Clinical Role of Aspirin in Mood Disorders: A Systematic Review
by
 ,
,
Qin Xiang Ng
1,2,* ,
,
Krishnapriya Ramamoorthy
1,2,
Wayren Loke
1,
Matthew Wei Liang Lee
3,
Wee Song Yeo
4,5,
Donovan Yutong Lim
2,5 and
Vivekanandan Sivalingam
2 1
MOH Holdings Pte Ltd., 1 Maritime Square, Singapore 099253, Singapore
2
Institute of Mental Health, Buangkok Green Medical Park, 10 Buangkok View, Singapore 539747, Singapore
3
Fitzwilliam College, University of Cambridge, Storey’s Way, Cambridge CB3 0DG, UK
4
National University Hospital, National University Health System, Singapore 119074, Singapore
5
Yong Loo Lin School of Medicine, National University of Singapore, Singapore 117597, Singapore
*
Author to whom correspondence should be addressed.
Brain Sci. 2019, 9(11), 296; https://doi.org/10.3390/brainsci9110296
Submission received: 29 September 2019
/
Revised: 25 October 2019
/
Accepted: 27 October 2019
/
Published: 29 October 2019
(This article belongs to the Special Issue Etiology, Pharmacological, and Brain Stimulation Interventions for Bipolar Disorders)
Abstract
:Worldwide, depression and bipolar disorder affect a large and growing number of people. However, current pharmacotherapy options remain limited. Despite adequate treatment, many patients continue to have subsyndromal symptoms, which predict relapse in bipolar illness and often result in functional impairments. Aspirin, a common nonsteroidal anti-inflammatory drug (NSAID), has purported beneficial effects on mood symptoms, showing protective effects against depression in early cohort studies. This systematic review thus aimed to investigate the role of aspirin in mood disorders. Using the keywords (aspirin or acetylsalicy* or asa) and (mood or depress* or bipolar or mania or suicid*), a comprehensive search of PubMed, EMBASE, Medline, PsycINFO, Clinical Trials Register of the Cochrane Collaboration Depression, Anxiety and Neurosis Group (CCDANTR), Clinicaltrials.gov and Google Scholar databases found 13,952 papers published in English between 1 January 1988 and 1 May 2019. A total of six clinical studies were reviewed. There were two randomized, placebo-controlled, double-blind trials and populations drawn from two main cohort studies (i.e., the Geelong Osteoporosis Study and the Osteoarthritis Initiative study). Using a random-effects model, the pooled hazard ratio of the three cohort studies was 0.624 (95% confidence interval: 0.0503 to 1.198, p = 0.033), supporting a reduced risk of depression with aspirin exposure. Overall, the dropout rates were low, and aspirin appears to be well-tolerated with minimal risk of affective switch. In terms of methodological quality, most studies had a generally low risk of bias. Low-dose aspirin (80 to 100 mg/day) is safe, well-tolerated and potentially efficacious for improving depressive symptoms in both unipolar and bipolar depression. Due to its ability to modulate neuroinflammation and central nervous system processes, aspirin may also have valuable neuroprotective and pro-cognitive effects that deserve further exploration. Further randomized, controlled trials involving the adjunctive use of aspirin should be encouraged to confirm its therapeutic benefits.
Keywords:
aspirin; anti-inflammatory; psychiatry; mood disorder; depression; bipolar; systematic review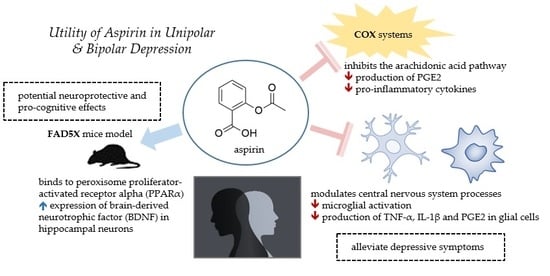
1. Introduction
Worldwide, mood disorders (depression and bipolar disorder) are a growing public health concern. Depression alone affects over 350 million people globally and accounts for approximately 7.5% of healthy years lost due to disability [1]. A 2010 Global Burden of Disease Study reported that depression and bipolar disorder resulted in more than 85 million disability-adjusted life years [2], a startling human and economic cost.
Depressive and bipolar disorders are both chronic conditions, and long-term maintenance treatment is necessary to prevent recurrence of symptoms, reduce residual symptoms, and maintain functioning [3,4]. However, pharmacotherapy of mood disorders remains suboptimal, often plagued with persistence of symptoms despite an adequate trial of treatment. Several large-scale meta-analyses have raised questions about the efficacy of selective serotonin reuptake inhibitor (SSRI) antidepressants, which are first-line drugs frequently used to treat depression [5,6]. The management of bipolar disorder remains a clinical challenge [7], with variable responses to treatment depending on the polarity of patients [8], and many patients continue to have subsyndromal symptoms. Subsyndromal symptoms in bipolar illness predict relapse and often result in functional impairments [9]. There is thus a need to research new and more-effective acute and maintenance therapies.
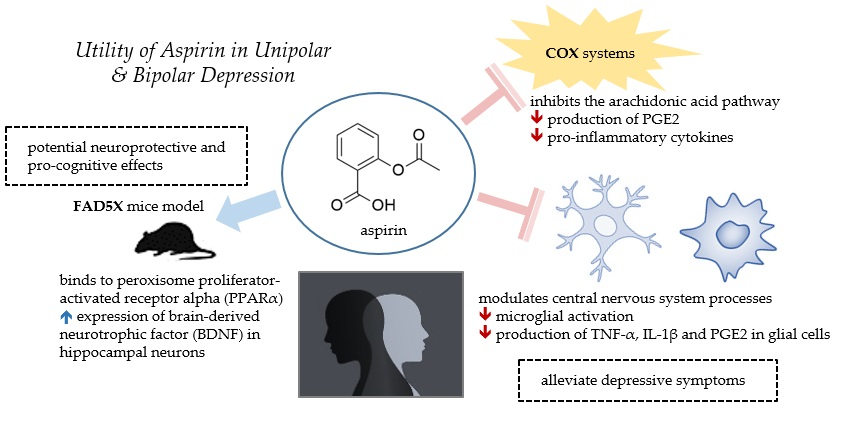
Aspirin, also known as acetylsalicylic acid (ASA), is a nonsteroidal anti-inflammatory drug (NSAID) commonly prescribed for pain, fever as well as the prevention of cardiovascular events (including stroke and myocardial infarction) [10]. Aspirin exerts its therapeutic effects via inhibition of cyclooxygenase (COX)-1 and COX-2 systems, reducing the production of prostaglandin E2 (PGE2) and pro-inflammatory cytokines [11]. Increasing evidence points to a pro-inflammatory state in patients with unipolar depression (increased serum interleukin (IL)-6) [12] and bipolar depression (increased levels of IL-1, IL-6 and TNF-alpha) [13]. As such, ASA may ameliorate systemic and brain inflammation and serve as an effective therapeutic adjunct for patients suffering from mood disorders.
The potential therapeutic benefit of ASA for the prevention of depression was suggested by early analyses of the longitudinal Geelong Osteoporosis Study conducted between 1994 and 1997 [14]. Exposure to ASA was associated with a significantly decreased risk of depression (odds ratio 0.18, 95% confidence interval (CI): 0.02 to 1.39). Newer studies showing supporting or null associations have emerged since then. No systematic review on the topic has been performed. A systematic review of the clinical role of ASA in mood disorders is therefore timely to summarize current evidence and guide further research.
2. Methods
2.1. Search Strategy and Study Identification
A systematic literature search was performed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. By using the following combinations of broad Major Exploded Subject Headings (MesH) terms or text words (aspirin or acetylsalicy* or asa) and (mood or depress* or bipolar or mania or suicid*), a comprehensive search of PubMed, EMBASE, Medline, PsycINFO, Clinical Trials Register of the Cochrane Collaboration Depression, Anxiety and Neurosis Group (CCDANTR), Clinicaltrials.gov and Google Scholar databases yielded 13,952 papers published in English between 1 January 1988 and 1 May 2019. Attempts were made to search the grey literature using Google search engine. Title/abstract screening were performed independently by three study investigators (Q.X. Ng, W.R. Loke, and M.W.L. Lee) to identify articles of interest. All retrieved publications were manually reviewed and also checked for references of interest.
2.2. Study Selection Criteria and Eligibility Criteria
The inclusion criteria for this review were (1) published clinical study, (2) study participants with diagnosed depressive or bipolar disorder, (3) use of ASA, and (4) available outcome data pertaining to mood symptoms and control. Any disagreement on inclusion was resolved by consensus. Conference abstracts and proceedings were not accepted for inclusion into this systematic review.
2.3. Data Extraction and Risk of Bias
Data were extracted using a standardized electronic form by one study investigator (Q.X. Ng) and cross-checked by a second investigator (W.R. Loke) for accuracy.
The Cochrane Collaboration’s tool for assessing risk of bias [15] of randomized, controlled trials and the Newcastle–Ottawa Scale [16] for cohort studies was independently applied by three study investigators (Q.X. Ng, K. Ramamoorthy, and M.W.L. Lee) to assess the quality of the studies reviewed. Any disagreement was resolved by discussion and consensus among the three researchers.
2.4. Statistical Analyses
Hazard ratios reported by the different cohort studies were pooled using a random-effects model, assuming that the selected studies are random samples from a larger population. Heterogeneity was examined using the I2 statistic and Cochran’s Q test. Publication bias was assessed using a funnel plot and Egger test. All analyses were done using MedCalc Statistical Software version 14.8.1 (MedCalc Software bvba, Ostend, Belgium; 2014).
3. Results
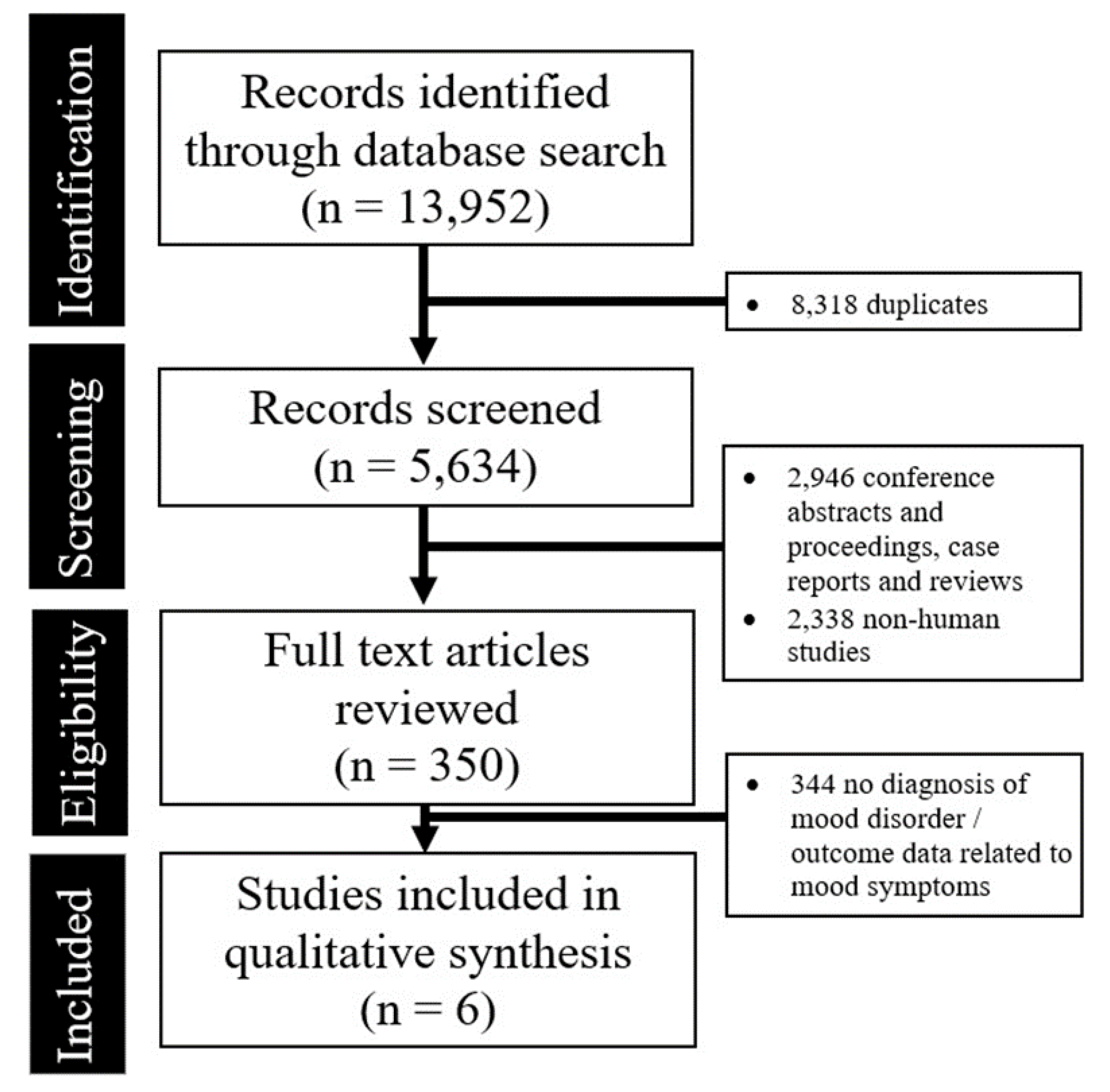
The abstraction process (and reasons for exclusion) is summarized in Figure 1.
A total of six clinical studies were systematically reviewed. The salient details of the studies are summarized in Table 1. There were two randomized, placebo-controlled, double-blind trials and two key cohort studies (the Geelong Osteoporosis Study [14] and the Osteoarthritis Initiative (OAI) study [17]). A meta-analysis was limited due to the small number of studies and dissimilar study designs and outcome measures. For the same reasons, a sensitivity analysis was not performed.
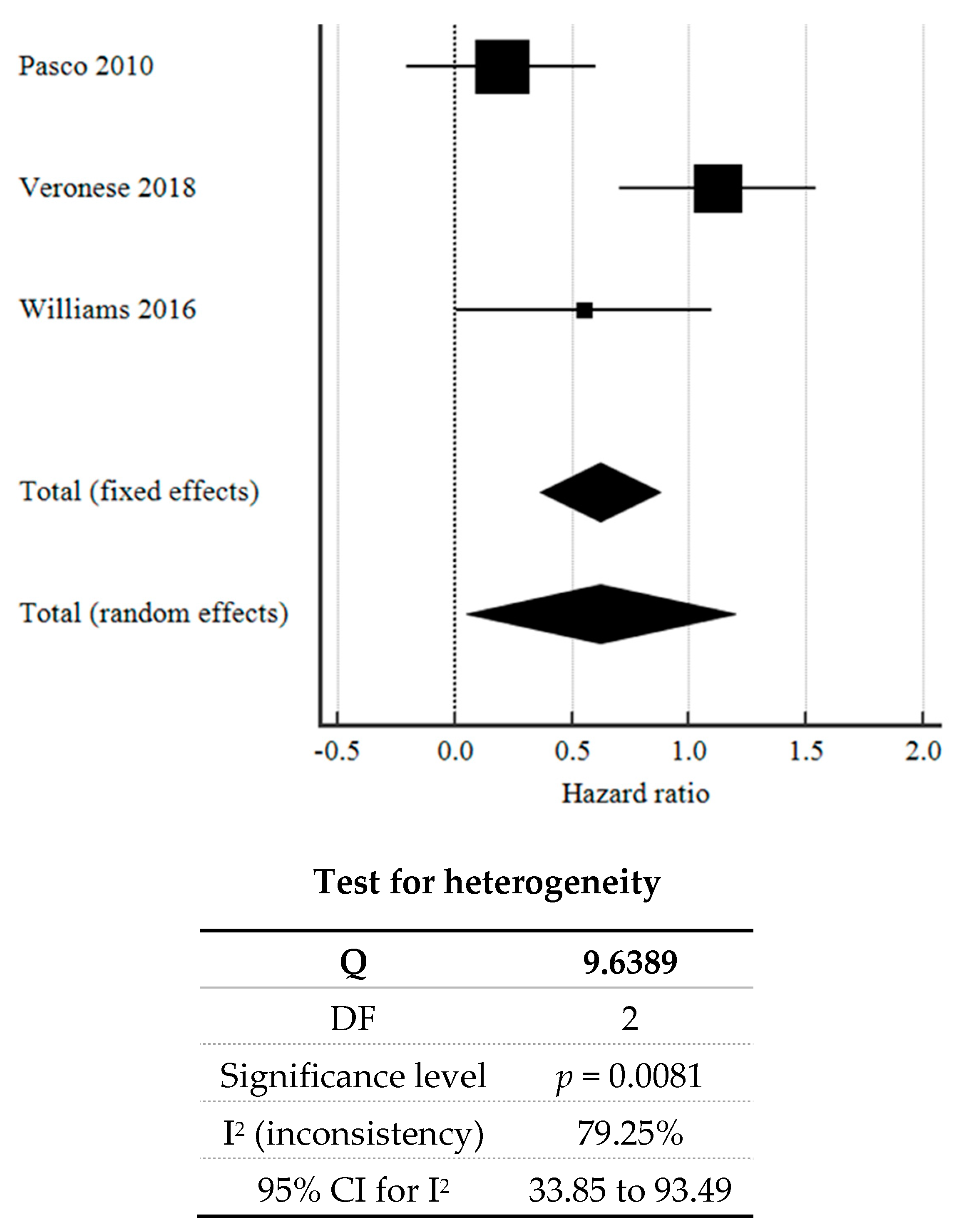
Using a random-effects model, the pooled HR of the three cohort studies [14,17,21] was 0.624 (95% CI: 0.0503 to 1.198, p = 0.033), supporting a reduced risk of depression with ASA exposure. The high heterogeneity (I2 = 79.25%), as seen in Figure 2, could be due to the different population characteristics studied (e.g., patients being at different phases of illness, of differing demographics, and on different treatments).
4. Discussion
Overall, there is some evidence to support the antidepressant effects of ASA for both unipolar and bipolar depression. The effective management of bipolar disorder remains a clinical challenge. The clinical role of serotonergic antidepressant medication in bipolar depression is still debated and often cautioned due to concerns of manic/hypomanic switch [22]. Importantly, ASA alleviates depressive symptoms and does not appear to induce affective switch or de-stabilization. In a randomized, controlled study of patients with bipolar disorder (N = 32) maintained on lithium and ASA (240 mg/day), baseline and endpoint serum lithium concentrations and mood symptoms remained stable throughout the duration of the study [18]. There was no significant difference in mania or depressive symptoms between the group who received aspirin (240 mg/day) or placebo, along with lithium maintenance therapy. In another randomized trial of bipolar patients (N = 99) who are at least moderately depressed, there was a main effect of ASA on treatment response, and only one patient who received both ASA (81 mg twice daily) and minocycline (100 mg twice daily) developed hypomania. Overall, the drop-out rate was low and ASA appears well-tolerated with minimal risk of affective switch.
The pooled HR of the three cohort studies [14,17,21] was 0.624 (95% CI: 0.0503 to 1.198, p = 0.033), supporting an overall reduced risk of depression with ASA exposure. The potential therapeutic mechanisms of ASA on mood likely stem from its effects on COX-1 and COX-2 systems, inhibiting the arachidonic acid pathway (which is a central regulator of inflammatory response) and in the process, reducing the production of PGE2 and pro-inflammatory cytokines [11]. Increasing evidence have supported a cytokine hypothesis of depression and the existence of a pro- inflammatory state in patients with unipolar depression (increased serum interleukin IL-6) [12] and bipolar depression (increased levels of IL-1, IL-6 and TNF-α) [13,23]. Animal studies have found that COX-2 inhibition attenuates neuroinflammation (hippocampal inflammatory markers cytokines IL-1β, TNF-α, and brain PGE2 levels) and circulating corticosterone, and may also alleviate symptoms of anxiety and cognitive decline [24]. Moreover, lithium, which is the current gold standard pharmacotherapy for bipolar patients [25], also shares these characteristics. Previous studies have found that it is able to decrease the production of TNF-α, IL-1β, and PGE2 in glial cells [26,27].
In addition to the effects of COX inhibition on the inflammatory cascade, ASA could also modulate central nervous system (CNS) processes. Adult human microglia predominantly express COX-1 [28]. Several lines of evidence suggest the involvement of microglial activation in the pathogenesis of bipolar disorder [23,29]. In this vein, as ASA covalently modifies COX-1, this could at least in part account for its therapeutic effects for patients with bipolar disorder. A recent study conducted using the FAD5X mice model for Alzheimer’s disease also found that ASA binds to peroxisome proliferator-activated receptor alpha (PPARα) and upregulates the expression of brain-derived neurotrophic factor (BDNF) in hippocampal neurons. These actions are beneficial for both cognition and mood as BDNF enhances serotonergic (5-HT) neurons and has a postulated central role in synaptic plasticity and neuroplasticity [30]. It is worth mentioning that cognitive dysfunction is common in patients with mood disorders, and it remains difficult-to-treat and is associated with poorer clinical outcomes and impaired functioning [31]. Some cohort studies have reported that ASA protects against cognitive decline [10,32]. Similarly, a new antidepressant, vortioxetine improves cognitive function by increasing BDNF in the hippocampus [33].
Minocycline, which was administered in one of the trials, along with aspirin [19], is an antibiotic that has anti-inflammatory properties and also acts on microglial cells [34]. It has demonstrated antidepressant effects in clinical studies [35], albeit contradictory results have been reported in animal models [36].
Finally, drug safety is also an important consideration, especially in choosing long-term therapies. In the above studies reviewed, there were no reports of any severe adverse events related to ASA use. Findings from the landmark Japanese Primary prevention of atherosclerosis with Aspirin for Diabetes (JPAD) trial also support the tolerability and safety of low-dose ASA (80 to 100 mg/day) [37]. As hemorrhagic stroke is more common in the Japanese than Western populations [38], it was encouraging that the risk of hemorrhagic stroke was similar between the treatment and control group in the JPAD trial [37]. Moreover, a 10-year follow-up of the patients enrolled in the original JPAD trial found no increased risk of cardiovascular events with low-dose ASA use but slight increased risk (p = 0.03) for gastrointestinal bleeding [39].
5. Conclusions
In conclusion, there is considerable evidence to support the clinical role of aspirin in the management of mood disorders. Low-dose aspirin (80 to 100 mg/day) appears safe, well-tolerated, and efficacious for improving depressive symptoms and preventing bipolar relapse. Due to its ability to modulate neuroinflammation and CNS processes, aspirin may also have valuable neuroprotective and pro-cognitive effects that deserve further exploration. More randomized, controlled trials involving the adjunctive use of aspirin are warranted to confirm its therapeutic benefits.
Author Contributions
Q.X.N. conceived, designed and carried out the study, and the relevant data analysis and interpretation, while D.Y.L. and V.S. supervised the study. W.L., M.W.L.L., K.R. and W.S.Y. carried out the study, and the relevant data analysis and interpretation. All authors contributed to the writing and proofreading of the final manuscript. The final manuscript was discussed and approved by all authors.
Acknowledgments
The authors thank Christopher Yi Wen Chan (Department of Mood and Anxiety, Institute of Mental Health) for reviewing an earlier version of the manuscript and providing useful comments and feedback.
Conflicts of Interest
The authors declare that there are no conflicts of interest. The authors alone are responsible for the content and writing of the article.
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Whiteford, H.A.; Degenhardt, L.; Rehm, J.; Baxter, A.J.; Ferrari, A.J.; Erskine, H.E.; Charlson, F.J.; Norman, R.E.; Flaxman, A.D.; Johns, N.; et al. Global burden of disease attributable to mental and substance use disorders: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 382, 1575–1586. [Google Scholar] [CrossRef]
- Grande, I.; Berk, M.; Birmaher, B.; Vieta, E. Bipolar disorder. Lancet 2016, 387, 1561–1572. [Google Scholar] [CrossRef]
- Klein, D.N.; Santiago, N.J. Dysthymia and chronic depression: Introduction, classification, risk factors, and course. J. Clin. Psychol. 2003, 59, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, J.C.; Katakam, K.K.; Schou, A.; Hellmuth, S.G.; Stallknecht, S.E.; Leth-Møller, K.; Iversen, M.; Banke, M.B.; Petersen, I.J.; Klingenberg, S.L.; et al. Selective serotonin reuptake inhibitors versus placebo in patients with major depressive disorder. A systematic review with meta-analysis and Trial Sequential Analysis. BMC Psychiatry 2017, 17, 58. [Google Scholar]
- Khin, N.A.; Chen, Y.F.; Yang, Y.; Yang, P.; Laughren, T.P. Exploratory analyses of efficacy data from major depressive disorder trials submitted to the US Food and Drug Administration in support of new drug applications. J. Clin. Psychiatry 2011, 72, 464–472. [Google Scholar] [CrossRef]
- Ng, Q.X.; Yeo, W.S.; Sivalingam, V. Lithium-associated Renal Dysfunction: To Stop or Not to Stop? Bipolar Disord. 2019. [Google Scholar] [CrossRef]
- Popovic, D.; Reinares, M.; Goikolea, J.M.; Bonnin, C.M.; Gonzalez-Pinto, A.; Vieta, E. Polarity index of pharmacological agents used for maintenance treatment of bipolar disorder. Eur. Neuropsychopharmacol. 2012, 22, 339–346. [Google Scholar] [CrossRef]
- Bauer, M.; Glenn, T.; Alda, M.; Grof, P.; Sagduyu, K.; Bauer, R.; Lewitzka, U.; Whybrow, P.C. Comparison of pre-episode and pre-remission states using mood ratings from patients with bipolar disorder. Pharmacopsychiatry 2011, 44, S49–S53. [Google Scholar] [CrossRef]
- Ogawa, H.; Nakayama, M.; Morimoto, T.; Uemura, S.; Kanauchi, M.; Doi, N.; Jinnouchi, H.; Sugiyama, S.; Saito, Y. Japanese Primary Prevention of Atherosclerosis with Aspirin for Diabetes (JPAD) Trial Investigators. Low-dose aspirin for primary prevention of atherosclerotic events in patients with type 2 diabetes: A randomized controlled trial. JAMA 2008, 300, 2134–2141. [Google Scholar] [CrossRef]
- Kalgutkar, A.S.; Crews, B.C.; Rowlinson, S.W.; Garner, C.; Seibert, K.; Marnett, L.J. Aspirin-like molecules that covalently inactivate cyclooxygenase-2. Science 1998, 280, 1268–1270. [Google Scholar] [CrossRef]
- Eller, T.; Vasar, V.; Shlik, J.; Maron, E. Pro-inflammatory cytokines and treatment response to escitaloprsam in major depressive disorder. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2008, 32, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Jung, H.G.; Myint, A.M.; Kim, H.; Park, S.H. Imbalance between pro-inflammatory and anti-inflammatory cytokines in bipolar disorder. J. Affect. Disord. 2007, 104, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Pasco, J.A.; Jacka, F.N.; Williams, L.J.; Henry, M.J.; Nicholson, G.C.; Kotowicz, M.A.; Berk, M. Clinical implications of the cytokine hypothesis of depression: The association between use of statins and aspirin and the risk of major depression. Psychother. Psychosom. 2010, 79, 323. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Wells, G.A. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non Randomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 29 June 2019).
- Veronese, N.; Koyanagi, A.; Stubbs, B.; Solmi, M.; Fornaro, M.; Fernandes, B.S.; Muller, C.; Thompson, T.; Carvalho, A.F.; Maggi, S. Aspirin and incident depressive symptoms: A longitudinal cohort study over 8 years. Int. J. Geriatr. Psychiatr 2018, 33, e193–e198. [Google Scholar] [CrossRef]
- Saroukhani, S.; Emami-Parsa, M.; Modabbernia, A.; Ashrafi, M.; Farokhnia, M.; Hajiaghaee, R.; Akhondzadeh, S. Aspirin for treatment of lithium-associated sexual dysfunction in men: Randomized double-blind placebo-controlled study. Bipolar Disord. 2013, 15, 650–656. [Google Scholar] [CrossRef]
- Savitz, J.B.; Teague, T.K.; Misaki, M.; Macaluso, M.; Wurfel, B.E.; Meyer, M.; Drevets, D.; Yates, W.; Gleason, O.; Drevets, W.C.; et al. Treatment of bipolar depression with minocycline and/or aspirin: An adaptive, 2 × 2 double-blind, randomized, placebo-controlled, phase IIA clinical trial. Transl. Psychiatry 2018, 8, 27. [Google Scholar] [CrossRef]
- Stolk, P.; Souverein, P.C.; Wilting, I.; Leufkens, H.G.; Klein, D.F.; Rapoport, S.I.; Heerdink, E.R. Is aspirin useful in patients on lithium? A pharmacoepidemiological study related to bipolar disorder. Prostaglandins Leukot. Essent. Fat. Acids 2010, 82, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Williams, L.J.; Pasco, J.A.; Mohebbi, M.; Jacka, F.N.; Stuart, A.L.; Venugopal, K.; O’Neil, A.; Berk, M. Statin and aspirin use and the risk of mood disorders among men. Int. J. Neuropsychopharmacol. 2016, 19. [Google Scholar] [CrossRef]
- Sidor, M.M.; MacQueen, G.M. An update on antidepressant use in bipolar depression. Curr. Psychiatry Rep. 2012, 14, 696–704. [Google Scholar] [CrossRef]
- Rao, J.S.; Harry, G.J.; Rapoport, S.I.; Kim, H.W. Increased excitotoxicity and neuroinflammatory markers in postmortem frontal cortex from bipolar disorder patients. Mol. Psychiatry 2010, 15, 384. [Google Scholar] [CrossRef] [PubMed]
- Casolini, P.; Catalani, A.; Zuena, A.R.; Angelucci, L. Inhibition of COX-2 reduces the age-dependent increase of hippocampal inflammatory markers, corticosterone secretion, and behavioral impairments in the rat. J. Neurosci. Res. 2002, 68, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Compton, M.T.; Nemeroff, C.B. The treatment of bipolar depression. J. Clinic. Psychiatry 2000, 61, 57–67. [Google Scholar]
- Nahman, S.; Belmaker, R.H.; Azab, A.N. Effects of lithium on lipopolysaccharide-induced inflammation in rat primary glia cells. Innate Immun. 2012, 18, 447–458. [Google Scholar] [CrossRef] [PubMed]
- Budni, J.; Feijó, D.P.; Batista-Silva, H.; Garcez, M.L.; Mina, F.; Belletini-Santos, T.; Krasilchik, L.R.; Luz, A.P.; Schiavo, G.L.; Quevedo, J. Lithium and memantine improve spatial memory impairment and neuroinflammation induced by β-amyloid 1-42 oligomers in rats. Neurobiol. Learn. Mem. 2017, 141, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Hoozemans, J.J.; Veerhuis, R.; Janssen, I.; van Elk, E.J.; Rozemuller, A.J.; Eikelenboom, P. The role of cyclo-oxygenase 1 and 2 activity in prostaglandin E2 secretion by cultured human adult microglia: Implications for Alzheimer’s disease. Brain Res. 2002, 951, 218–226. [Google Scholar] [CrossRef]
- Söderlund, J.; Olsson, S.K.; Samuelsson, M.; Walther-Jallow, L.; Johansson, C.; Erhardt, S.; Landén, M.; Engberg, G. Elevation of cerebrospinal fluid interleukin-1β in bipolar disorder. J. Psychiatry Neurosci. JPN 2011, 36, 114. [Google Scholar] [CrossRef]
- Patel, D.; Roy, A.; Kundu, M.; Jana, M.; Luan, C.H.; Gonzalez, F.J.; Pahan, K. Aspirin binds to PPARα to stimulate hippocampal plasticity and protect memory. Proc. Nat. Acad. Sci. USA 2018, 115, E7408–E7417. [Google Scholar] [CrossRef]
- MacQueen, G.M.; Memedovich, K.A. Cognitive dysfunction in major depression and bipolar disorder: A ssessment and treatment options. Psychiatry Clin. Neurosci. 2017, 71, 18–27. [Google Scholar] [CrossRef]
- Chang, C.W.; Horng, J.T.; Hsu, C.C.; Chen, J.M. Mean daily dosage of aspirin and the risk of incident Alzheimer’s dementia in patients with type 2 diabetes mellitus: A nationwide retrospective cohort study in Taiwan. J. Diabetes Res. 2016, 2016. [Google Scholar] [CrossRef]
- Lu, Y.; Ho, C.S.; McIntyre, R.S.; Wang, W.; Ho, R.C. Effects of vortioxetine and fluoxetine on the level of Brain Derived Neurotrophic Factors (BDNF) in the hippocampus of chronic unpredictable mild stress-induced depressive rats. Brain Res. Bull. 2018, 142, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, F.; Hader, W.; Yong1, V.W. Minocycline attenuates T cell and microglia activity to impair cytokine production in T cell-microglia interaction. J. Leukoc. Biol. 2005, 78, 135–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenblat, J.D.; McIntyre, R.S. Efficacy and tolerability of minocycline for depression: A systematic review and meta-analysis of clinical trials. J. Affect. Disord. 2018, 227, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Vogt, M.A.; Mallien, A.S.; Pfeiffer, N.; Inta, I.; Gass, P.; Inta, D. Minocycline does not evoke anxiolytic and antidepressant-like effects in C57BL/6 mice. Behav. Brain Res. 2016, 301, 96–101. [Google Scholar] [CrossRef]
- Gao, R.; Li, X. Risk assessment and aspirin use in Asian and Western populations. Vasc. Health Risk Manag. 2010, 6, 943. [Google Scholar]
- Jonker, C.; Comijs, H.C.; Smit, J.H. Does aspirin or other NSAIDs reduce the risk of cognitive decline in elderly persons? Results from a population-based study. Neurobiol. Aging 2003, 24, 583–588. [Google Scholar] [CrossRef]
- Saito, Y.; Okada, S.; Ogawa, H.; Soejima, H.; Sakuma, M.; Nakayama, M.; Doi, N.; Jinnouchi, H.; Waki, M.; Masuda, I.; et al. Low-dose aspirin for primary prevention of cardiovascular events in patients with type 2 diabetes mellitus: 10-year follow-up of a randomized controlled trial. Circulation 2017, 135, 659–670. [Google Scholar] [CrossRef]
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram summarizing the studies identified during the literature search and the abstraction process.
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram summarizing the studies identified during the literature search and the abstraction process.

Figure 2.
Forest plot showing pooled hazard ratios for the effect of ASA exposure on incident depression.
Figure 2.
Forest plot showing pooled hazard ratios for the effect of ASA exposure on incident depression.


Table 1.
Clinical studies investigating the effects of acetylsalicylic acid (ASA) on mood disorders (arranged alphabetically by first author’s last name).
Table 1.
Clinical studies investigating the effects of acetylsalicylic acid (ASA) on mood disorders (arranged alphabetically by first author’s last name).
| Author, Year | Study Design | Sample Size (N) | Study Population and Duration | Country of Origin | Conclusions |
|---|---|---|---|---|---|
| Saroukhani, 2013 [18] | Randomized, placebo-controlled, double-blind | 32 | Males with stable bipolar affective disorder (DSM-IV-TR) on maintenance lithium therapy; 6 weeks | Iran | Patients who received aspirin (240 mg/day) had significant improvements in total sexual function and erective function domain scores than placebo group. Baseline and endpoint serum lithium concentrations and mood symptoms remained stable throughout the duration of the study. |
| Savitz, 2018 [19] | Multi-site, randomized, placebo-controlled, double-blind | 99 | At least moderately depressed psychiatric outpatients with Bipolar I, II or NOS (DSM-IV-TR criteria); 6 weeks | United States | Active minocycline (100 mg twice daily) and aspirin (81 mg twice daily) significantly improved depressive symptoms. There was a main effect of aspirin on treatment response. |
| Stolk, 2010 [20] | Retrospective linkage record | 5145 | Patients ≥18 years old, who had been dispensed at least five prescriptions for lithium; 10-year period of observation | Netherlands | Presumably, low-dose ASA (30 or 80 mg/day) significantly reduced the relative risk of clinical deteriorations in patients on lithium (adjusted incidence density of medication events (dose increase or drug change) was 0.84, 95% CI: 0.75 to 0.94). |
| Pasco, 2010 [14] | Study 1: Nested case–control | 386 | Community-dwelling females; followed for 10 years; population derived from the Geelong Osteoporosis Study | Australia | ASA use associated with protective effect against major depression (age-adjusted OR 0.18, 95% CI: 0.02 to 1.39, p = 0.1). |
| Study 2: Retrospective cohort | 345 | Reduced risk of major depression in individuals with history of ASA and statin exposure (HR 0.20, 95% CI: 0.04 to 0.85, p = 0.03). | |||
| Veronese, 2018 [17] | Longitudinal cohort | 4070 | Community-dwelling adults; followed for 8 years; population derived from ongoing multicenter, longitudinal Osteoarthritis Initiative (OAI) study | United States | Adjusting for confounders, ASA use did not protect against incident depressive symptoms over the study period of 8 years (HR 1.12; 95% CI: 0.78 to 1.62, p = 0.54). |
| Williams, 2016 [21] | Study 1: Nested case–control | 937 | Community-dwelling males, 24–98 years old; followed for 5 years; population derived from ongoing Geelong Osteoporosis Study | Australia | After adjustment for age and antidepressant use, exposure to ASA was associated with a reduced likelihood of major depression (OR 0.4, 95% CI: 0.2 to 0.9, p = 0.03). |
| Study 2: Retrospective cohort | 836 | Reduced risk of major depression in individuals with history of ASA and statin use (HR 0.55, 95% CI: 0.23 to 1.32, p = 0.18). |
Abbreviations: ASA, aspirin; DSM-IV-TR, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition Text Revision; HR, hazard ratio; OR, odds ratio; CI, confidence interval.
Table 2.
The Newcastle–Ottawa Scale for assessing the quality of cohort studies reviewed.
| Study | Representativeness of the Exposed Cohort a | Selection of the Non-Exposed Cohort a | Ascertainment of Exposure a | Demonstration that Outcome of Interest was Not Present at Start of Study a | Comparability of Cohorts b | Assessment of Outcome a | Follow-up Duration a | Follow-up Adequacy a |
|---|---|---|---|---|---|---|---|---|
| Pasco, 2010 (Study 2) [14] | * | * | * | * | ** | * | * | * |
| Veronese, 2018 [17] | * | * | * | * | ** | * | * | * |
| Williams, 2016 (Study 2) [21] | * | * | * | * | ** | * | * | * |
a A study can be awarded a maximum of one star. b A maximum of two stars can be given for comparability.


{kind=link}
{kind=link}
{kind=link}
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ng, Q.X.; Ramamoorthy, K.; Loke, W.; Lee, M.W.L.; Yeo, W.S.; Lim, D.Y.; Sivalingam, V. Clinical Role of Aspirin in Mood Disorders: A Systematic Review. Brain Sci. 2019, 9, 296. https://doi.org/10.3390/brainsci9110296
AMA Style
Ng QX, Ramamoorthy K, Loke W, Lee MWL, Yeo WS, Lim DY, Sivalingam V. Clinical Role of Aspirin in Mood Disorders: A Systematic Review. Brain Sciences. 2019; 9(11):296. https://doi.org/10.3390/brainsci9110296
Chicago/Turabian StyleNg, Qin Xiang, Krishnapriya Ramamoorthy, Wayren Loke, Matthew Wei Liang Lee, Wee Song Yeo, Donovan Yutong Lim, and Vivekanandan Sivalingam. 2019. "Clinical Role of Aspirin in Mood Disorders: A Systematic Review" Brain Sciences 9, no. 11: 296. https://doi.org/10.3390/brainsci9110296
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.