Behavioral and Electrophysiological Arguments in Favor of a Relationship between Impulsivity, Risk-Taking, and Success on the Iowa Gambling Task

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Tasks
2.2.1. Iowa Gambling Task
2.2.2. EEG Recording at Rest
2.2.3. Balloon Analog Risk Task
2.3. Data Analyses
3. Results
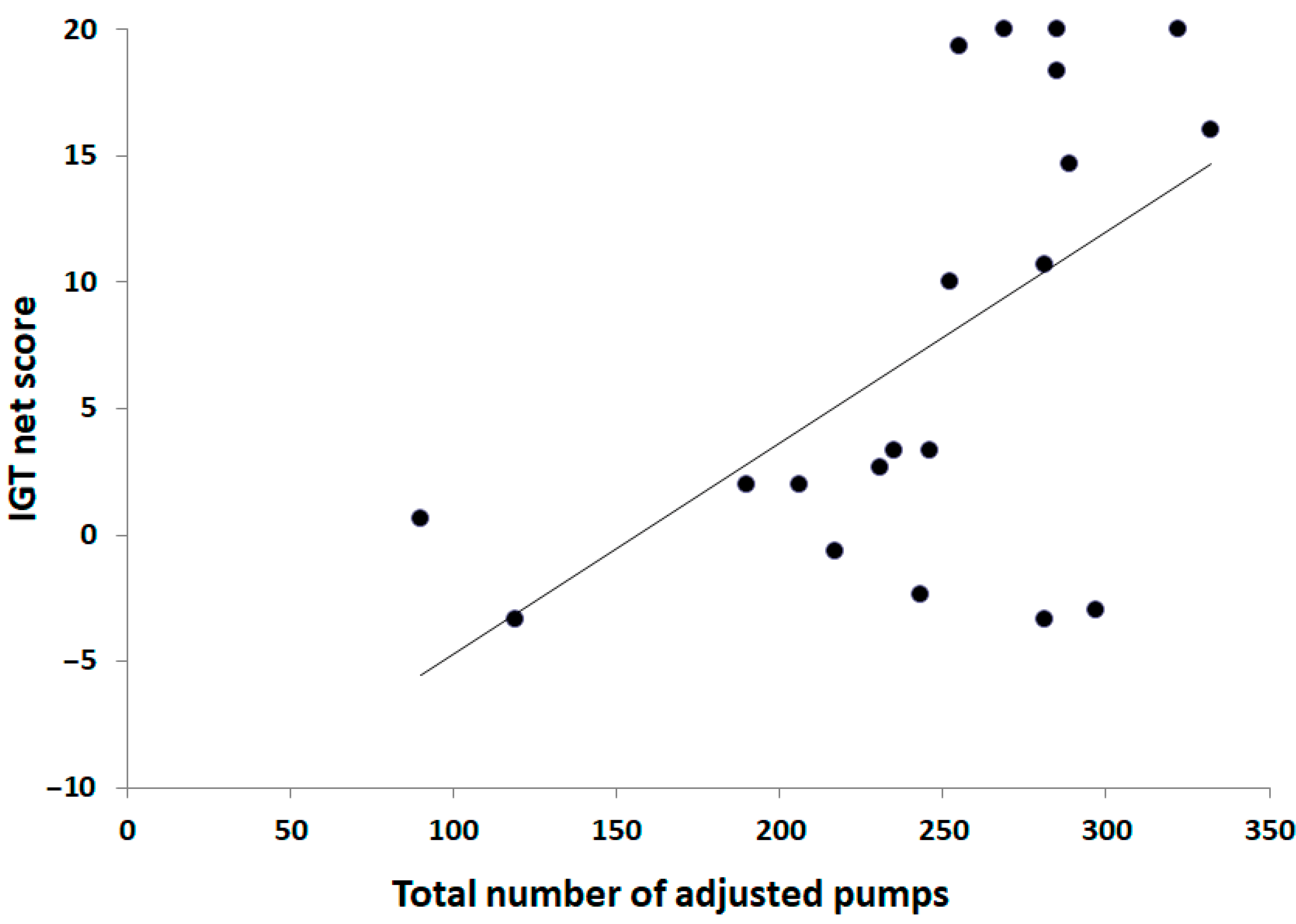
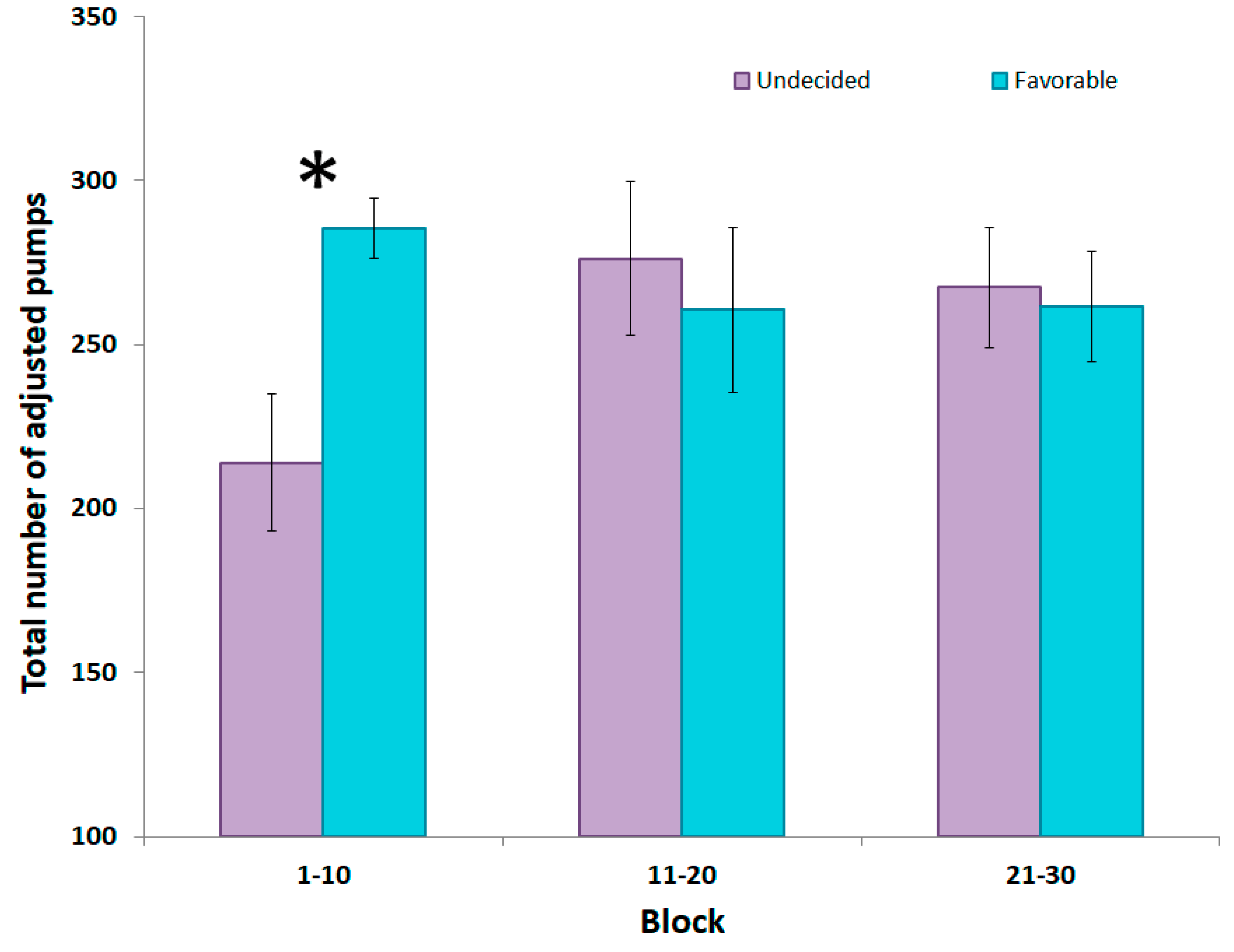
3.1. Relationship between the Participants’ Strategy on the IGT and Risk-Taking on the BART
3.2. Relationship between the Participants’ Strategy on the IGT and Impulsivity
3.3. Relationship between Impulsivity and Risk-Taking
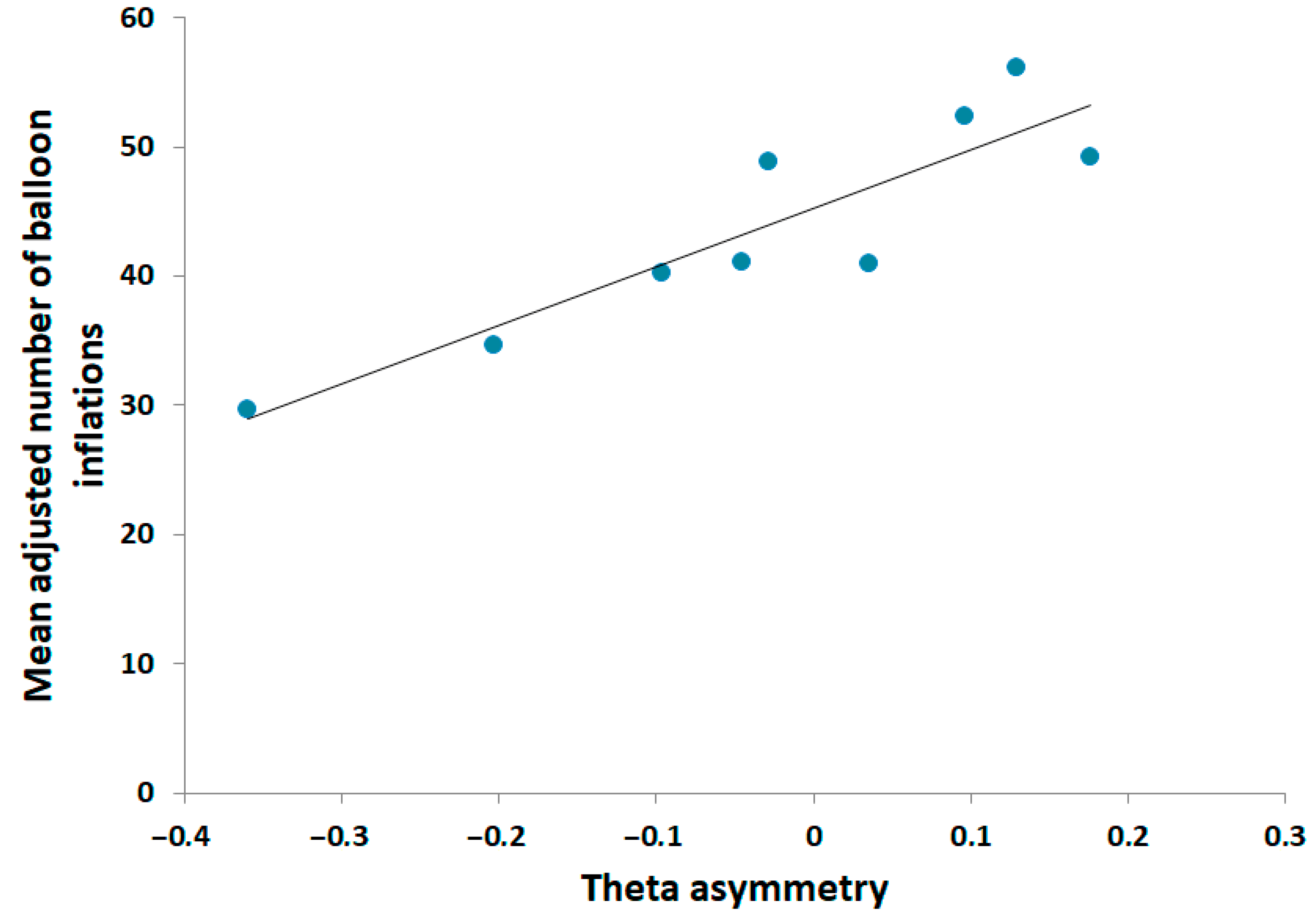
3.4. Relationship between Cortical Asymmetry and Behavioral Scores
4. Discussion
4.1. Association between Decision-Making, Risk-Taking, and Impulsivity
4.2. Association between Impulsivity and Risk-Taking
4.3. Association between Neural Activity and Behavioral Performance
4.4. Impulsivity, Risk-Taking, and Decision-Making
4.5. Limitations and Recommendations for Future Works
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bechara, A.; Damasio, A.R. The somatic marker hypothesis: A neural theory of economic decision. Games Econ. Behav. 2005, 52, 336–372. [Google Scholar] [CrossRef]
- Platt, M.L.; Huettel, S.A. Risky business: the neuroeconomics of decision making under uncertainty. Nat. Neurosci. 2008, 11, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Cavedini, P.; Riboldi, G.; D’Annucci, A.; Belotti, P.; Cisima, M.; Bellodi, L. Decision-making heterogeneity in obsessive-compulsive disorder: Ventromedial prefrontal cortex function predicts different treatment outcomes. Neuropsychologia 2002, 40, 205–211. [Google Scholar] [CrossRef]
- Cavedini, P.; Bassi, T.; Ubbiali, A.; Casolari, A.; Giordani, S.; Zorzi, C.; Bellodi, L. Neuropsychological investigation of decision-making in anorexia nervosa. Psychiatry Res. 2004, 127, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Jollant, F.; Guillaume, S.; Jaussent, I.; Castelnau, D.; Malafosse, A.; Courtet, P. Impaired decision-making in suicide attempters may increase the risk of problems in affective relationships. J. Affect. Disord. 2007, 99, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Cavedini, P.; Riboldi, G.; Keller, R.; D’Annucci, A.; Bellodi, L. Frontal lobe dysfunction in pathological gambling patients. Biol. Psychiatry 2002, 51, 334–341. [Google Scholar] [CrossRef]
- Bechara, A.; Damasio, H. Decision-making and addiction (part I): impaired activation of somatic states in substance dependent individuals when pondering decisions with negative future consequences. Neuropsychologia 2002, 40, 1675–1689. [Google Scholar] [CrossRef]
- Bechara, A.; Dolan, S.; Hindes, A. Decision-making and addiction (part II): myopia for the future or hypersensitivity to reward? Neuropsychologia 2002, 40, 1690–1705. [Google Scholar] [CrossRef]
- Tanabe, J.; Thompson, L.; Claus, E.; Dalwani, M.; Hutchison, K.; Banich, M.T. Prefrontal cortex activity is reduced in gambling and nongambling substance users during decision-making. Hum. Brain Mapp. 2007, 28, 1276–1286. [Google Scholar] [CrossRef]
- Bechara, A.; Damasio, A.R.; Damasio, H.; Anderson, S.W. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition 1994, 50, 7–15. [Google Scholar] [CrossRef]
- Oberg, S.A.K.; Christie, G.J.; Tata, M.S. Problem gamblers exhibit reward hypersensitivity in medial frontal cortex during gambling. Neuropsychologia 2011, 49, 3768–3775. [Google Scholar] [CrossRef] [PubMed]
- Bagneux, V.; Thomassin, N.; Gonthier, C.; Roulin, J.-L. Working memory in the processing of the Iowa Gambling Task: an individual differences approach. PLoS ONE 2013, 8, e81498. [Google Scholar] [CrossRef] [PubMed]
- Bechara, A.; Dolan, S.; Denburg, N.; Hindes, A.; Anderson, S.W.; Nathan, P.E. Decision-making deficits, linked to a dysfunctional ventromedial prefrontal cortex, revealed in alcohol and stimulant abusers. Neuropsychologia 2001, 39, 376–389. [Google Scholar] [CrossRef]
- Giustiniani, J.; Gabriel, D.; Nicolier, M.; Monnin, J.; Haffen, E. Neural Correlates of Successful and Unsuccessful Strategical Mechanisms Involved in Uncertain Decision-Making. PLoS ONE 2015, 10, e0130871. [Google Scholar] [CrossRef] [PubMed]
- Mapelli, D.; Di Rosa, E.; Cavalletti, M.; Schiff, S.; Tamburin, S. Decision and dopaminergic system: an ERPs study of Iowa gambling task in Parkinson’s disease. Front. Psychol. 2014, 5, 684. [Google Scholar] [CrossRef]
- Dunn, B.D.; Dalgleish, T.; Lawrence, A.D. The somatic marker hypothesis: a critical evaluation. Neurosci. Biobehav. Rev. 2006, 30, 239–271. [Google Scholar] [CrossRef]
- Xu, S.; Korczykowski, M.; Zhu, S.; Rao, H. Assessment of risk-taking and impulsive behaviors: A comparison between three tasks. Soc. Behav. Personal. 2013, 41, 477–486. [Google Scholar] [CrossRef]
- Patton, J.H.; Stanford, M.S.; Barratt, E.S. Factor structure of the Barratt impulsiveness scale. J. Clin. Psychol. 1995, 51, 768–774. [Google Scholar] [CrossRef]
- Swann, A.C.; Bjork, J.M.; Moeller, F.G.; Dougherty, D.M. Two models of impulsivity: relationship to personality traits and psychopathology. Biol. Psychiatry 2002, 51, 988–994. [Google Scholar] [CrossRef]
- Grassi, G.; Pallanti, S.; Righi, L.; Figee, M.; Mantione, M.; Denys, D.; Piccagliani, D.; Rossi, A.; Stratta, P. Think twice: Impulsivity and decision making in obsessive-compulsive disorder. J. Behav. Addict. 2015, 4, 263–272. [Google Scholar] [CrossRef]
- Ochoa, C.; Alvarez-Moya, E.M.; Penelo, E.; Aymami, M.N.; Gómez-Peña, M.; Fernández-Aranda, F.; Granero, R.; Vallejo-Ruiloba, J.; Menchón, J.M.; Lawrence, N.S.; et al. Decision-making deficits in pathological gambling: the role of executive functions, explicit knowledge and impulsivity in relation to decisions made under ambiguity and risk. Am. J. Addict. 2013, 22, 492–499. [Google Scholar] [CrossRef]
- Goudriaan, A.E.; Oosterlaan, J.; de Beurs, E.; van den Brink, W. Decision making in pathological gambling: a comparison between pathological gamblers, alcohol dependents, persons with Tourette syndrome, and normal controls. Brain Res. Cogn. Brain Res. 2005, 23, 137–151. [Google Scholar] [CrossRef] [PubMed]
- Franken, I.H.A.; van Strien, J.W.; Nijs, I.; Muris, P. Impulsivity is associated with behavioral decision-making deficits. Psychiatry Res. 2008, 158, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Lejuez, C.W.; Read, J.P.; Kahler, C.W.; Richards, J.B.; Ramsey, S.E.; Stuart, G.L.; Strong, D.R.; Brown, R.A. Evaluation of a behavioral measure of risk taking: The Balloon Analogue Risk Task (BART). J. Exp. Psychol. Appl. 2002, 8, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Lejuez, C.W.; Aklin, W.M.; Zvolensky, M.J.; Pedulla, C.M. Evaluation of the Balloon Analogue Risk Task (BART) as a predictor of adolescent real-world risk-taking behaviours. J. Adolesc. 2003, 26, 475–479. [Google Scholar] [CrossRef]
- Ríos-Bedoya, C.F.; Wilcox, H.C.; Piazza, M.; Anthony, J.C. Children taking risks: the association with cocaine and other drug use by young adulthood. Addict. Behav. 2008, 33, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Jain, L.C.; Zhang, G. Risk Management in Decision Making. In Handbook on Decision Making: Vol 2: Risk Management in Decision Making; Lu, J., Jain, L.C., Zhang, G., Eds.; Intelligent Systems Reference Library; Springer: Berlin/Heidelberg, Germany, 2012; pp. 3–7. ISBN 978-3-642-25755-1. [Google Scholar]
- Upton, D.J.; Bishara, A.J.; Ahn, W.-Y.; Stout, J.C. Propensity for risk taking and trait impulsivity in the Iowa Gambling Task. Personal. Individ. Differ. 2011, 50, 492–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bechara, A.; Damasio, H.; Damasio, A.R. Emotion, decision making and the orbitofrontal cortex. Cereb. Cortex N. Y. N 1991 2000, 10, 295–307. [Google Scholar] [CrossRef] [PubMed]
- Gianotti, L.R.R.; Knoch, D.; Faber, P.L.; Lehmann, D.; Pascual-Marqui, R.D.; Diezi, C.; Schoch, C.; Eisenegger, C.; Fehr, E. Tonic activity level in the right prefrontal cortex predicts individuals’ risk taking. Psychol. Sci. 2009, 20, 33–38. [Google Scholar] [CrossRef]
- Schutter, D.J.L.G.; de Haan, E.H.F.; van Honk, J. Anterior asymetrical alpha activity predicts Iowa gambling performance: distinctly but reversed. Neuropsychologia 2004, 42, 939–943. [Google Scholar] [CrossRef]
- Balconi, M.; Finocchiaro, R. Decisional impairments in cocaine addiction, reward bias, and cortical oscillation “unbalance”. Neuropsychiatr. Dis. Treat. 2015, 11, 777–786. [Google Scholar] [CrossRef] [PubMed]
- Balconi, M.; Mazza, G. Brain oscillations and BIS/BAS (behavioral inhibition/activation system) effects on processing masked emotional cues. ERS/ERD and coherence measures of alpha band. Int. J. Psychophysiol. Off. J. Int. Organ. Psychophysiol. 2009, 74, 158–165. [Google Scholar]
- Davidson, R.J. What does the prefrontal cortex “do” in affect: perspectives on frontal EEG asymmetry research. Biol. Psychol. 2004, 67, 219–233. [Google Scholar] [CrossRef] [PubMed]
- Harmon-Jones, E. Contributions from research on anger and cognitive dissonance to understanding the motivational functions of asymmetrical frontal brain activity. Biol. Psychol. 2004, 67, 51–76. [Google Scholar] [CrossRef] [PubMed]
- Bechara, A.; Damasio, H.; Tranel, D.; Damasio, A.R. Deciding advantageously before knowing the advantageous strategy. Science 1997, 275, 1293–1295. [Google Scholar] [CrossRef] [PubMed]
- Lejoyeux, M. Abrégés Addictologie; Masson: Paris, France, 2009. [Google Scholar]
- Reynaud, M. Usage nocif de substances psychoactives; La documentation française: Paris, France, 2002. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Carbin, M.G. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clin. Psychol. Rev. 1988, 8, 77–100. [Google Scholar] [CrossRef]
- Yao, S.N.; Note, I.; Fanget, F.; Albuisson, E.; Bouvard, M.; Jalenques, I.; Cottraux, J. [Social anxiety in patients with social phobia: Validation of the Liebowitz social anxiety scale: The French version]. L’Encéphale 1999, 25, 429–435. [Google Scholar] [PubMed]
- Plaisant, O.; Courtois, R.; Réveillère, C.; Mendelsohn, G.A.; John, O.P. Validation par analyse factorielle du Big Five Inventory français (BFI-Fr). Analyse convergente avec le NEO-PI-R. Ann. Méd.-Psychol. Rev. Psychiatr. 2010, 168, 97–106. [Google Scholar] [CrossRef]
- Bouvard, M. Questionnaires et échelles d’évaluation de la personnalité; Elsevier Masson: Paris, France, 2009. [Google Scholar]
- Monterosso, J.; Ehrman, R.; Napier, K.L.; O’Brien, C.P.; Childress, A.R. Three decision-making tasks in cocaine-dependent patients: Do they measure the same construct? Addict. Abingdon Engl. 2001, 96, 1825–1837. [Google Scholar] [CrossRef]
- De Groot, K.; Thurik, R. Disentangling Risk and Uncertainty: When Risk-Taking Measures Are Not About Risk. Front. Psychol. 2018, 9. [Google Scholar] [CrossRef]
- Brand, M.; Recknor, E.C.; Grabenhorst, F.; Bechara, A. Decisions under ambiguity and decisions under risk: Correlations with executive functions and comparisons of two different gambling tasks with implicit and explicit rules. J. Clin. Exp. Neuropsychol. 2007, 29, 86–99. [Google Scholar] [CrossRef] [PubMed]
- Buelow, M.T.; Suhr, J.A. Construct validity of the Iowa Gambling Task. Neuropsychol. Rev. 2009, 19, 102–114. [Google Scholar] [CrossRef] [PubMed]
- Gomide Vasconcelos, A.; Sergeant, J.; Corrêa, H.; Mattos, P.; Malloy-Diniz, L. When self-report diverges from performance: The usage of BIS-11 along with neuropsychological tests. Psychiatry Res. 2014, 218, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Vigil-Colet, A. Impulsivity and decision making in the balloon analogue risk-taking task. Personal. Individ. Differ. 2007, 43, 37–45. [Google Scholar] [CrossRef]
- Dickman, S.J. Functional and dysfunctional impulsivity: Personality and cognitive correlates. J. Pers. Soc. Psychol. 1990, 58, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Smillie, L.D.; Jackson, C.J. Functional impulsivity and reinforcement sensitivity theory. J. Pers. 2006, 74, 47–84. [Google Scholar] [CrossRef] [PubMed]
- Panwar, K.; Rutherford, H.J.V.; Mencl, W.E.; Lacadie, C.M.; Potenza, M.N.; Mayes, L.C. Differential associations between impulsivity and risk-taking and brain activations underlying working memory in adolescents. Addict. Behav. 2014, 39, 1606–1621. [Google Scholar] [CrossRef] [PubMed]
- Black, C.L.; Goldstein, K.E.; LaBelle, D.R.; Brown, C.W.; Harmon-Jones, E.; Abramson, L.Y.; Alloy, L.B. Behavioral approach system sensitivity and risk taking interact to predict left-frontal EEG asymmetry. Behav. Ther. 2014, 45, 640–650. [Google Scholar] [CrossRef] [PubMed]
- Schutter, D.J.L.G.; Van Honk, J. Electrophysiological ratio markers for the balance between reward and punishment. Brain Res. Cogn. Brain Res. 2005, 24, 685–690. [Google Scholar] [CrossRef]
- Studer, B.; Pedroni, A.; Rieskamp, J. Predicting Risk-Taking Behavior from Prefrontal Resting-State Activity and Personality. PLoS ONE 2013, 8, e76861. [Google Scholar] [CrossRef]
- Sutton, S.K.; Davidson, R.J. Prefrontal Brain Asymmetry: A Biological Substrate of the Behavioral Approach and Inhibition Systems. Psychol. Sci. 1997, 8, 204–210. [Google Scholar] [CrossRef]
- Harmon-Jones, E.; Allen, J.J. Behavioral activation sensitivity and resting frontal EEG asymmetry: Covariation of putative indicators related to risk for mood disorders. J. Abnorm. Psychol. 1997, 106, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Knyazev, G.G. Motivation, emotion, and their inhibitory control mirrored in brain oscillations. Neurosci. Biobehav. Rev. 2007, 31, 377–395. [Google Scholar] [CrossRef] [PubMed]
- Harmon-Jones, E. Early Career Award. Clarifying the emotive functions of asymmetrical frontal cortical activity. Psychophysiology 2003, 40, 838–848. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zheng, J.; Huang, S.; Sun, H. P300 and Decision Making under Risk and Ambiguity. Comput. Intell. Neurosci. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Van den Bos, R.; Homberg, J.; de Visser, L. A critical review of sex differences in decision-making tasks: Focus on the Iowa Gambling Task. Behav. Brain Res. 2013, 238, 95–108. [Google Scholar] [CrossRef]
- Lighthall, N.R.; Mather, M.; Gorlick, M.A. Acute stress increases sex differences in risk seeking in the balloon analogue risk task. PLoS ONE 2009, 4, e6002. [Google Scholar] [CrossRef]
- Mata, R.; Josef, A.K.; Samanez-Larkin, G.R.; Hertwig, R. Age differences in risky choice: A meta-analysis. Ann. N. Y. Acad. Sci. 2011, 1235, 18–29. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Favorable Groups | Undecided Group | Favorable versus Undecided Group | ||
|---|---|---|---|---|
| Average | Average | t-Value | p-Value | |
| (SD) | (SD) | (Two Tailed) | ||
| BDI | 1.11 (0.93) | 2 (2.14) | −1.15 | 0.26 |
| BFI-Fr | ||||
| Neuroticism | 21.33 (5.36) | 18.63 (7.03) | 0.95 | 0.36 |
| Extraversion | 27.33 (5.70) | 26.09 (6.11) | 0.47 | 0.65 |
| Openness to experience | 36.33 (6.12) | 35.54 (5.64) | 0.29 | 0.77 |
| Agreableness | 41.55 (5.08) | 42.18 (6.29) | −0.24 | 0.81 |
| Conscientiousness | 33.67 (7.50) | 36.45 (4.99) | −0.99 | 0.33 |
| LIEBOWITZ SCALE | 6.36 (1.49) | 5.20 (1.08) | 0.64 | 0.53 |
| Performance | 6.05 (1.96) | 5.91 (0.77) | 0.08 | 0.93 |
| Anxiety | 7.44 (4.27) | 6.45 (5.14) | 0.46 | 0.65 |
| Avoidance | 4.67 (3.74) | 5.36 (4.13) | −0.39 | 0.7 |
| Social interaction | 6.67 (1.57) | 4.50 (0.96) | 1.06 | 0.3 |
| Anxiety | 7.78 (5.47) | 5.18 (4.64) | 1.15 | 0.27 |
| Avoidance | 5.55 (5.34) | 3.81 (4.24) | 0.81 | 0.43 |
| AUDIT | 4.55 (3.74) | 2.36 (2.16) | 1.64 | 0.12 |
| Fagerström Scale | 0.44 (1.33) | 0.18 (0.60) | 0.59 | 0.56 |
| DETC/CAGE | 0 | 0 | - | - |
| SOGS | 0 | 0.09 (0.30) | −0.9 | 0.38 |
| BART | ||||||
|---|---|---|---|---|---|---|
| Average | Total | |||||
| Whole Subjects | Advantageous | Undecided | Whole Subjects | Advantageous | Undecided | |
| N = 20 | N = 9 | N = 11 | N = 20 | N = 9 | N = 11 | |
| BIS-10 motor | −0.16 (−0.69) | - | - | 0.39 (1.80) | - | - |
| BIS-10 cognitive | −0.68 (−3.89) * | 0.16 (0.44) | −0.68 (−3.59) * | −0.33 (−1.50) | - | - |
| BIS-10 no planning | −0.35 (−1.58) | - | - | −0.27 (−1.20) | - | - |
| BIS-10 total | −0.50 (−2.43) | - | - | −0.03 (−0.14) | - | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giustiniani, J.; Joucla, C.; Bennabi, D.; Nicolier, M.; Chabin, T.; Masse, C.; Trojak, B.; Vandel, P.; Haffen, E.; Gabriel, D. Behavioral and Electrophysiological Arguments in Favor of a Relationship between Impulsivity, Risk-Taking, and Success on the Iowa Gambling Task. Brain Sci. 2019, 9, 248. https://doi.org/10.3390/brainsci9100248
Giustiniani J, Joucla C, Bennabi D, Nicolier M, Chabin T, Masse C, Trojak B, Vandel P, Haffen E, Gabriel D. Behavioral and Electrophysiological Arguments in Favor of a Relationship between Impulsivity, Risk-Taking, and Success on the Iowa Gambling Task. Brain Sciences. 2019; 9(10):248. https://doi.org/10.3390/brainsci9100248
Chicago/Turabian StyleGiustiniani, Julie, Coralie Joucla, Djamila Bennabi, Magali Nicolier, Thibault Chabin, Caroline Masse, Benoît Trojak, Pierre Vandel, Emmanuel Haffen, and Damien Gabriel. 2019. "Behavioral and Electrophysiological Arguments in Favor of a Relationship between Impulsivity, Risk-Taking, and Success on the Iowa Gambling Task" Brain Sciences 9, no. 10: 248. https://doi.org/10.3390/brainsci9100248