1. Introduction
The pelvis is a complex ring structure in which both hemi-pelvises are connected dorsally via the sacrum and ventrally via the pubic symphysis. The pubic symphysis is a non-synovial, amphiar-throtic joint with the opposing pubic bone surfaces covered by a thin, hyaline layer of cartilage and with the discus interpubicus, a fibrocartilaginous disc, firmly anchored in between them. Circumfer-ential ligaments provide the pubic symphysis with a passive, mechanical stability [
1]. The pubic symphysis is subjected to tensile strain when standing (bipedal stand), to pressure while in a supine position, and to shear while walking (lifting the swinging leg) [
2]. Injuries and damage to the pubic symphysis are of the utmost significance, especially in high-performance and professional sports, and can lead to prolonged idle times of up to 2 years. Predisposed sports include soccer, rugby, and American football, that is, sports with quick changes of direction or sprint and interval strain [
3]. Regardless of the sports practiced, however, athletes with biomechanical deficits, such as different leg lengths, pelvic instability, or restricted flexibility in the hip joints, can also be affected. For professional athletes, the incidence of chronic athletic pubalgia is estimated to range between 0.5 and 6.2% [
4]. The highest values (up to 18%) are found in ice hockey and soccer players [
5]. More detailed numbers, particularly pertaining to young athletes, cannot be derived from international literature owing to the inhomogeneity of studies.
If both hemi-pelvises move in opposite directions in the sagittal plane, minimal torsions in a millimeter range occur in the joints involved. Such a pelvic torsion triggers shearing forces in the sacroiliac joints and the pubic symphysis. Repetitive mechanical strain can lead to symphyseal instability and consequently cause unphysiologically high shearing forces in the pubic symphysis. This is considered the etiological factor that most frequently leads to complaints [
6,
7].
For prevention purposes, it is thus important to identify at an early stage potential factors that may lead to unfavorable strain of the pubic symphysis. Potential causes being discussed include reduced muscular flexibility, an existing deformity (e.g., femoroacetabular impingement) [
8,
9], or muscular imbalances [
10,
11]. Muscular, antagonist concatenations with insertion directly at the pubic symphysis (esp. rectus abdominis, adductors) or with an immediate effect on the pubic symphysis (especially psoas/gluteus, rectus femoris/hamstrings) play a significant role in the mechanical strain of the pubic symphysis. Early on, Meyers et al. postulated that imbalances between rectus abdominis and adductor muscles would result in secondary symptomatic pubic symphysis instability and pain [
12]. Tyler et al. showed that, in ice hockey players, injuries of the adductor muscles and tendons close to the pubic symphysis were 17 times more likely to occur when the strength of the adductors was 80% less than that of the abductor muscles [
13].
The influence of muscular activity on the pelvic position is particularly interesting because it might be a possible approach to derive both preventive and curative intervention methods. Also of particular interest are those muscle groups that are able to influence the anteversion of the hemi-pelvises, such as rectus femoris (as part of the quadriceps femoris muscle) and hamstrings [
14]. With extended knees, both muscle groups act as antagonists to the pelvic anteversion or retroversion, respectively.
This study thus aims to identify any potential interconnection between the maximum torques of quadriceps and hamstrings and the spatial positioning of the hemi-pelvises, as well as the tenderness to palpation of the pubic symphysis in healthy young athletes.
This study aimed to verify the following:
- (i)
whether imbalances of the force ratio of quadriceps and hamstrings when comparing sides have an impact on the three-dimensional positioning of the hemi-pelvises in habitual upright posture;
- (ii)
whether changes to the pain on palpation occur in the pubic symphysis depending on the three-dimensional positioning of the hemi-pelvises in habitual upright posture.
2. Materials and Methods
2.1. Test Subjects
Thirty-seven adolescents participated in a routine posture examination within the framework of an interdisciplinary research project (Kid-Check). At the time of testing, they were asymptomatic and without any obvious orthopedic, neurological, or internal diagnoses. Exclusion criteria were anatomical or functional leg length discrepancy or functional limitations in the sacroiliac joints. The study includes data from 26 male young athletes who fulfilled the inclusion criteria (see
Table 1 for anthropometric data). Of the 26 athletes, 18 were soccer players, 4 track and field athletes, 3 handball players, 1 biathlete, 1 fitness athlete (machine-assisted resistance training), and 1 fencer. The adolescents and their parents were informed of the intention and procedure of the study and gave their written informed consent in accordance with the Declaration of Helsinki. The university’s ethics commission approved the study (Ref. Nr. 15-03/05).
2.2. Manual Testing
Before the actual measurement, the sacroiliac joints were tested for dysfunction by means of a test cluster comprising a sacral thrust test, distraction test, and Gaenslen’s test [
15]. Applying a visual metric analog scale from 0 (no pain) to 10 (maximum pain), the test persons assessed the tenderness to palpation of the pubic symphysis [
16]. As it is known that a leg length discrepancy influences pelvic torsion [
17,
18], it was checked in advance by photometric comparison of the positions of the posterior superior iliac spines (PSIS) and the anterior superior iliac spines (ASIS). Furthermore, 3 of the 37 interested subjects were excluded during posture analysis because of a scoliotic malposition of the spine owing to a potential correlation with malpositioning of the hemi-pelvises [
19].
2.3. Three-Dimensional Posture Measurement
To determine the three-dimensional pelvis contour, marker spheres (diameter 8 mm) were applied to anatomical landmarks on the shaved skin in the pelvic area [
20] by means of double-sided adhesive pads (
Figure 1). All palpations were performed by the same experienced examiner. The test persons were standing in habitual posture, arms crossed in front of the chest. Three-dimensional posture scans were performed dorsally and ventrally using the Rothballer 3D Scanner (Rothballer electronic systems, Weiden, Germany). This system generated a three-dimensional image of the pelvis in the shape of a mathematical point cloud. System reliability and validity for postural measurements have been confirmed by other studies (comparable inter-trial reliability to 3D motion analysis systems: intraclass correlation coefficient difference = 0.06 ± 0.05, range 0.00−0.16; very good validity: Pearson’s r = 0.96 ± 0.04; range 0.84−0.99 [
21,
22]).
For the evaluation, the position of the marker spheres was determined individually using the analysis software, and their spatial coordinates were extracted. The marker spheres on the trochanters were visible on both 3D images and served as reference points for the spatial coordinates of all points.
Figure 2 shows the simplified geometries of both hemi-pelvises, calculated trigonometrically from the coordinates. The torsion of both triangles against each other was calculated as an angle using MATLAB (R230a, MathWorks Inc., Natick, MA, USA) and Microsoft Excel (Microsoft, Redmond, WA, USA); this angle was then used as the measured value for pelvic torsion. In addition, pelvic anteversion was calculated as the angle of the connection line between pubic symphysis and S1 and the horizontal.
2.4. Error Analysis
The accuracy of the determination of the forward tilt of the pelvis and thus pelvic torsion depends on the accuracy of marker spheres’ placement on the skin. In a preliminary study, the retest reliability of marker positioning was determined by the same investigator on twelve subjects from the test group at intervals of one day. Cronbach’s alpha was 0.998 and confirmed a very good reliability. The mean deviation of the marker spheres was 1.4 ± 0.9 mm. Therefore, an assumed inaccuracy of ±1 mm in marker positioning and an average pelvis depth of 200 mm lead to a calculated error of <1.5°, which ensures sufficient distinguishability of the groups when looking at the group mean values (
Table 2), and thus an acceptable inaccuracy.
2.5. Isometric Torque Measurement
The maximum isometric torques for knee flexion and extension were measured in a sitting position using an isometry measurement device (Easytorque, Fa. Tonus, Zemmer, Germany). The knee angle was set to 80 degrees for measuring knee flexion and to 90 degrees for knee extension (
Figure 3). The thighs were fixated with pads and the calves pressed isometrically against the pads, and thus against the force transducers. The test persons had to build up strength for five seconds and hold it for five more. For familiarization purposes, a trial was performed for each measurement. Both sides were tested alternatingly. At least three isometric measurements were performed for each side. Whenever the third value turned out to be the maximum value, further tests were performed until the last measurement value was smaller than the penultimate value. Only the maximum value achieved was included in the subsequent calculations. The reproducibility of this type of isometric measurement has been shown in other studies (intraclass correlation coefficient 0.97–0.99, Pearson’s correlation coefficient 0.95 [
23,
24].
2.6. Statistics
On the basis of the 3D model, the side with the strongest pelvic rotation was determined. The ipsilateral torque ratio,
(with Ex
IPSI = torque of the extension movement of the ipsilateral side and Flex
IPSI = torque of the flexion movement of the ipsilateral side), between knee extensors and flexors for this side was calculated, as well as the contralateral torque ratio,
(with Ex
CON = torque of the extension movement of the contralateral side and Flex
CON = torque of the flexion movement of the contralateral side), and the crossed torque ratio,
Afterwards, the test persons were divided into two groups based on the pelvic torsion median (2.15°): one group with lower pelvic torsion (pelvic torsion ≤ 2.15°; n = 13) and one with higher pelvic torsion (>2.15°; n = 13).
IBM SPSS Statistics 23 was used for calculating the statistical tests. The significance level was set to 0.05. The sample size could not be determined a priori, but was given by the number of subjects participating in the interdisciplinary research project (Kid-Check) at that time.
Testing for multicollinearity was done by calculating Pearson’s correlation coefficient r for all com bi nations of variables. After checking the starting conditions, a MANOVA with post hoc univariate ANOVAs was performed between the two groups for the variables IPSI Ex/Flex, CON Ex/Flex, and CTR. Partial η2 was calculated as effect size, with η2 < 0.06 indicating a small effect, values between 0.06 and 0.14 a medium effect, and η2 > 0.14 a large effect.
The variable ‘tenderness on palpation of the pubic symphysis’ (TPS) was not included in the MANOVA, because, according to our model, TPS would be the result and not the cause of pelvic torsion. Therefore, differences between the groups for tenderness on palpation were calculated separately using a one-way ANOVA.
Linear regression models were calculated for pelvic torsion, crossed torque ratio, and tenderness on palpation (bivariate regressions with pelvic torsion = dependent variable, CTR = independent variable, and pelvic torsion = independent variable, TPS = dependent variable), and R2 was determined.
3. Results
Correlations between the absolute torque values were high (Pearson’s correlation coeffi cient: IPSI Flex–CON Flex: r = 0.905; IPSI Ex–CON Ex: r = 0.871), and multicollinearity was thus present. Therefore, only the ratios IPSI Ex/Flex, CON Ex/Flex, and CTR were included in the following MANOVA. These variables were normally distributed in both groups, as assessed by the Shapiro–Wilk test (IPSI Ex/Flex: p = 0.224; CON Ex/Flex: p = 0.321; CTR: p = 0.876). There were no outliers in the data. No multivariate outliers were found, as assessed by the Mahalanobis distance MD (cut-off (3) = 16.27, MDmax = 7.78, p > 0.001). Linearity between the dependent variables was verified by visual inspection of the scatter plots.
The homogeneity of the error variances was checked with Levene’s test and showed no significance for the dependent variables (IPSI Ex/Flex: p = 0.517; CON Ex/Flex: p = 0.881; CTR: p = 0.779). Box’s test confirmed the homogeneity of covariances (p > 0.001).
The one-way MANOVA showed a statistically significant difference between the groups on the combined dependent variables, with F(3, 22) = 6.640, p = 0.002, partial η2 = 0.475, Wilk’s Λ = 0.525.
Post-hoc univariate ANOVAs showed no statistically significant difference between the groups for CON Ex/Flex, with F(1, 24) = 0.006, p = 0.941, and partial η2 < 0.001. However, a statistically significant difference between the two groups was found for IPSI Ex/Flex (F(1, 24) = 5.864, p = 0.023, partial η2 = 0.196) and for CTR (F(1, 24) = 19.885, p < 0.001, partial η2 = 0.453).
The group with the higher pelvic torsion angle exhibited a higher (but statistically not significant) torque in the extensors on the side of the anteverted hemi-pelvis (IPSI Ex), and consequently a statistically significant higher torque ratio between extensors and flexors (
Table 2). A contralateral difference between the flexor and extensor torque in both subgroups was not found. The torque ratio on the contralateral side (CON Ex/Flex) was also not significantly different. However, the crossed torque ratio at
p < 0.001 was significantly higher in the group with higher pelvic torsion (
Table 2). The effect size was partial η
2 = 0.453, which represents a large effect.
In the linear regression models, the crossed torque ratio (CTR) showed the strongest correlation with the pelvic torsion angle with a correlation coefficient of 0.668 (
Table 3).
At the same time, the subgroup with higher pelvic torsion reported statistically significant higher values for tenderness to palpation (
Table 2, partial η
2 = 0.309, large effect). The linear regression models showed that 39% of the variance of tenderness to palpation can be explained by the pelvic torsion angle and 44% of the variance of the pelvic torsion angle can be explained by the crossed torque ratio (
Figure 4).
4. Discussion
This study aimed to verify the existence of interconnections between contralateral imbalances of the torque ratios of quadriceps and hamstrings and the three-dimensional positioning of the hemi-pelvises. As a matter of fact, our results support this assumption because a significant difference of the calculated crossed torque ratio was found between the two groups with a lower and higher pelvic torsion angle.
The biomechanics of the pelvic bones and their joints is complex and has come into scientific focus over the past few years. Very low amplitude movements occur in the sacroiliac joints and the pubic symphysis, which could be the cause for complaints [
1,
25]. If we assume, in a simplified biomechanical model, that both hemi-pelvises are slightly twistable against each other (‘inflare’ [
26,
27]), three different cases can arise:
1. The torque ratios are balanced both anterior–posterior and left–right (
Figure 5a). Both hemi-pelvises are not tilted toward each other.
2. The absolute anterior and posterior torques are left–right different, but show the same ratio, with the torque of the knee extensors (more precisely, the torque of the rectus femoris as part of the quadriceps femoris) being predominant. This can lead to an anteversion of the pelvis, which affects both hemi-pelvises equally (
Figure 5b). Shearing forces would not develop in the pubic symphysis. The influence of the relevant muscle groups on the positioning of the pelvis has been analyzed in other studies [
14].
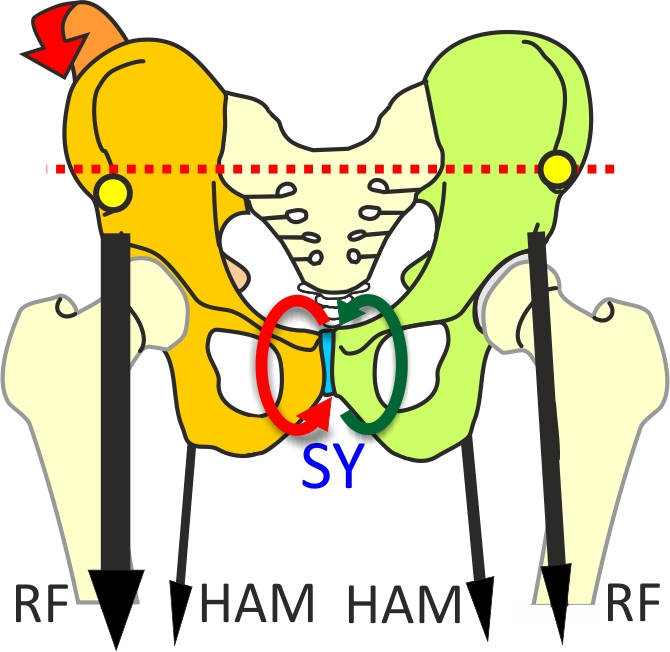
3. The anterior–posterior torque ratios differ. If this is the case, the pelvis tilts forward on the side with the higher quadriceps–hamstrings ratio. The pubic symphysis may experience shearing forces (
Figure 5c).
The crossed torque ratio had the most expressed influence on the pelvic torsion angle. This is interesting because this harmonizes with our model-based assumption, according to which differing agonist/antagonist torque ratios between the left and right side are more decisive for torsion than the absolute values of the agonist–antagonist ratios. Differences in the agonist–antagonist torque ratios would, if they were identical left and right, allow the pelvis to antevert, but they would not necessarily have an effect on the torsion of the hemi-pelvises. The absolute torque of the muscles involved, however, do play a role, as shown by the correlation coefficient of the quadriceps at the side of the anteverted hemi-pelvis (quadriceps torque IPSI Ex,
Table 3). The crossed torque ratio (Equation (3)) seems to have a more expressed influence, though. Nevertheless, our results do not allow a direct derivation of a causal connection. This means that we cannot identify the muscular torque ratios measured as a reason for the three-dimensional torsion of the hemi-pelvises and the increased tenderness to palpation in the pubic symphysis. However, the findings still fit in the pelvis movement model described.
Only a few studies focus on the three-dimensional movement of the hemi-pelvises against each other and the sacrum. Becker et al. describe physiological, rotatory movements of one degree in the pubic symphysis [
28]. Strain caused by standing on one leg results in relative vertical shearing stress and tensile stress on the stabilizing sacroiliac joints, as well as in vertical shearing and pressure strain on the pubic symphysis [
25,
29]. In vivo measurements of healthy test persons with metal wires implanted in the pubic bone ramus (ramus ossis superior pubis) showed translation values of <2 mm and <3° rotation at the pubic symphysis when subjected to various strain-causing maneuvers [
30]. In a radiological study with asymptomatic test persons who were standing alternatingly on the left and right leg, Garras et al. were able to prove that physiological movements up to 5 mm can occur at the pubic symphysis (functional instability) and that higher values are to be interpreted as a sign of "macro" instability [
2]. Macro instabilities do not necessarily cause direct problems. They may, however, represent a significantly increased risk factor for the development of groin pain/injuries. Golden and colleagues define a pelvis as stable if a vertical rotational symphyseal displacement of less than 11 mm occurs [
31]. These data refer to traumatic pelvis injuries only, therefore, they cannot be generalized or even transferred to an athletic population. It is known that routine movements like walking already lead to slight physiologic movements that cause shearing forces in the pubic symphysis during the one-leg stance phase. This may explain why our test persons with higher pelvic torsion exhibited a significantly increased tenderness to palpation of the pubic symphysis. Even if they did not complain of pain in the pubic symphysis during everyday (sports) activities, we assume that strain in the area of the articular capsule caused by shearing forces may be a potential factor that might increase tenderness to palpation and sensitivity. Therefore, it may make sense to keep this in mind as a potential precursor for later pathologies and perform further studies on this topic.
Some studies could show that the muscular balance between quadriceps and hamstrings depends on the type of sports performed. For example, Iga et al. found significant differences in the hamstrings–quadriceps ratio between the dominant and non-dominant leg of adolescent soccer players [
32]. Gür et al. were able to show that these changes are adaptations to soccer-specific requirements [
33]. This torsion of the hemi-pelvises may play an important role as a potentially pathogen mechanism in athletes, especially those with a heavy muscular imbalance between the dominant and non-dominant leg. This information is particularly relevant to our study because most of our participants were indeed soccer players.
Key aspects pertaining to the prevention and rehabilitation of groin/pubic bone problems could be derived if the strength ratios of quadriceps and hamstrings were analyzed and improved, in the case of contralateral imbalances. Iga et al. emphasize that imbalances of the leg muscles might be improved by including resistance exercises in the habitual training routines of youth soccer players [
32]. To date, therapeutic focus has mostly been placed on strengthening adductors and rectus abdominis. In a prospectively randomized study, Holmich et al. were able to show that a group achieved significantly better results through active adductor training than through physical therapy treatment [
34].
The results of our study point to a potential biomechanical-pathogen mechanism that should be taken into account in primary prevention and diagnostics of groin pain.
Limitations
This study analyzed the potential influence factor of only two major muscle groups on the three-dimensional pelvis orientation. Many other muscles and their torque ratios also have an influence on the orientation of the pelvis and that of the hemi-pelvises against each other. This includes mainly the gluteus maximus, the adductor muscles, iliopsoas muscle, and the abdominal and pelvic floor muscles. Our study is thus based only on a simplified model.
In daily athletic routine, not only the absolute isometric strength plays a key role, but also the neuromuscular responsivity of the muscles when accelerating or changing directions, which was not investigated in our study. For example, Cowan et al. found that the feed-forward activation of transversus abdominis during a straight leg raise movement was delayed in patients with persistent groin pain [
35]. Owing to the potential stabilizing role of the transversely oriented abdominal muscles for the anterior pelvic ring, a late reaction of these muscles can have consequences for the stability of the pelvis.
We also need to emphasize that we only examined healthy male test persons. Therefore, the results cannot be applied directly to patients or to female athletes. However, we still need to state that a notable pain on palpation of the pubic symphysis was often observed in asymptomatic test persons.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}