
Considering Material Culture in Assessing Assistive Devices: “Breaking up the Rhythm”


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. The “Getting On” Intervention
3. Taking a Concrete Approach to Project Learning: Material Culture
[Dis]ability Discourses as Material Culture [Objects]
4. The Meaning of Assistive Devices Project
4.1. Data Analysis
4.2. Meaning Assigned to Assistive Devices
4.2.1. Markers of Progress
Over the next couple of days I improved in my walking with this miracle walker. I was permitted to walk without the therapist or the therapy attendant holding on to a gaitbelt placed around my waist. Boy did I ever feel great when that occurred. I felt so free and independent. The fact that I could only walk inside the department, which was pretty small, and that they kept a pretty close eye on me didn't bother me. I WAS WALKING without anyone’s help and that was good enough for me (46-year-old male).
I waited until she went to work and then I would practice. First, I had to use my cane, because as I stepped from stone to stone, I would almost topple over. But I kept at it. It took months before I finally had the confidence to go up the steps to the field. I got my balance back on those stones. I gave the cane away so I couldn’t take a picture of it.
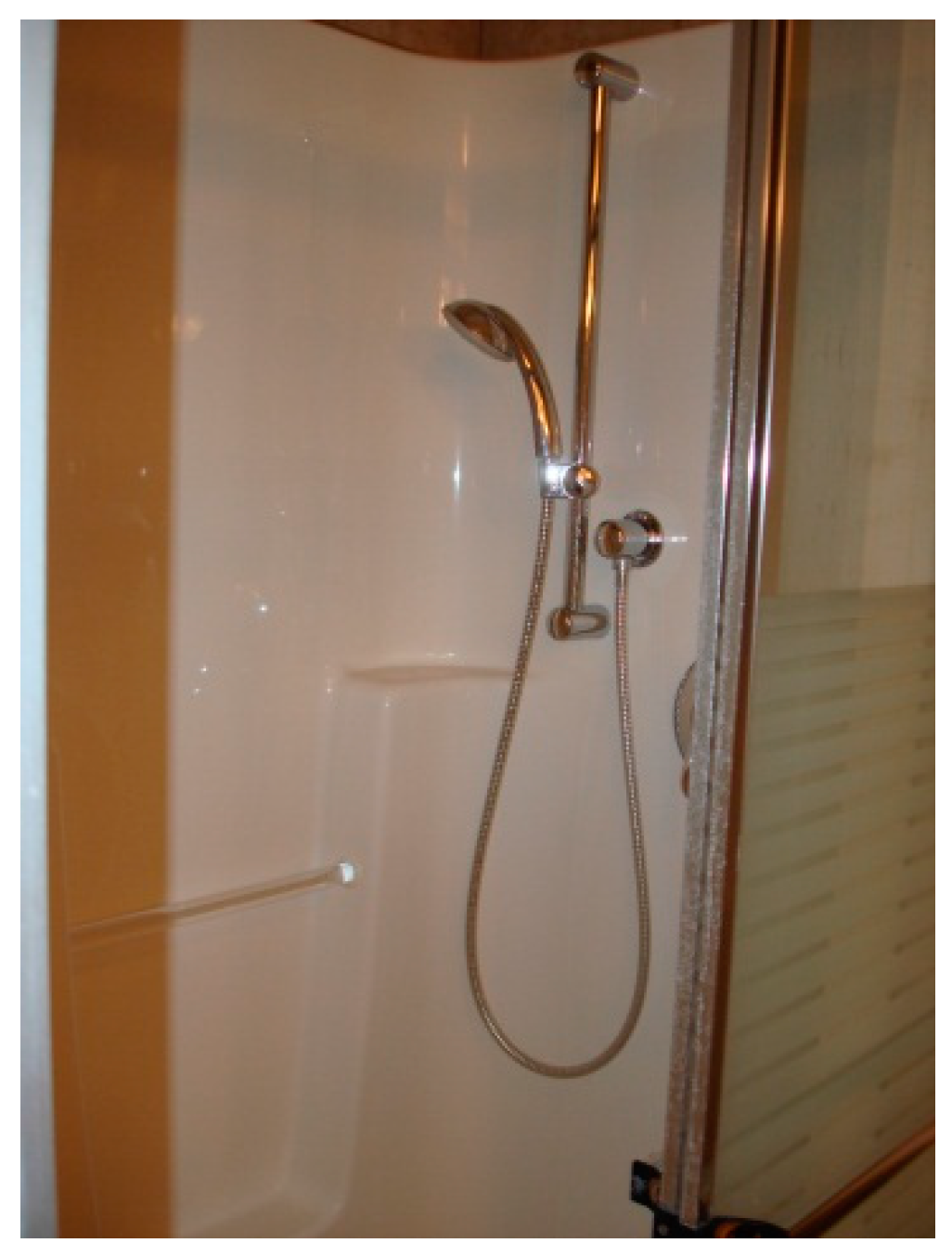
We built a new house with accessible showers and kitchen so I went from needing help with everything to doing most things by myself. I felt like such heavy load on my husband. I am not back at work. We went from two incomes to one, but I do all the cooking and cleaning now. It has taken me a long time to do the things I wanted to do. You will see; I found lots things that work with one hand.
I had nothing. I felt like I couldn’t do anything with one hand. Like how do you peel a potato or cut a tomato? I was looking all over for some stainless steel nails for a cutting board. We couldn’t find any, so the OT gave me a couple so I could start doing some stuff myself. She was awesome. Then I found the ulu knife, so at least I could make a tomato sandwich. Small thing, but life started to become normal with a tomato sandwich.
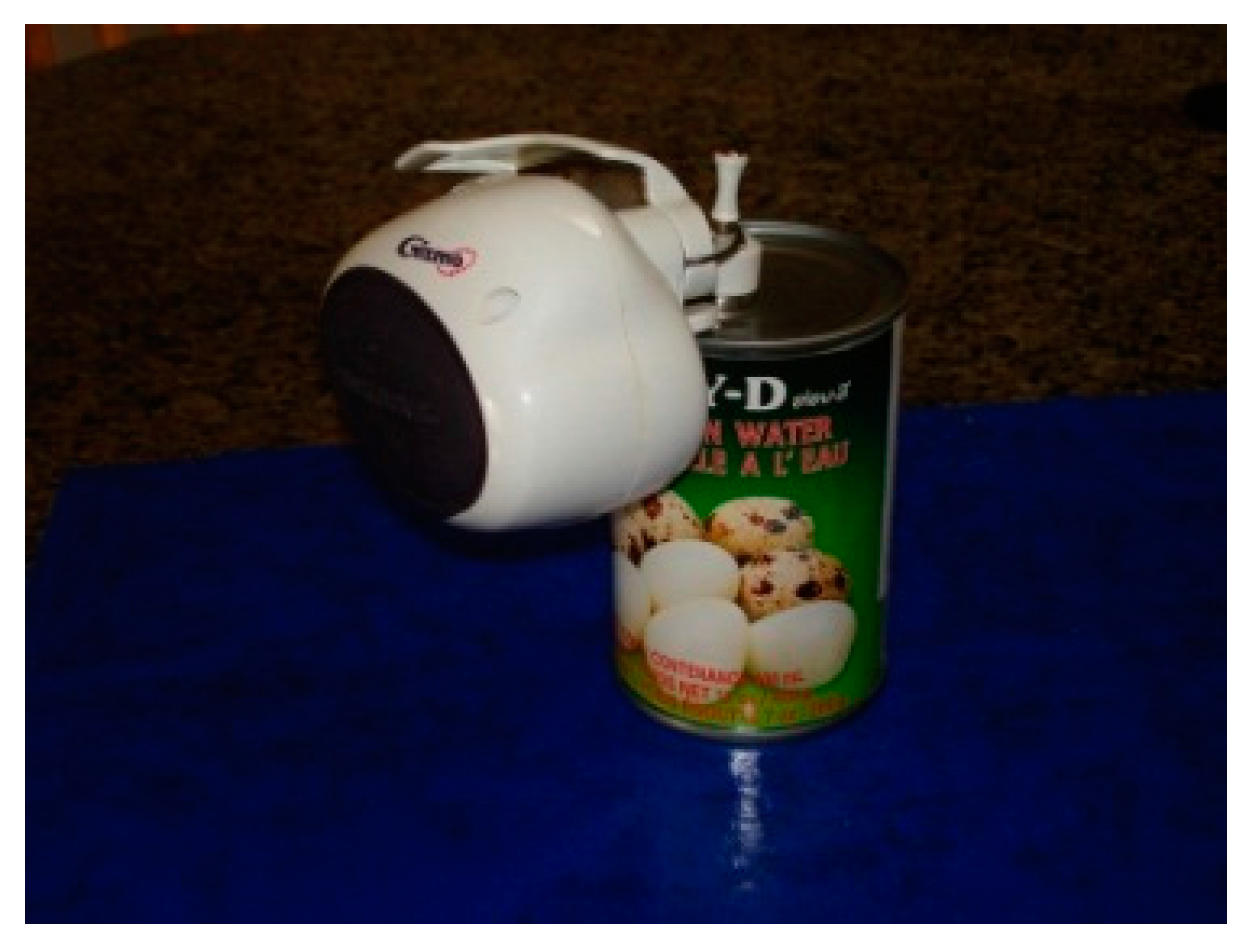
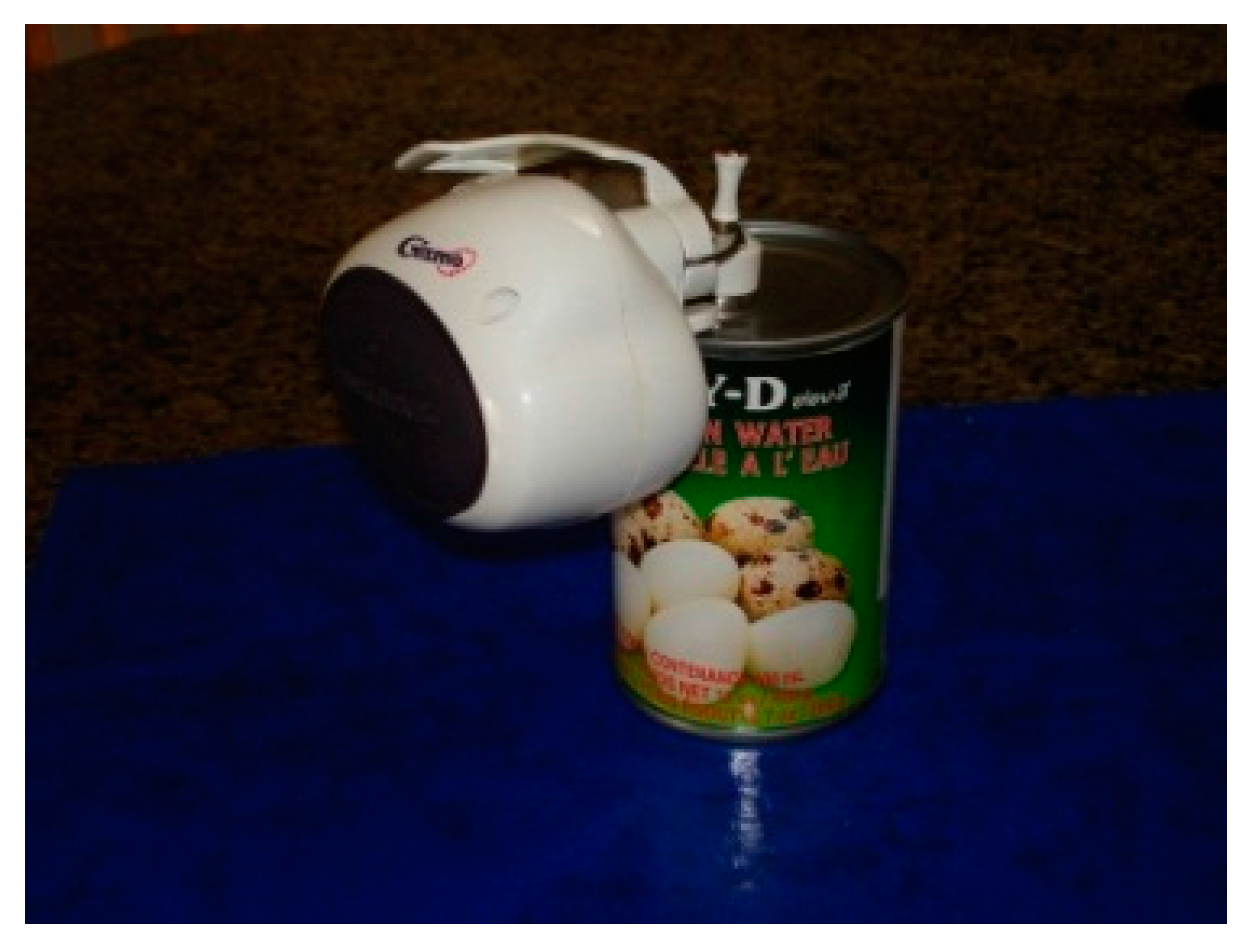
The men in our family always carved the meat at the table. I tried electric knives, but I really couldn’t cut with one hand. My wife had to do it. Then I came on the meat slicer. I just get boneless roasts or turkey and voila! I can cut meat again.
I always worried that I would get lost or I would fall and so did my family. Then I got the cellphone. I started by walking to Safeway to get groceries. It was just a couple of blocks, but I knew I could call if I was in trouble. Now I walk everywhere.
4.2.2. Symbolic Objects of Disability
I need this old black wheelchair whenever I go out, but it screams different. People won’t look at me. I didn’t realize what being in a wheelchair does to your sense of self until I had to use this one.
I have to get shoes one size larger, then this one is too big on my good foot. Sloppy, looks horrible.
When they see me coming in my scooter, they see an old man, and old people are not valuable to them.
Well sure they’re in a hurry to get me seated and get their tip and me out so they can get the next people seated. It’s the rhythm and I am breaking up the rhythm. The manager wants to get as many seatings as possible and if I’m walking slowly it’s ruining their rhythm.
The door wasn’t even accessible at [name of fitness facility]. It was heavy and with my cane, my gym bag, and only this hand, I couldn’t open it. My 80-year-old mother had to come to open it… The door says only young able-bodied people.
A small purchasing error. Must have just slipped my mind that I only had a left hand, [laugh] but at least I could return them. Funny how I didn’t see that from the picture in the catalogue.
4.2.3. Possibility of Independent Participation
I came home and cried. My husband said I just didn’t want to be realistic. It took me a long time to choose this model. Now I use it to go everywhere, the mall, to the gym. I still work at walking at the gym, but when I use my electric wheelchair, I go shopping.
I bought the same type of manual wheelchair as Sarah for the same reason. The OT wanted me to get an electric wheelchair, but come hell or high water I was going to walk everywhere. And then last summer I decided that I wanted to be able to go to [Safeway] to buy groceries. I was using Meals-on-Wheels, but it was expensive and I thought I could cook for myself. So I decided to get a scooter. I would never have been able to walk far enough or fast enough to get around the store. I gave up my dreams of walking like I did before stroke, but I regained my life. I gave up Meals-on-Wheels. I get my own groceries and make my own meals.
4.2.4. Project Evaluation
5. Material Culture as a Framework to Understand the Meaning of [Dis]ability
5.1. Implications
5.2. Strengths and Limitations
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix: Project Evaluation Questions (Completed by Participants)
- Was this project useful to you? (1) Not useful at all; (2) a little useful; (3) useful; (4) quite useful; and (5) very useful.
- Was this project fun? (1) Not fun at all; (2) a little fun; (3) fun; (4) quite a lot of fun; and (5) lots of fun.
- What did you learn from the project?
- How did taking picture and sharing your experiences of “things that helped” help you?
- What do you suggest we could do to make this project better for other stroke survivors?
References
- Miodownik, M. Stuff Matters: Exploring the Marvelousmaterials that Shape our Man-Made World; Houghton Mifflin Harcourt: New York, NY, USA, 2014. [Google Scholar]
- Dant, T. The “pragmatics“ of material interaction. J. Consum. Cult. 2008, 8, 11–33. [Google Scholar] [CrossRef]
- Bourdieu, P. Distinction: A Social Critique of the Judgment of Taste; Routledge: London, UK, 1984. [Google Scholar]
- Csikszentmihalyi, M.; Rochbert-Halton, E. The Meaning of Things: Domestic Symbols and the Self; Cambridge University Press: New York, NY, USA, 1981. [Google Scholar]
- Burkette, A. Language and Material Culture; John Benjamins Publishing Company: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Harrison, T.C.; Kahn, D.L. Disability rites: The cultural shift following impairment. Fam. Community Health 2004, 27, 86–93. [Google Scholar] [CrossRef] [PubMed]
- McDermott, R.; Varenne, H.V. Culture as disability. Anthropol. Educ. Q. 1995, 26, 324–345. [Google Scholar] [CrossRef]
- Pullin, G. Design Meets Disability; The MIT Press: Cambridge, MA, USA, 2011. [Google Scholar]
- Hurst, A.; Tobias, J. Empowering Individuals with Do-it-Yourself Assistive Technology; ACM: New York, NY, USA, 2011; pp. 11–18. [Google Scholar]
- De Couvreur, L.; Goossens, R. Design for (every)one: Co-creation as a bridge between universal design and rehabilitation engineering. CoDesign 2011, 7, 107–121. [Google Scholar] [CrossRef]
- Goljar, N.; Burger, H.; Vidmar, G.; Marincek, C.; Krizaj, J.; Chatterji, S.; Raggi, A.; Leonardi, M.; Bickenbach, J.E. Functioning and disability in stroke. Disabil. Rehabil. 2010, 32, S50–S58. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, L.N.; Luborsky, M.R.; Schemm, R.L. Emerging concerns of older stroke patients about assistive device use. Gerontologist 1998, 38, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Rodeschini, G. Gerotechnology: A new kind of care for aging? An analysis of the relationship between older people and technology. Nurs. Health Sci. 2011, 13, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.J. Braces, wheelchairs, and iron lungs: The paralyzed body and the machinery of rehabilitation in the polio epidemics. J. Med. Hum. 2005, 26, 173–190. [Google Scholar] [CrossRef] [PubMed]
- Shakespeare, T. Disability: Suffering, Social Oppression, or Complex Predicament? In The Contingent Nature of Life; Springer: Berlin/Heidelberg, Germany, 2008; Volume 39, pp. 235–246. [Google Scholar]
- Jacobson, S. Overcoming the Stigma Associated with Assistive Devices. In Proceedings of the 7th International Conference on Design and Emotion, Chicago, IL, USA, 4–7 October 2010.
- Parette, P.; Scherer, M. Assistive technology use and stigma. Educ. Train. Deve. Disabil. 2004, 39, 217–226. [Google Scholar]
- Hammel, J.; Magasi, S.; Heinemann, A.; Gray, D.B.; Stark, S.; Kisala, P.; Carlozzi, N.E.; Tulsky, D.; Garcia, S.F.; Hahn, E.A. Environmental barriers and supports to everyday participation: A qualitative insider perspective from people with disabilities. Arch. Phys. Med. Rehabil. 2015, 96, 578–588. [Google Scholar] [CrossRef] [PubMed]
- Phillips, B.; Zhao, H. Predictors of assistive technology abandonment. Assist. Technol. 1993, 5, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Demers, L.; Fuhrer, M.J.; Jutai, J.W.; Scherer, M.J.; Pervieux, I.; DeRuyter, F. Tracking mobility-related assistive technology in an outcomes study. Assist. Technol. 2008, 20, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Gelderblom, G.J.; Wessels, R.; Dijcks, A.; Soede, T. Assistive Technology Abandonment and Its Determinants. In Assistive Technology—Added Value to the Quality of Life; Marincek, C., Buhler, C., Knops, H., Andrich, R., Eds.; IOS Press: Amsterdam, The Netherland, 2001; pp. 454–459. [Google Scholar]
- Pettersson, I.; Berndtsson, I.; Appelros, P.; Ahlstrom, G. Lifeworld perspectives on assistive devices: Lived experiences of spouses of persons with stroke. Scand. J. Occup. Ther. 2005, 12, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Scherer, M.J.; Craddock, G.; Mackeogh, T. The relationship of personal factors and subjective well-being to the use of assistive technology devices. Disabil. Rehabil. 2011, 33, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Johnston, P.; Currie, L.M.; Drynan, D.; Stainton, T.; Jongbloed, L. Getting it “right“: How collaborative relationships between people with disabilities and professionals can lead to the acquisition of needed assistive technology. Disabil. Rehabil. Assist. Technol. 2014, 9, 421–431. [Google Scholar] [CrossRef] [PubMed]
- Gruman, J.; Rovner, M.H.; French, M.E.; Jeffress, D.; Sofaer, S.; Shaller, D.; Prager, D.J. From patient education to patient engagement: Implications for the field of patient education. Patient Educ. Couns. 2010, 78, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Domecq, J.P.; Prutsky, G.; Elraiyah, T.; Wang, Z.; Nabhan, M.; Shippee, N.; Brito, J.P.; Boehmer, K.; Hasan, R.; Firwana, B.; et al. Patient engagement in research: A systematic review. BMC Health Serv. Res. 2014. [Google Scholar] [CrossRef] [PubMed]
- Schegloff, E.A. Discourse as an interactional achievement iii: The omnirelevance of action. In The Handbook of Discourse Analysis; John Wiley & Sons: Somerset, NJ, USA, 2008; pp. 229–249. [Google Scholar]
- Mayo, N.E.; Anderson, S.; Barclay, R.; Cameron, J.I.; Desrosiers, J.; Eng, J.J.; Huijbregts, M.; Kagan, A.; Lyons, M.M.; Moriello, C.; et al. Getting on with the rest of your life following stroke: A randomized trial of a complex intervention aimed at enhancing life participation post stroke. Clin. Rehabil. 2015. [Google Scholar] [CrossRef] [PubMed]
- Dant, T. Material civilization: Things and society. Br. J. Sociol. 2006, 57, 289–308. [Google Scholar] [CrossRef] [PubMed]
- Deetz, J. In Small Things Forgotten: An Archeology of Early American Life; Doubleday: New York, NY, USA, 1996. [Google Scholar]
- Krantz, O. Assistive devices utilisation in activities of everyday life—A proposed framework of understanding a user perspective. Disabil. Rehabil. Assist. Technol. 2012, 7, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Higgins, M. Placing photovoice under erasure: A critical and complicit engagement with what it theoretically is (not). Int. J. Qual. Stud. Educ. 2016, 29, 670–685. [Google Scholar] [CrossRef]
- Ozanne, J.L.; Moscato, E.M.; Kunkel, D.R. Transformative photography: Evaluation and best practices for eliciting social and policy changes. J. Public Policy Mark. 2013, 32, 45–60. [Google Scholar] [CrossRef]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Harre, R. Material objects in social worlds. Theory Cult. Soc. 2002. [Google Scholar] [CrossRef]
- Duxbury, S.; Depaul, V.; Alderson, M.; Moreland, J.; Wilkins, S. Individuals with stroke reporting unmet need for occupational therapy following discharge from hospital. Occup. Ther. Health Care 2011, 26, 16–32. [Google Scholar] [CrossRef] [PubMed]
- Boissy, P.; Hester, T.; Sherrill, D.; Corriveau, H.; Bonato, P. Monitoring Mobility Assistive Device Use in Post-Stroke Patients. In Proceedings of the 29th Annual International Conference of the IEEE Engineering in Medicine and Biology, Lyon, France, 22–26 August 2007; pp. 4372–4375.
- McCain, K.J.; Smith, P.S.; Querry, R. Ankle-foot orthosis selection to facilitate gait recovery in adults after stroke: A case series. J. Prosthet. Orthot. 2012, 24, 111–121. [Google Scholar] [CrossRef]
- Skolarus, L.E.; Burke, J.F.; Freedman, V.A. The role of accommodations in poststroke disability management. J. Gerontol. B Psychol. Sci. Soc. Sci. 2014, 69, S26–S34. [Google Scholar] [CrossRef] [PubMed]
- Krueger, H.; Koot, J.; Hall, R.E.; O’Callaghan, C.; Bayley, M.; Corbett, D. Prevalence of individuals experiencing the effects of stroke in canada: Trends and projections. Stroke J. Cereb. Circ. 2015, 46, 2226–2231. [Google Scholar] [CrossRef] [PubMed]






© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anderson, S.; Kaiser Gladwin, K.; Mayo, N. Considering Material Culture in Assessing Assistive Devices: “Breaking up the Rhythm”. Societies 2016, 6, 14. https://doi.org/10.3390/soc6020014
Anderson S, Kaiser Gladwin K, Mayo N. Considering Material Culture in Assessing Assistive Devices: “Breaking up the Rhythm”. Societies. 2016; 6(2):14. https://doi.org/10.3390/soc6020014
Chicago/Turabian StyleAnderson, Sharon, Kerri Kaiser Gladwin, and Nancy Mayo. 2016. "Considering Material Culture in Assessing Assistive Devices: “Breaking up the Rhythm”" Societies 6, no. 2: 14. https://doi.org/10.3390/soc6020014
APA StyleAnderson, S., Kaiser Gladwin, K., & Mayo, N. (2016). Considering Material Culture in Assessing Assistive Devices: “Breaking up the Rhythm”. Societies, 6(2), 14. https://doi.org/10.3390/soc6020014