
Towards Effective and Efficient Patient-Specific Quality Assurance for Spot Scanning Proton Therapy

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
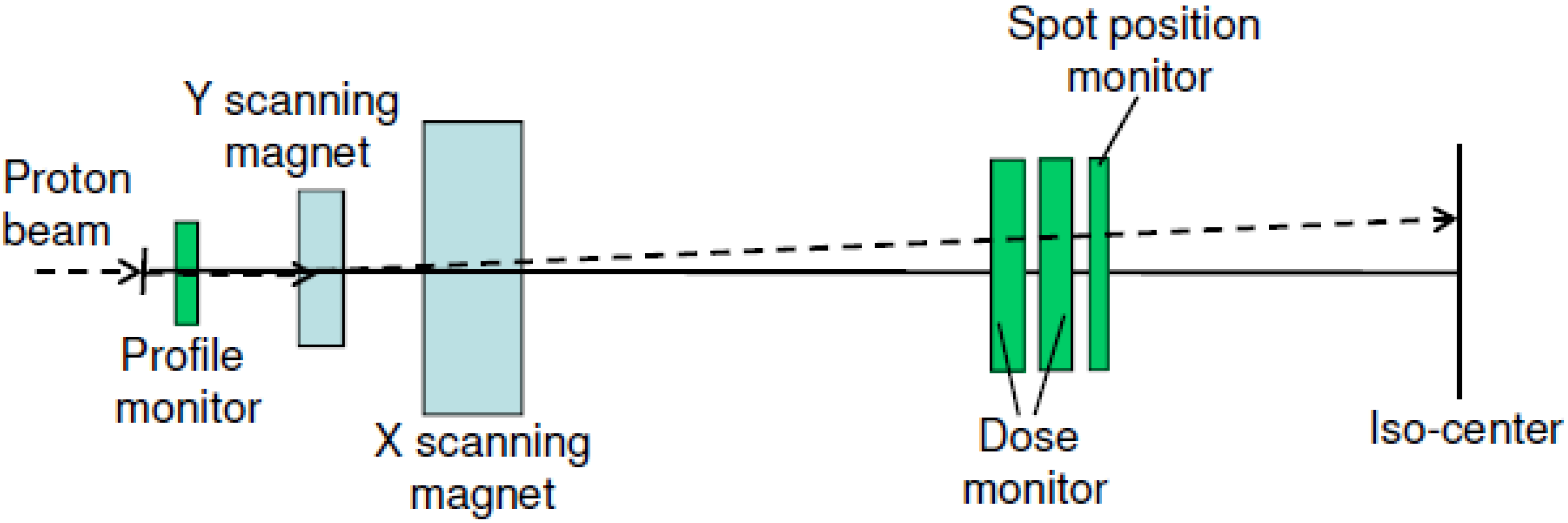
2. SSPT Beam Delivery System and TPS

3. Measurement-Based PSQA
3.1. Prostate Patients Treated with SFUD

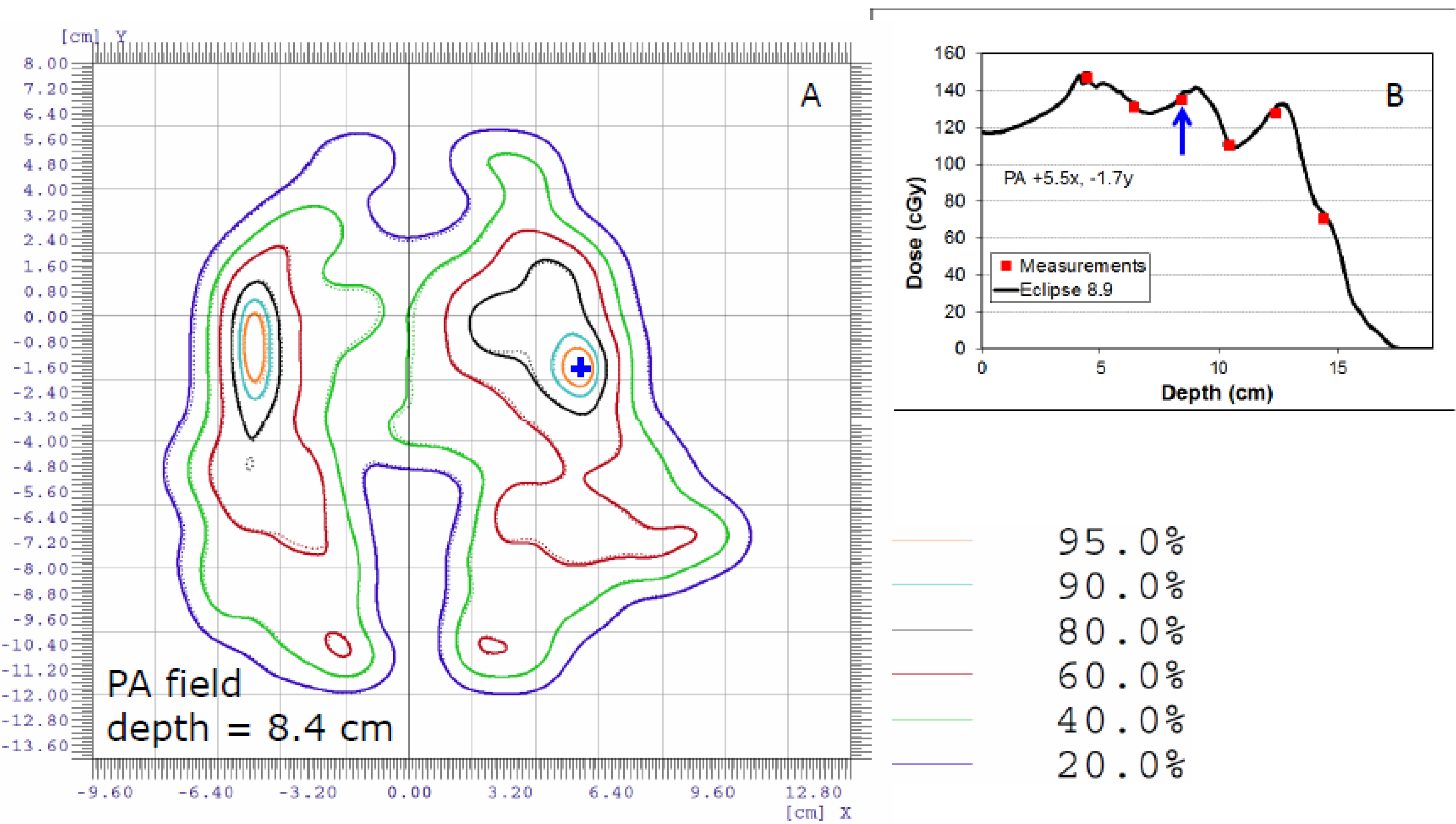
3.2. Patients with Target Volumes Outside the Pelvis: SFO and MFO Plans



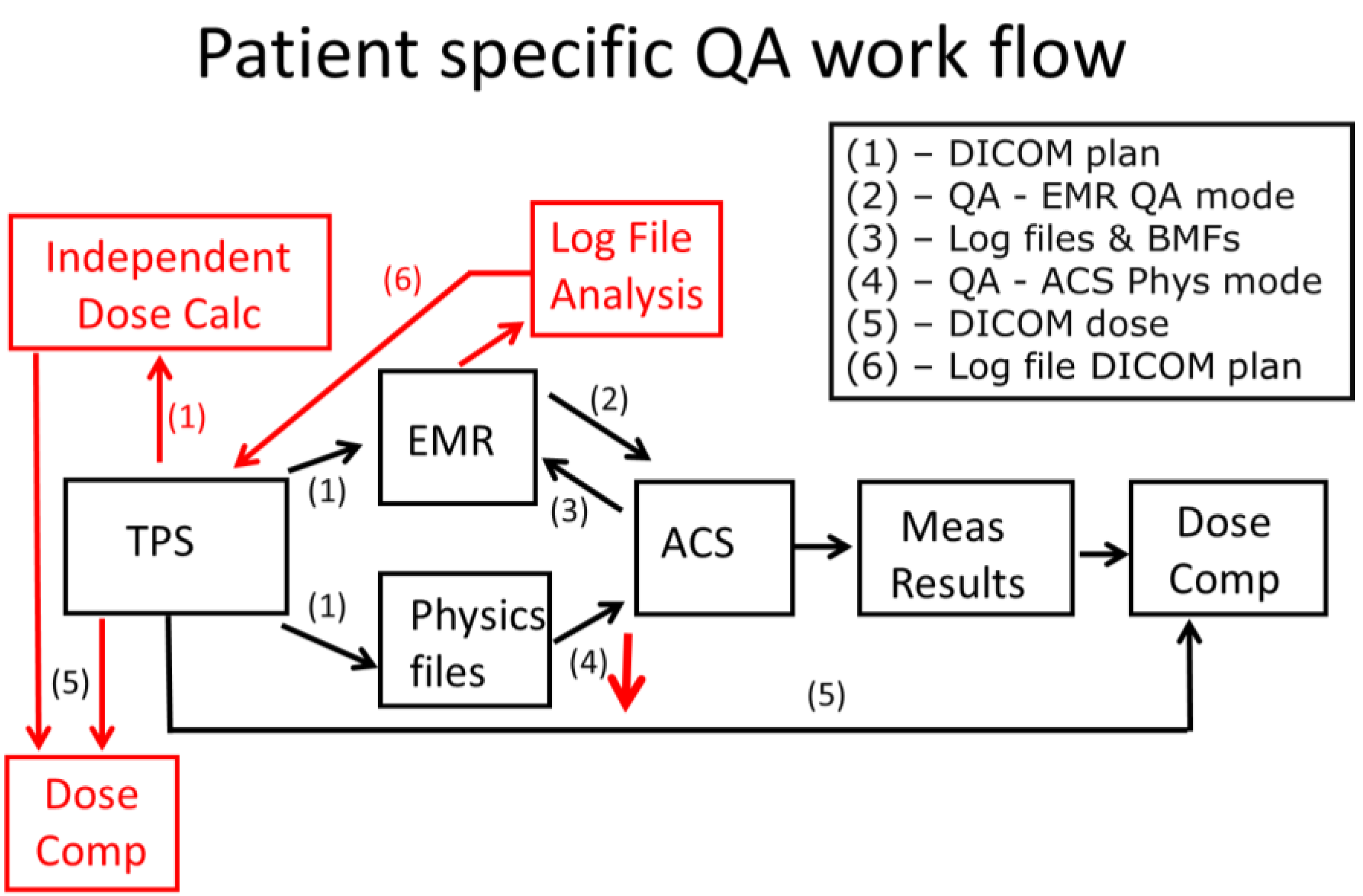
4. A Combined Approach for PSQA
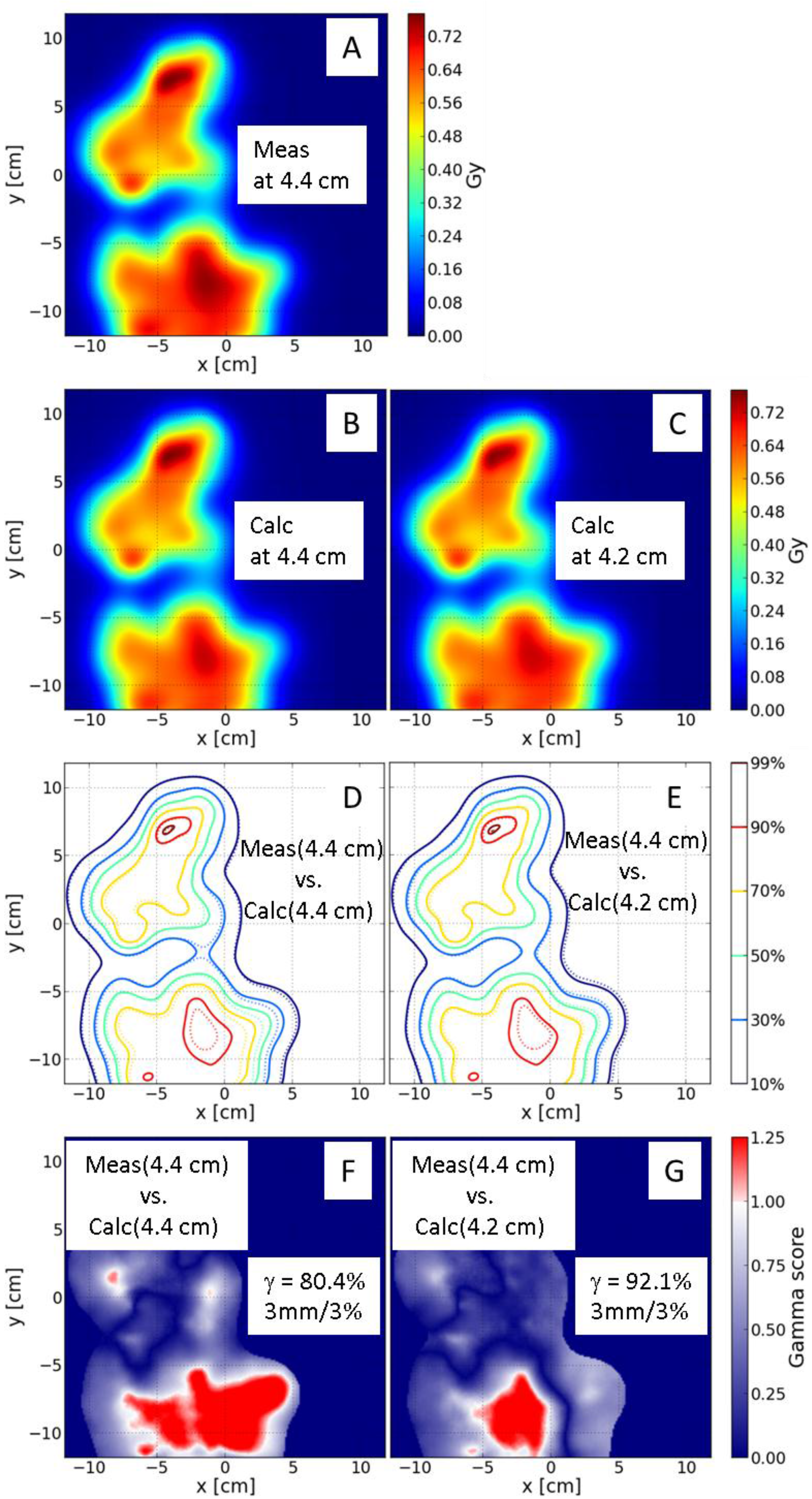
4.1. Independent Dose Calculation

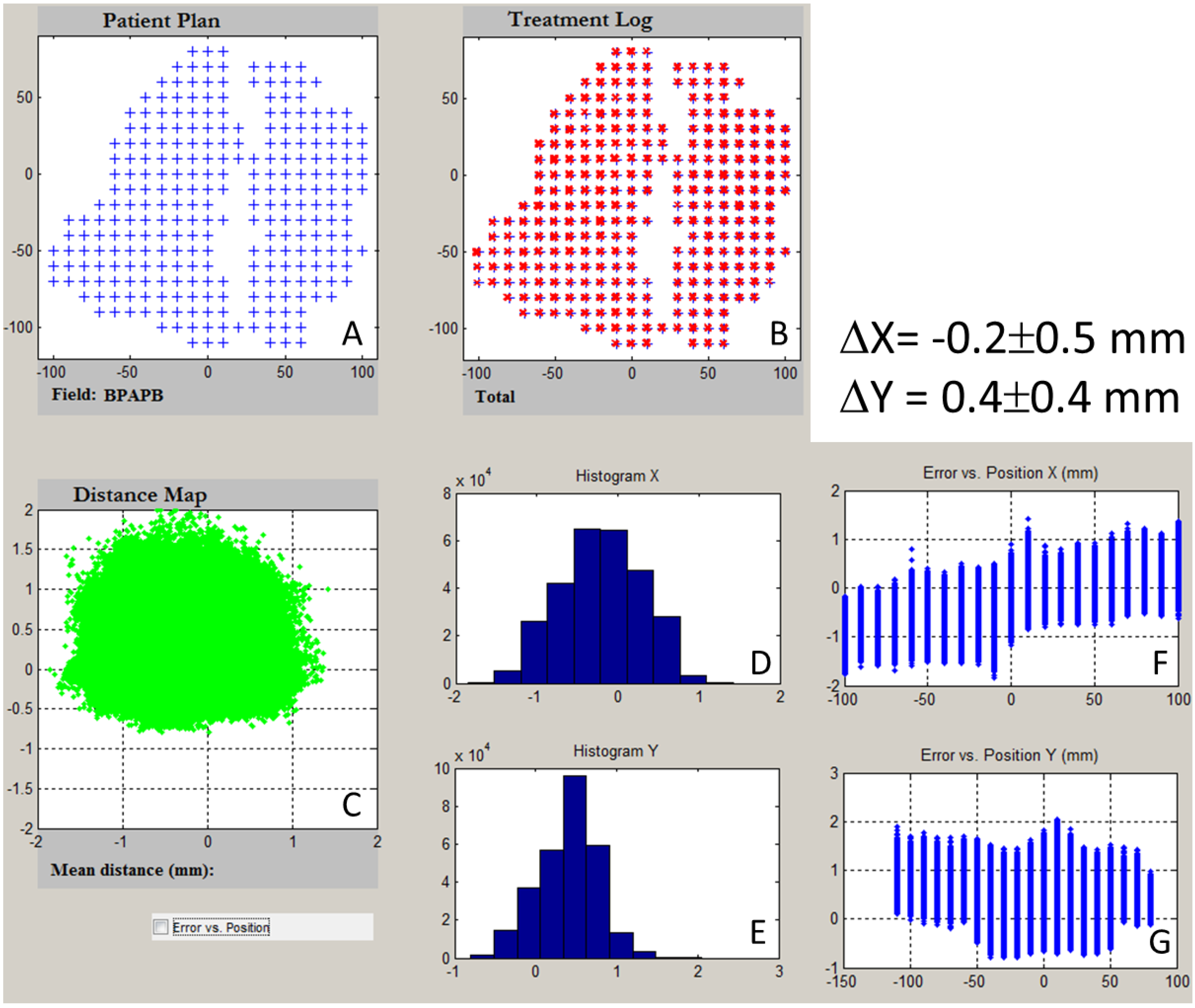
4.2. Analysis of Patient-Specific Treatment Delivery Log Files
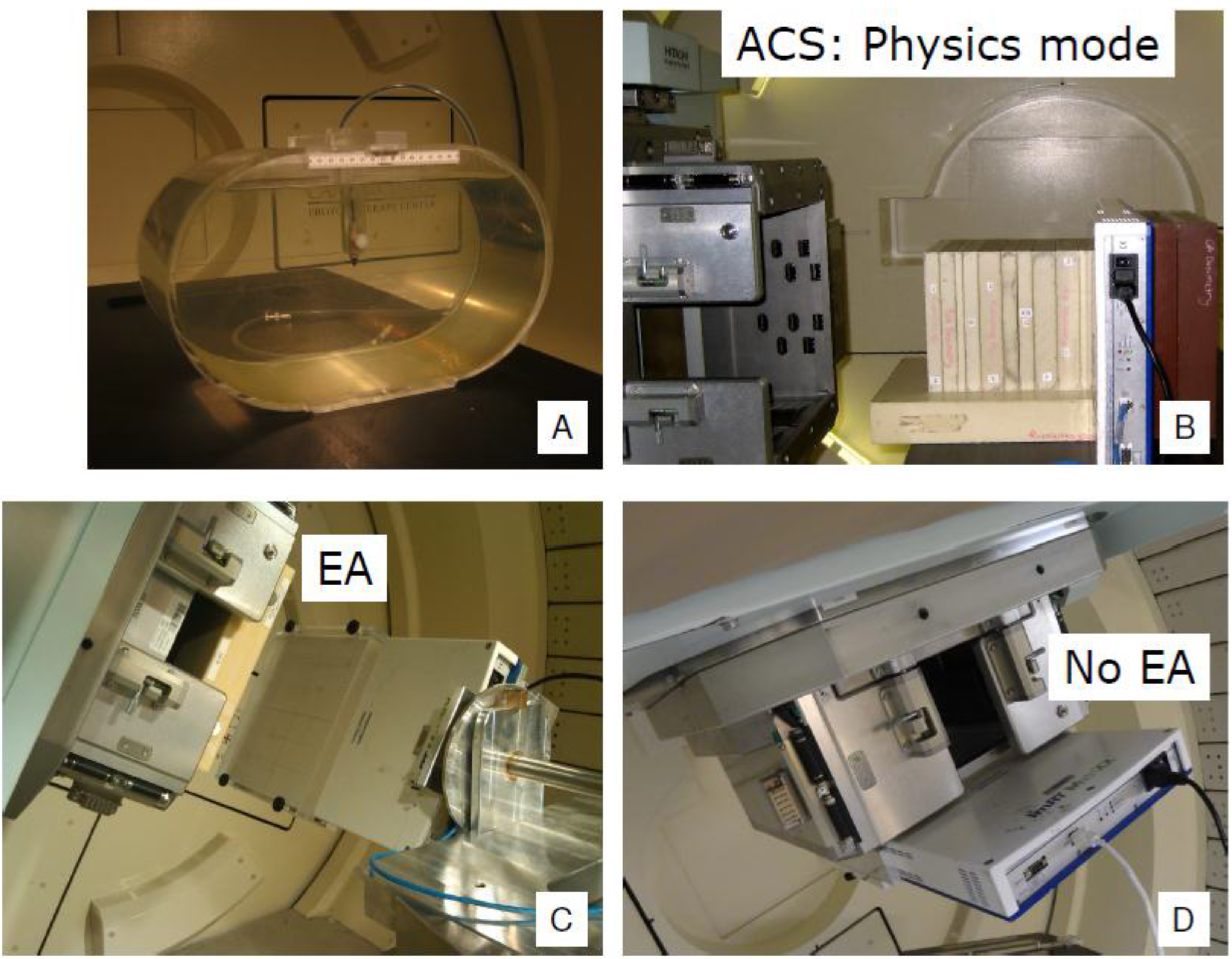
5. Use of the Treatment Room for PSQA

6. Discussion
7. Summary
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Delaney, T.F.; Kooy, H.M. Proton and Charged Particle Radiotherapy: Wolters Kluwer Lippincott; Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- International Commission on Radiation Units and Measurements. Prescribing, Recording, and Reporting Proton-Beam Therapy; ICRU: Washington, DC, USA, 2007. [Google Scholar]
- Pedroni, E.; Bacher, R.; Blattmann, H.; Bohringer, T.; Coray, A.; Lomax, A.; Lin, S.; Munkel, G.; Scheib, S.; Schneider, U.; et al. The 200-mev proton therapy project at the paul scherrer institute: Conceptual design and practical realization. Med. Phys. 1995, 22, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Gillin, M.T.; Sahoo, N.; Bues, M.; Ciangaru, G.; Sawakuchi, G.; Poenisch, F.; Arjomandy, B.; Martin, C.; Titt, U.; Suzuki, K.; et al. Commissioning of the discrete spot scanning proton beam delivery system at the University of Texas M. D. Anderson Cancer Center, Proton Therapy Center, Houston. Med. Phys. 2010, 37, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Lomax, A. Intensity modulation methods for proton radiotherapy. Phys. Med. Biol. 1999, 44, 185–205. [Google Scholar] [CrossRef] [PubMed]
- Lomax, A.J.; Bohringer, T.; Bolsi, A.; Coray, D.; Emert, F.; Goitein, G.; Jermann, M.; Lin, S.; Pedroni, E.; Rutz, H.; et al. Treatment planning and verification of proton therapy using spot scanning: Initial experiences. Med. Phys. 2004, 31, 3150–3157. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.R.; Poenisch, F.; Li, H.; Zhang, X.; Sahoo, N.; Wu, R.Y.; Li, X.; Lee, A.K.; Chang, E.L.; Choi, S.; et al. A single-field integrated boost treatment planning technique for spot scanning proton therapy. Radiat. Oncol. 2014. [Google Scholar] [CrossRef]
- Zhu, X.R.; Poenisch, F.; Song, X.; Johnson, J.L.; Ciangaru, G.; Taylor, M.B.; Lii, M.; Martin, C.; Arjomandy, B.; Lee, A.K.; et al. Patient-specific quality assurance for prostate cancer patients receiving spot scanning proton therapy using single-field uniform dose. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, T.; Inaniwa, T.; Hara, Y.; Mizushima, K.; Shirai, T.; Noda, K. Patient-specific QA and delivery verification of scanned ion beam at NIRS-HIMAC. Med. Phys. 2013. [Google Scholar] [CrossRef]
- Arjomandy, B.; Sahoo, N.; Ciangaru, G.; Zhu, R.; Song, X.; Gillin, M. Verification of patient-specific dose distributions in proton therapy using a commercial two-dimensional ion chamber array. Med. Phys. 2010, 37, 5831–5837. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, K.; Gillin, M.; Summers, P.A.; Dhanesar, S.; Gifford, K.A.; Buzdar, S.A. Quality assurance evaluation of spot scanning beam proton therapy with an anthropomorphic prostate phantom. Br. J. Radiol. 2013. [Google Scholar] [CrossRef]
- Jakel, O.; Hartmann, G.H.; Karger, C.P.; Heeg, P.; Rassow, J. Quality assurance for a treatment planning system in scanned ion beam therapy. Med. Phys. 2000, 27, 1588–1600. [Google Scholar] [CrossRef] [PubMed]
- Karger, C.P.; Jakel, O.; Hartmann, G.H. A system for three-dimensional dosimetric verification of treatment plans in intensity-modulated radiotherapy with heavy ions. Med. Phys. 1999, 26, 2125–2132. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Sahoo, N.; Poenisch, F.; Suzuki, K.; Li, Y.; Li, X.; Zhang, X.; Lee, A.K.; Gillin, M.T.; Zhu, X.R. Use of treatment log files in spot scanning proton therapy as part of patient-specific quality assurance. Med. Phys. 2013. [Google Scholar] [CrossRef]
- Mackin Dennis, L.Y.; Taylor Michael, B. Improving spot-scanning proton therapy patient specific quality assurance with hplusqa, a second-check dose calculation engine. Med. Phys. 2013. [Google Scholar] [CrossRef]
- Smith, A.; Gillin, M.; Bues, M.; Zhu, X.R.; Suzuki, K.; Mohan, R.; Woo, S.; Lee, A.; Komaki, R.; Cox, J.; et al. The M. D. Anderson proton therapy system. Med. Phys. 2009, 36, 4068–4083. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.R.; Poenisch, F.; Lii, M.; Sawakuchi, G.O.; Titt, U.; Bues, M.; Song, X.; Zhang, X.; Li, Y.; Ciangaru, G.; et al. Commissioning dose computation models for spot scanning proton beams in water for a commercially available treatment planning system. Med. Phys. 2013. [Google Scholar] [CrossRef]
- Bortfeld, T. An analytical approximation of the bragg curve for therapeutic proton beams. Med. Phys. 1997, 24, 2024–2033. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Liu, W.; Li, Y.; Li, X.; Quan, M.; Mohan, R.; Anand, A.; Sahoo, N.; Gillin, M.; Zhu, X.R. Parameterization of multiple bragg curves for scanning proton beams using simultaneous fitting of multiple curves. Phys. Med. Biol. 2011, 56, 7725–7735. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhu, R.X.; Sahoo, N.; Anand, A.; Zhang, X. Beyond gaussians: A study of single-spot modeling for scanning proton dose calculation. Phys. Med. Biol. 2012, 57, 983–997. [Google Scholar] [CrossRef] [PubMed]
- Mackin, D.; Zhu, X.R.; Poenisch, F.; Li, H.; Sahoo, N.; Kerr, M.; Holmes, C.; Li, Y.; Lii, M.; Wu, R.; et al. Spot-scanning proton therapy patient-specific quality assurance: Results from 309 treatment plans. Int. J. Part. Ther. 2014, 1, 711–720. [Google Scholar] [CrossRef]
- Archambault, L.; Poenisch, F.; Sahoo, N.; Robertson, D.; Lee, A.; Gillin, M.T.; Mohan, R.; Beddar, S. Verification of proton range, position, and intensity in impt with a 3D liquid scintillator detector system. Med. Phys. 2012, 39, 1239–1246. [Google Scholar] [CrossRef] [PubMed]
- Robertson, D.; Mirkovic, D.; Sahoo, N.; Beddar, S. Quenching correction for volumetric scintillation dosimetry of proton beams. Phys. Med. Biol. 2013, 58, 261–273. [Google Scholar] [CrossRef] [PubMed]
- Kroll, F.; Pawelke, J.; Karsch, L. Preliminary investigations on the determination of three-dimensional dose distributions using scintillator blocks and optical tomography. Med. Phys. 2013. [Google Scholar] [CrossRef]
- Gorjiara, T.; Kuncic, Z.; Doran, S.; Adamovics, J.; Baldock, C. Water and tissue equivalence of a new presage® formulation for 3D proton beam dosimetry: A Monte Carlo study. Med. Phys. 2012, 39, 7071–7079. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Newton, J.; Oldham, M.; Das, I.J.; Cheng, C.W.; Adamovics, J. Feasibility of using presage® for relative 3D dosimetry of small proton fields. Phys. Med. Biol. 2012, 57, N431–N443. [Google Scholar] [CrossRef] [PubMed]
- Lopatiuk-Tirpak, O.; Su, Z.; Li, Z.; Zeidan, O.A.; Meeks, S.L.; Maryanski, M.J. Direct response to proton beam linear energy transfer (LET) in a novel polymer gel dosimeter formulation. Technol. Cancer Res. Treat. 2012, 11, 441–445. [Google Scholar] [PubMed]
- Zeidan, O.A.; Sriprisan, S.I.; Lopatiuk-Tirpak, O.; Kupelian, P.A.; Meeks, S.L.; Hsi, W.C.; Li, Z.; Palta, J.R.; Maryanski, M.J. Dosimetric evaluation of a novel polymer gel dosimeter for proton therapy. Med. Phys. 2010, 37, 2145–2152. [Google Scholar] [CrossRef] [PubMed]
- Anjum, M.N.; Parker, W.; Ruo, R.; Aldahlawi, I.; Afzal, M. IMRT quality assurance using a second treatment planning system. Med. Dosim. 2010, 35, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Arumugam, S.; Xing, A.; Goozee, G.; Holloway, L. Independent calculation-based verification of IMRT plans using a 3D dose-calculation engine. Med. Dosim. 2013, 38, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Xing, L.; Nath, R. Independent monitor unit calculation for intensity modulated radiotherapy using the mimic multileaf collimator. Med. Phys. 2002, 29, 2041–2051. [Google Scholar] [CrossRef] [PubMed]
- Georg, D.; Stock, M.; Kroupa, B.; Olofsson, J.; Nyholm, T.; Ahnesjo, A.; Karlsson, M. Patient-specific IMRT verification using independent fluence-based dose calculation software: Experimental benchmarking and initial clinical experience. Phys. Med. Biol. 2007, 52, 4981–4992. [Google Scholar] [CrossRef] [PubMed]
- Goetzfried, T.; Rickhey, M.; Treutwein, M.; Koelbl, O.; Bogner, L. Monte carlo simulations to replace film dosimetry in IMRT verification. Z. Med. Phys. 2011, 21, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Pawlicki, T.; Yoo, S.; Court, L.E.; McMillan, S.K.; Rice, R.K.; Russell, J.D.; Pacyniak, J.M.; Woo, M.K.; Basran, P.S.; Shoales, J.; et al. Moving from IMRT QA measurements toward independent computer calculations using control charts. Radiother. Oncol. 2008, 89, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Pisaturo, O.; Moeckli, R.; Mirimanoff, R.O.; Bochud, F.O. A monte carlo-based procedure for independent monitor unit calculation in IMRT treatment plans. Phys. Med. Biol. 2009, 54, 4299–4310. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Xing, L.; Li, J.G.; Palta, J.; Chen, Y.; Luxton, G.; Boyer, A. Independent dosimetric calculation with inclusion of head scatter and mlc transmission for IMRT. Med. Phys. 2003, 30, 2937–2947. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Vazquez, L.A.; Shi, C.; Papanikolaou, N. Sensitivity study to evaluate the dosimetric impact of off-axis ratio profiles misalignment on tomotherapy second dose validation. Technol. Cancer Res. Treat. 2010, 9, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; Lee, L.; Liu, W.; Chu, K.; Mok, E.; Luxton, G.; Le, Q.T.; Xing, L. Dose reconstruction for volumetric modulated arc therapy (VMAT) using cone-beam CT and dynamic log files. Phys. Med. Biol. 2010, 55, 3597–3610. [Google Scholar] [CrossRef] [PubMed]
- Visser, R.; Wauben, D.J.; de Groot, M.; Godart, J.; Langendijk, J.A.; van’t Veld, A.A.; Korevaar, E.W. Efficient and reliable 3D dose quality assurance for IMRT by combining independent dose calculations with measurements. Med. Phys. 2013. [Google Scholar] [CrossRef]
- Agnew, C.E.; King, R.B.; Hounsell, A.R.; McGarry, C.K. Implementation of phantom-less IMRT delivery verification using varian dynalog files and R/V output. Phys. Med. Biol. 2012, 57, 6761–6777. [Google Scholar] [CrossRef] [PubMed]
- Dinesh Kumar, M.; Thirumavalavan, N.; Venugopal Krishna, D.; Babaiah, M. QA of intensity-modulated beams using dynamic mlc log files. J. Med. Phys. 2006, 31, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Li, J.G.; Dempsey, J.F.; Ding, L.; Liu, C.; Palta, J.R. Validation of dynamic mlc-controller log files using a two-dimensional diode array. Med. Phys. 2003, 30, 799–805. [Google Scholar] [CrossRef] [PubMed]
- Litzenberg, D.W.; Moran, J.M.; Fraass, B.A. Verification of dynamic and segmental IMRT delivery by dynamic log file analysis. J. Appl. Clin. Med. Phys. Am. Coll. Med. Phys. 2002, 3, 63–72. [Google Scholar] [CrossRef]
- Luo, W.; Li, J.; Price, R.A., Jr.; Chen, L.; Yang, J.; Fan, J.; Chen, Z.; McNeeley, S.; Xu, X.; Ma, C.M. Monte carlo based IMRT dose verification using MLC log files and R/V outputs. Med. Phys. 2006, 33, 2557–2564. [Google Scholar] [CrossRef] [PubMed]
- Okumura, M.; Obata, Y.; Shimomura, K.; Tamura, M.; Nishimura, Y. The effect of gantry and collimator angles on leaf limited velocity and position in dynamic multileaf collimator intensity-modulated radiation therapy. Phys. Med. Biol. 2010, 55, 3101–3113. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.; Rangaraj, D.; Boddu, S.; Goddu, M.; Yang, D.; Palaniswaamy, G.; Yaddanapudi, S.; Wooten, O.; Mutic, S. Evaluation of the efficiency and effectiveness of independent dose calculation followed by machine log file analysis against conventional measurement based IMRT QA. J. Appl. Clin. Med. Phys. Am. Coll. Med. Phys. 2012. [Google Scholar] [CrossRef]
- Teke, T.; Bergman, A.M.; Kwa, W.; Gill, B.; Duzenli, C.; Popescu, I.A. Monte carlo based, patient-specific rapidarc QA using linac log files. Med. Phys. 2010, 37, 116–123. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, X.R.; Li, Y.; Mackin, D.; Li, H.; Poenisch, F.; Lee, A.K.; Mahajan, A.; Frank, S.J.; Gillin, M.T.; Sahoo, N.; et al. Towards Effective and Efficient Patient-Specific Quality Assurance for Spot Scanning Proton Therapy. Cancers 2015, 7, 631-647. https://doi.org/10.3390/cancers7020631
Zhu XR, Li Y, Mackin D, Li H, Poenisch F, Lee AK, Mahajan A, Frank SJ, Gillin MT, Sahoo N, et al. Towards Effective and Efficient Patient-Specific Quality Assurance for Spot Scanning Proton Therapy. Cancers. 2015; 7(2):631-647. https://doi.org/10.3390/cancers7020631
Chicago/Turabian StyleZhu, X. Ronald., Yupeng Li, Dennis Mackin, Heng Li, Falk Poenisch, Andrew K. Lee, Anita Mahajan, Steven J. Frank, Michael T. Gillin, Narayan Sahoo, and et al. 2015. "Towards Effective and Efficient Patient-Specific Quality Assurance for Spot Scanning Proton Therapy" Cancers 7, no. 2: 631-647. https://doi.org/10.3390/cancers7020631