Immunocytokines

Department of Chemistry and Applied Biosciences, ETH Zürich, Wolfgang-Pauli-Strasse 10, CH-8093 Zürich, Switzerland
*
Author to whom correspondence should be addressed.
Antibodies 2012, 1(1), 70-87; https://doi.org/10.3390/antib1010070
Submission received: 27 April 2012
/
Revised: 15 May 2012
/
Accepted: 17 May 2012
/
Published: 31 May 2012
(This article belongs to the Special Issue Modes of Antibody Action for Cancer Therapy)
Abstract
:A number of cytokines have shown beneficial effects in preclinical animal models of cancer and chronic inflammatory diseases. However, cytokine treatment is often associated with severe side effects, which prevent the administration of clinically relevant doses in humans. Immunocytokines are a novel class of biopharmaceuticals, consisting of a cytokine moiety fused to monoclonal antibodies or to an antibody fragment, which selectively accumulate at the disease site and thereby enhance the therapeutic effects of cytokines. This review surveys the recent preclinical and clinical advances in the field, with a special focus on the impact of antibody formats, target antigen and cytokine moieties on the therapeutic performance in vivo. We also discuss emerging data about the possibility to combine immunocytokines with other pharmacological agents.
1. Introduction
A number of cytokines have shown beneficial effects in preclinical animal models of cancer and immune disorders and represent promising agents for therapy. However, despite encouraging results, only few cytokines are approved as drugs (e.g., interleukin 2 (IL2, Proleukin®), tumor necrosis factor (TNF, Beromun®), interferon alpha (IFNα, Roferon A® and Intron A®)). Current indications in cancer include metastatic renal cell cancer, malignant melanoma, hairy cell leukemia, chronic myeloid lymphoma, sarcoma and multiple myeloma, either as single agents or in combination with chemotherapy. In addition, certain cytokines are used for the treatment of viral and bacterial infections in the clinic and are administered to patients suffering from chronic inflammatory conditions.
Unfortunately, considerable toxicities can be observed at low doses, which prevent escalation to therapeutically active regimens. For this reason the systemic administration of cytokines rarely induces complete cure, making the further clinical development of cytokines for therapeutic approaches difficult. Alternative delivery pathways have been successfully exploited, leading to complete tumor eradication in preclinical cancer models. The most promising results were obtained by intratumoral or peritumoral application of cytokines and gene therapy approaches, including intratumoral implantation of cytokine-producing cells or cytokine gene transfection of cancer cells before implantation [1,2,3,4,5]. However, these approaches are rarely applicable in the clinical setting and are typically not efficacious in the case of disseminated disease. Nonetheless, these findings do show that cytokines can promote disease eradication, if the drug is delivered to the disease environment at a sufficient concentration.
One way to achieve specific localization of cytokines at the disease site after systemic administration consists in the use of antibodies as delivery vehicles, leading to a new class of biopharmaceutical agents, termed “immunocytokines”. These products consist of a cytokine moiety fused to monoclonal antibodies or to an antibody fragment, capable of mediating a preferential localization of the immunostimulatory payload at the site of disease. Immunocytokines have been evaluated for applications in cancer and chronic inflammatory disease [6,7]. Their therapeutic potency depends on molecular format, target antigen and cytokine fusion, as well as their combinatory function with other pharmacological agents.
2. Molecular Formats
Monoclonal antibodies bind target proteins with high affinity and selectivity and therefore represent ideal mediators of targeted therapeutic approaches for applications in cancer and immune diseases.
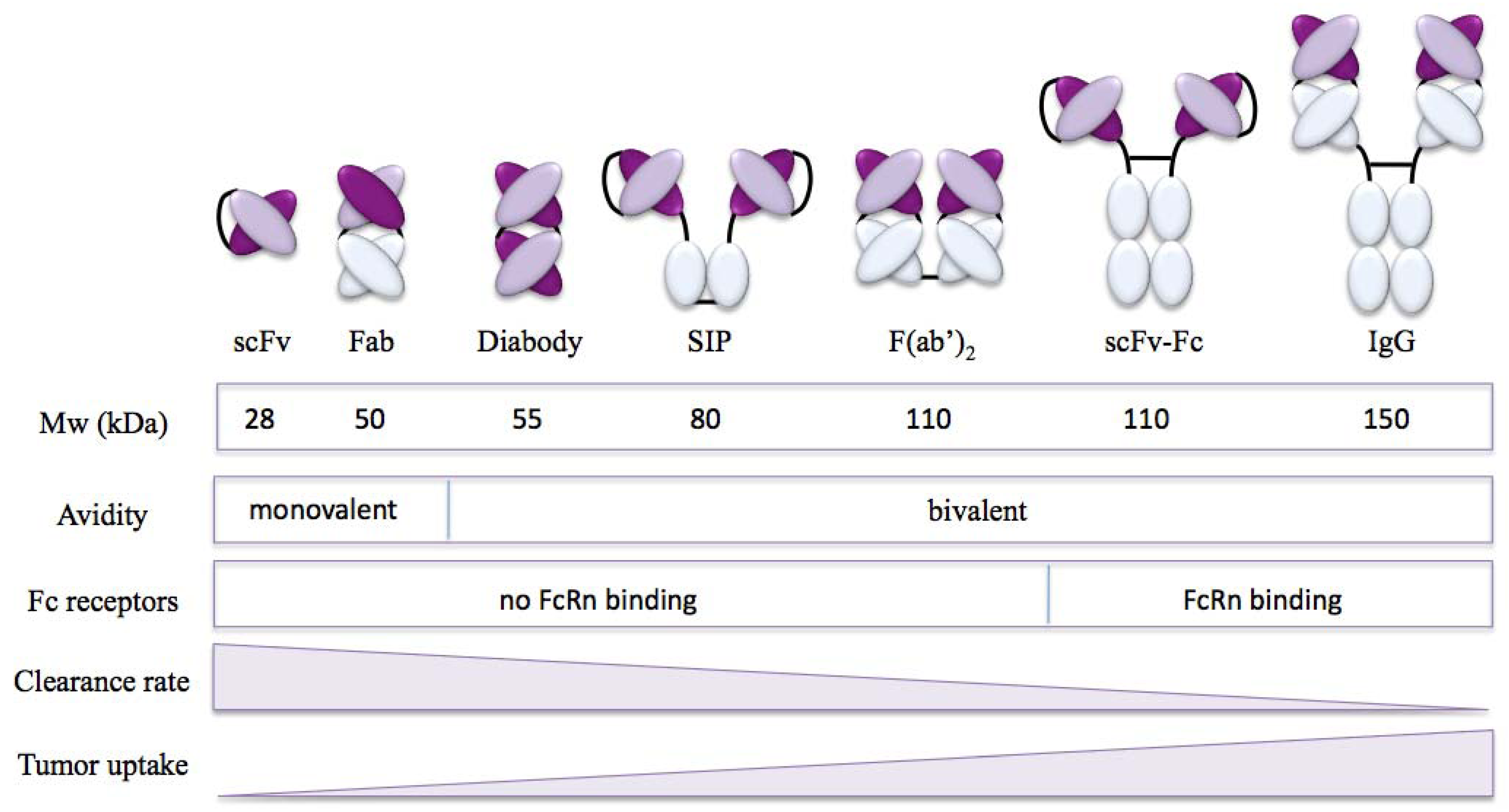
The full size IgG antibody is the most often used format for therapeutic development. However, protein engineering allows the generation of various antibody fragments with specific targeting properties defined by molecular size, blood clearance and tissue penetration and retention [8]. A number of these formats have been explored for the development of immunocytokines (Figure 1).
2.1. Targeting Properties of Antibody Formats
Full size IgG antibodies (Mw ~ 150 kDa) are Y-shaped multidomain proteins consisting of two heavy (H) chains and two light (L) chains, each of which contain a constant (C) and variable (V) region. Antigen binding is mediated in a bivalent fashion by VH and VL domains located on the two Fab (VHVLCH1CL) arms of the antibody. The remaining constant domains (CH2CH3) form the Fc region, which recruits effector functions. The bivalent nature of antibodies contributes to high affinity binding of the antigen and provides long retention times at the target site. IgGs typically display a long serum half-life (t1/2) of several days, which is mainly mediated by interaction of the Fc region with neonatal Fc receptors (FcRn) [9,10]. Binding to FcRn allows the transport of IgGs within and across cells and salvages them from default lysosomal degradation [11]. The role of this interaction in mediating prolonged antibody half-life is underlined by the finding, that IgGs with lower binding affinity to FcRn are more rapidly cleared. A number of genetic modifications as well as isotype-specific Fc properties have been explored to modify FcRn binding and serum half-life of IgG antibodies [12,13]. Tissue penetration of IgGs has been found to be slow and heterogeneous. In particular in solid tumors, which display elevated interstitial pressure, the large IgG molecule shows limited extravasation and diffusion capacity [14].
Figure 1.
Antibody formats used for the development of immunocytokines and their targeting properties.
Figure 1.
Antibody formats used for the development of immunocytokines and their targeting properties.
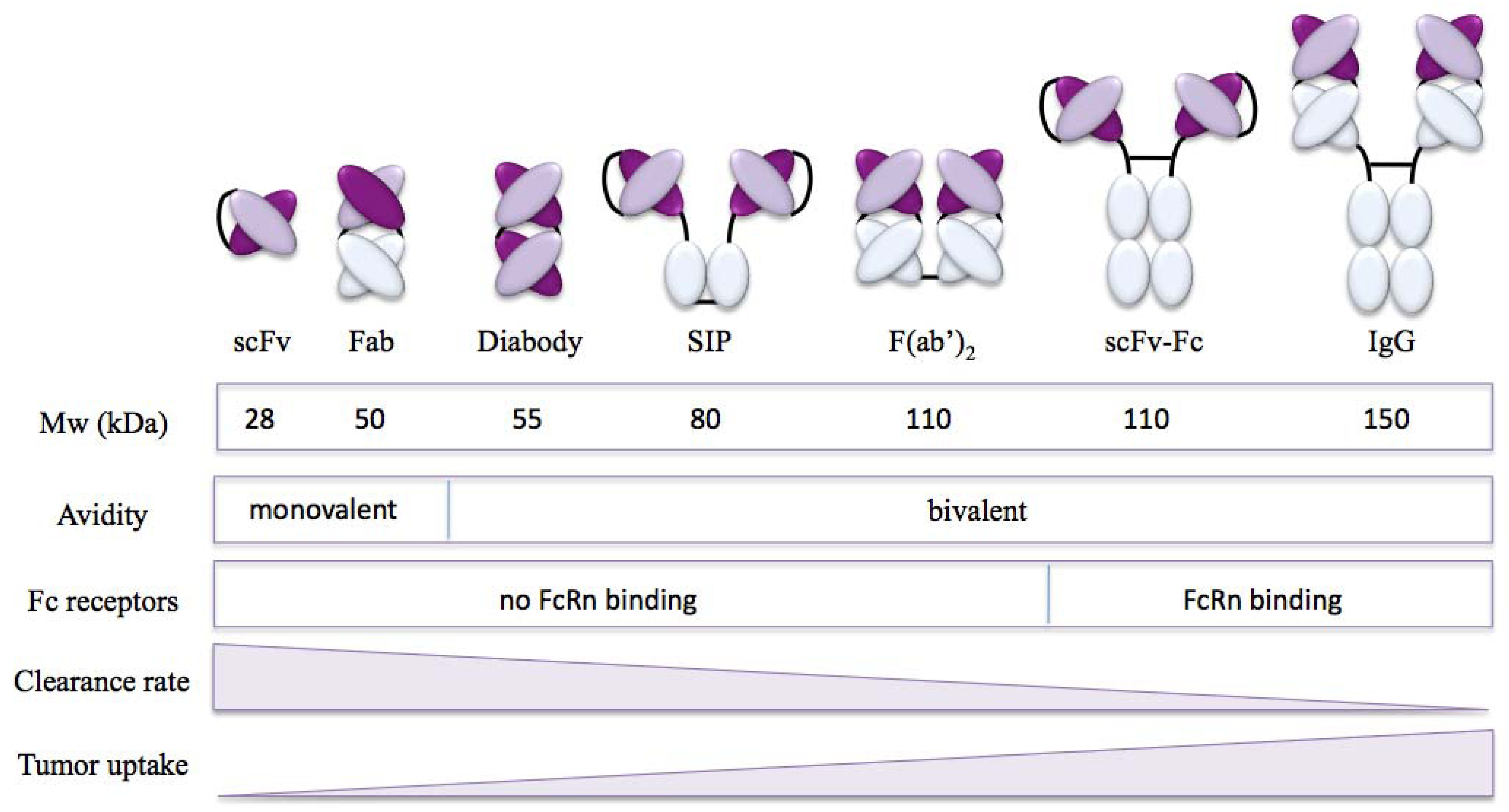
To the other extreme, single-chain Fvs (scFvs; Mw ~ 28 kDa) represent the smallest format, which retains the antigen-binding affinity, but not avidity, of the parental antibody. They consist of a variable VH and a variable VL domain fused by a flexible polypeptide linker. The low molecular weight of scFvs has shown to improve tissue penetration compared to IgGs [15,16]. However, rapid clearance of the small fragments combined with reduced retention property due to the monovalent nature of the antigen interaction leads to low absolute accumulation (8–10 fold lower than IgG) at the target site [17].
A number of multivalent antibody formats (i.e., diabody, SIP, scFvFc) of intermediate size have been engineered to profit from longer target-site retention than scFvs, as well as deeper tissue penetration compared to full size IgGs [8,18]. For example, reducing the linker length of the scFv to 5 residues or less, promotes the formation of stable scFv homodimers, called diabodies (Mw ~ 55k Da) [19]. This bivalent format displays high tumor-to-blood ratios with an increased absolute tumor accumulation compared to scFv of the same antigen specificity.
2.2. Targeting Properties of Immunocytokines
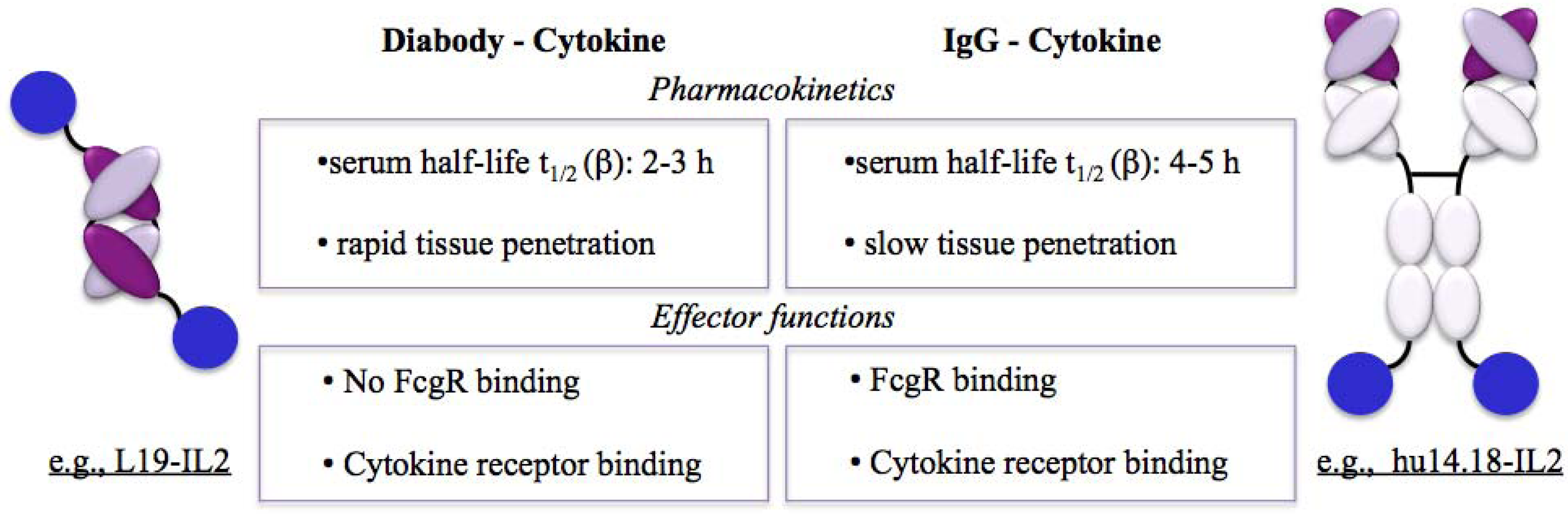
The clinically most advanced immunocytokines are recombinant fusion proteins in which the antibody moiety is used in the full IgG or in diabody format (Figure 2).
Figure 2.
Comparison of the antibody formats of clinical stage immunocytokines.
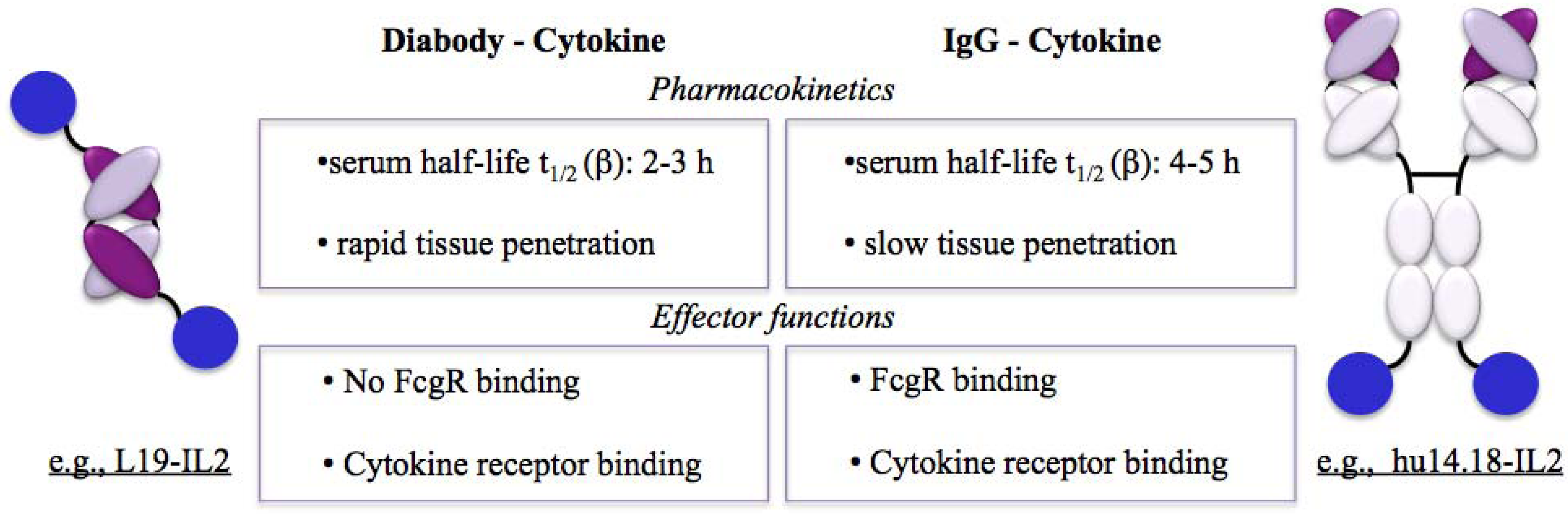
Immunocytokines have been reported to display a significantly reduced serum half-life compared to their corresponding naked antibody [20]. The IgG-IL2 fusion protein hu14.18-IL2, for example, displayed a serum half-life of ~4 h in melanoma and neuroblastoma patients [21]. In comparison, the serum half-life of the diabody L19 was 2–3 h when fused to IL2 [22]. In either case this represents a significant decrease of blood clearance of IL2 alone (t1/2 ~ 30–45 min) [20].
In some cases the cytokine moiety of immunocytokines can significantly interfere with targeting. One example is the immunocytokine L19-IFNγ, which targeted tumors in mice lacking IFNγ receptors, but not in wild-type mice [23].
Enrichment of cytokines at the target site is mediated by the antibody-antigen interaction. Recruiting effector functions is crucial for the therapeutic effect of immunocytokines and is mediated by binding of the cytokine moiety to the correspondent cytokine receptors on effector cells. For example, binding of the IL2 moiety of immunocytokines to the IL2 receptor stimulates the expansion and activation of immune cells such as cytotoxic T cells and natural killer (NK) cells. Newly generated antibody fusion proteins are validated for functional cytokine signaling.
In addition, immunocytokines can activate antigen dependent cellular cytotoxicity (ADCC). The Fc region of IgG-based fusion proteins mediates ADCC by binding Fcγ receptors (FcγR) on the surface of immune effector cells, such as NK cells. IL2 immunocytokines have shown that IL2 enhances the ADCC function of antibodies [7,24,25]. Recent findings describe the formation of activating immune synapses (AIS) between FcR-deficient NK cells and tumor cells mediated by IL2 immunocytokines. These functional AIS were formed by the interaction of the IL2 component of the immunocytokine and IL2 receptors on effector cells [26,27], demonstrating that IL2 immunocytokines can initiate direct target cell lysis even without Fc involvement.
3. Targets
Antibody-based delivery of cytokines to the site of disease requires the presence of accessible, abundant and stable target antigens, which allow a clear discrimination between diseased tissue and healthy organs. Potential targets can be expressed either directly on the surface of cancer cells or in the disease environment. Both of these targeting strategies have been exploited for the development of immunocytokines. The targets of the most advanced immunocytokines are described in Table 1.

{kind=link}
{kind=link}
| Antigen | Expression profile | Antibody |
|---|---|---|
| Disease cell surface | ||
| EpCAM Epithelial cell adhesion molecule | Physiologically expressed in epithelia Over-expressed in breast, colorectal and pancreatic carcinomas. | KS |
| GD2 Disialoganglioside | Physiological expression restricted to cerebellum and peripheral nerves. Expressed in neuroectodermal tumors including melanoma, neuroblastoma. | Ch14.18 |
| Disease environment | ||
| EDA / EDB of fibronectin Extra-domains EDA and EDB of fibronectin | Physiological expression restricted to endometrium in the proliferating phase. Expressed around the neo-vasculature and in the stroma of aggressive tumours and in chronic inflammation. | F8 / L19 and BC1 |
| A1 domain of Tenascin-C | Physiological expression restricted to endometrium in the proliferating phase. Expressed around the neo-vasculature and in the stroma of aggressive tumours and in chronic inflammation. | F16 |
| DNA / Histone complexes | Normally not accessible. Exposed in necrotic tissue. | NHS |
3.1. Targeting the Cell Surface
Epithelial cell adhesion molecule (EpCAM) is a well-described cell surface antigen for a broad range of carcinomas, such as breast, colorectal and pancreatic carcinomas. EpCAM overexpression is considered to be a marker of tumor initiating cells and is involved in cancer metastasis. However, the selectivity of EpCAM is limited by its expression in healthy epithelia [28,29].
3.2. Targeting the Disease Environment
Progression of cancer or immune diseases involves the formation of a specific disease environment, which involves tissue remodeling, angiogenesis and the recruitment of stromal and immune cells [33,34]. Disease environments provide a number of well accessible target structures.
Newly formed blood vessels are particularly attractive targets for antibody-mediated delivery approaches. Vascular antigens are readily reached via the blood stream and angiogenesis is involved in the disease progression of most cancers as well as numerous inflammatory diseases [35]. Our group has extensively studied the in vivo performance of vascular targeting antibodies [36]. Splice isoforms of fibronectin and of tenascin-C represent some of the best-characterized markers of newly formed blood vessels [37]. Specifically, the alternatively-spliced extra-domains EDA and EDB of fibronectin, as well as the extra-domain A1 of tenascin-C, are virtually undetectable in normal adult tissues, but are strongly expressed at sites of physiological and pathogenic angiogenesis. The human monoclonal antibodies F8, L19 and F16 specifically recognize the EDA and EDB domains of fibronectin and the A1 domain of tenascin-C, respectively, and have shown selective accumulation at the disease site in a broad range of cancers and inflammatory disorders in animal models as well as in patients [38,39,40,41].
An alternative approach, termed target necrosis therapy (TNT), targets necrotic tissue, which is present primarily in the hypoxic environment of solid tumors and is absent in the healthy body. The monoclonal antibody NHS76 recognizes DNA / histone complexes, which have been demonstrated to be exposed by necrotic cells in the tumor core as well as metastases [42,43].
3.3. Target Identification
The identification of novel disease markers is of great importance for the development of targeted therapies. This process is driven mainly by comparative transcriptomic [44] and proteomic technologies, which have rapidly advanced in the past years [44,45,46]. For example, in vivo labeling followed by proteomic analysis has led to the identification a number of vascular accessible antigens [47,48], some of which are expressed in a broad range of diseases [39,49], while others are more restricted to specific malignancies [50].
4. Fusion Partners
Cytokines are a diverse group of immune-modulators, which can have pro-inflammatory or anti-inflammatory activity, depending on the microenvironment. Under normal conditions pro- and anti-inflammatory stimuli are carefully balanced to ensure an adequate immune response. This balance is disturbed in pathological settings, such as cancer progression and inflammatory disorders [51,52]. Understanding the functions of cytokines as well as the immunological environment of pathologies is important when choosing antibody fusion partners for the generation of immunocytokines as therapeutic agents. A number of cytokines have been tested for the generation of immunocytokines. A conclusive list of preclinical findings can be found in [6]. In this review we will focus on the clinical stage antibody-cytokine fusions, which are listed in Table 2.
4.1. Cytokines in Cancer
Tumor formation and progression is a complex process involving a multitude of changes within both cancer cells and the body’s defense mechanisms. The tumor microenvironment harbors cytokines and other inflammatory mediators, which influence immunosurveillance, the growth of cancer cells, tissue remodeling and angiogenesis [33]. Anti-inflammatory factors, mainly IL10 and TGFβ, interfere with the cell-mediated immune response against cancer cells and promote tumor development. However, pro-inflammatory signals and chronic inflammation also play a crucial role in tumor growth and progression [51,53].
The development of immunocytokines for cancer therapies has so far focused on the delivery of pro-inflammatory cytokines, which mediate the infiltration of leukocytes into the tumor mass and promote an antitumor immune response. The most promising results were reported for fusion proteins with interleukin 2 (IL2), interleukin 12 (IL12) and tumor necrosis factor (TNF).
| Compound | Antibody format | Target antigen | Indications | Clinical phase | Company |
|---|---|---|---|---|---|
| Pro-inflammatory | |||||
| F16-IL2 | Diabody | A1 domain of tenascin-C | Breast cancer and lung cancer | Phase II | Philogen |
| L19-IL2 | Diabody | EDB of fibronectin | Melanoma | Phase II | Philogen |
| hu14.18-IL2 | IgG | GD2 | Melanoma and neuroblastoma | Phase I/II | Merck KGaA |
| KS-IL2 | IgG | EpCAM | Ovarian cancer, colorectal cancer, prostate cancer and NSCL carcinoma | Phase I | Merck KGaA |
| NHS-IL2LT | IgG | DNA/ histone | Non-Hodgkin lymphoma and NSCL carcinoma | Phase I | Merck KGaA |
| NHS-IL12 | IgG | DNA/ histone | Epithelial and mesenchymal malignant tumors | Phase I | Merck KGaA |
| BC1-IL12 | IgG | EDB of fibronectin | Melanoma | Phase I/II | Antisoma |
| L19-TNF | Trimeric scFv | EDB of fibronectin | Melanoma (isolated limb perfusion) | Phase I/II | Philogen |
| Anti-inflammatory | |||||
| F8-IL10 | Diabody | EDA of fibronectin | Rheumatoid arthritis | Phase I | Philogen |
4.1.1. IL2-Based Immunocytokines
Recombinant IL2 (rIL2, Proleukin®) is commonly used in the clinic for the treatment of patients with metastatic renal cell carcinoma and melanoma [54,55]. For this reason, IL2 fusion proteins account for the most advanced immunocytokines in clinical development. There are currently five IL2 based immunocytokines in clinical trials.
L19-IL2 successfully targeted the neo-vasculature of several tumors in preclinical mouse models, as determined by quantitative biodistribution studies and therapy experiments [56,57]. Clinical trials in patients with metastatic renal carcinoma resulted in disease stabilization in 83% of the patients after the two cycles of the recommended dose (i.e., 22.5 Mio IU/patient/day—3 injections/week), promoting a median progression-free survival of 8 months (1.5–30.5 months) [22].
F16-IL2, a second vascular targeting antibody-IL2 fusion protein, is currently being tested in a phase II trial in patients with breast or lung cancer [58].
Ch14.18-IL2, which recognizes GD2, was clinically tested for applications in melanoma and neuroblastoma. Disease stabilization was achieved in 58% of melanoma patients after the first cycle (i.e., one week) of ch14.18-IL2 administration in a phase I trial. However, after the second cycle (i.e., six weeks) only 24% of the patients still displayed stable disease. The maximal tolerated dose was determined to be 7.5 mg/m2/d. In line with the results from the phase I trial, only 2 out of 9 patients reached disease stabilization after treatment with 4–6 cycles (at 4 mg/m2/d) of ch14.18-IL2 in phase II studies. No objective responses were observed [59,60]. In children with neuroblastoma, the recommended dose of ch14.18-IL2 was determined (110 Mio IU/m2 over 3 days) and its administration led to disease stabilization in 54% of the patients in a phase I trial. In a subsequent phase II trial 21.7% of patients with low tumor load (i.e., disease evaluable only by (123I)metaiodobenzylguanidine scintigraphy or bone marrow histology) experienced a complete response, whereas patients with bulky disease unfortunately did not respond [61,62].
Two additional immunocytokines, the EpCAM targeting KS-IL2 and the DNA targeting NHS-IL2LT, have been tested in phase I clinical trials [63,64].
In general, the adverse side effects caused by IL2 immunocytokines are comparable to the ones reported for IL2 alone, including hypotension, fever, rigor, neuropathic pain, hypoxia, pruritus, allergic reactions, hypophosphatemia, thrombocytopenia, leucopenia and neutropenia. IL2 based immunocytokines have so far been administered at 67.5–110 Mio IU IL2 equivalents/m2 per week for 4–6 treatment cycles (one cycle: 21–28 days) [22,62]. In comparison, rIL2 is applied from 100 Mio IU/m2 per week for at least 6 cycles as a low dose regimen to 900 Mio IU/ week as an intense regimen [65,66]. The reduction in dose, which can be achieved by selective delivery of IL2 to the site of disease helps reduce the incidence and severity of side effects.
4.1.2. IL12- and TNF-Based Immunocytokines
IL12 plays an important role in the activities of natural killer cells and T lymphocytes. The antitumor activity of recombinant IL12 (rIL12) has been demonstrated in several animal models and further evaluated in a number of clinical trials in humans. However, the systemic administration of 1–1.5 μg/week of rIL12 was associated with significant toxicities, which prevented further clinical development of rIL12 as a single agent for cancer therapy [67].
Preclinical findings show that the antibody-based targeted delivery of IL12 mediated the infiltration of macrophages, lymphocyte-activated killer (LAK) cells, NK cells, and T lymphocytes into the tumor mass and resulted in an increase of anti-angiogenic stimuli. IL12-based immunocytokines can greatly improve the effects of IL12, allowing therapeutic benefits at (up to 20-fold) lower administrated doses [68].
Two IL12 based immunocytokines have progressed to clinical trials.
The immunocytokine NHS-IL12, which targets DNA / histone complexes in necrotic regions of tumors, is currently being evaluated in a phase I trial [69].
The antibody BC1-IL12 recognizes the neo-vascular antigen EDB of fibronectin and was tested in a phase I trial in patients with malignant melanoma or renal cell carcinoma. The recommended dose was set at 15 μg/kg weekly (corresponds to a 3–5 fold molar increase compared to rIL12) and treatment promoted disease stabilization in 2 out of 13 patients [70].
TNF is one of the most potent antitumor cytokines. However, its substantial toxic side effects prevent systemic administration at therapeutically effective doses. The clinical use of TNF has therefore been limited to regional applications, such as Isolated Limb Perfusion for the treatment of nonresectable sarcoma and melanoma [71]. The immunocytokine L19-TNF is being evaluated in a phase I/II clinical trial [72,73].
4.2. Cytokines in Chronic Inflammatory Diseases
Chronic inflammatory diseases, such as rheumatoid arthritis, psoriasis, endometriosis, atherosclerosis or inflammatory bowel disease, are characterized by persistent inflammation mediated by complex interactions between immune cells and the disease microenvironment. These commonly both activate the immune system and interfere with pathways involved in the resolution of inflammation [34,52].
Immunocytokines based on the anti-inflammatory cytokine interleukin 10 (IL10) have been tested for applications in rheumatoid arthritis, psoriasis and endometriosis.
4.2.1. IL10 Immunocytokines
Recombinant IL10 (rIL10, TenovilTM) demonstrated promising in vitro immunomodulatory activity as well as therapeutic benefit in a number of animal models of chronic inflammation. And clinical evaluation in patients with inflammatory disorders showed an excellent tolerability profile at doses up to 25 μg/kg. However, the clinical development of rIL10 was discontinued due to lack of efficacy 74,75]. IL10-based immunocytokines targeting the neo-vasculature (F8-IL10 and L19-IL10) were tested in preclinical models of rheumatoid arthritis, psoriasis and endometriosis with encouraging outcomes. F8-IL10 has progressed to the clinic and is currently being tested in a phase I trial in patients with rheumatoid arthritis [76,77,78].
5. Combination Studies
5.1. Selected Preclinical Combination Therapies
A number of preclinical studies have been performed to explore the combinatorial effect of immunocytokines with other therapeutic agents, such as chemotherapeutics, monoclonal antibodies and other biologicals.
Most chemotherapeutics that are used for cancer therapy are traditionally considered to be immunosuppressive by killing or inhibiting the progression of dividing cells, including lymphocytes. But accumulating evidence indicates that cytotoxic drugs and radiotherapy also indirectly and directly effect the immune system to contribute to tumor regression [79].
For example, preclinical combination experiments with F8-IL2 [80] and KS-IL2 [81] showed that paclitaxel, when administered prior to the immunocytokine, enhances the antibody-targeted delivery of IL2 to the disease site and promotes a synergistic anti-cancer effect in different cancer models. Encouraging results were also observed for the combination of F16-IL2 and temozolomide in an ortothopic glioblastoma mouse model, demonstrating the effective delivery of cytokines to a pathological disorder in the brain [82]. In this case simultaneous administration of the immunocytokine and the chemotherapeutic agent led to complete eradication of lymphoma xenografts [57].
Radiofrequency ablation (RFA) followed by KS-IL2 treatment enhanced the antitumor effect and survival, compared to mice treated with RFA or KS-IL2 alone, in a murine colon adenocarcinoma model [83].
Some antibody-cytokine fusions (in particular IL2- and TNF-based immunocytokines) display vasoactive properties and can therefore also enhance the uptake of therapeutic agents at disease site, if administered as a pretreatment [84]. In general, immunocytokines and conventional chemotherapeutic agents are promising combination partners because they typically do not exhibit overlapping limiting toxicities. But the ideal combination partners, dose regimen and also administration sequence have to be elucidated for different disease settings.
The combined use of therapeutic antibodies and cytokines has been shown to potentiate the ADCC, due to an increase of effector cells [85,86]. And in fact, a synergistic therapeutic effect was observed for F8-IL2 and the monoclonal antibody sunitinib in mouse models of renal cell carcinomas [87]. A comparable effect was described for the combination of L19-IL2 and rituximab in a mouse model of B-cell lymphoma [57].
In addition, the combination of different immunocytokines, such as L19-IL12 and L19-TNF, demonstrated enhanced therapeutic benefit compared to the administration of each immunocytokine alone [88]. In accordance with these findings, bifunctional antibody cytokine fusion proteins (KS-IL2/IL12) displayed synergistic effects in vivo [89].
5.2. Combination Therapies in Clinical Development
Some clinical results of combination therapies with immunocytokines and chemotherapeutic agents have recently been reported. The combination of KS-IL2 with cyclophosphamide and the combination of F16-IL2 with doxorubicin or with paclitaxel are being studied in phase Ib clinical trials in patients with solid tumors [90,91]. And the combined use of L19-IL2 (at the same dose applied as monotherapy) with dacarbazine showed an excellent tolerability profile and led to objective responses in 8/29 patients and a complete response in one patient in a phase Ib trial in patients with metastatic melanoma. This combination therapy is currently being evaluated in a randomized phase II trial [92].
6. Concluding Remarks
This review surveys the recent preclinical and clinical advances in the field of immunocytokines, with a special focus on the impact of molecular formats, target antigen, cytokine moieties and combination approaches on therapeutic performance.
Several antibody formats and their specific targeting properties have been explored during the development of immunocytokines. The clinically most advanced immunocytokines are recombinant fusion proteins in which the antibody moiety is in the full IgG or in the diabody format.
The identification of selective antigens is a prerequisite for the antibody-based delivery of cytokines to the site of disease. A number of potential targets can be considered, including those located on the surface of diseased cells (e.g., cancer cells) or in the modified extracellular matrix. The targeting of newly formed pathological blood vessels is particularly attractive and has found application in a wide range of malignancies, but also for the treatment of chronic inflammatory diseases.
Preclinical and clinical experiments with antibody-cytokine fusion proteins have demonstrated that increased accumulation at the disease site enhances the therapeutic index of the corresponding cytokine [6]. The development of immunocytokines for cancer therapies has focused on the delivery of pro-inflammatory cytokines (IL2, IL12 and TNF), whereas anti-inflammatory cytokines (IL10) are used for the treatment of chronic diseases, such as rheumatoid arthritis.
The translation of preclinical findings to clinical settings, however, remains one of the main challenges for the future.
When used as single agent, immunocytokines are rarely curative. For this reason, a number of combination therapies with other pharmacological agents have been tested. The combined use of immunocytokines and chemotherapeutics for cancer therapy has been extensively studied and is currently being investigated in clinical trials.
The large diversity in disease characteristics as well as immunological state of patients may have a significant impact on the function of immunocytokines. To address this issue imaging techniques (e.g., nuclear medicine techniques like positron emission tomography) could in principle be used to screen patients for antigen expression and selective targeting of the antibody prior to treatment [93]. In addition, the recent discovery that cancer cells release peptides bound to soluble HLA-I molecules, which can be identified and quantified by mass spectrometry, indicates potential avenues for non-invasive assessment of tumor-antigens that are displayed at the tumor site [94].
Taken together, progress in antibody engineering, identification of accessible and selective markers of disease, use of different cytokine moieties and the combination with other therapeutics has driven the development of immunocytokine therapies. We anticipate that immunocytokines will find an increasing use in clinical settings, in particular for the treatment of cancers and chronic inflammatory diseases.
Acknowledgments
This work was supported by the Swiss National Science Foundation, the ETH Zürich, the European Union (ADAMANT Project), the Swiss Cancer League, the Swiss Bridge Foundation and the Stammbach Foundation.
Conflict of Interest
Dario Neri is a co-founder and shareholder of Philogen (www.philogen.com), the company that owns the F8, L19 and F16 antibodies.
References
- Miller, P.W.; Sharma, S.; Stolina, M.; Butterfield, L.H.; Luo, J.; Lin, Y.; Dohadwala, M.; Batra, R.K.; Wu, L.; et al. Intratumoral administration of adenoviral interleukin 7 gene-modified dendritic cells augments specific antitumor immunity and achieves tumor eradication. Hum. Gene Ther. 2000, 11, 53–65. [Google Scholar] [CrossRef]
- Aoki, T.; Tashiro, K.; Miyatake, S.; Kinashi, T.; Nakano, T.; Oda, Y.; Kikuchi, H.; Honjo, T. Expression of murine interleukin 7 in a murine glioma cell line results in reduced tumorigenicity in vivo. Proc. Natl. Acad. Sci. USA 1992, 89, 3850–3854. [Google Scholar]
- Koshita, Y.; Lu, Y.; Fujii, S.; Neda, H.; Matsuyama, T.; Satoh, Y.; Itoh, Y.; Takahashi, M.; Kato, J.; Sakamaki, S.; et al. Efficacy of TNF-alpha gene-transduced tumor cells in treatment of established in vivo tumor. Int. J. Cancer 1995, 63, 130–135. [Google Scholar] [CrossRef]
- Barker, S.E.; Grosse, S.M.; Siapati, E.K.; Kritz, A.; Kinnon, C.; Thrasher, A.J.; Hart, S.L. Immunotherapy for neuroblastoma using syngeneic fibroblasts transfected with IL-2 and IL-12. Br. J. Cancer 2007, 97, 210–217. [Google Scholar] [CrossRef]
- Jackaman, C.; Bundell, C.S.; Kinnear, B.F.; Smith, A.M.; Filion, P.; van Hagen, D.; Robinson, B.W.; Nelson, D.J. IL-2 intratumoral immunotherapy enhances CD8+ T cells that mediate destruction of tumor cells and tumor-associated vasculature: A novel mechanism for IL-2. J. Immunol. 2003, 171, 5051–5063. [Google Scholar]
- Pasche, N.; Neri, D. Immunocytokines: A novel class of potent armed antibodies. Drug Discov. Today 2012.
- Schrama, D.; Reisfeld, R.A.; Becker, J.C. Antibody targeted drugs as cancer therapeutics. Nat. Rev. Drug Discov. 2006, 5, 147–159. [Google Scholar]
- Holliger, P.; Hudson, P.J. Engineered antibody fragments and the rise of single domains. Nat. Biotechnol. 2005, 23, 1126–1136. [Google Scholar] [CrossRef]
- Kuo, T.T.; Aveson, V.G. Neonatal Fc receptor and IgG-based therapeutics. MAbs 2011, 3, 422–430. [Google Scholar] [CrossRef]
- Woof, J.M.; Burton, D.R. Human antibody-Fc receptor interactions illuminated by crystal structures. Nat. Rev. Immunol. 2004, 4, 89–99. [Google Scholar] [CrossRef]
- Ward, E.S.; Martinez, C.; Vaccaro, C.; Zhou, J.; Tang, Q.; Ober, R.J. From sorting endosomes to exocytosis: Association of Rab4 and Rab11 GTPases with the Fc receptor, FcRn, during recycling. Mol. Biol. Cell 2005, 16, 2028–2038. [Google Scholar] [CrossRef]
- Vaccaro, C.; Zhou, J.; Ober, R.J.; Ward, E.S. Engineering the Fc region of immunoglobulin G to modulate in vivo antibody levels. Nat. Biotechnol. 2005, 23, 1283–1288. [Google Scholar] [CrossRef]
- Pop, L.M.; Liu, X.; Ghetie, V.; Vitetta, E.S. The generation of immunotoxins using chimeric anti-CD22 antibodies containing mutations which alter their serum half-life. Int. Immunopharmacol. 2005, 5, 1279–1290. [Google Scholar] [CrossRef]
- Jain, R.K.; Baxter, L.T. Mechanisms of heterogeneous distribution of monoclonal antibodies and other macromolecules in tumors: Significance of elevated interstitial pressure. Cancer Res. 1988, 48, 7022–7032. [Google Scholar]
- Yokota, T.; Milenic, D.E.; Whitlow, M.; Schlom, J. Rapid tumor penetration of a single-chain Fv and comparison with other immunoglobulin forms. Cancer Res. 1992, 52, 3402–3408. [Google Scholar]
- Graff, C.P.; Wittrup, K.D. Theoretical analysis of antibody targeting of tumor spheroids: Importance of dosage for penetration, and affinity for retention. Cancer Res. 2003, 63, 1288–1296. [Google Scholar]
- Milenic, D.E.; Yokota, T.; Filpula, D.R.; Finkelman, M.A.; Dodd, S.W.; Wood, J.F.; Whitlow, M.; Snoy, P.; Schlom, J. Construction, binding properties, metabolism, and tumor targeting of a single-chain Fv derived from the pancarcinoma monoclonal antibody CC49. Cancer Res. 1991, 51, 6363–6371. [Google Scholar]
- Borsi, L.; Balza, E.; Bestagno, M.; Castellani, P.; Carnemolla, B.; Biro, A.; Leprini, A.; Sepulveda, J.; Burrone, O.; Neri, D.; Zardi, L. Selective targeting of tumoral vasculature: Comparison of different formats of an antibody (L19) to the ED-B domain of fibronectin. Int. J. Cancer 2002, 102, 75–85. [Google Scholar] [CrossRef]
- Holliger, P.; Prospero, T.; Winter, G. Diabodies": Small bivalent and bispecific antibody fragments. Proc. Natl. Acad. Sci. USA 1993, 90, 6444–6448. [Google Scholar]
- Kendra, K.; Gan, J.; Ricci, M.; Surfus, J.; Shaker, A.; Super, M.; Frost, J.D.; Rakhmilevich, A.; Hank, J.A.; Gillies, S.D.; Sondel, P.M. Pharmacokinetics and stability of the ch14.18-interleukin-2 fusion protein in mice. Cancer Immunol. Immunother. 1999, 48, 219–229. [Google Scholar] [CrossRef]
- Yamane, B.H.; Hank, J.A.; Albertini, M.R.; Sondel, P.M. The development of antibody-IL-2 based immunotherapy with hu14.18-IL2 (EMD-273063) in melanoma and neuroblastoma. Expert Opin. Investig. Drugs 2009, 18, 991–1000. [Google Scholar] [CrossRef]
- Johannsen, M.; Spitaleri, G.; Curigliano, G.; Roigas, J.; Weikert, S.; Kempkensteffen, C.; Roemer, A.; Kloeters, C.; Rogalla, P.; Pecher, G.; et al. The tumour-targeting human L19-IL2 immunocytokine: Preclinical safety studies, phase I clinical trial in patients with solid tumours and expansion into patients with advanced renal cell carcinoma. Eur. J. Cancer 2010, 46, 2926–2935. [Google Scholar]
- Ebbinghaus, C.; Ronca, R.; Kaspar, M.; Grabulovski, D.; Berndt, A.; Kosmehl, H.; Zardi, L.; Neri, D. Engineered vascular-targeting antibody-interferon-gamma fusion protein for cancer therapy. Int. J. Cancer 2005, 116, 304–313. [Google Scholar] [CrossRef]
- Naramura, M.; Gillies, S.D.; Mendelsohn, J.; Reisfeld, R.A.; Mueller, B.M. Mechanisms of cellular cytotoxicity mediated by a recombinant antibody-IL2 fusion protein against human melanoma cells. Immunol. Lett. 1993, 39, 91–99. [Google Scholar] [CrossRef]
- Alderson, K.L.; Sondel, P.M. Clinical cancer therapy by NK cells via antibody-dependent cell-mediated cytotoxicity. J. Biomed. Biotechnol. 2011, 379123. [Google Scholar]
- Buhtoiarov, I.N.; Neal, Z.C.; Gan, J.; Buhtoiarova, T.N.; Patankar, M.S.; Gubbels, J.A.; Hank, J.A.; Yamane, B.; Rakhmilevich, A.L.; Reisfeld, R.A.; et al. Differential internalization of hu14.18-IL2 immunocytokine by NK and tumor cell: Impact on conjugation, cytotoxicity, and targeting. J. Leukoc. Biol. 2011, 89, 625–638. [Google Scholar] [CrossRef]
- Gubbels, J.A.; Gadbaw, B.; Buhtoiarov, I.N.; Horibata, S.; Kapur, A.K.; Patel, D.; Hank, J.A.; Gillies, S.D.; Sondel, P.M.; Patankar, M.S.; Connor, J. Ab-IL2 fusion proteins mediate NK cell immune synapse formation by polarizing CD25 to the target cell-effector cell interface. Cancer Immunol. Immunother. 2011, 60, 1789–1800. [Google Scholar] [CrossRef]
- Patriarca, C.; Macchi, R.M.; Marschner, A.K.; Mellstedt, H. Epithelial cell adhesion molecule expression (CD326) in cancer: A short review. Cancer Treat. Rev. 2012, 38, 68–75. [Google Scholar] [CrossRef]
- Gires, O. Lessons from common markers of tumor-initiating cells in solid cancers. Cell Mol. Life Sci. 2011, 68, 4009–4022. [Google Scholar] [CrossRef]
- Mujoo, K.; Cheresh, D.A.; Yang, H.M.; Reisfeld, R.A. Disialoganglioside GD2 on human neuroblastoma cells: Target antigen for monoclonal antibody-mediated cytolysis and suppression of tumor growth. Cancer Res. 1987, 47, 1098–1104. [Google Scholar]
- Chang, H.R.; Cordon-Cardo, C.; Houghton, A.N.; Cheung, N.K.; Brennan, M.F. Expression of disialogangliosides GD2 and GD3 on human soft tissue sarcomas. Cancer 1992, 70, 633–638. [Google Scholar] [CrossRef]
- Svennerholm, L.; Bostrom, K.; Fredman, P.; Jungbjer, B.; Lekman, A.; Mansson, J.E.; Rynmark, B.M. Gangliosides and allied glycosphingolipids in human peripheral nerve and spinal cord. Biochim. Biophys. Acta 1994, 1214, 115–123. [Google Scholar]
- Allen, M.; Louise Jones, J. Jekyll and Hyde: The role of the microenvironment on the progression of cancer. J. Pathol. 2011, 223, 162–176. [Google Scholar]
- Filer, A.; Pitzalis, C.; Buckley, C.D. Targeting the stromal microenvironment in chronic inflammation. Curr. Opin. Pharmacol. 2006, 6, 393–400. [Google Scholar] [CrossRef]
- Carmeliet, P. Angiogenesis in health and disease. Nat. Med. 2003, 9, 653–660. [Google Scholar] [CrossRef]
- Schliemann, C.; Neri, D. Antibody-based vascular tumor targeting. Recent Results Cancer Res. 2010, 180, 201–216. [Google Scholar] [CrossRef]
- Neri, D.; Bicknell, R. Tumour vascular targeting. Nat. Rev. Cancer 2005, 5, 436–446. [Google Scholar] [CrossRef]
- Neri, D.; Carnemolla, B.; Nissim, A.; Leprini, A.; Querze, G.; Balza, E.; Pini, A.; Tarli, L.; Halin, C.; Neri, P.; Zardi, L.; Winter, G. Targeting by affinity-matured recombinant antibody fragments of an angiogenesis associated fibronectin isoform. Nat. Biotechnol. 1997, 15, 1271–1275. [Google Scholar]
- Schwager, K.; Villa, A.; Rosli, C.; Neri, D.; Rosli-Khabas, M.; Moser, G. A comparative immunofluorescence analysis of three clinical-stage antibodies in head and neck cancer. Head Neck Oncol. 2011, 3, 25. [Google Scholar] [CrossRef]
- Santimaria, M.; Moscatelli, G.; Viale, G.L.; Giovannoni, L.; Neri, G.; Viti, F.; Leprini, A.; Borsi, L.; Castellani, P.; Zardi, L.; Neri, D.; Riva, P. Immunoscintigraphic detection of the ED-B domain of fibronectin, a marker of angiogenesis, in patients with cance. Clin. Cancer Res. 2003, 9, 571–579. [Google Scholar]
- Tarli, L.; Balza, E.; Viti, F.; Borsi, L.; Castellani, P.; Berndorff, D.; Dinkelborg, L.; Neri, D.; Zardi, L. A high-affinity human antibody that targets tumoral blood vessels. Blood 1999, 94, 192–198. [Google Scholar]
- Sharifi, J.; Khawli, L.A.; Hu, P.; King, S.; Epstein, A.L. Characterization of a phage display-derived human monoclonal antibody (NHS76) counterpart to chimeric TNT-1 directed against necrotic regions of solid tumors. Hybrid. Hybridomics 2001, 20, 305–312. [Google Scholar] [CrossRef]
- Chen, S.; Yu, L.; Jiang, C.; Zhao, Y.; Sun, D.; Li, S.; Liao, G.; Chen, Y.; Fu, Q.; Tao, Q.; et al. Pivotal study of iodine-131-labeled chimeric tumor necrosis treatment radioimmunotherapy in patients with advanced lung cancer. J. Clin. Oncol. 2005, 23, 1538–1547. [Google Scholar]
- St Croix, B.; Rago, C.; Velculescu, V.; Traverso, G.; Romans, K.E.; Montgomery, E.; Lal, A.; Riggins, G.J.; Lengauer, C.; Vogelstein, B.; Kinzler, K.W. Genes expressed in human tumor endothelium. Science 2000, 289, 1197–1202. [Google Scholar]
- Oh, P.; Li, Y.; Yu, J.; Durr, E.; Krasinska, K.M.; Carver, L.A.; Testa, J.E.; Schnitzer, J.E. Subtractive proteomic mapping of the endothelial surface in lung and solid tumours for tissue-specific therapy. Nature 2004, 429, 629–635. [Google Scholar]
- Strassberger, V.; Fugmann, T.; Neri, D.; Roesli, C. Chemical proteomic and bioinformatic strategies for the identification and quantification of vascular antigens in cancer. J. Proteomics 2010, 73, 1954–1973. [Google Scholar] [CrossRef]
- Rybak, J.N.; Ettorre, A.; Kaissling, B.; Giavazzi, R.; Neri, D.; Elia, G. In vivo protein biotinylation for identification of organ-specific antigens accessible from the vasculature. Nat. Methods 2005, 2, 291–298. [Google Scholar]
- Borgia, B.; Roesli, C.; Fugmann, T.; Schliemann, C.; Cesca, M.; Neri, D.; Giavazzi, R. A proteomic approach for the identification of vascular markers of liver metastasis. Cancer Res. 2010, 70, 309–318. [Google Scholar]
- Frey, K.; Fiechter, M.; Schwager, K.; Belloni, B.; Barysch, M.J.; Neri, D.; Dummer, R. Different patterns of fibronectin and tenascin-C splice variants expression in primary and metastatic melanoma lesions. Exp. Dermatol. 2011, 20, 685–688. [Google Scholar] [CrossRef]
- Schliemann, C.; Roesli, C.; Kamada, H.; Borgia, B.; Fugmann, T.; Klapper, W.; Neri, D. In vivo biotinylation of the vasculature in B-cell lymphoma identifies BST-2 as a target for antibody-based therapy. Blood 2010, 115, 736–744. [Google Scholar]
- Seruga, B.; Zhang, H.; Bernstein, L.J.; Tannock, I.F. Cytokines and their relationship to the symptoms and outcome of cancer. Nat. Rev. Cancer 2008, 8, 887–899. [Google Scholar] [CrossRef]
- Douglas, M.R.; Morrison, K.E.; Salmon, M.; Buckley, C.D. Why does inflammation persist: A dominant role for the stromal microenvironment. Expert Rev. Mol. Med. 2002, 4, 1–18. [Google Scholar]
- Zamarron, B.F.; Chen, W. Dual roles of immune cells and their factors in cancer development and progression. Int. J. Biol. Sci. 2011, 7, 651–658. [Google Scholar] [CrossRef]
- McDermott, D.F.; Regan, M.M.; Atkins, M.B. Interleukin-2 therapy of metastatic renal cell carcinoma: Update of phase III trials. Clin. Genitourin. Cancer 2006, 5, 114–119. [Google Scholar] [CrossRef]
- Philip, P.A. Interleukin-2 in the treatment of malignant melanoma. Expert Opin. Investig. Drugs 1998, 7, 361–371. [Google Scholar] [CrossRef]
- Carnemolla, B.; Borsi, L.; Balza, E.; Castellani, P.; Meazza, R.; Berndt, A.; Ferrini, S.; Kosmehl, H.; Neri, D.; Zardi, L. Enhancement of the antitumor properties of interleukin-2 by its targeted delivery to the tumor blood vessel extracellular matrix. Blood 2002, 99, 1659–1665. [Google Scholar]
- Schliemann, C.; Palumbo, A.; Zuberbuhler, K.; Villa, A.; Kaspar, M.; Trachsel, E.; Klapper, W.; Menssen, H.D.; Neri, D. Complete eradication of human B-cell lymphoma xenografts using rituximab in combination with the immunocytokine L19-IL2. Blood 2009, 113, 2275–2283. [Google Scholar]
- Marlind, J.; Kaspar, M.; Trachsel, E.; Sommavilla, R.; Hindle, S.; Bacci, C.; Giovannoni, L.; Neri, D. Antibody-mediated delivery of interleukin-2 to the stroma of breast cancer strongly enhances the potency of chemotherapy. Clin. Cancer Res. 2008, 14, 6515–6524. [Google Scholar]
- King, D.M.; Albertini, M.R.; Schalch, H.; Hank, J.A.; Gan, J.; Surfus, J.; Mahvi, D.; Schiller, J.H.; Warner, T.; Kim, K.; et al. Phase I clinical trial of the immunocytokine EMD 273063 in melanoma patients. J. Clin. Oncol. 2004, 22, 4463–4473. [Google Scholar]
- Ribas, A.; Kirkwood, J.M.; Atkins, M.B.; Whiteside, T.L.; Gooding, W.; Kovar, A.; Gillies, S.D.; Kashala, O.; Morse, M.A. Phase I/II open-label study of the biologic effects of the interleukin-2 immunocytokine EMD 273063 (hu14.18-IL2) in patients with metastatic malignant melanom. J. Transl. Med. 2009, 7, 68. [Google Scholar]
- Osenga, K.L.; Hank, J.A.; Albertini, M.R.; Gan, J.; Sternberg, A.G.; Eickhoff, J.; Seeger, R.C.; Matthay, K.K.; Reynolds, C.P.; Twist, C.; et al. A phase I clinical trial of the hu14.18-IL2 (EMD 273063) as a treatment for children with refractory or recurrent neuroblastoma and melanoma: A study of the Children's Oncology Group. Clin. Cancer Res. 2006, 12, 1750–1759. [Google Scholar]
- Shusterman, S.; London, W.B.; Gillies, S.D.; Hank, J.A.; Voss, S.D.; Seeger, R.C.; Reynolds, C.P.; Kimball, J.; Albertini, M.R.; Wagner, B.; et al. Antitumor activity of hu14.18-IL2 in patients with relapsed/refractory neuroblastoma: A Children's Oncology Group (COG) phase II study. J. Clin. Oncol. 2010, 28, 4969–4975. [Google Scholar]
- Ko, Y.J.; Bubley, G.J.; Weber, R.; Redfern, C.; Gold, D.P.; Finke, L.; Kovar, A.; Dahl, T.; Gillies, S.D. Safety, pharmacokinetics, and biological pharmacodynamics of the immunocytokine EMD 273066 (huKS-IL2): Results of a phase I trial in patients with prostate cance. J. Immunother. 2004, 27, 232–239. [Google Scholar]
- Gillies, S.D.; Lan, Y.; Hettmann, T.; Brunkhorst, B.; Sun, Y.; Mueller, S.O.; Lo, K.M. A low-toxicity IL-2-based immunocytokine retains antitumor activity despite its high degree of IL-2 receptor selectivity. Clin. Cancer Res. 2011, 17, 3673–3685. [Google Scholar]
- Yang, J.C.; Sherry, R.M.; Steinberg, S.M.; Topalian, S.L.; Schwartzentruber, D.J.; Hwu, P.; Seipp, C.A.; Rogers-Freezer, L.; Morton, K.E.; White, D.E.; et al. Randomized study of high-dose and low-dose interleukin-2 in patients with metastatic renal cancer. J. Clin. Oncol. 2003, 21, 3127–3132. [Google Scholar]
- Rosenberg, S.A.; Yang, J.C.; White, D.E.; Steinberg, S.M. Durability of complete responses in patients with metastatic cancer treated with high-dose interleukin-2: Identification of the antigens mediating response. Ann. Surg. 1998, 228, 307–319. [Google Scholar]
- Atkins, M.B.; Robertson, M.J.; Gordon, M.; Lotze, M.T.; DeCoste, M.; DuBois, J.S.; Ritz, J.; Sandler, A.B.; Edington, H.D.; Garzone, P.D.; et al. Phase I evaluation of intravenous recombinant human interleukin 12 in patients with advanced malignancies. Clin. Cancer Res. 1997, 3, 409–417. [Google Scholar]
- Halin, C.; Rondini, S.; Nilsson, F.; Berndt, A.; Kosmehl, H.; Zardi, L.; Neri, D. Enhancement of the antitumor activity of interleukin-12 by targeted delivery to neovasculature. Nat. Biotechnol. 2002, 20, 264–269. [Google Scholar] [CrossRef]
- Li, J.; Hu, P.; Khawli, L.A.; Yun, A.; Epstein, A.L. chTNT-3/hu IL-12 fusion protein for the immunotherapy of experimental solid tumors. Hybrid. Hybridomics 2004, 23, 1–10. [Google Scholar] [CrossRef]
- Rudman, S.M.; Jameson, M.B.; McKeage, M.J.; Savage, P.; Jodrell, D.I.; Harries, M.; Acton, G.; Erlandsson, F.; Spicer, J.F. A phase 1 study of AS1409, a novel antibody-cytokine fusion protein, in patients with malignant melanoma or renal cell carcinoma. Clin. Cancer Res. 2011, 17, 1998–2005. [Google Scholar]
- Lejeune, F.J.; Lienard, D.; Matter, M.; Ruegg, C. Efficiency of recombinant human TNF in human cancer therapy. Cancer Immun. 2006, 6, 6. [Google Scholar]
- Borsi, L.; Balza, E.; Carnemolla, B.; Sassi, F.; Castellani, P.; Berndt, A.; Kosmehl, H.; Biro, A.; Siri, A.; Orecchia, P.; et al. Selective targeted delivery of TNFalpha to tumor blood vessels. Blood 2003, 102, 4384–4392. [Google Scholar]
- Balza, E.; Mortara, L.; Sassi, F.; Monteghirfo, S.; Carnemolla, B.; Castellani, P.; Neri, D.; Accolla, R.S.; Zardi, L.; Borsi, L. Targeted delivery of tumor necrosis factor-alpha to tumor vessels induces a therapeutic T cell-mediated immune response that protects the host against syngeneic tumors of different histologic origin. Clin. Cancer Res. 2006, 12, 2575–2582. [Google Scholar]
- Huhn, R.D.; Radwanski, E.; O'Connell, S.M.; Sturgill, M.G.; Clarke, L.; Cody, R.P.; Affrime, M.B.; Cutler, D.L. Pharmacokinetics and immunomodulatory properties of intravenously administered recombinant human interleukin-10 in healthy volunteers. Blood 1996, 87, 699–705. [Google Scholar]
- Rosenblum, I.Y.; Johnson, R.C.; Schmahai, T.J. Preclinical safety evaluation of recombinant human interleukin-10. Regul. Toxicol. Pharmacol. 2002, 35, 56–71. [Google Scholar] [CrossRef]
- Schwager, K.; Kaspar, M.; Bootz, F.; Marcolongo, R.; Paresce, E.; Neri, D.; Trachsel, E. Preclinical characterization of DEKAVIL (F8-IL10), a novel clinical-stage immunocytokine which inhibits the progression of collagen-induced arthritis. Arthritis Res. Ther. 2009, 11, R142. [Google Scholar] [CrossRef]
- Schwager, K.; Bootz, F.; Imesch, P.; Kaspar, M.; Trachsel, E.; Neri, D. The antibody-mediated targeted delivery of interleukin-10 inhibits endometriosis in a syngeneic mouse model. Hum. Reprod. 2011, 26, 2344–2352. [Google Scholar] [CrossRef]
- Trachsel, E.; Kaspar, M.; Bootz, F.; Detmar, M.; Neri, D. A human mAb specific to oncofetal fibronectin selectively targets chronic skin inflammation in vivo. J. Invest. Dermatol. 2007, 127, 881–886. [Google Scholar]
- Zitvogel, L.; Apetoh, L.; Ghiringhelli, F.; Kroemer, G. Immunological aspects of cancer chemotherapy. Nat. Rev. Immunol. 2008, 8, 59–73. [Google Scholar]
- Moschetta, M.; Pretto, F.; Berndt, A.; Galler, K.; Richter, P.; Bassi, A.; Oliva, P.; Micotti, E.; Valbusa, G.; Schwager, K.; et al. Paclitaxel Enhances Therapeutic Efficacy of the F8-IL2 Immunocytokine to EDA-Fibronectin-Positive Metastatic Human Melanoma Xenografts. Cancer Res. 2012, 72, 1814–1824. [Google Scholar] [CrossRef]
- Holden, S.A.; Lan, Y.; Pardo, A.M.; Wesolowski, J.S.; Gillies, S.D. Augmentation of antitumor activity of an antibody-interleukin 2 immunocytokine with chemotherapeutic agents. Clin. Cancer Res. 2001, 7, 2862–2869. [Google Scholar]
- Pedretti, M.; Verpelli, C.; Marlind, J.; Bertani, G.; Sala, C.; Neri, D.; Bello, L. Combination of temozolomide with immunocytokine F16-IL2 for the treatment of glioblastoma. Br. J. Cancer 2010, 103, 827–836. [Google Scholar] [CrossRef]
- Johnson, E.E.; Yamane, B.H.; Buhtoiarov, I.N.; Lum, H.D.; Rakhmilevich, A.L.; Mahvi, D.M.; Gillies, S.D.; Sondel, P.M. Radiofrequency ablation combined with KS-IL2 immunocytokine (EMD 273066) results in an enhanced antitumor effect against murine colon adenocarcinoma. Clin. Cancer Res. 2009, 15, 4875–4884. [Google Scholar]
- Hornick, J.L.; Khawli, L.A.; Hu, P.; Sharifi, J.; Khanna, C.; Epstein, A.L. Pretreatment with a monoclonal antibody/interleukin-2 fusion protein directed against DNA enhances the delivery of therapeutic molecules to solid tumors. Clin. Cancer Res. 1999, 5, 51–60. [Google Scholar]
- Liu, Z.; Smyth, F.E.; Renner, C.; Lee, F.T.; Oosterwijk, E.; Scott, A.M. Anti-renal cell carcinoma chimeric antibody G250: Cytokine enhancement of in vitro antibody-dependent cellular cytotoxicity. Cancer Immunol. Immunother. 2002, 51, 171–177. [Google Scholar] [CrossRef]
- Friedberg, J.W.; Neuberg, D.; Gribben, J.G.; Fisher, D.C.; Canning, C.; Koval, M.; Poor, C.M.; Green, L.M.; Daley, J.; Soiffer, R.; et al. Combination immunotherapy with rituximab and interleukin 2 in patients with relapsed or refractory follicular non-Hodgkin's lymphoma. Br. J. Haematol. 2002, 117, 828–834. [Google Scholar] [CrossRef]
- Frey, K.; Schliemann, C.; Schwager, K.; Giavazzi, R.; Johannsen, M.; Neri, D. The immunocytokine F8-IL2 improves the therapeutic performance of sunitinib in a mouse model of renal cell carcinoma. J. Urol. 2010, 184, 2540–2548. [Google Scholar] [CrossRef]
- Halin, C.; Gafner, V.; Villani, M.E.; Borsi, L.; Berndt, A.; Kosmehl, H.; Zardi, L.; Neri, D. Synergistic therapeutic effects of a tumor targeting antibody fragment, fused to interleukin 12 and to tumor necrosis factor alpha. Cancer Res. 2003, 63, 3202–3210. [Google Scholar]
- Gillies, S.D.; Lan, Y.; Brunkhorst, B.; Wong, W.K.; Li, Y.; Lo, K.M. Bi-functional cytokine fusion proteins for gene therapy and antibody-targeted treatment of cancer. Cancer Immunol. Immunother. 2002, 51, 449–460. [Google Scholar] [CrossRef]
- Connor, J.P.; Stupp, R.; Cristea, M.C.; Lewis, N.; Lewis, L.D.; Mattiacci, M.R.; Felder, M.; Stewart, S.; Henslee-Downey, J.; Neugebauer, R.; Komarnitsky, P.B. Phase IB trial of EMD 273066 (huKS-IL2) with cyclophosphamide in patients with EpCAM-positive advanced solid tumor. J Clin Oncol 2011, 29 (suppl; abstr 2556), 2011. [Google Scholar]
- De Braud, F.G.; Catania, C.; Onofri, A.; Pierantoni, C.; Cascinu, S.; Maur, M.; Masini, C.; Conte, P.F.; Giovannoni, L.; Tasciotti, A.; Lovato, V.; Neri, D.; Menssen, H.D. Combinations of the immunocytokine F16-IL2 with doxorubicin or with paclitaxel investigated in phase Ib studies in patients with advanced solid tumors. J Clin Oncol 2010, 28 (suppl; abstr e13017), 2010. [Google Scholar]
- Eigentler, T.K.; Weide, B.; de Braud, F.; Spitaleri, G.; Romanini, A.; Pflugfelder, A.; Gonzalez-Iglesias, R.; Tasciotti, A.; Giovannoni, L.; Schwager, K.; et al. A dose-escalation and signal-generating study of the immunocytokine L19-IL2 in combination with dacarbazine for the therapy of patients with metastatic melanoma. Clin. Cancer Res. 2011, 17, 7732–7742. [Google Scholar]
- Tijink, B.M.; Perk, L.R.; Budde, M.; Stigter-van Walsum, M.; Visser, G.W.; Kloet, R.W.; Dinkelborg, L.M.; Leemans, C.R.; Neri, D.; van Dongen, G.A. 124)I-L19-SIP for immuno-PET imaging of tumour vasculature and guidance of (131)I-L19-SIP radioimmunotherapy. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 1235–1244. [Google Scholar]
- Bassani-Sternberg, M.; Barnea, E.; Beer, I.; Avivi, I.; Katz, T.; Admon, A. Soluble plasma HLA peptidome as a potential source for cancer biomarkers. Proc. Natl. Acad. Sci. USA 2010, 107, 18769–18776. [Google Scholar] [CrossRef]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
MDPI and ACS Style
Gutbrodt, K.L.; Neri, D. Immunocytokines. Antibodies 2012, 1, 70-87. https://doi.org/10.3390/antib1010070
AMA Style
Gutbrodt KL, Neri D. Immunocytokines. Antibodies. 2012; 1(1):70-87. https://doi.org/10.3390/antib1010070
Chicago/Turabian StyleGutbrodt, Katrin L., and Dario Neri. 2012. "Immunocytokines" Antibodies 1, no. 1: 70-87. https://doi.org/10.3390/antib1010070