An Altered Treatment Plan Based on Direct to Consumer (DTC) Genetic Testing: Personalized Medicine from the Patient/Pin-cushion Perspective

{kind=link}
Abstract
:1. Introduction
2. P4 Medicine: A Real World Example
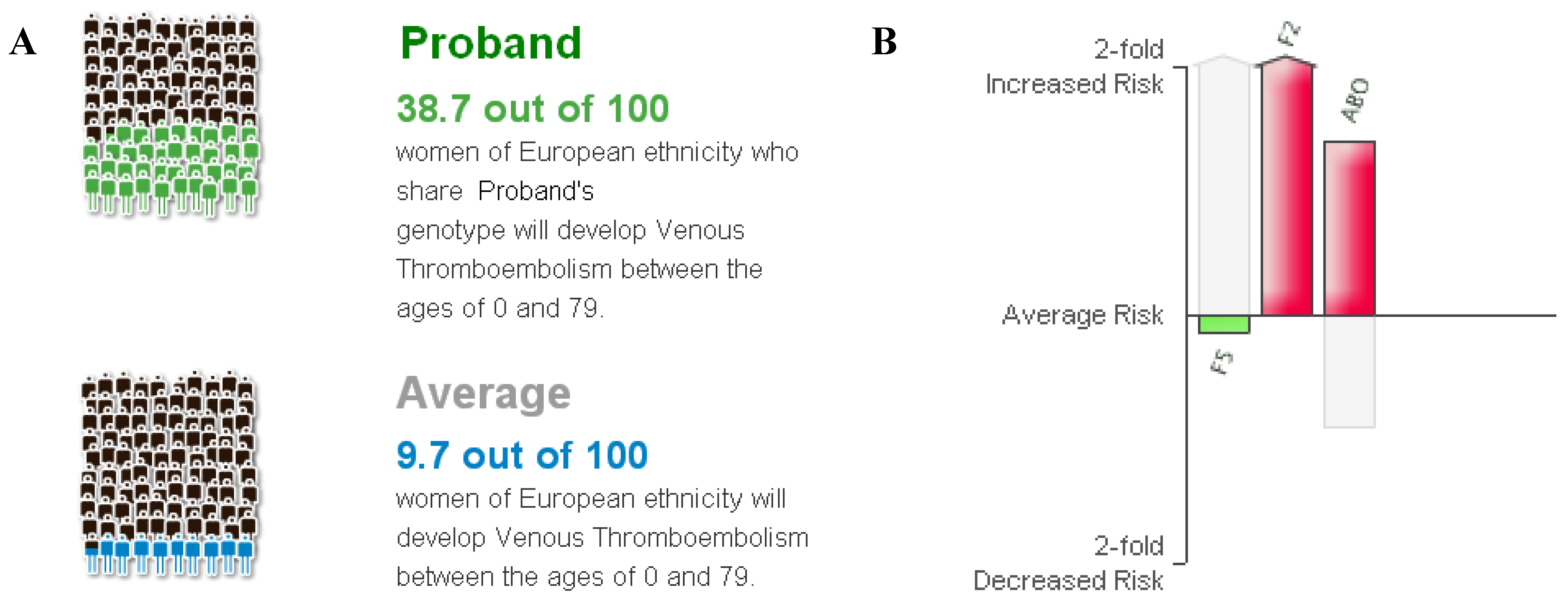
2.1. Case Presentation
2.2. Relative Risk Calculation

2.3. Clinical Perspective
2.4. Patient Perspective
2.5. Prediction, Prevention, and Probability
3. Discussion
Future Steps Needed
4. Conclusions
Acknowledgments
Conflict of Interest
References and Notes
- Hood, L.; Friend, S.H. Predictive, personalized, preventive, participatory (P4) cancer medicine. Nat. Rev. Clin. Oncol. 2011, 8, 184–187. [Google Scholar] [CrossRef]
- Hood, L.; Flores, M. A personal view on systems medicine and the emergence of proactive P4 medicine: Predictive, preventive, personalized and participatory. New Biotechnol. 2012, 29, 613–624. [Google Scholar]
- Tian, Q.; Price, N.D.; Hood, L. Systems cancer medicine: Towards realization of predictive, preventive, personalized and participatory (P4) medicine. J. Intern. Med. 2012, 271, 111–121. [Google Scholar] [CrossRef]
- Auffray, C.; Charron, D.; Hood, L. Predictive, preventive, personalized and participatory medicine: Back to the future. Genome Med. 2010, 2. [Google Scholar] [CrossRef]
- Harmon, K. Genome Sequencing for the Rest of Us. Scientific American. 2010. Available online: http://www.scientificamerican.com/article.cfm?id=personal-genome-sequencing (accessed on 24 August 2012).
- Guttmacher, A.E.; Collins, F.S. Genomic medicine-A primer. N. Engl. J. Med. 2002, 347, 1512–1520. [Google Scholar] [CrossRef]
- Trusheim, M.R.; Berndt, E.R.; Douglas, F.L. Stratified medicine: strategic and economic implications of combining drugs and clinical biomarkers. Nat. Rev. Drug Discov. 2007, 6, 287–293. [Google Scholar]
- National Research Council. Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease. Available online: http://www.ucsf.edu/sites/default/files/documents/new-taxonomy.pdf (accessed on 24 August 2012).
- Evans, W.E.; Relling, M.V. Moving towards individualized medicine with pharmacogenomics. Nature 2004, 429, 464–468. [Google Scholar]
- Manolio, T.A.; Collins, F.S.; Cox, N.J.; Goldstein, D.B.; Hindorff, L.A.; Hunter, D.J.; McCarthy, M.I.; Ramos, E.M.; Cardon, L.R.; Chakravarti, A.; et al. Finding the missing heritability of complex diseases. Nature 2009, 461, 747–753. [Google Scholar]
- Burke, W.; Psaty, B.M. Personalized medicine in the era of genomics. JAMA 2007, 298, 1682–1684. [Google Scholar] [CrossRef]
- Wu, S. Personal Communication, 23andMe Inc.: Mountain View, CA, USA, 25 June 2012.
- Franco, R.F.; Santos, S.E.; Elion, J.; Tavella, M.H.; Zago, M.A. Prevalence of the G20210A polymorphism in the 3'-untranslated region of the prothrombin gene in different human populations. Acta Haematol. 1998, 100, 9–12. [Google Scholar] [CrossRef]
- Pihusch, R.; Buchholz, T.; Lohse, P.; Rubsamen, H.; Rogenhofer, N.; Hasbargen, U.; Hiller, E.; Thaler, C.J. Thrombophilic gene mutations and recurrent spontaneous abortion: Prothrombin mutation increases the risk in the first trimester. Am. J. Reprod. Immunol. 2001, 46, 124–131. [Google Scholar]
- Alfirevic, Z.; Roberts, D.; Martlew, V. How strong is the association between maternal thrombophilia and adverse pregnancy outcome? A systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2002, 101, 6–14. [Google Scholar] [CrossRef]
- Wu, O.; Robertson, L.; Twaddle, S.; Lowe, G.D.; Clark, P.; Greaves, M.; Walker, I.D.; Langhorne, P.; Brenkel, I.; Regan, L.; et al. Screening for thrombophilia in high-risk situations: Systematic review and cost-effectiveness analysis. The Thrombosis: Risk and Economic Assessment of Thrombophilia Screening (TREATS) study. Health Technol. Assess. 2006, 10, 1–110. [Google Scholar]
- Silver, R.M.; Zhao, Y.; Spong, C.Y.; Sibai, B.; Wendel, G., Jr.; Wenstrom, K.; Samuels, P.; Caritis, S.N.; Sorokin, Y.; Miodovnik, M.; et al. Prothrombin gene G20210A mutation and obstetric complications. Obstet. Gynecol. 2010, 115, 14–20. [Google Scholar] [CrossRef]
- Jacobsen, A.F.; Dahm, A.; Bergrem, A.; Jacobsen, E.M.; Sandset, P.M. Risk of venous thrombosis in pregnancy among carriers of the factor V Leiden and the prothrombin gene G20210A polymorphisms. J. Thromb Haemost. 2010, 8, 2443–2449. [Google Scholar] [CrossRef]
- Peters, E.; Hibbard, J.; Slovic, P.; Dieckmann, N. Numeracy skill and the communication, comprehension, and use of risk-benefit information. Health Aff. (Millwood) 2007, 26, 741–748. [Google Scholar]
- James, A.H.; Jamison, M.G.; Brancazio, L.R.; Myers, E.R. Venous thromboembolism during pregnancy and the postpartum period: Incidence, risk factors, and mortality. Am. J. Obstet. Gynecol. 2006, 194, 1311–1315. [Google Scholar] [CrossRef]
- EGAPP Working Group. Recommendations from the EGAPP Working Group: Routine testing for Factor V Leiden (R506Q) and prothrombin (20210G>A) mutations in adults with a history of idiopathic venous thromboembolism and their adult family members. Genet. Med. 2011, 13, 67–76. [Google Scholar]
- Spector, E.B.; Grody, W.W.; Matteson, C.J.; Palomaki, G.E.; Bellissimo, D.B.; Wolff, D.J.; Bradley, L.A.; Prior, T.W.; Feldman, G.; Popovich, B.W.; et al. Technical standards and guidelines: venous thromboembolism (Factor V Leiden and prothrombin 20210G>A testing): A disease-specific supplement to the standards and guidelines for clinical genetics laboratories. Genet. Med. 2005, 7, 444–453. [Google Scholar] [CrossRef]
- Lockwood, C.; Wendel, G. Practice bulletin No. 124: Inherited thrombophilias in pregnancy. Obstet. Gynecol. 2011, 118, 730–770. [Google Scholar] [CrossRef]
- Stead, W.W.; Searle, J.R.; Fessler, H.E.; Smith, J.W.; Shortliffe, E.H. Biomedical informatics: Changing what physicians need to know and how they learn. Acad. Med. 2011, 86, 429–434. [Google Scholar] [CrossRef]
- McGinnis, J.M. Evidence-based medicine-Engineering the Learning Healthcare System. Stud. Health Technol. Inform. 2010, 153, 145–157. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Tenenbaum, J.D.; James, A.; Paulyson-Nuñez, K. An Altered Treatment Plan Based on Direct to Consumer (DTC) Genetic Testing: Personalized Medicine from the Patient/Pin-cushion Perspective. J. Pers. Med. 2012, 2, 192-200. https://doi.org/10.3390/jpm2040192
Tenenbaum JD, James A, Paulyson-Nuñez K. An Altered Treatment Plan Based on Direct to Consumer (DTC) Genetic Testing: Personalized Medicine from the Patient/Pin-cushion Perspective. Journal of Personalized Medicine. 2012; 2(4):192-200. https://doi.org/10.3390/jpm2040192
Chicago/Turabian StyleTenenbaum, Jessica D., Andra James, and Kristin Paulyson-Nuñez. 2012. "An Altered Treatment Plan Based on Direct to Consumer (DTC) Genetic Testing: Personalized Medicine from the Patient/Pin-cushion Perspective" Journal of Personalized Medicine 2, no. 4: 192-200. https://doi.org/10.3390/jpm2040192