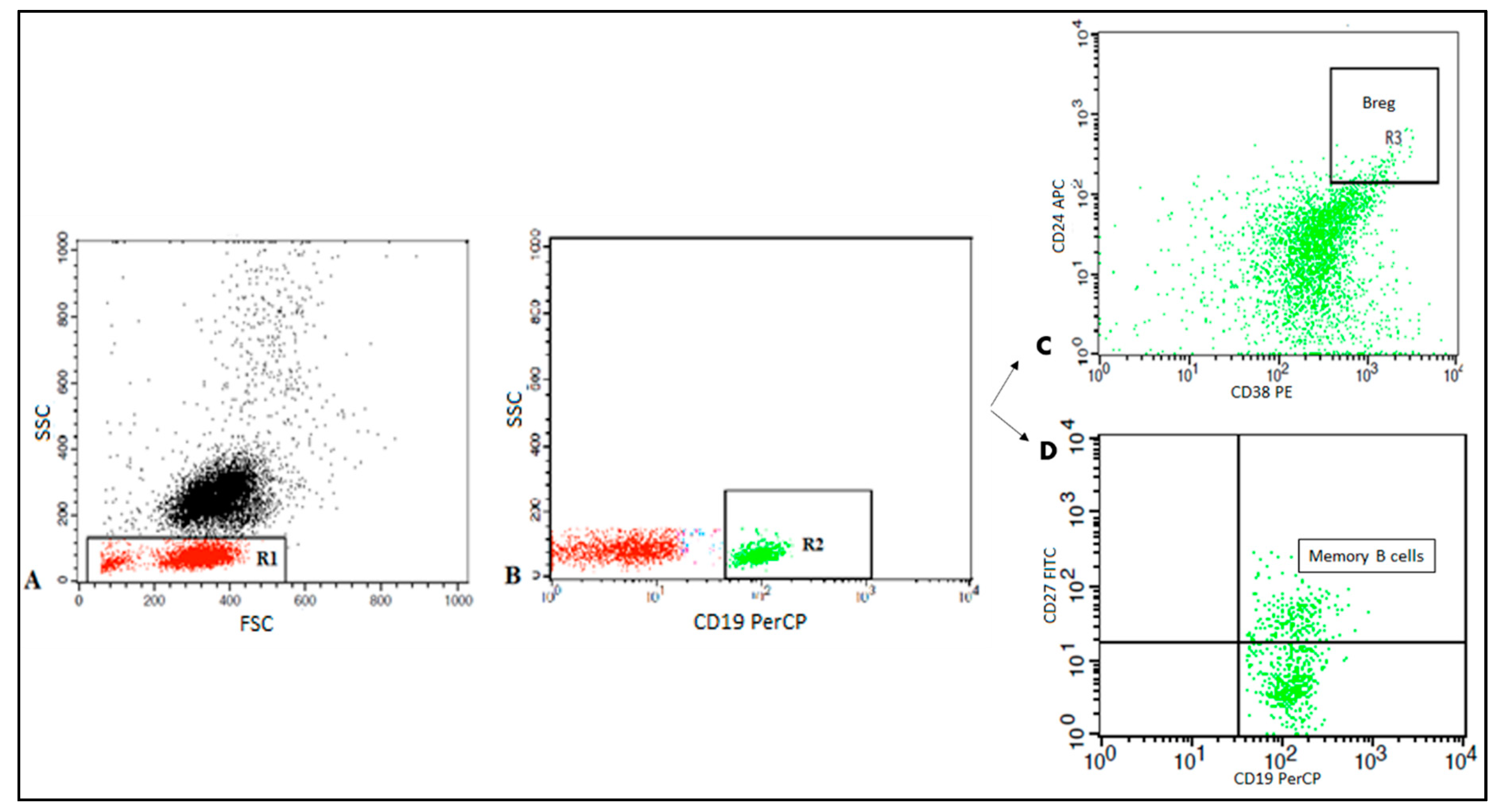
2.5. Flow Cytometric Detection of Regulatory B and Memory B Cells
2.6. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Frequency of CD19+ B Cells, Memory B Cells, and Breg Cells among Periodontitis Patients
3.3. Pro-Inflammatory and Anti-Inflammatory Cytokine Levels in the Studied Groups
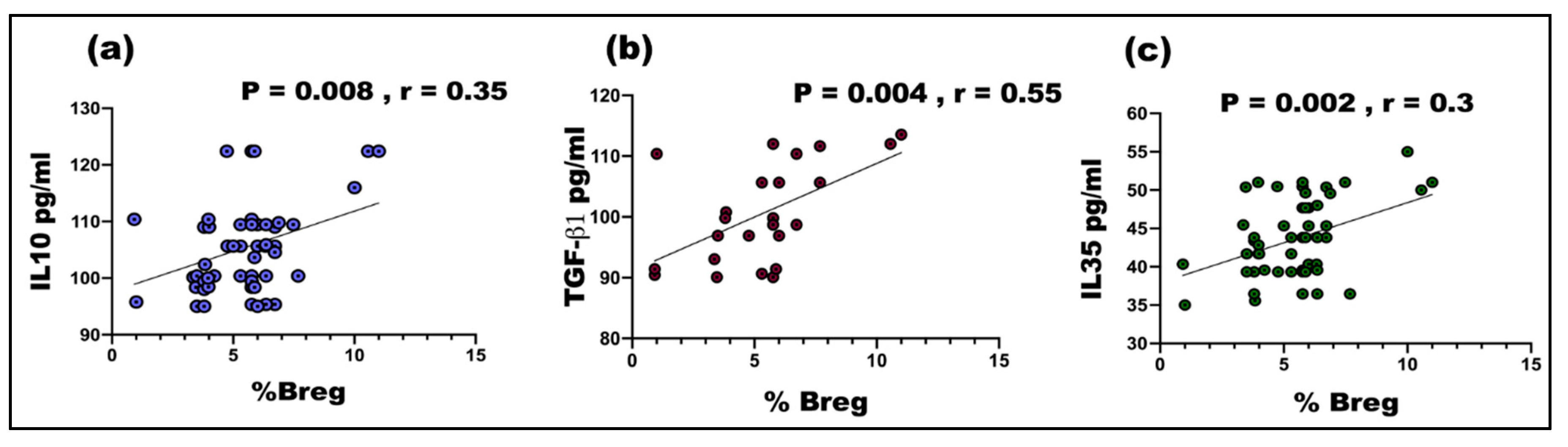
3.4. Correlation between the Frequency of Breg and Serum Cytokines Levels among Periodontitis Patients
4. Discussion
5. Future Recommendations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Luan, X.; Zhou, X.; Naqvi, A.; Francis, M.; Foyle, D.; Nares, S.; Diekwisch, T.G. MicroRNAs and immunity in periodontal health and disease. Int. J. Oral Sci. 2018, 10, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Babay, N.; Alshehri, F.; Al Rowis, R. Majors highlights of the new 2017 classification of periodontal and peri-implant diseases and conditions. Saudi Dent. J. 2019, 31, 303–305. [Google Scholar] [CrossRef] [PubMed]
- Okada, H.; Kida, T.; Yamagami, H. Identification and distribution of immunocompetent cells in inflamed gingiva of human chronic periodontitis. Infect. Immun. 1983, 41, 365–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueredo, C.M.; Lira-Junior, R.; Love, R.M. T and B cells in periodontal disease: New functions in a complex scenario. Int. J. Mol. Sci. 2019, 20, 3949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, M.; Rui, K.; Wang, S.; Lu, L. Regulatory B cells in autoimmune diseases. Cell. Mol. Immunol. 2013, 10, 122–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauri, C.; Menon, M. Human regulatory B cells in health and disease: Therapeutic potential. J. Clin. Investig. 2017, 127, 772–779. [Google Scholar] [CrossRef] [Green Version]
- Armitage, G.C. Development of a classification system for periodontal diseases and conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef]
- Abrumson, G.H. The Cornell medical index as an epidemiological tool. Am. J. Public Health 1966, 65, 287–298 . [Google Scholar] [CrossRef]
- Alrefai, H.; Muhammad, K.; Rudolf, R.; Pham, D.A.T.; Klein-Hessling, S.; Patra, A.K.; Avots, A.; Bukur, V.; Sahin, U.; Tenzer, S.; et al. NFATc1 supports imiquimod-induced skin inflammation by suppressing IL-10 synthesis in B cells. Nat. Commun. 2016, 7, 11724. [Google Scholar] [CrossRef] [Green Version]
- Seymour, G.J.; Powell, R.; Davies, W. The immunopathogenesis of progressive chronic inflammatory periodontal disease. J. Oral Pathol. Med. 1979, 8, 249–265. [Google Scholar] [CrossRef]
- Zouali, M. The emerging roles of B cells as partners and targets in periodontitis. Autoimmunity 2017, 50, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Oliver-Bell, J.; Butcher, J.; Malcolm, J.; MacLeod, M.K.L.; Planell, A.A.; Campbell, L.; Nibbs, R.J.B.; Garside, P.; McInnes, I.; Culshaw, S. Periodontitis in the absence of B cells and specific anti-bacterial antibody. Mol. Oral Microbiol. 2015, 30, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Alsarhan, M.; Benakanakere, M.R.; Maekawa, T.; Kinane, D.F.; Cancro, M.P.; Korostoff, J.M.; Hajishengallis, G. The B cell–stimulatory cytokines BLyS and APRIL are elevated in human periodontitis and are required for B cell–dependent bone loss in experimental murine periodontitis. J. Immunol. 2015, 195, 1427–1435. [Google Scholar] [CrossRef] [PubMed]
- Brecx, M.C.; Schlegel, K.; Gehr, P.; Lang, N.P. Comparison between histological and clinical parameters during human experimental gingivitis. J. Periodontal Res. 1987, 22, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Brecx, M.C.; Gautschi, M.; Gehr, P.; Lang, N.P. Variability of histologic criteria in clinically healthy human gingiva. J. Periodontal Res. 1987, 22, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Demoersman, J.; Pochard, P.; Framery, C.; Simon, Q.; Boisramé, S.; Soueidan, A.; Pers, J.O. B cell subset distribution is altered in patients with severe periodontitis. PLoS ONE 2018, 13, e0192986. [Google Scholar]
- Mahanonda, R.; Champaiboon, C.; Subbalekha, K.; Sa-Ard-Iam, N.; Rattanathammatada, W.; Thawanaphong, S.; Rerkyen, P.; Yoshimura, F.; Nagano, K.; Lang, N.P.; et al. Human memory B cells in healthy gingiva, gingivitis, and periodontitis. J. Immunol. 2016, 197, 715–725. [Google Scholar] [CrossRef] [Green Version]
- Yanaba, K.; Yoshizaki, A.; Asano, Y.; Kadono, T.; Tedder, T.F.; Sato, S. IL-10-producing regulatory B10 cells inhibit intestinal injury in a mouse model. Am. J. Pathol. 2011, 178, 735–743. [Google Scholar] [CrossRef] [Green Version]
- Dai, J.; Bi, L.; Lin, J.; Qi, F. Evaluation of interleukin-10 producing CD19(+) B cells in human gingival tissue. Arch. Oral Biol. 2017, 84, 112–117. [Google Scholar] [CrossRef]
- Hu, Y.; Yu, P.; Yu, X.; Hu, X.; Kawai, T.; Han, X. IL-21/anti-Tim1/CD40 ligand promotes B10 activity in vitro and alleviates bone loss in experimental periodontitis in vivo. Biochim. Biophys. Acta Mol. Basis Dis. 2017, 1863, 2149–2157. [Google Scholar] [CrossRef]
- Wang, Y.; Yu, X.; Lin, J.; Hu, Y.; Zhao, Q.; Kawai, T.; Taubman, M.A.; Han, X. B10 cells alleviate periodontal bone loss in experimental periodontitis. Infect. Immun. 2017, 85. [Google Scholar] [CrossRef] [Green Version]
- Rosser, E.C.; Mauri, C. Regulatory B cells: Origin, phenotype, and function. Immunity 2015, 42, 607–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blair, P.A.; Yassin, L.M.; Flores-Borja, F.; Rawlings, D.J.; A Isenberg, D.; Ehrenstein, M.R.; Mauri, C. CD19+CD24hiCD38hi B cells exhibit regulatory capacity in healthy individuals but are functionally impaired in systemic lupus erythematosus patients. Immunity 2010, 32, 129–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flores-Borja, F.; Bosma, A.; Ng, D.; Reddy, V.; Ehrenstein, M.R.; A Isenberg, D.; Mauri, C. CD19+CD24hiCD38hi B cells maintain regulatory T cells while limiting TH1 and TH17 differentiation. Sci. Transl. Med. 2013, 5, 173ra23. [Google Scholar] [CrossRef]
- Heidari, Z.; Moudi, B.; Mahmoudzadeh-Sagheb, H. Immunomodulatory factors gene polymorphisms in chronic periodontitis: An overview. BMC Oral Health 2019, 19, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinsvoll, S.; Halstensen, T.S.; Schenck, K. Extensive expression of TGF-beta1 in chronically-inflamed periodontal tissue. J. Clin. Periodontol. 1999, 26, 366–373. [Google Scholar] [CrossRef]
- Okada, H.; Murakami, S. Cytokine expression in periodontal health and disease. Crit. Rev. Oral Biol. Med. 1998, 9, 248–266. [Google Scholar] [CrossRef] [Green Version]
- McDevitt, M.J.; Wang, H.-Y.; Knobelman, C.; Newman, M.G.; Di Giovine, F.; Timms, J.; Duff, G.; Kornman, K.S. Interleukin-1 genetic association with periodontitis in clinical practice. J. Periodontol. 2000, 71, 156–163. [Google Scholar] [CrossRef] [Green Version]
- Sattari, M.; Fathiyeh, A.R.; Gholami, F.; Tamijani, H.D.; Samani, M.G. Effect of surgical flap on IL-1beta and TGF-beta concentrations in the gingival crevicular fluid of patients with moderate to severe chronic periodontitis. Iran. J. Immunol. 2011, 8, 20–26. [Google Scholar]
- Vikram, V.; Ramakrishnan, T.; Anilkumar, K.; Ambalavanan, N. Changes in transforming growth factor-β1 in gingival crevicular fluid of patients with chronic periodontitis following periodontal flap surgery. J. Clin. Diagn. Res. 2015, 9, Zc13. [Google Scholar]
- Shen, P.; Roch, T.; Lampropoulou, V.; O’Connor, R.A.; Stervbo, U.; Hilgenberg, E.; Ries, S.; Dang, V.D.; Jaimes, Y.; Daridon, C.; et al. IL-35-producing B cells are critical regulators of immunity during autoimmune and infectious diseases. Nature 2014, 507, 366–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, R.X.; Yu, C.-R.; Dambuza, I.M.; Mahdi, R.M.; Dolinska, M.B.; Sergeev, Y.V.; Wingfield, P.T.; Kim, S.-H.; Egwuagu, C.E.; Sergeey, Y.V. Interleukin-35 induces regulatory B cells that suppress autoimmune disease. Nat. Med. 2014, 20, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.M.; Zhang, X.-H.; Feng, M.-M.; Qiao, Y.-J.; Ye, L.-Q.; Chen, J.; Fan, F.-F.; Guo, L.-L. Interleukin-35 suppresses the antitumor activity of T cells in patients with non-small cell lung cancer. Cell. Physiol. Biochem. 2018, 47, 2407–2419. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameters | Periodontitis Patients (n = 55) | Healthy Controls (n = 20) |
|---|---|---|
| Age (years) mean ± SD | 37.46 ± 4.2 | 35.65 ± 1.6 |
| Gender (male:female) | 32:23 | 13:7 |
| Plaque score (mean) % | 2.2 | 0.58 |
| Bleeding on probing (mean) % | 2.5 | 0.77 |
| Probing depth (PD) mm | 5.4 | 1.4 |
| Clinical attachment loss (CAL) mm | 3.3 | 0 |
| Percentage (%) | Periodontitis Patients (n = 55) | Healthy Controls (n = 20) | p-Value |
|---|---|---|---|
| CD 19+B lymphocytes | 13.92 ± 4.61 | 11.27 ± 3.20 | 0.04 |
| Total memory B cells | 21.68 ± 6.06 | 34.48 ± 5.17 | 0.0001 |
| Breg cells | 5.60 ± 2.59 | 3.78 ± 0.77 | 0.007 |
| Cytokines (pg/mL) | Periodontitis Patients (n = 55) | Healthy Controls (n = 20) | p-Value |
|---|---|---|---|
| Pro-inflammatory cytokines | |||
| IL6 | 125.4 ± 19.03 | 19.03 ± 4.26 | 0.0001 |
| TNF-α | 202.71 ± 103.8 | 11.01 ± 7.77 | 0.0001 |
| IL1β | 84.02 ± 11.77 | 7.03 ± 3.53 | 0.0001 |
| Anti-inflammatory cytokines | |||
| IL10 | 109.4 ± 7.75 | 17.90 ± 5.44 | 0.0001 |
| TGF-β1 | 99.89 ± | 28.26 ± 6.60 | 0.0001 |
| IL35 | 43.06 ± 5.17 | 23.44 ± 3.39 | 0.0001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hetta, H.F.; Mwafey, I.M.; Batiha, G.E.-S.; Alomar, S.Y.; Mohamed, N.A.; Ibrahim, M.A.; Elkady, A.; Meshaal, A.K.; Alrefai, H.; Khodeer, D.M.; et al. CD19+ CD24hi CD38hi Regulatory B Cells and Memory B Cells in Periodontitis: Association with Pro-Inflammatory and Anti-Inflammatory Cytokines. Vaccines 2020, 8, 340. https://doi.org/10.3390/vaccines8020340
Hetta HF, Mwafey IM, Batiha GE-S, Alomar SY, Mohamed NA, Ibrahim MA, Elkady A, Meshaal AK, Alrefai H, Khodeer DM, et al. CD19+ CD24hi CD38hi Regulatory B Cells and Memory B Cells in Periodontitis: Association with Pro-Inflammatory and Anti-Inflammatory Cytokines. Vaccines. 2020; 8(2):340. https://doi.org/10.3390/vaccines8020340
Chicago/Turabian StyleHetta, Helal F., Ibrahim M. Mwafey, Gaber El-Saber Batiha, Suliman Y. Alomar, Nahed A. Mohamed, Maggie A. Ibrahim, Abeer Elkady, Ahmed Kh. Meshaal, Hani Alrefai, Dina M. Khodeer, and et al. 2020. "CD19+ CD24hi CD38hi Regulatory B Cells and Memory B Cells in Periodontitis: Association with Pro-Inflammatory and Anti-Inflammatory Cytokines" Vaccines 8, no. 2: 340. https://doi.org/10.3390/vaccines8020340