
Cross-National Vaccine Concerns and Predictors of Vaccine Hesitancy in Not-Fully Vaccinated Individuals: Findings from USA, Canada, Sweden, and Italy
 , and
, and
Abstract
:1. Introduction
Specific Objectives
- To assess if COVID-19 vaccine related concerns are common across the four countries: USA, Sweden, Italy, and Canada);
- To identify the relationship between the vaccine related concerns and vaccine hesitancy in each country of interest; and,
- To identify and interpret heterogeneity in the relationship between vaccine-related concerns and vaccine hesitancy across the four countries.
2. Materials and Methods
2.1. Data Collection
2.2. Development of the COVID-19 Vaccine Concerns Scales
Item Generation Process
2.3. Concerns about Contracting COVID-19 (“CCC”) Scale
2.4. COVID-19 Vaccine Hesitancy Outcome Measure
2.5. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Objective 1: Vaccine-Related Concerns by Country
3.2.1. Exploratory Factor Analysis
3.2.2. Measurement Invariance Using a Confirmatory Factor Analysis (CFA)
3.2.3. Differential Item Functioning (DIF) Analysis
3.3. Objective 2: Vaccine-Related Hesitancy by Country
3.3.1. Modeling of the Vaccine Hesitancy Outcome
3.3.2. Model Main Effects
3.4. Objective 3: Vaccine Related Concerns Effect on Vaccine Hesitancy including Exploration of Heterogeneity
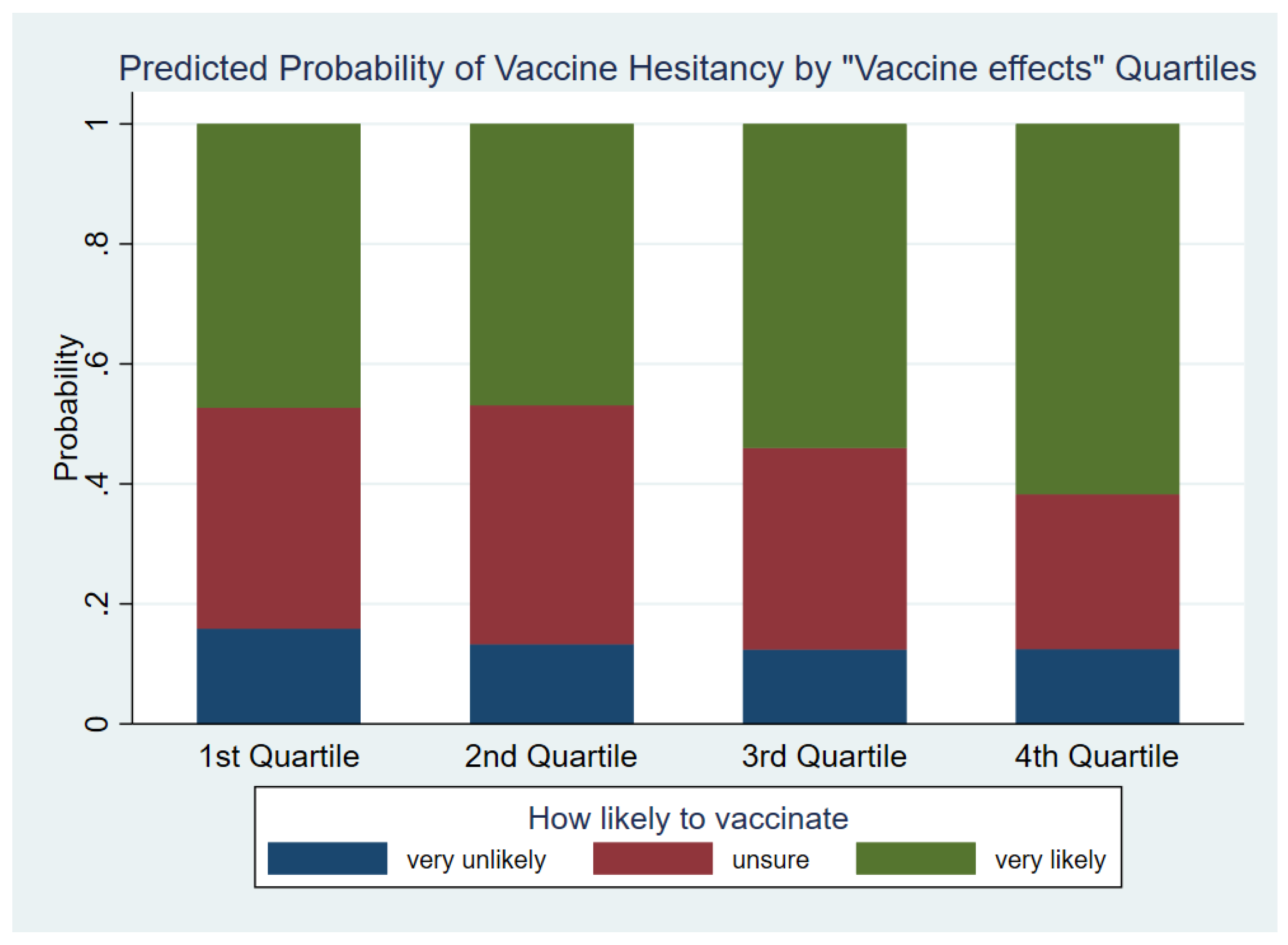
3.4.1. Vaccine Effects Factor
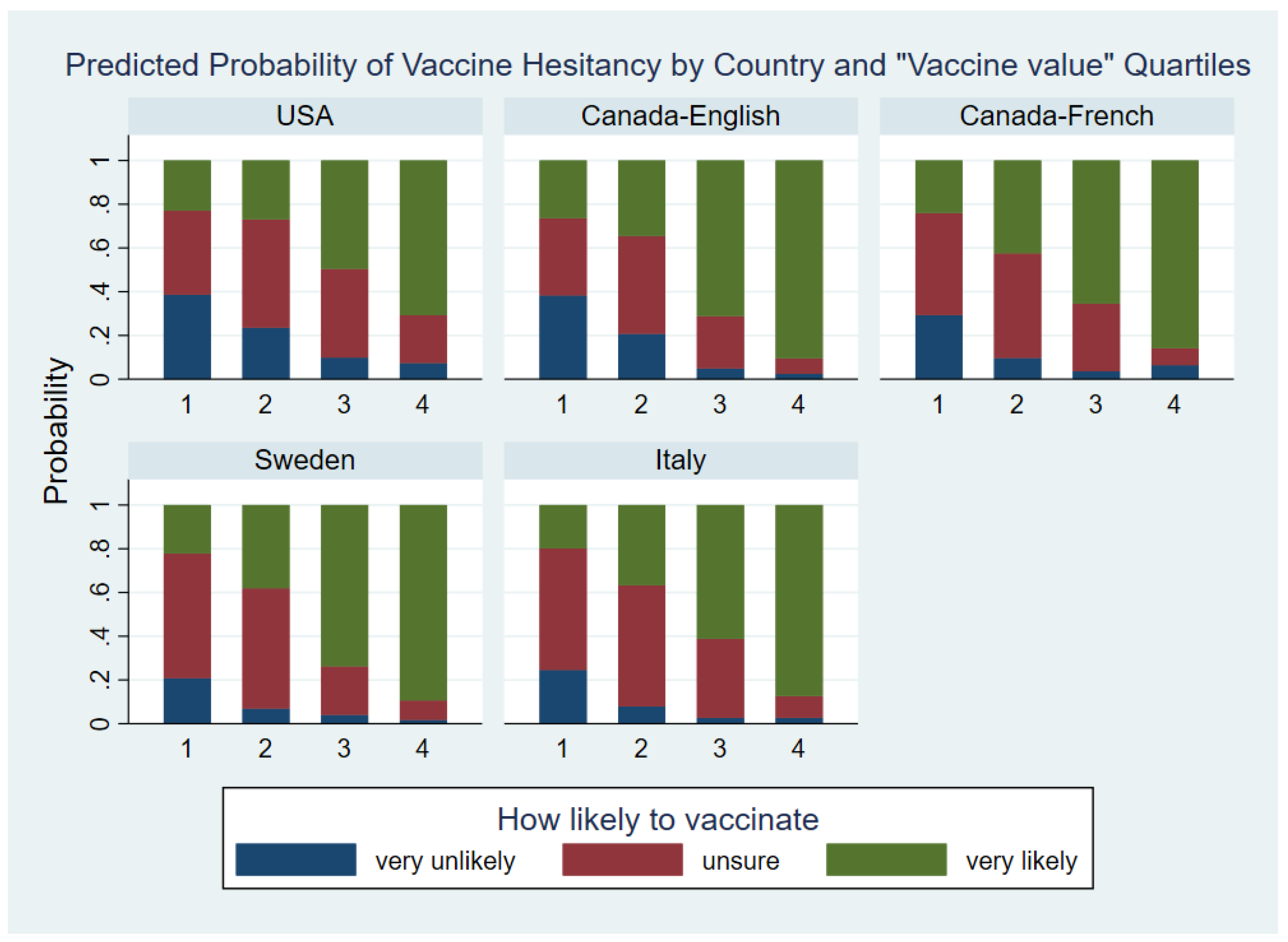
3.4.2. Vaccine Value Factor
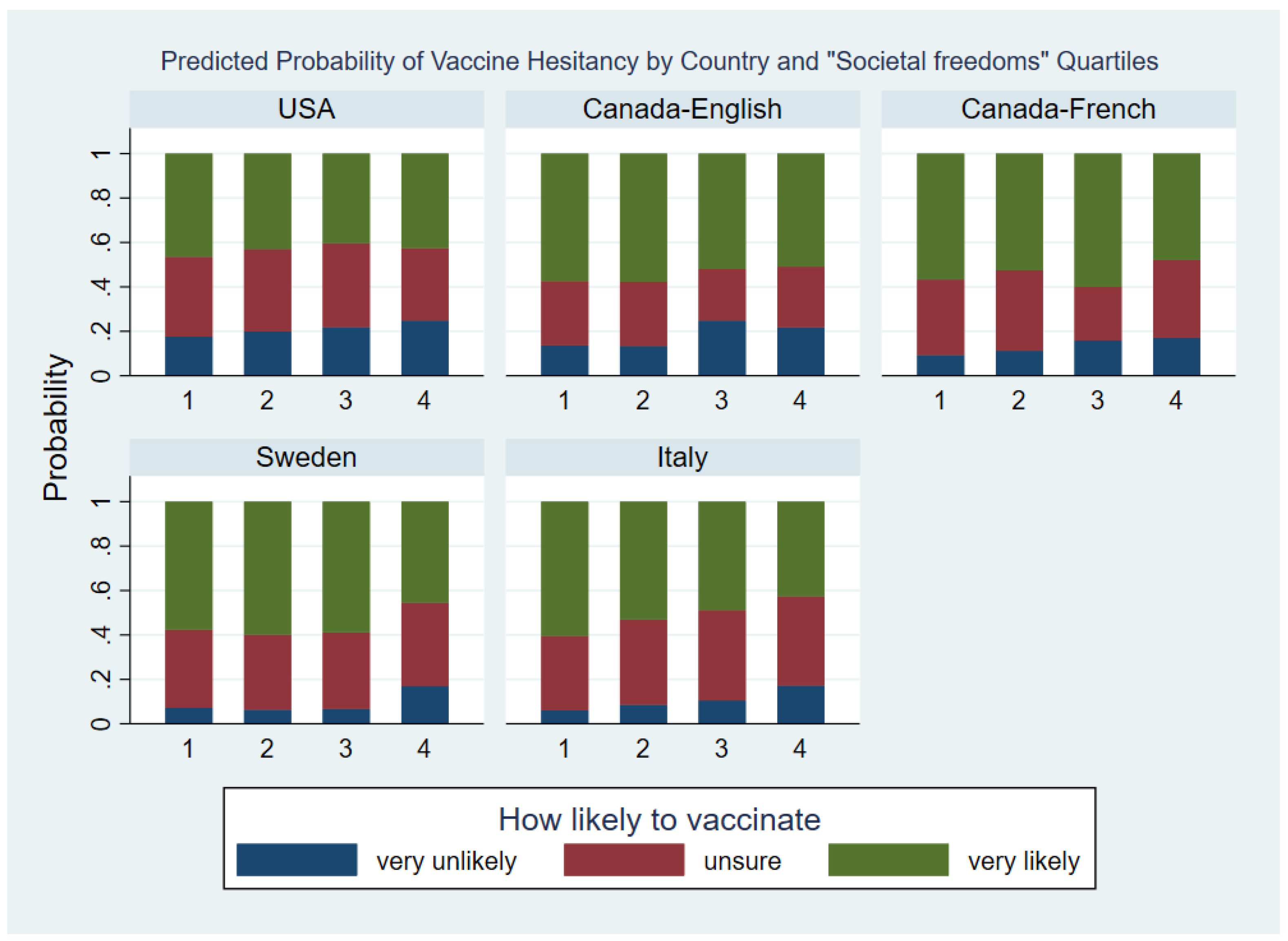
3.4.3. Societal Freedoms Factor
4. Discussion
5. Limitations
6. Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Methods
Appendix A.1. Modeling Vaccine Hesitancy Outcome
Appendix A.2. Vaccine Value Factor Interaction Term
Appendix A.3. Societal Freedom Interaction Term

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| USA n (%) | Canada English n (%) | Canad French n (%) | Sweden n (%) | Italy n (%) | Total | |
|---|---|---|---|---|---|---|
| Age | ||||||
| 18–24 | 142 (20) | 99 (20) | 99 (20) | 188 (19) | 194 (20) | 722 (20) |
| 25–34 | 147 (20) | 95 (19) | 98 (20) | 195 (20) | 196 (20) | 731 (20) |
| 35–44 | 143 (20) | 99 (20) | 97 (20) | 195 (20) | 198 (20) | 732 (20) |
| 45–54 | 149 (21) | 100 (20) | 99 (20) | 192 (20) | 198 (20) | 738 (20) |
| 55+ | 146 (20) | 100 (20) | 99 (20) | 195 (20) | 200 (20) | 740 (20) |
| Gender | ||||||
| Male | 364 (50) | 246 (50) | 245 (50) | 477 (49) | 489 (50) | 1821 (50) |
| Female | 363 (50) | 247 (50) | 247 (50) | 488 (51) | 497 (50) | 1842 (50) |
| Education | ||||||
| <High school | 49 (7) | 20 (4) | 29 (6) | 89 (9) | 83 (8) | 270 (7) |
| High school | 162 (22) | 83 (17) | 155 (32) | 463 (48) | 440 (45) | 1303 (36) |
| Some college | 140 (19) | 131 (27) | 145 (29) | 161 (17) | 133 (13) | 710 (19) |
| Bachelor’s degree | 132 (18) | 177 (36) | 119 (24) | 155 (16) | 277 (28) | 860 (23) |
| Post-graduate degree | 221 (30) | 74 (15) | 44 (9) | 85 (9) | 51 (5) | 475 (13) |
| Other | 22 (3) | 8 (2) | 0 (0) | 12 (1) | 2 (0) | 44 (1) |
| Income | ||||||
| Prefer not to say | 52 (7) | 52 (11) | 56 (11) | 156 (16) | 196 (20) | 512 (14) |
| Lower I | 141 (19) | 53 (11) | 63 (13) | 118 (12) | 206 (21) | 581 (16) |
| Lower II | 108 (15) | 71 (14) | 78 (16) | 90 (9) | 303 (31) | 650 (18) |
| Middle I | 93 (13) | 102 (21) | 82 (17) | 95 (10) | 155 (16) | 527 (14) |
| Middle II | 85 (12) | 87 (18) | 79 (16) | 114 (12) | 82 (8) | 447 (12) |
| High I | 38 (5) | 76 (15) | 76 (15) | 91 (9) | 29 (3) | 310 (8) |
| High II | 73 (10) | 27 (5) | 37 (8) | 90 (9) | 6 (1) | 233 (6) |
| High III | 137 (19) | 25 (5) | 21 (4) | 211 (22) | 9 (1) | 403 (11) |
| Are you eligible to receive a COVID-19 vaccine? | ||||||
| No | 176 (24) | 73 (15) | 93 (19) | 343 (36) | 153 (16) | 838 (23) |
| Yes | 551 (76) | 420 (85) | 399 (81) | 622 (64) | 833 (84) | 2825 (77) |
| In your life, were you ever recommended a vaccine (other than the COVID-19 vaccine) by a healthcare provider that you did not take? | ||||||
| No | 375 (52) | 391 (79) | 382 (78) | 691 (72) | 893 (91) | 2732 (75) |
| Yes | 352 (48) | 102 (21) | 110 (22) | 274 (28) | 93 (9) | 931 (25) |
| mean ± SD | mean ± SD | mean ± SD | mean ± SD | mean ± SD | mean ± SD | |
| Concerns about contracting COVID-19 score | 3.3 ± 2.1 | 3.3 ± 1.8 | 3.0 ± 12.0 | 3.5 ± 1.8 | 3.8 ± 1.7 | 3.2 ± 1.9 |
| USA n (%) | Canada English n (%) | Canada French n (%) | Sweden n (%) | Italy n (%) | ||
|---|---|---|---|---|---|---|
| Factor 1 score (Vaccine Effects) | ||||||
| Q1 | 239 (33) | 95 (19) | 113 (23) | 269 (28) | 199 (20) | 915 (25) |
| Q2 | 187 (26) | 121 (25) | 107 (22) | 293 (30) | 208 (21) | 916 (25) |
| Q3 | 120 (17) | 126 (26) | 126 (26) | 229 (24) | 315 (32) | 916 (25) |
| Q4 | 181 (25) | 151 (31) | 146 (30) | 174 (18) | 264 (27) | 916 (25) |
| Factor 2 score (Vaccine Value) | ||||||
| Q1 | 279 (38) | 82 (17) | 92 (19) | 221 (23) | 152 (15) | 826 (23) |
| Q2 | 210 (29) | 131 (27) | 136 (28) | 299 (31) | 229 (23) | 1005 (27) |
| Q3 | 133 (18) | 146 (30) | 97 (20) | 220 (23) | 315 (32) | 911 (25) |
| Q4 | 105 (14) | 134 (27) | 167 (34) | 225 (23) | 290 (29) | 921 (25) |
| Factor 3 score (Societal freedoms) | ||||||
| Q1 | 154 (21) | 126 (26) | 114 (23) | 285 (30) | 230 (23) | 909 (25) |
| Q2 | 149 (21) | 164 (33) | 122 (25) | 256 (27) | 215 (22) | 906 (25) |
| Q3 | 192 (26) | 131 (27) | 98 (20) | 185 (19) | 226 (23) | 832 (23) |
| Q4 | 232 (32) | 72 (15) | 158 (32) | 239 (25) | 315 (32) | 1016 (28) |
| Population Logit for | Total | USA | Canada English | Canada French | Sweden | Italy | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2 + 3 vs. 1 | 3 vs. 1 + 2 | 2 + 3 vs. 1 | 3 vs. 1 + 2 | 2 + 3 vs. 1 | 3 vs. 1 + 2 | 2 + 3 vs. 1 | 3 vs. 1 + 2 | 2 + 3 vs. 1 | 3 vs. 1 + 2 | 2 + 3 vs. 1 | 3 vs. 1 + 2 | |
| OR | OR | OR | OR | OR | OR | OR | OR | OR | OR | OR | OR | |
| Factor 1 (Vaccine Effects) | ||||||||||||
| Q2 vs. Q1 | 1.4 * | 1.0 | ||||||||||
| Q3 vs. Q1 | 1.5 † | 1.5 † | ||||||||||
| Q4 vs. Q1 | 1.5 | 2.5 † | ||||||||||
| Q3 vs. Q2 | 1.1 | 1.6 † | ||||||||||
| Q4 vs. Q2 | 1.1 | 2.6 † | ||||||||||
| Q4 vs. Q3 | 1.0 | 1.6 † | ||||||||||
| Factor 2 (Vaccine Value) | ||||||||||||
| Q2 vs. Q1 | 3.7 † | 2.0 † | 2.3 † | 1.3 | 2.9 † | 1.5 | 4.8 † | 2.6 * | 4.4 † | 2.4 † | 4.8 † | 2.6 † |
| Q3 vs. Q1 | 12.4 † | 8.0 † | 7.6 † | 3.8 † | 17.8 † | 9.0 † | 15.4 † | 7.8 † | 8.3 † | 14.3 † | 16.7 † | 8.5 † |
| Q4 vs. Q1 | 16.3 † | 30.7 † | 10.7 † | 10.7 † | 39.6 † | 39.6 † | 8.0 † | 28.5 † | 20.4 † | 49.3 † | 16.4 † | 45.7 † |
| Q3 vs. Q2 | 3.3 † | 4.0 † | 3.3 † | 3.0 † | 6.2 † | 5.8 † | 3.2 * | 3.0 † | 1.9 | 5.9 † | 3.5 † | 3.2 † |
| Q4 vs. Q2 | 4.4 † | 15.3 † | 4.6 † | 8.5 † | 13.9 † | 25.6 † | 1.7 | 10.9 † | 4.6 * | 20.4 † | 3.4 * | 17.4 † |
| Q4 vs. Q3 | 1.3 | 3.8 † | 1.4 | 2.8 * | 2.2 | 4.4 * | 0.5 | 3.7 † | 2.5 | 3.4 † | 1.0 | 5.4 † |
| Factor 3 (Societal freedoms) | ||||||||||||
| Q2 vs. Q1 | 0.9 | 0.9 | 0.8 | 0.8 | 1.0 | 1.0 | 0.8 | 0.8 | 1.2 | 1.2 | 0.6 * | 0.6 * |
| Q3 vs. Q1 | 0.5 † | 0.8 * | 0.7 | 0.7 | 0.3 * | 0.7 | 0.4 | 1.2 | 1.1 | 1.1 | 0.4 * | 0.4 * |
| Q4 vs. Q1 | 0.3 † | 0.5 † | 0.5 * | 0.8 | 0.4 * | 0.6 | 0.4 * | 0.6 | 0.3 † | 0.4 † | 0.2 † | 0.3 † |
| Q3 vs. Q2 | 0.6 * | 0.9 | 0.8 | 0.8 | 0.3 * | 0.7 | 0.6 | 1.6 | 0.9 | 0.9 | 0.7 | 0.7 |
| Q4 vs. Q2 | 0.4 † | 0.6 † | 0.7 | 1.0 | 0.4 * | 0.6 | 0.5 * | 0.7 | 0.2 † | 0.3 † | 0.3 † | 0.5 † |
| Q4 vs. Q3 | 0.6 * | 0.6 * | 0.8 | 1.2 | 1.3 | 0.9 | 0.9 | 0.5 * | 0.2 † | 0.4 † | 0.4 † | 0.6 * |
Appendix B. Scale Items
| Item | Strongly Disagree | Disagree | Somewhat Disagree | Unsure | Somewhat Agree | Agree | Strongly Agree | |
|---|---|---|---|---|---|---|---|---|
| You cannot get COVID-19 from the vaccine itself | misin_1_c19_vax | |||||||
| There are no toxic ingredients in the vaccine that can harm your health | misin_2_tox_ingred | |||||||
| The vaccine cannot mess up your DNA | misin_3_DNA | |||||||
| The vaccine cannot cause infertility | misin_4_infert | |||||||
| The vaccine cannot cause other diseases | misin_5_other_dis | |||||||
| The fast production of the vaccine did not compromise its safety | misin_6_fast_prod | |||||||
| The vaccine is not going to be used by Governments as a tool to limit our civil rights (right of assembly, right of movement, right of religion, etc.) | misin_7_rights |
| Item | Strongly Disagree | Disagree | Somewhat Disagree | Unsure | Somewhat Agree | Agree | Strongly Agree | |
|---|---|---|---|---|---|---|---|---|
| The vaccine will work in protecting me from getting COVID-19 | vax_conf_1_work | |||||||
| By taking the vaccine I will protect my friends and family from getting COVID-19 | vax_conf_2_friends | |||||||
| Everyone should get the vaccine to achieve herd immunity | vax_conf_3_herd | |||||||
| Getting COVID-19 is worse than experiencing potential side effects from the vaccine | vax_conf_4_c19worse | |||||||
| Natural remedies will not protect me from COVID-19 | vax_conf_5_natural |
| Item | Strongly Disagree | Disagree | Somewhat Disagree | Unsure | Somewhat Agree | Agree | Strongly Agree | |
|---|---|---|---|---|---|---|---|---|
| People should be free to decide if they get vaccinated or not with no consequences for their job or personal life | vax_op_1_decide | |||||||
| People should have the option to choose the vaccine brand they want | vax_op_2_brand | |||||||
| People should be allowed to live their life with no restrictions once vaccinated | vax_op_3_no_restrict | |||||||
| Healthcare professionals and scientists with concerns about the vaccine should have opportunities to share their opinions with the public | vax_op_4_hc_share_op | |||||||
| Everybody should have equal access to the most effective and safe vaccine regardless of income, race, or immigration status | dropped from analysis due to loadings | |||||||
| There is no elite group that will achieve financial power if people are getting vaccinated | dropped from analysis due to loadings | |||||||
| There is no microchip with tracking capabilities inserted in the vaccine | vax_op_7_microchip |
References
- World Health Organization. Top Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 29 August 2022).
- Rozek, L.S.; Jones, P.; Menon, A.; Hicken, A.; Apsley, S.; King, E.J. Understanding Vaccine Hesitancy in the Context of COVID-19: The Role of Trust and Confidence in a Seventeen-Country Survey. Int. J. Public Health 2021, 66, 636255. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Wyka, K.; Rauh, L.; Rabin, K.; Ratzan, S.; Gostin, L.O.; Larson, H.J.; El-Mohandes, A. Hesitant or Not? The Association of Age, Gender, and Education with Potential Acceptance of a COVID-19 Vaccine: A Country-level Analysis. J. Health Commun. 2020, 25, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Lima, G.; Cha, M.; Cha, C.; Kulshrestha, J.; Ahn, Y.-Y.; Varol, O. Misinformation, believability, and vaccine acceptance over 40 countries: Takeaways from the initial phase of the COVID-19 infodemic. PLoS ONE 2022, 17, e0263381. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Savoia, E.; Piltch-Loeb, R.; Goldberg, B.; Miller-Idriss, C.; Hughes, B.; Montrond, A.; Kayyem, J.; Testa, M.A. Predictors of COVID-19 vaccine hesitancy: Socio-demographics, co-morbidity, and past experience of racial discrimination. Vaccines 2021, 9, 767. [Google Scholar] [CrossRef] [PubMed]
- Piltch-Loeb, R.; Silver, D.R.; Kim, Y.; Norris, H.; McNeill, E.; Abramson, D.M. Determinants of the COVID-19 vaccine hesitancy spectrum. PLoS ONE 2022, 17, e0267734. [Google Scholar] [CrossRef] [PubMed]
- Savoia, E.; Harriman, N.W.; Piltch-Loeb, R.; Bonetti, M.; Toffolutti, V.; Testa, M.A. Exploring the Association between Misinformation Endorsement, Opinions on the Government Response, Risk Perception, and COVID-19 Vaccine Hesitancy in the US, Canada, and Italy. Vaccines 2022, 10, 671. [Google Scholar] [CrossRef] [PubMed]
- Piltch-Loeb, R.; Savoia, E.; Goldberg, B.; Hughes, B.; Verhey, T.; Kayyem, J.; Miller-Idriss, C.; Testa, M. Examining the effect of information channel on COVID-19 vaccine acceptance. PLoS ONE 2021, 16, e0251095. [Google Scholar] [CrossRef]
- Piltch-Loeb, R.; Harriman, N.W.; Healey, J.; Bonetti, M.; Toffolutti, V.; Testa, M.A.; Su, M.; Savoia, E. COVID-19 Vaccine Concerns about Safety, Effectiveness, and Policies in the United States, Canada, Sweden, and Italy among Unvaccinated Individuals. Vaccines 2021, 9, 1138. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Trends in COVID-19 Vaccine Confidence in the US. Available online: https://covid.cdc.gov/covid-data-tracker/#vaccine-confidence (accessed on 29 August 2022).
- Griffith, J.; Marani, H.; Monkman, H. COVID-19 Vaccine Hesitancy in Canada: Content Analysis of Tweets Using the Theoretical Domains Framework. J. Med. Internet Res. 2021, 23, e26874. [Google Scholar] [CrossRef]
- Moscardino, U.; Musso, P.; Inguglia, C.; Ceccon, C.; Miconi, D.; Rousseau, C. Sociodemographic and psychological correlates of COVID-19 vaccine hesitancy and resistance in the young adult population in Italy. Vaccine 2022, 40, 2379–2387. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.; Rempel, E.; Roe, I.; Adu, P.; Carenini, G.; Janjua, N.Z. Tracking Public Attitudes Toward COVID-19 Vaccination on Tweets in Canada: Using Aspect-Based Sentiment Analysis. J. Med. Internet Res. 2022, 24, e35016. [Google Scholar] [CrossRef] [PubMed]
- Fues, W.H.; Wikman, E.B.; Sahlin, C.; Nyaku, M.; Benĉina, G. Analysis of vaccine messages on social media (Twitter) in Scandinavia. Human Vaccines Immunother. 2022, 18, 2026711. [Google Scholar] [CrossRef] [PubMed]
- Rotolo, B.; Dubé, E.; Vivion, M.; MacDonald, S.E.; Meyer, S.B. Hesitancy towards COVID-19 vaccines on social media in Canada. Vaccine 2022, 40, 2790–2796. [Google Scholar] [CrossRef]
- Public Health Agency of Canada. COVID-19 Vaccine Uptake and Intent: Canadian Community Health Survey (CCHS) Insight. Available online: https://www.canada.ca/en/public-health/services/publications/vaccines-immunization/covid-19-vaccine-uptake-intent-canadian-community-health-survey.html#shr-pg0 (accessed on 29 August 2022).
- Di Giuseppe, G.; Pelullo, C.P.; Volgare, A.S.; Napolitano, F.; Pavia, M. Parents’ Willingness to Vaccinate Their Children With COVID-19 Vaccine: Results of a Survey in Italy. J. Adolesc. Health 2022, 70, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, O.V.; Johnson, M.S.; Ebling, S.; Amundsen, O.M.; Halsøy, Ø.; Hoffart, A.; Skjerdingstad, N.; Johnson, S.U. Risk, Trust, and Flawed Assumptions: Vaccine Hesitancy During the COVID-19 Pandemic. Front. Public Health 2021, 9, 700213. [Google Scholar] [CrossRef] [PubMed]
- Pollfish. Available online: www.pollfish.com (accessed on 8 December 2020).
- Government of Canada. Coronavirus Disease (COVID-19). Available online: https://www.canada.ca/en/public-health/services/diseases/coronavirus-disease-covid-19.html (accessed on 16 August 2021).
- How CDC Is Making COVID-19 Vaccine Recommendations. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations-process.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fvaccines%2Frecommendations.html (accessed on 30 August 2021).
- Folkhalsomyndigheten-Public Health Agency of Sweden: Vaccination against COVID-19. Available online: https://www.folkhalsomyndigheten.se/the-public-health-agency-of-sweden/communicable-disease-control/covid-19/vaccination-against-covid-19/ (accessed on 16 August 2021).
- L’epidemiologia per la Sanità Pubblica-Istituto Superiore di Sanità-Piano Nazionale di Vaccinazione COVID-19. Available online: https://www.epicentro.iss.it/vaccini/covid-19-piano-vaccinazione (accessed on 10 August 2021).
- Rothschild, D.; Konitzer, T. Random Device Engagement (RDE) with Organic Samples; Pollfish: New York, NY, USA, 2018. [Google Scholar]
- Hughes, B.; Miller-Idriss, C.; Piltch-Loeb, R.; Goldberg, B.; White, K.; Criezis, M.; Savoia, E. Development of a Codebook of Online Anti-Vaccination Rhetoric to Manage COVID-19 Vaccine Misinformation. Int. J. Environ. Res. Public Health 2021, 18, 7556. [Google Scholar] [CrossRef]
- Jodoin, M.G.; Gierl, M.J. Evaluating type I error and power rates using an effect size measure with the logistic regression procedure for DIF detection. Appl. Meas. Educ. 2001, 14, 329–349. [Google Scholar] [CrossRef]
- Petersen, M.A.; Groenvold, M.; Bjorner, J.B.; Aaronson, N.; Conroy, T.; Cull, A.; Fayers, P.; Hjermstad, M.; Sprangers, M.; Sullivan, M.; et al. Use of differential item functioning analysis to assess the equivalence of translations of a questionnaire. Qual. Life Res. 2003, 12, 373–385. [Google Scholar] [CrossRef]
- Scott, N.W.; Fayers, P.M.; Bottomley, A.; Aaronson, N.K.; de Graeff, A.; Groenvold, M.; Koller, M.; Petersen, M.A. Sprangers MAG: Comparing translations of the EORTC QLQ-C30 using differential item functioning analyses. Qual. Life Res. 2006, 15, 1103–1115. [Google Scholar] [CrossRef]
- Dziuban, C.D.; Shirkey, E.C. When is a correlation matrix appropriate for factor analysis? Psychol. Bull. 1974, 81, 358–361. [Google Scholar] [CrossRef]
- Cervantes, L.; Hazel, C.A.; Mancini, D.; Pereira, R.I.; Podewils, L.J.; Stella, S.A.; Durfee, J.; Barshney, A.; Steiner, J.F. Perspectives of Latinx Individuals Who Were Unvaccinated and Hospitalized for COVID-19: A Qualitative Study. JAMA Netw. Open 2022, 5, e2218362. [Google Scholar] [CrossRef] [PubMed]
- Kreps, S.; Dasgupta, N.; Brownstein, J.S.; Hswen, Y.; Kriner, D.L. Public attitudes toward COVID-19 vaccination: The role of vaccine attributes, incentives, and misinformation. NPJ Vaccines 2021, 6, 73. [Google Scholar] [CrossRef] [PubMed]
- Palamenghi, L.; Barello, S.; Boccia, S.; Graffigna, G. Mistrust in biomedical research and vaccine hesitancy: The forefront challenge in the battle against COVID-19 in Italy. Eur. J. Epidemiol. 2020, 35, 785–788. [Google Scholar] [CrossRef] [PubMed]
- Muric, G.; Wu, Y.; Ferrara, E. COVID-19 Vaccine Hesitancy on Social Media: Building a Public Twitter Data Set of Antivaccine Content, Vaccine Misinformation, and Conspiracies. JMIR Public Health Surveill. 2021, 7, e30642. [Google Scholar] [CrossRef] [PubMed]
- Neely, S.; Eldredge, C.; Sanders, R. Health Information Seeking Behaviors on Social Media During the COVID-19 Pandemic Among American Social Networking Site Users: Survey Study. J. Med. Internet Res. 2021, 23, e29802. [Google Scholar] [CrossRef]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccin. Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef]
- Abbasi, J. Widespread Misinformation About Infertility Continues to Create COVID-19 Vaccine Hesitancy. JAMA 2022, 327, 1013. [Google Scholar] [CrossRef]
- Coronavirus Pandemic (COVID-19). OurWorldInData.org. Available online: https://ourworldindata.org/coronavirus (accessed on 29 August 2022).
- Ontario Ministry of Health. COVID-19 Vaccine Administration. Available online: https://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/vaccine/COVID-19_vaccine_administration.pdf (accessed on 29 August 2022).
- American Journal of Managed Care. A Timeline of COVID-19 Vaccine Developments in 2021. Available online: https://www.ajmc.com/view/a-timeline-of-covid-19-vaccine-developments-in-2021 (accessed on 29 August 2022).
- Oliani, F.; Savoia, A.; Gallo, G.; Tiwana, N.; Letzgus, M.; Gentiloni, F.; Piatti, A.; Chiappa, L.; Bisesti, A.; Laquintana, D.; et al. Italy’s rollout of COVID-19 vaccinations: The crucial contribution of the first experimental mass vaccination site in Lombardy. Vaccine 2022, 40, 1397–1403. [Google Scholar] [CrossRef]
- The Local. Who Is Eligible for a COVID-19 Vaccine in Your Region of Italy. Available online: https://www.thelocal.it/20210506/which-groups-are-eligible-for-a-covid-19-vaccine-in-your-region-of-italy/ (accessed on 29 August 2022).
- Guay, M.; Gosselin, V.; Petit, G.; Baron, G.; Gagneur, A. Determinants of vaccine hesitancy in Quebec: A large population-based survey. Hum. Vaccines Immunother. 2019, 15, 2527–2533. [Google Scholar] [CrossRef]
- Lavoie, K.; Gosselin-Boucher, V.; Stojanovic, J.; Gupta, S.; Gagné, M.; Joyal-Desmarais, K.; Séguin, K.; Gorin, S.S.; Ribeiro, P.; Voisard, B.; et al. Understanding national trends in COVID-19 vaccine hesitancy in Canada: Results from five sequential cross-sectional representative surveys spanning April 2020-March 2021. BMJ Open 2022, 12, e059411. [Google Scholar] [CrossRef]
- Bolsen, T.; Palm, R. Politicization and COVID-19 vaccine resistance in the U.S. Prog. Mol. Biol. Transl. Sci. 2022, 188, 81–100. [Google Scholar] [CrossRef] [PubMed]
- The White House Briefing Room. Remarks from President Biden on the Fight against COVID-19. Available online: https://www.whitehouse.gov/briefing-room/speeches-remarks/2021/12/21/remarks-by-president-biden-on-the-fight-against-covid-19/ (accessed on 29 August 2022).
- Allin, S.; Fitzpatrick, T.; Marchildon, G.P.; Quesnel-Vallée, A. The federal government and Canada’s COVID-19 responses: From ‘we’re ready, we’re prepared’ to ‘fires are burning’. Health Econ. Policy Law 2022, 17, 76–94. [Google Scholar] [CrossRef]
- Warren, G.W.; Lofstedt, R. COVID-19 vaccine rollout risk communication strategies in Europe: A rapid response. J. Risk Res. 2021, 24, 369–379. [Google Scholar] [CrossRef]
- Stoler, J.; Klofstad, C.A.; Enders, A.M.; Uscinski, J.E. Sociopolitical and psychological correlates of COVID-19 vaccine hesitancy in the United States during summer 2021. Soc. Sci. Med. 2022, 306, 115112. [Google Scholar] [CrossRef] [PubMed]




| Item | Factor Loading | Item-Total Correlation | Communality |
|---|---|---|---|
| Factor 1 “Vaccine effects” | |||
| misin_1_c19_vax | 0.54 | 0.68 | 0.36 |
| misin_2_tox_ingred | 0.65 | 0.76 | 0.51 |
| misin_3_DNA | 0.56 | 0.73 | 0.45 |
| misin_4_infert | 0.63 | 0.73 | 0.45 |
| misin_5_other_dis | 0.68 | 0.73 | 0.45 |
| misin_6_fast_prod | 0.54 | 0.69 | 0.39 |
| misin_7_rights | 0.47 | 0.69 | 0.38 |
| Factor 2 “Vaccine value” | |||
| vax_conf_1_work | 0.76 | 0.82 | 0.64 |
| vax_conf_2_friends | 0.84 | 0.84 | 0.67 |
| vax_conf_3_herd | 0.86 | 0.85 | 0.7 |
| vax_conf_4_c19worse | 0.61 | 0.76 | 0.46 |
| vax_conf_5_natural | 0.51 | 0.71 | 0.38 |
| vax_op_7_microchip | 0.49 | 0.71 | 0.43 |
| Factor 3 “Societal freedoms” | |||
| vax_op_1_decide | 0.59 | 0.72 | 0.36 |
| vax_op_2_brand | 0.57 | 0.72 | 0.33 |
| vax_op_3_no_restrict | 0.41 | 0.63 | 0.23 |
| vax_op_4_hc_share_op | 0.55 | 0.69 | 0.33 |
| Country-Language | RMSEA | CFI | TLI |
|---|---|---|---|
| USA | 0.053 | 0.957 | 0.950 |
| Canada-English | 0.058 | 0.937 | 0.926 |
| Canada-French | 0.068 | 0.939 | 0.928 |
| Sweden | 0.069 | 0.902 | 0.885 |
| Italy | 0.063 | 0.915 | 0.900 |
| Country-Language | Vaccine Effects (Factor 1) | Vaccine Value (Factor 2) | Societal Freedoms (Factor 3) |
|---|---|---|---|
| USA | −0.18 ± 1.13 | −0.39 ± 0.98 | 0.02 ± 0.70 |
| Canada-English | 0.19 ± 0.99 | 0.13 ± 0.92 | −0.18 ± 0.64 |
| Canada-French | 0.15 ± 1.01 | 0.15 ± 1.02 | 0.09 ± 0.86 |
| Sweden | −0.12 ± 0.82 | −0.03 ± 0.89 | −0.05 ± 0.83 |
| Italy | 0.08 ± 0.76 | 0.17 ± 0.85 | 0.08 ± 0.82 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piltch-Loeb, R.; Su, M.; Bonetti, M.; Testa, M.; Stanton, E.; Toffolutti, V.; Savoia, E. Cross-National Vaccine Concerns and Predictors of Vaccine Hesitancy in Not-Fully Vaccinated Individuals: Findings from USA, Canada, Sweden, and Italy. Vaccines 2022, 10, 1652. https://doi.org/10.3390/vaccines10101652
Piltch-Loeb R, Su M, Bonetti M, Testa M, Stanton E, Toffolutti V, Savoia E. Cross-National Vaccine Concerns and Predictors of Vaccine Hesitancy in Not-Fully Vaccinated Individuals: Findings from USA, Canada, Sweden, and Italy. Vaccines. 2022; 10(10):1652. https://doi.org/10.3390/vaccines10101652
Chicago/Turabian StylePiltch-Loeb, Rachael, Max Su, Marco Bonetti, Marcia Testa, Eva Stanton, Veronica Toffolutti, and Elena Savoia. 2022. "Cross-National Vaccine Concerns and Predictors of Vaccine Hesitancy in Not-Fully Vaccinated Individuals: Findings from USA, Canada, Sweden, and Italy" Vaccines 10, no. 10: 1652. https://doi.org/10.3390/vaccines10101652