2.1. The Precision Cancer Medicine Knowledgebase and Wiki
We have developed a unique knowledgebase utilizing a novel approach for capturing, storing and sharing knowledge concerned with precision cancer medicine (
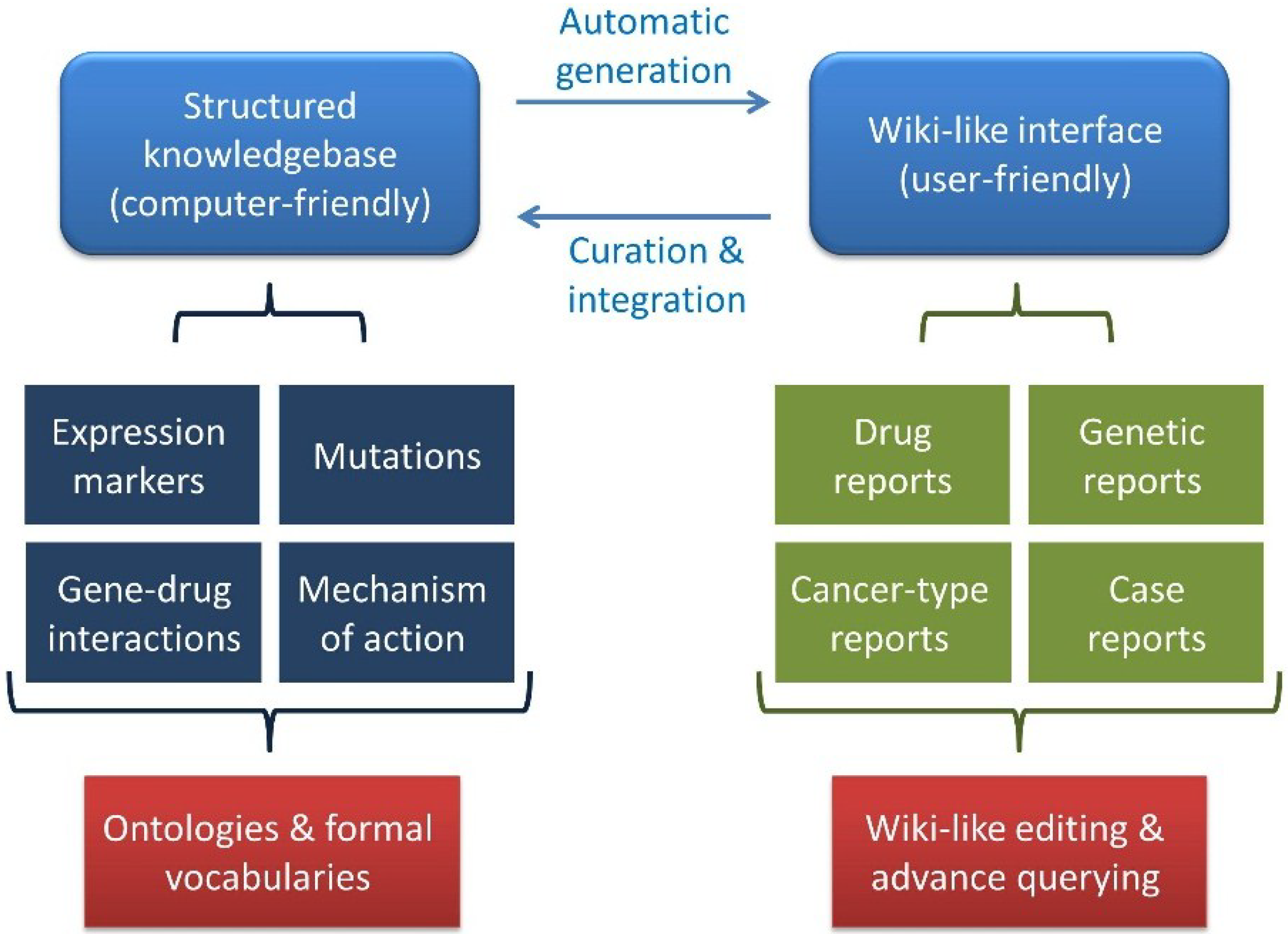
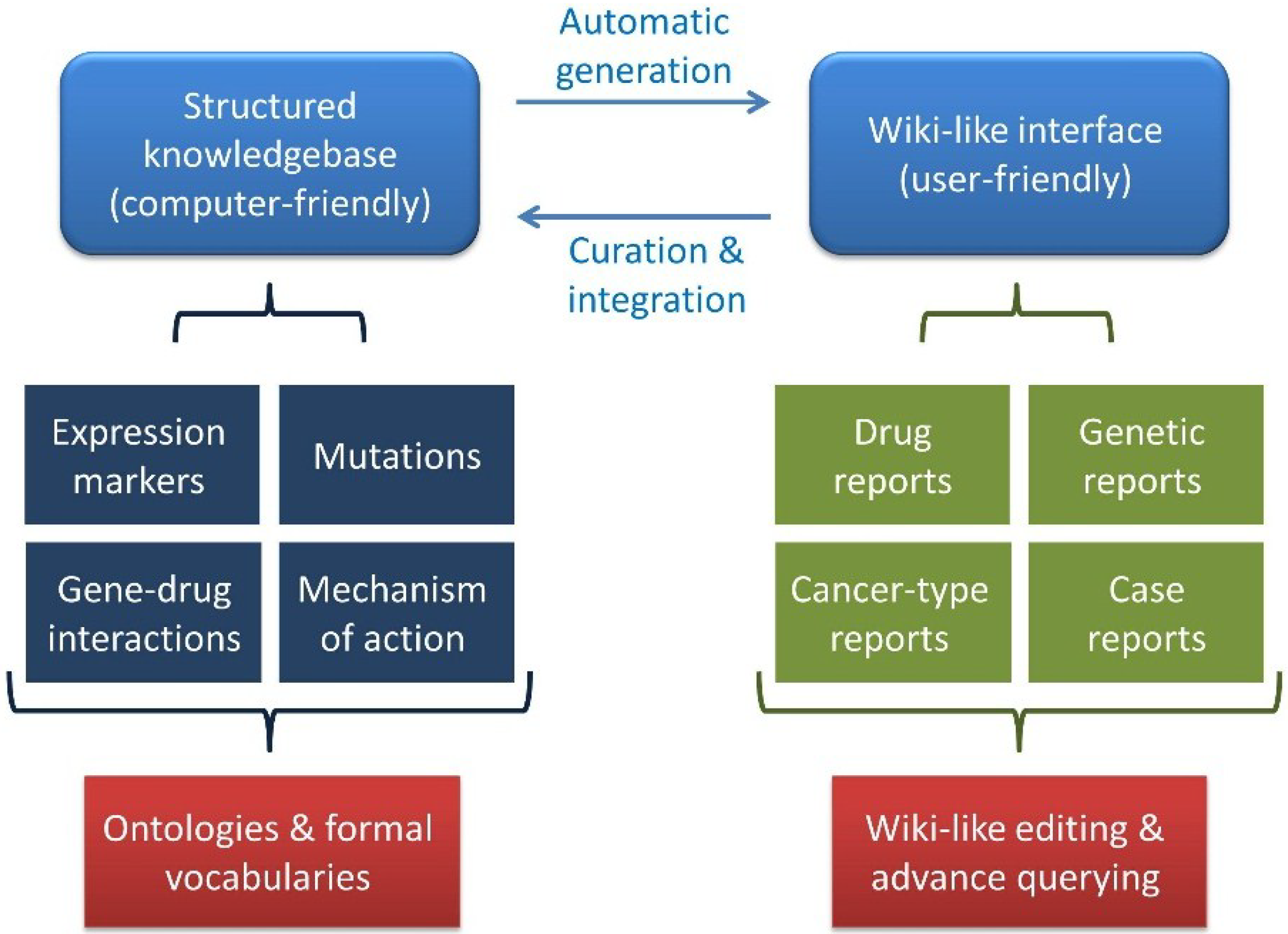
http://pcm-wiki.bgu.ac.il). The knowledgebase is comprised of two arms, a structured knowledgebase on the one hand and a user-friendly Wiki-like interface on the other (
Figure 1). The knowledgebase holds information mined from the literature regarding different types of cancers, drugs, genetic markers and their co-occurrences in publications, as well as case studies introduced through a specialized form. This information is represented, wherever possible, by appropriate ontologies and formal vocabularies that allow a “computer-friendly” representation of the data. To render these data accessible to humans, the knowledge was transformed to the PCM Wiki interface, where the information stored in the knowledgebase is presented on two types of pages, namely information reports summarizing literature-mined information regarding cancer types, drugs and genetic markers and case reports describing actual precision cancer patient reports submitted by the community. The use of the Wiki platform allows users to suggest corrections, offer additions or point to errors in the knowledgebase. Any such suggestions become immediately visible to other users for further revision or rejection. The result is a community-driven knowledgebase holding integrated and consolidated knowledge of markers and indications for personalized cancer medicine.
Figure 1.
The Precision Cancer Medicine Wiki and Knowledgebase model. The precision cancer medicine (PCM) Wiki and Knowledgebase (KB) model comprises a structured knowledgebase together with a user-friendly Wiki-like interface.
Figure 1.
The Precision Cancer Medicine Wiki and Knowledgebase model. The precision cancer medicine (PCM) Wiki and Knowledgebase (KB) model comprises a structured knowledgebase together with a user-friendly Wiki-like interface.
In addition to the Wiki, users can query the knowledgebase through a query engine designed for the search of specific information or case reports (
http://pcm-crs.med.ad.bgu.ac.il/Query/). This query engine is designed to allow physicians to find “patients like mine”. Using such a query engine allows the clinician to search for evidence that a particular treatment would benefit a patient by searching for patients who shared similar characteristics as the patient at hand in situations were no clear guidelines are available. A case report of a patient with good outcome could help prioritize possible treatments. Indeed, a similar approach is already in use in a web tool called “Patients like me” that allows users to find and compare their disease history and treatment course to other patients sharing similar conditions or symptoms [
16]. The tool we propose here, however, is specific for cancer precision medicine and is aimed for use by physicians rather than patients.
To simplify the contribution of case reports from our community of users, we have developed a simple user-friendly case report submission form (
http://pcm-crs.med.ad.bgu.ac.il/form.html). Users provide all of the information pertaining to a case (such as diagnosis, molecular aberration, personalized treatment, treatment outcomes,
etc.). This data is subsequently used to automatically generate a case report page on the PCM Wiki.
The submission mechanism sets a uniform structure for the initial submission, thus keeping case report Wiki pages consistent. In addition, the use of a standard web form means that users do not have to familiarize themselves with Wiki page editing. On the other hand, given that a standard form may not be suitable for all possible cases, the use of a Wiki allows for the necessary flexibility in capturing knowledge. Since variability in precision cancer medicine cases is high, it may be the case that the form does not contain all of the fields needed to properly capture a given patient report. In such cases, the user can add any additional fields or patient data through editing of the Wiki page generated by the standard form. Indeed, in one of the first case reports that we attempted to contribute through the form (provided by Prof. Shmuel Ariad, Soroka University Medical Center, Beersheva, Israel), the information could not be completely captured by the form alone as it involved reversals of diagnosis (from BRCA1 negative to positive), a possibility we did not consider likely when designing the form. In this case, the ability to edit the submitted report was essential for our ability to faithfully present the case.
Another advantage of the use of the patient case submission form is that it allows for formal knowledge representation. With this form, users can choose a diagnosis from a provided list of International Classification of Diseases for Oncology (ICD-O) cancer names or from a list of cancer types compiled from the Disease Ontology. By allowing users to select diagnoses from lists of formal terms taken from medical vocabularies and ontologies (
i.e., the Disease Ontology and ICD-O), case report data collected by the submission form can be easily formalized, thus making it amendable to complex computational analyses. This formalization of the data stored in the PCM knowledgebase can be easily extended by incorporating appropriate formal terminologies to describe other fields of the form (such as using RxNorm [
17] to represent drugs and treatments). Capturing subsequent edits introduced through the Wiki interface is also relatively straightforward. The Wiki stores, all changes introduced to any page by default. Upon mining these page edits, it is possible to correct the information stored in the structured knowledgebase. Although this step is currently conducted manually, it can be automated (at least in part) in the future by using text mining technologies [
18,
19].
A possible concern with direct contribution of patient information is the potential for compromising patient privacy. In this context, it may be worthwhile to consider the PCM Wiki as a rapid publication journal in that it only includes information that is also included in journal case reports. Contributors merely need to adhere to the ethical guidelines of journal case reporting to ensure that patient privacy will not be compromised. As with any other use of patient information, it is the contributor’s responsibility to adhere to HIPAA or equivalent privacy regulations. Nevertheless, to ensure that private patient information is not introduced accidently or deliberately, cases are manually reviewed periodically. In future, when the number of cases reported becomes too large for manual review, an automatic review mechanism (for example using simple text mining to detect mentions of names, addresses, etc.) will be needed.
2.2. Mining Drug, Gene and Disease Associations from the Literature
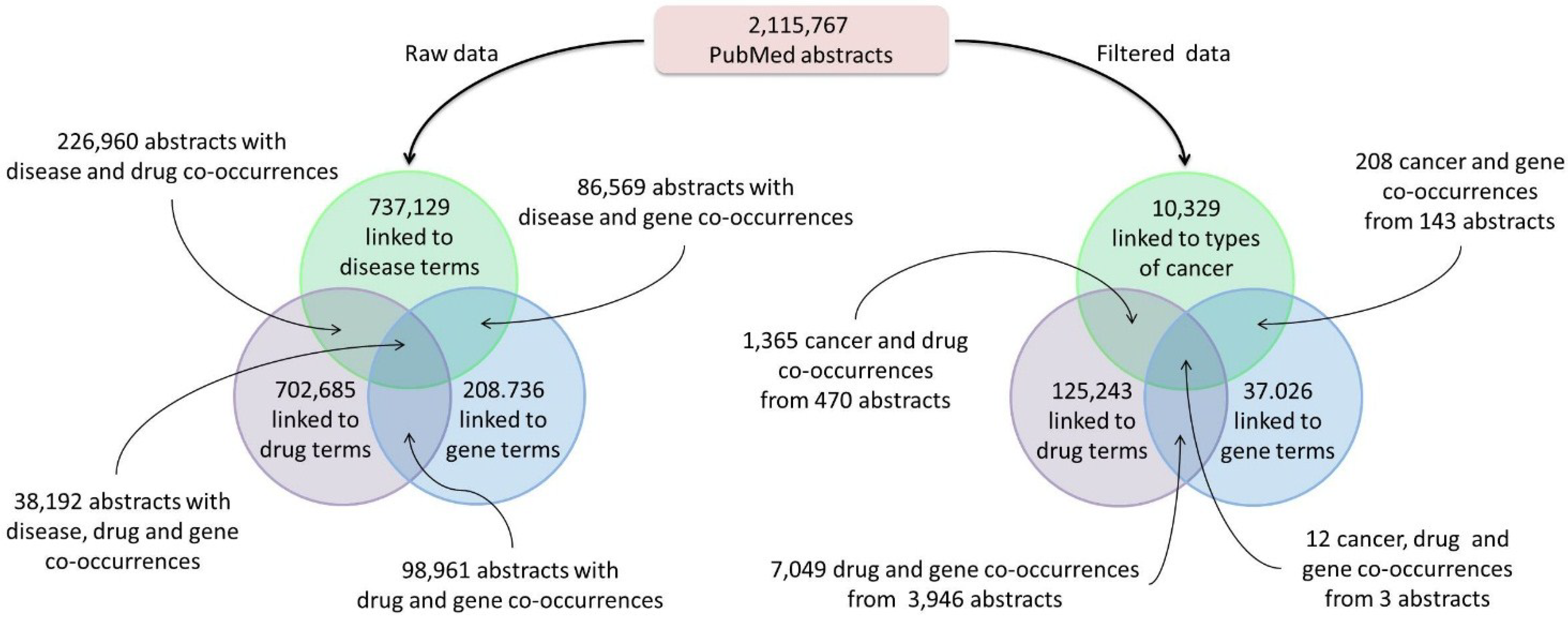
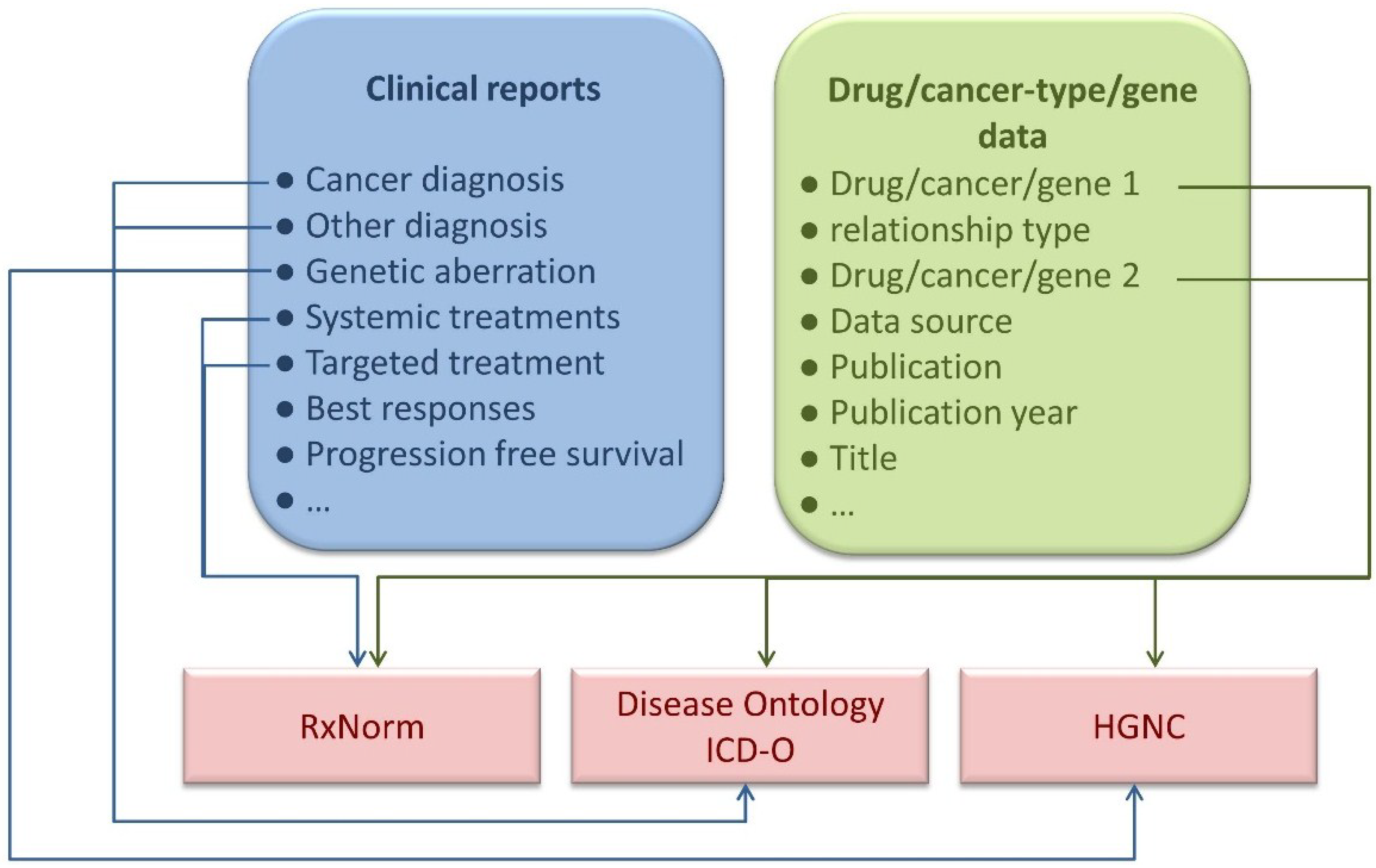
In addition to precision cancer medicine patient case reports, the PCM Wiki and Knowledgebase was seeded with information about associations between types of cancer, treatments and genes mined from the literature. Using a simple knowledge extraction pipeline, MeSH terms associated with over two million PubMed abstracts were mined for occurrences of drug, disease and gene terms (
Figure 2). From this mining process, we were able to capture the co-occurrence of different diseases, drugs and genes within the biomedical literature. Furthermore, since these associations were mined using terms from formal ontologies and vocabularies, such as the Disease Ontology and RxNorm, advanced representations and mining could be applied to this type information.
Figure 2.
Text mining results. The process of mining Medical Subject Headings (MeSH) terms associated with PubMed abstracts yielded associations with disease, drug and/or gene terms (
left). The resulting data were filtered (
right) by selecting only those abstracts linked to cancer and by selecting only abstracts linked to specific types of MeSH categories (See
Clustering Analysis in the
Experimental Section).
Figure 2.
Text mining results. The process of mining Medical Subject Headings (MeSH) terms associated with PubMed abstracts yielded associations with disease, drug and/or gene terms (
left). The resulting data were filtered (
right) by selecting only those abstracts linked to cancer and by selecting only abstracts linked to specific types of MeSH categories (See
Clustering Analysis in the
Experimental Section).
Once captured, these associations and co-occurrences were used to create the drug, disease and genetics reports that are presented in the PCM Wiki. For each cancer type, drug or gene, a report summarizing the co-occurrences of this entity with the other entity types was created. For example, for the cancer type “Melanoma”, the report summarizes its co-occurrence with different drugs and genes and includes, for each co-occurrence, a link to the PubMed abstract from which the co-occurrence was captured.
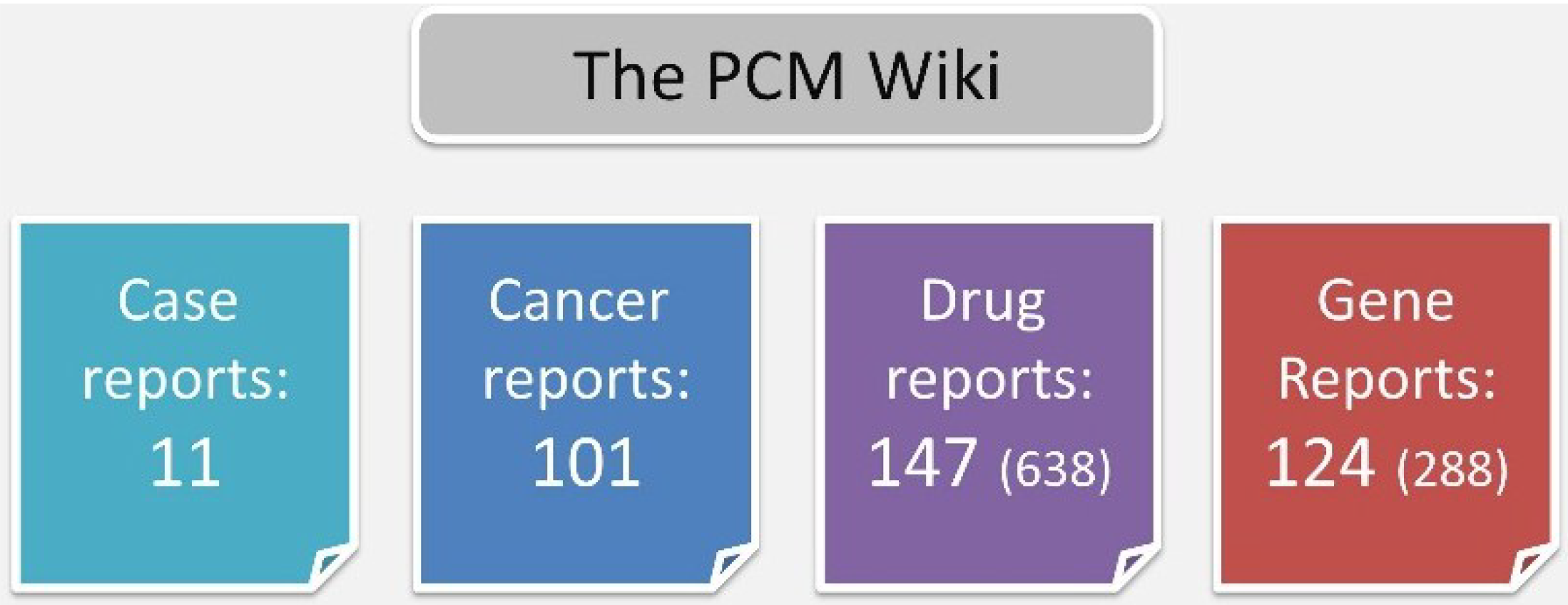
The MeSH-based pipeline yielded 101 cancer type reports, 638 drug reports and 288 gene reports. For the Wiki, we chose to include only drugs or genes with >10 co-occurrences (N = 147 and N = 288 for drugs and genes, respectfully) (
Figure 3).
Figure 3.
Cancer, drug and gene reports. For each entity (cancer type, drug or gene), a report summarizing its co-occurrence in the literature with other entities was generated. For drugs and genes, only reports with >10 co-occurrences were included. The total number of reports prior to this filtration is given in parenthesis.
Figure 3.
Cancer, drug and gene reports. For each entity (cancer type, drug or gene), a report summarizing its co-occurrence in the literature with other entities was generated. For drugs and genes, only reports with >10 co-occurrences were included. The total number of reports prior to this filtration is given in parenthesis.
To explore the usefulness of capturing this type of information, we used these data to cluster cancer types and therapies. Gene-cancer type-drug co-occurrence tables were used to cluster different cancer types based on their co-occurrence with different drugs and therapies (a selected example is presented in
Figure 4) and for clustering different drugs and treatments based on their co-occurrence with different types of cancer (a selected example is presented in
Figure 5).
Figure 4.
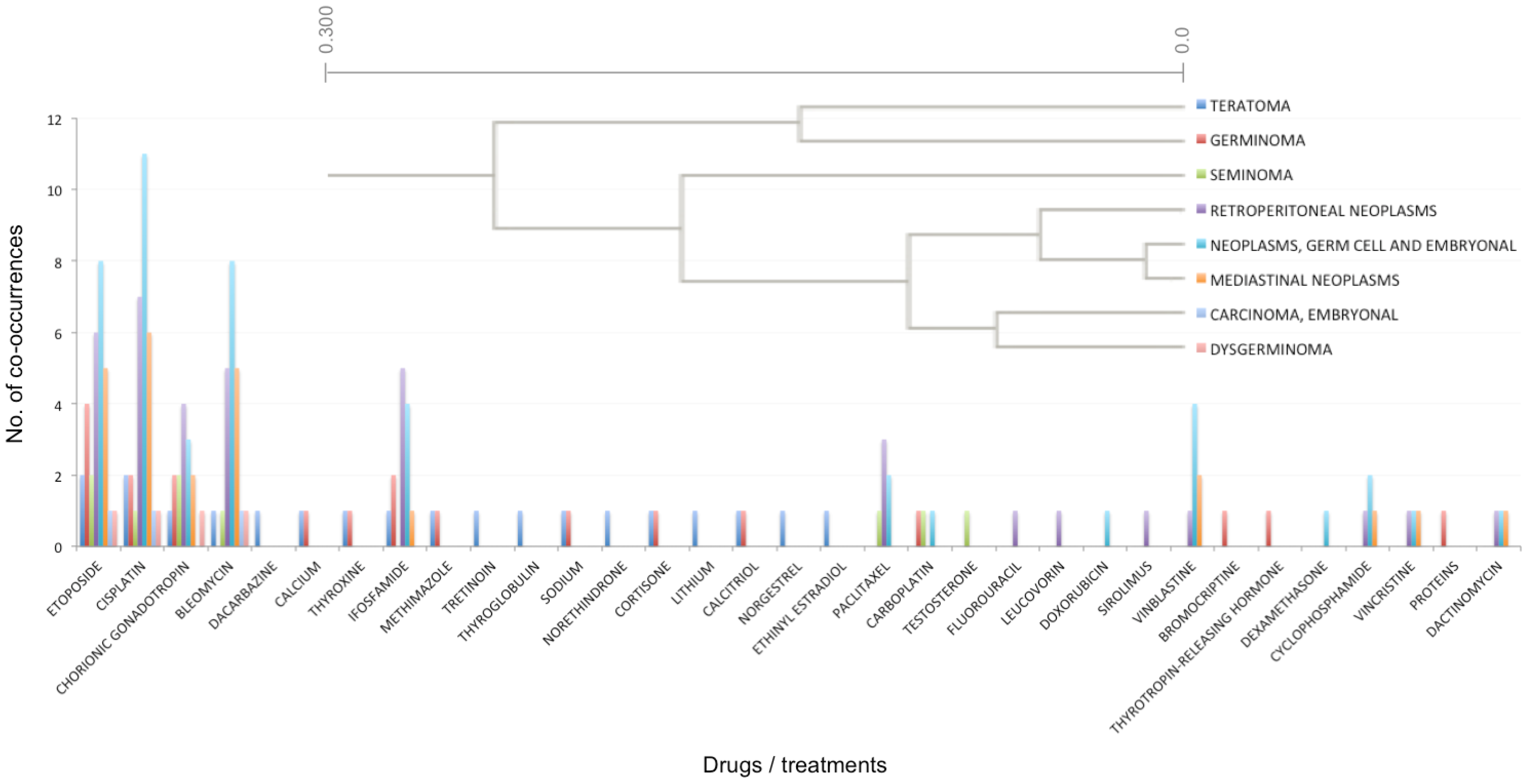
An example cluster generated by hierarchical clustering of cancer types. Cancer types were clustered based on their association (co-occurrence in PubMed abstracts) with different drugs and treatments. The top right corner illustrates the clustering dendrogram, while the plot illustrates the number of co-occurrences for each cancer type and drug/treatment.
Figure 4.
An example cluster generated by hierarchical clustering of cancer types. Cancer types were clustered based on their association (co-occurrence in PubMed abstracts) with different drugs and treatments. The top right corner illustrates the clustering dendrogram, while the plot illustrates the number of co-occurrences for each cancer type and drug/treatment.
Figure 5.
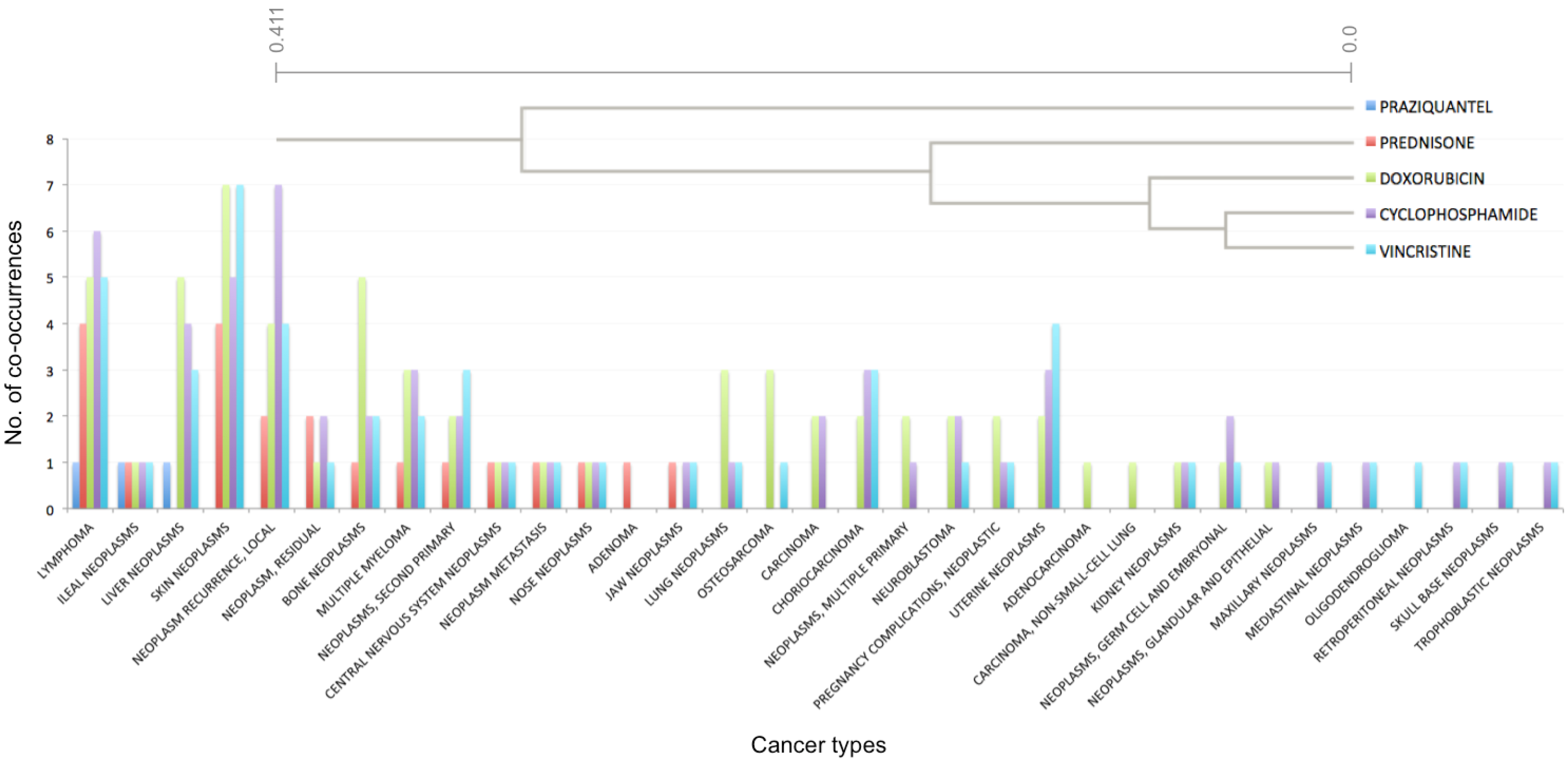
An example cluster generated by hierarchical clustering of drugs and treatments. Various drugs and treatments were clustered based on their association (co-occurrence in PubMed abstracts) with different types of cancer. The top right corner illustrates the clustering dendrogram, while the plot illustrates the number of co-occurrences for each drug/treatment and cancer type.
Figure 5.
An example cluster generated by hierarchical clustering of drugs and treatments. Various drugs and treatments were clustered based on their association (co-occurrence in PubMed abstracts) with different types of cancer. The top right corner illustrates the clustering dendrogram, while the plot illustrates the number of co-occurrences for each drug/treatment and cancer type.
Our results indicate that despite the simple mechanism used for obtaining data, the knowledge we have extracted is sufficient and accurate enough to draw conclusions. In one example (
Figure 4), different types of cancer were clustered based on their associations with various drugs and treatments. This cluster combined many germ cell and embryonic cancers, such as “Germinoma”, “Dysgerminoma”, “Teratoma”, “Seminoma”, “Neoplasms, germ cell and embryonal” and “Carcinoma, embryonal”. These cancer types were clustered based on their high co-occurrence with treatments, such as: “etoposide”, “cisplatin” and “bleomycin”. Each of these drugs has a different mechanism of action. Etoposide is a topoisomerase inhibitor, cisplatin triggers apoptosis by causing crosslinking of DNA, while bleomycin causes DNA breaks. This cluster of cancer types was also generated due to their association with “Chorionic gonadotropin”, known to be produced by some cancer types [
20]. Indeed, in our data, “Chorionic gonadotropin” was associated with “choriocarcinomas” and “trophoblastic neoplasms” for which human chorionic gonadotropin is a marker.
In a second example (
Figure 5), different types of drugs/treatments were clustered together based on their associations with various cancer types. Specifically, vincristine clustered with cyclophosphamide, doxorubicin, prednisone and praziquantel (in increasing order of distance). Vincristine is used for treatment of several cancers, including lymphomas, acute lymphoblastic leukemia (ALL), and nephroblastoma. Our pipeline identified abstracts associating vincristine with lymphomas, as well as skin neoplasms, local recurrent neoplasms and uterine cancer. In our knowledgebase, cyclophosphamide was mostly associated with local recurrent neoplasms, lymphomas, skin neoplasms and liver neoplasms. A more complete literature search revealed that cyclophosphamide is most often used for the treatment of lymphomas, some forms of brain cancers, leukemia [
21] and some solid tumors [
22], in combination with other chemotherapy agents. Doxorubicin is used to treat a wide range of cancers, including hematological malignancies. Prednisone, a synthetic corticosteroid, is used to help treat some leukemias, lymphomas, and other types of cancer (usually along with chemotherapy). These treatments were grouped together due to their high association with several cancer types, including “lymphoma”, “multiple myeloma”, “skin neoplasms” and “neuroblastoma”. In addition to the drugs/treatments mentioned above, the cluster also included praziquantel, a trematodicide used for the treatment of schistosome infections and infections due to liver fluke. In the PCM knowledgebase, praziquantel was linked to cancer through several PubMed abstracts. In one of these, praziquantel was described as successful in treatment of a pseudo-tumor form of hepatic distomatosis [
23]. In a second instance, a case of ileocolonic schistosomiasis presenting as lymphoma was described [
24].
These two examples illustrate that the cancer type-treatment associations data are concordant with current medical knowledge, as reflected in the grouping of different germ cell tumors based on their associations with different treatments. On the other hand, the approach of using text mining to capture precision medicine cancer-related associations has its limitations. The most prominent is that associations are captured without any context, based solely on simple co-occurrence of terms of interest. This means that the type of association between cancer types, drugs or genes is not captured. Furthermore, the context of the association (e.g., different patient parameters, such as age, gender, ethnicity
etc.) is ignored. The two examples given above also illustrate that there is some degree of noise in the data, such as in the association of chorionic gonadotropin to cancers that secrete this compound, rather than association to cancer types treated by chorionic gonadotropin. Nevertheless, we have demonstrated that even in its current simplistic form, the collection of information addressing therapy/gene/cancer type co-occurrences that we have assembled can be of use. Future improvement of this resource, through human editing and/or better text mining (see
Section 2.3 Future Directions) can mold it into an even more valuable resource for cancer research.
2.3. Future Directions
As mentioned above, the PCM Wiki and Knowledgebase employs a straightforward approach to capturing patient case reports in precision cancer medicine. While the use of a Wiki does help overcome limitations of the case report submission form, the model of the form could be expanded to allow for capturing more complex cases (e.g., where more than one line of targeted treatment was used). Furthermore, by capturing the manner in which precision cancer cases are reported by Wiki users, standards of reporting can be assessed. Since such standards would be derived from user contributions, they are likely not only to be best suited for capturing precision cancer medicine-related knowledge but also to appeal to the community that would eventually be using such information.
In addition to improving the manner in which case reports are captured in the knowledgebase, more complex associations between cancer types, drugs and genes could be captured from the literature. In their current form, the Wiki information cards capture information about cancer/drug/gene co-occurrences from publications. Using more advanced text mining techniques, the type of relationships and their context could also be captured and represented for users of the Wiki, for example through the use of interactive networks.
We strongly believe that the interfaces included as part of the knowledgebase (such as the Wiki, the case submission form and the query engine) are user-friendly, straightforward and will appeal to a wide range of users. However, a structured assessment of the interfaces provided by the knowledgebase (for example, using a focus group that would “play around” with the interfaces and point out any issues) would be of great benefit for the further development and improvement of the knowledgebase.
Contributions of PCM Wiki and Knowledgebase information is on a voluntary basis, meaning that physicians add cases as they see fit rather than including all possible cases found in hospital records. Our choice to base the PCM Wiki and Knowledgebase on physician-contributed cases means that only interesting precision cancer medicine cases are captured at the cost of partial and biased coverage of the case spectrum. One possible future direction for the knowledgebase would thus be to allow patients to add their own cases. This would, however, require the development of a submission mechanism that is oriented at non-medically-educated users, and would have to include careful safeguards and filters to prevent mistaken or fraudulent entries from degrading the value of the knowledgebase. Furthermore, a mechanism to flag contributors differently will also be needed so to allow filtering of cases based on whether they were contributed by physicians or patients.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}