The Potential Use of Electrochemotherapy in the Treatment of Uveal Melanoma: In Vitro Results in 3D Tumor Cultures and In Vivo Results in a Chick Embryo Model

 ,
, 
 and
and
Abstract
1. Introduction
2. Results
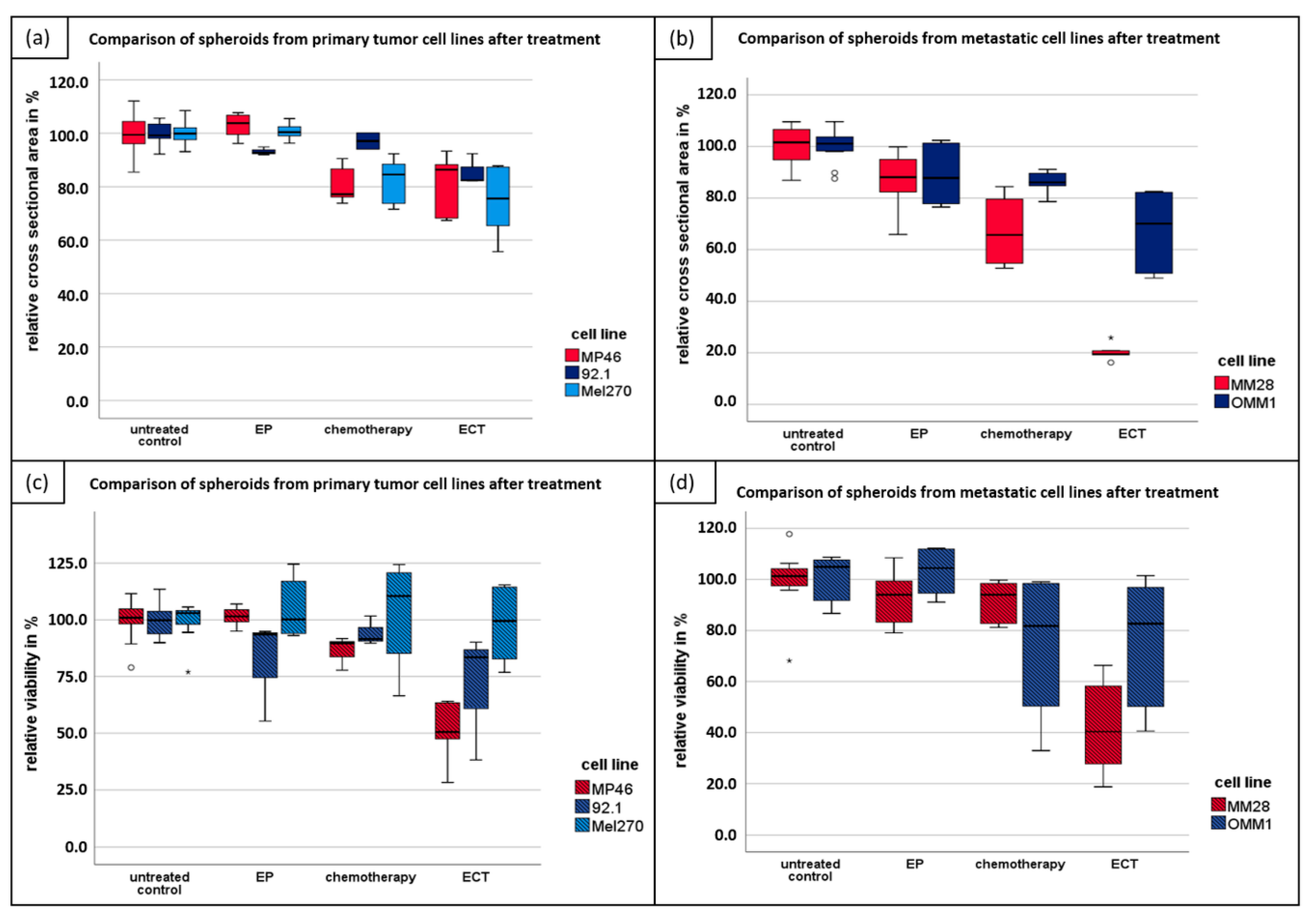
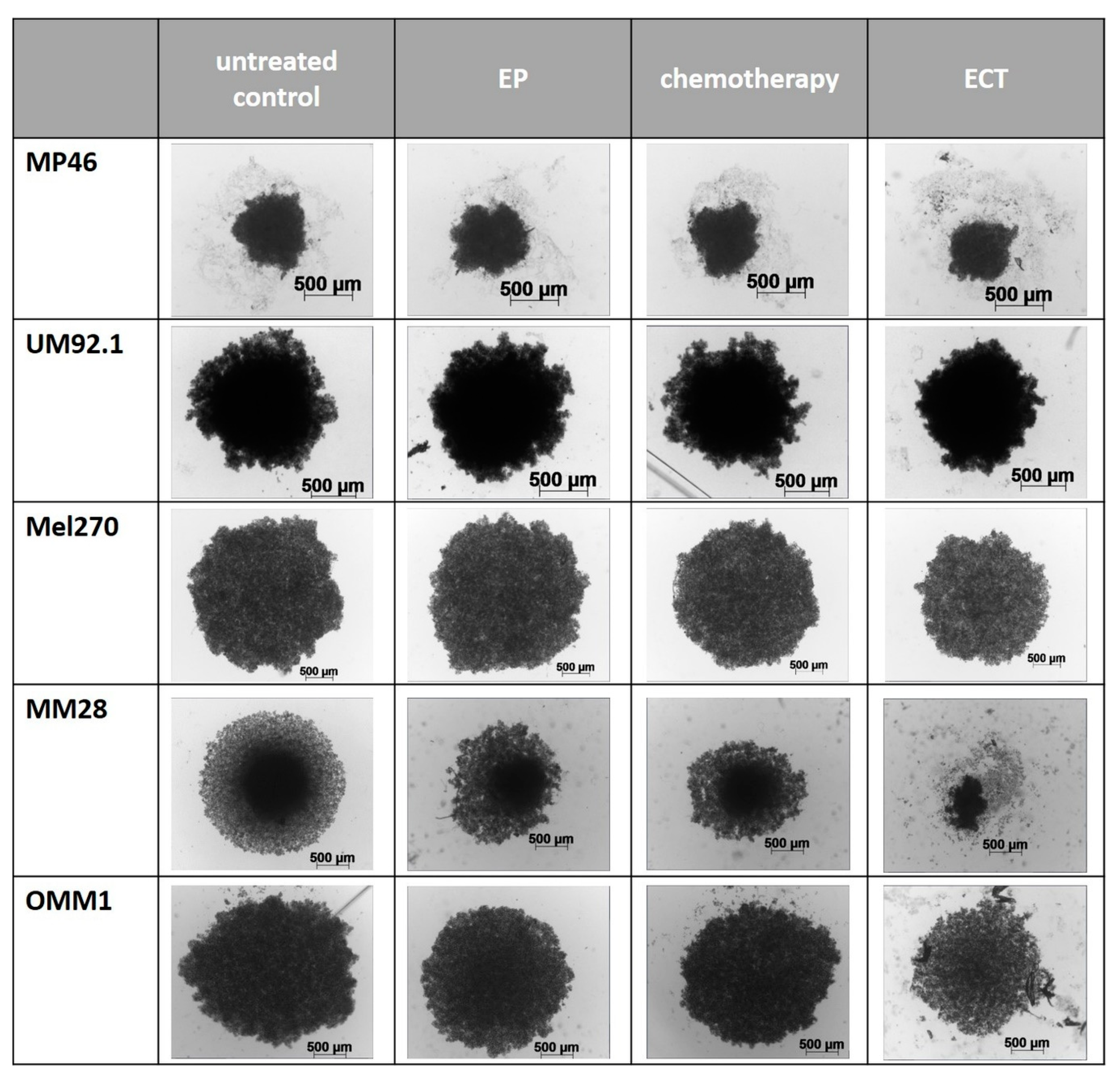
2.1. ECT of 3D Spheroids
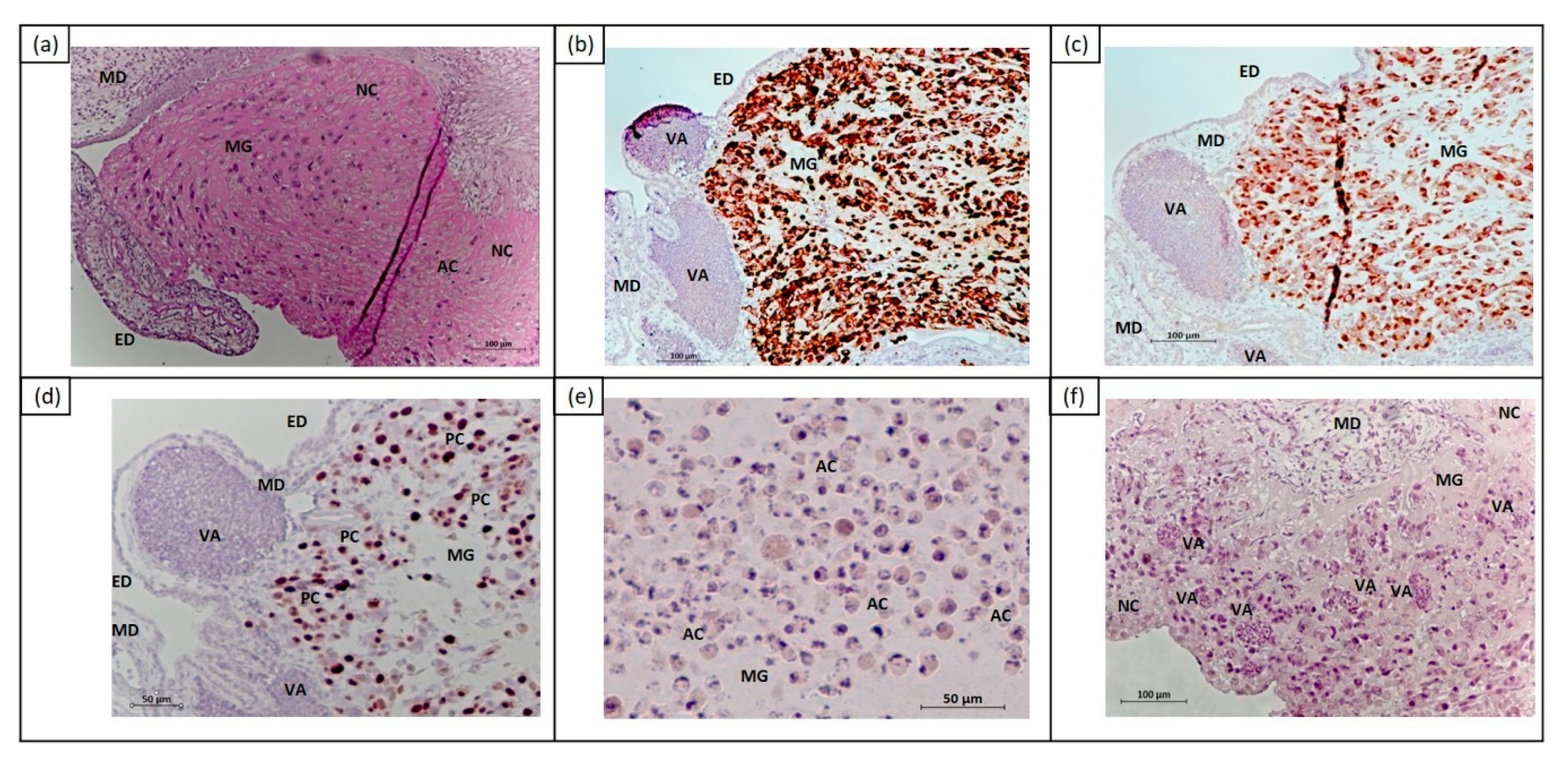
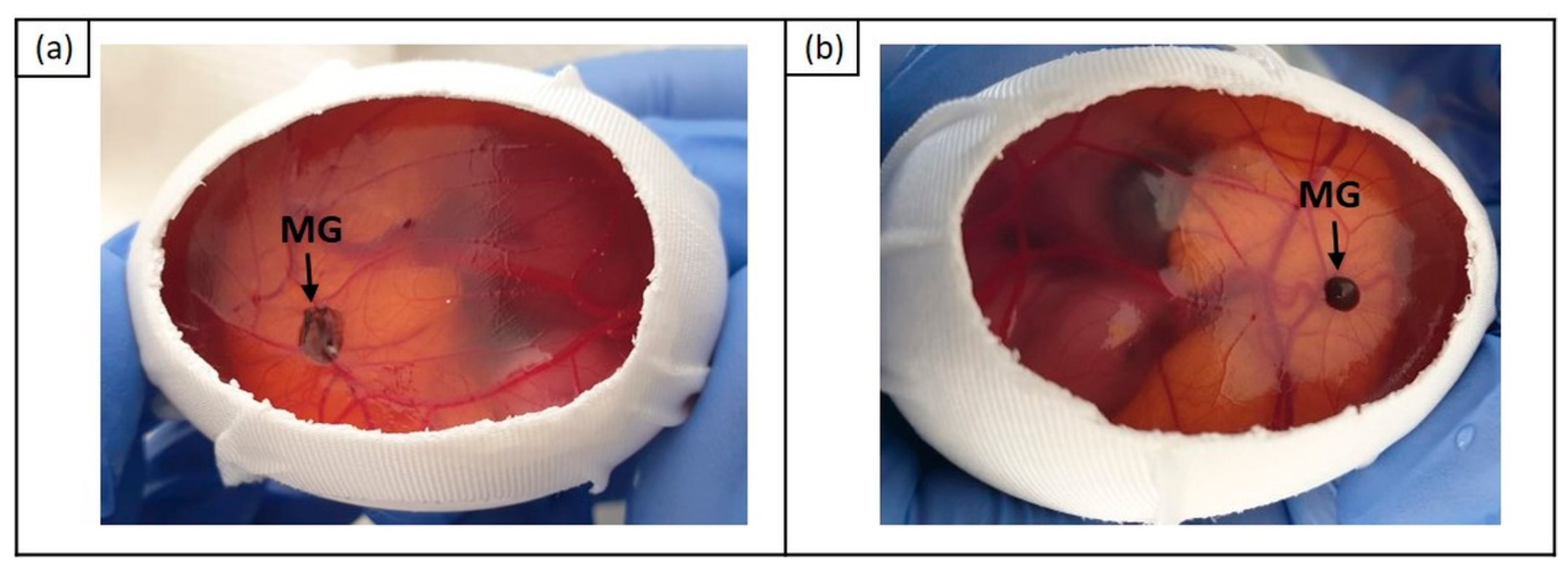
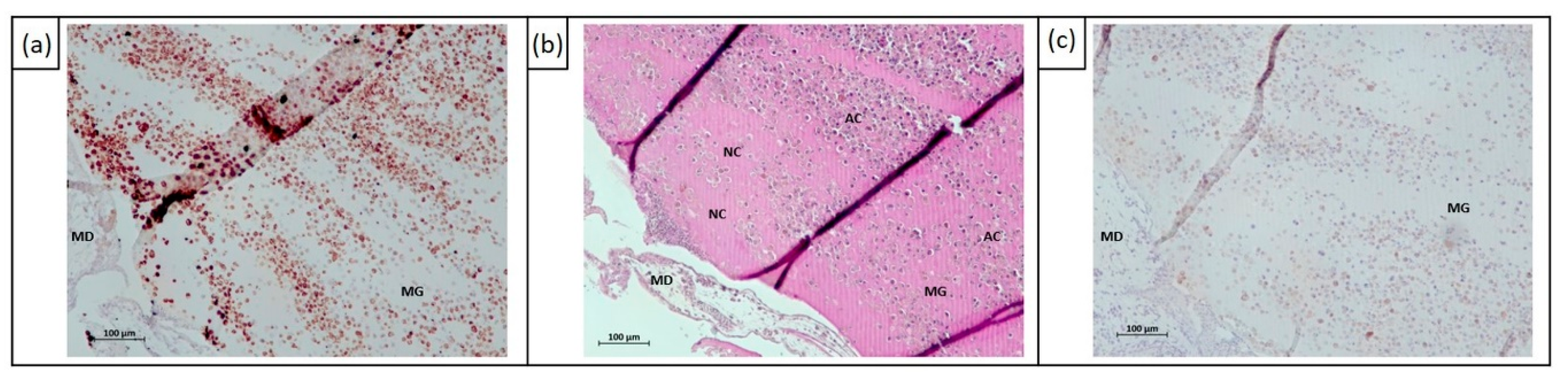
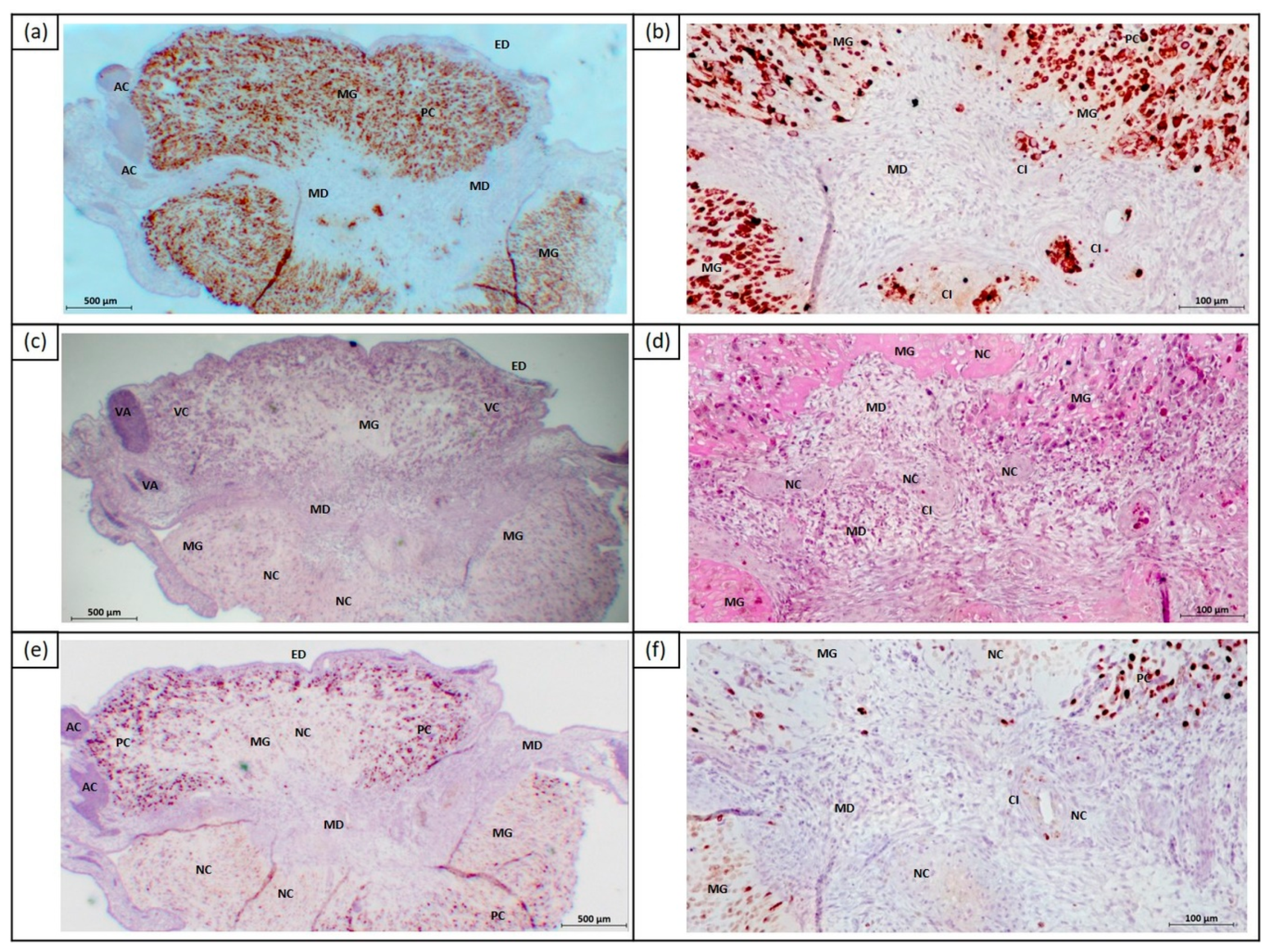
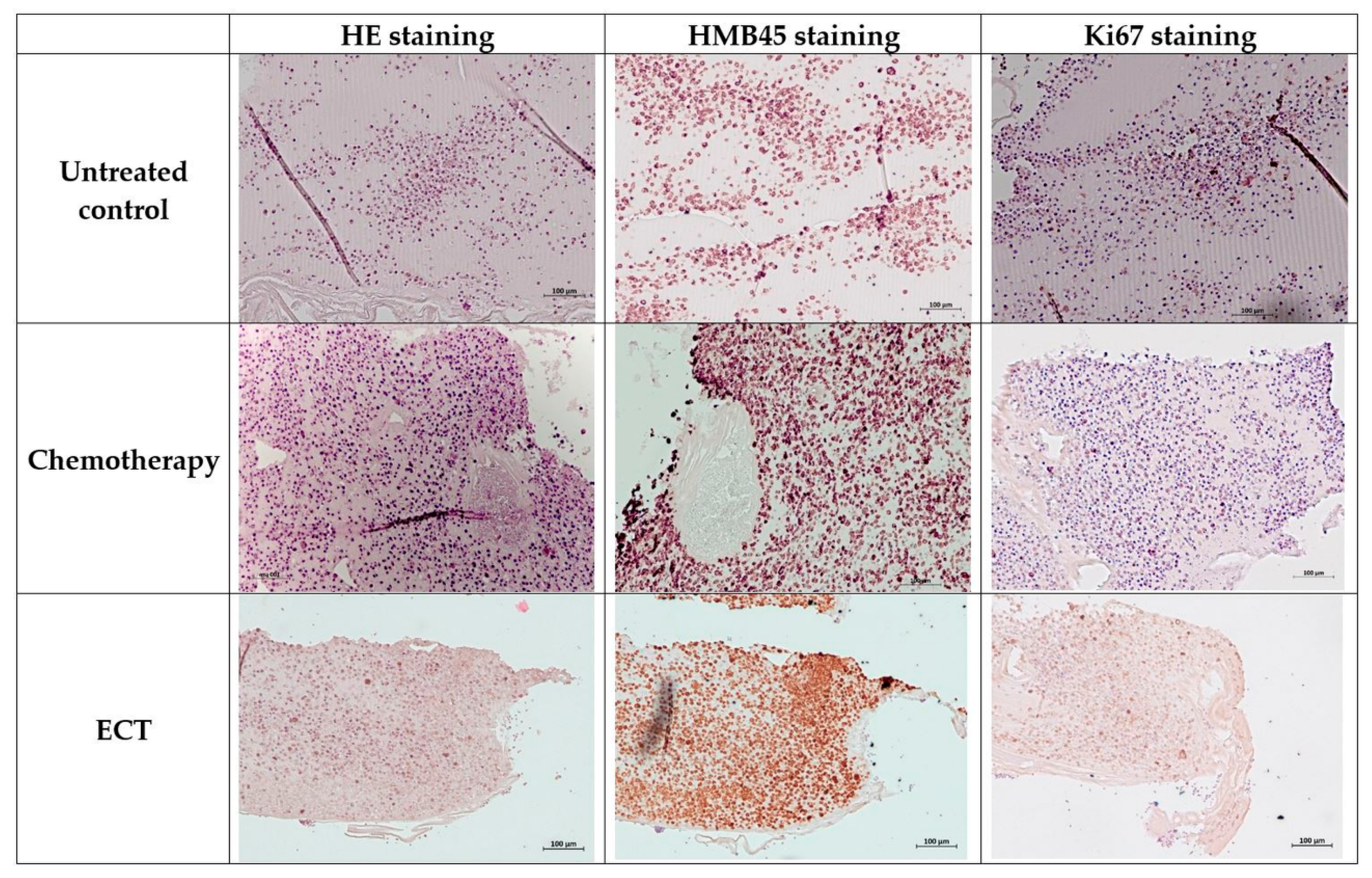
2.2. In Vivo Effects of ECT on Uveal Melanoma Cells Using Chick Embryo Chorioallantoic Membrane (CAM) Assay
3. Discussion
4. Materials and Methods
4.1. Culture of Uveal Melanoma Cell Lines
4.2. Treatment of Spheroids
4.3. Determination of Spheroid Growth
4.4. Determination of Spheroid Viability
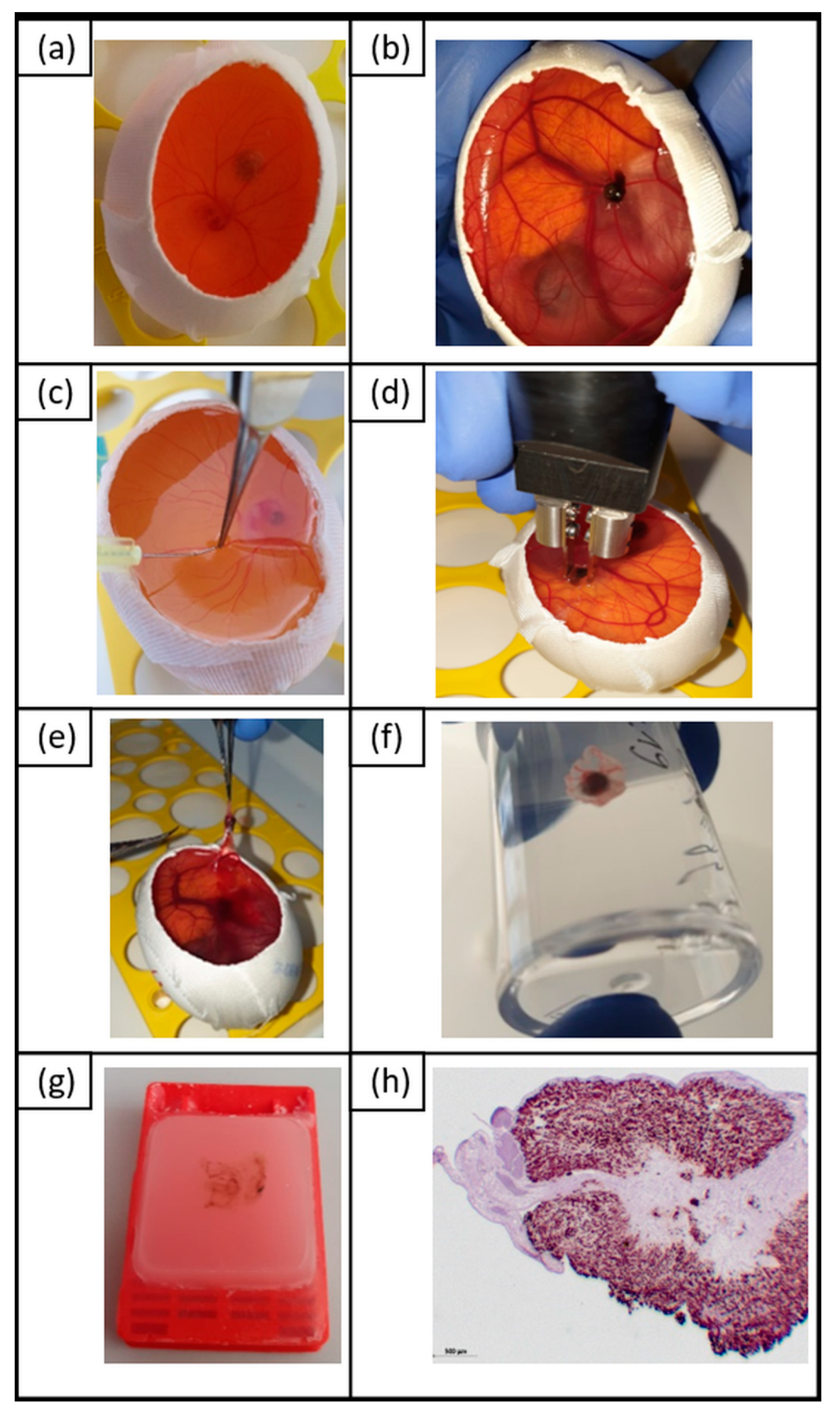
4.5. In Vivo Chick Embryo Chorioallantoic Membrane Assay (CAM) Assay as a Model to Investigate Tumor Growth and Viability after ECT
- (A)
- 750 V/cm pulse strength or
- (B)
- 1000 V/cm pulse strength.
4.6. Immunohistochemistry
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kaliki, S.; Shields, C.L. Uveal Melanoma: Relatively Rare but Deadly Cancer. Eye 2017, 31, 241–257. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.D.; Bergman, L.; Seregard, S. Uveal Melanoma: Epidemiologic Aspects. Ophthalmol. Clin. North. Am. 2005, 18, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Shields, C.L.; Furuta, M.; Thangappan, A.; Nagori, S.; Mashayekhi, A.; Lally, D.R.; Kelly, C.C.; Rudich, D.S.; Nagori, A.V.; Wakade, O.A.; et al. Metastasis of Uveal Melanoma Millimeter-by-Millimeter in 8033 Consecutive Eyes. Arch. Ophthalmol. 2009, 127, 989–998. [Google Scholar] [CrossRef] [PubMed]
- Weis, E.; Shah, C.P.; Lajous, M.; Shields, J.A.; Shields, C.L. The Association of Cutaneous and Iris Nevi with Uveal Melanoma: A Meta-Analysis. Ophthalmology 2009, 116, 536–543.e2. [Google Scholar] [CrossRef] [PubMed]
- Coupland, S.E.; Lake, S.L.; Zeschnigk, M.; Damato, B.E. Molecular Pathology of Uveal Melanoma. Eye 2013, 27, 230–242. [Google Scholar] [CrossRef] [PubMed]
- Shain, A.H.; Bagger, M.M.; Yu, R.; Chang, D.; Liu, S.; Vemula, S.; Weier, J.F.; Wadt, K.; Heegaard, S.; Bastian, B.C.; et al. The Genetic Evolution of Metastatic Uveal Melanoma. Nat. Genet. 2019, 51, 1123–1130. [Google Scholar] [CrossRef]
- Robertson, A.G.; Shih, J.; Yau, C.; Gibb, E.A.; Oba, J.; Mungall, K.L.; Hess, J.M.; Uzunangelov, V.; Walter, V.; Danilova, L.; et al. Integrative Analysis Identifies Four Molecular and Clinical Subsets in Uveal Melanoma. Cancer Cell 2018, 33, 151. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Manson, D.K.; Marr, B.P.; Carvajal, R.D. Treatment of Uveal Melanoma: Where Are We Now? Ther. Adv. Med. Oncol. 2018, 10, 1758834018757175. [Google Scholar] [CrossRef]
- Gothelf, A.; Mir, L.M.; Gehl, J. Electrochemotherapy: Results of Cancer Treatment Using Enhanced Delivery of Bleomycin by Electroporation. Cancer Treat. Rev. 2003, 29, 371–387. [Google Scholar] [CrossRef]
- Marty, M.; Sersa, G.; Garbay, J.R.; Gehl, J.; Collins, C.G.; Snoj, M.; Billard, V.; Geertsen, P.F.; Larkin, J.O.; Miklavcic, D.; et al. Electrochemotherapy - an Easy, Highly Effective and Safe Treatment of Cutaneous and Subcutaneous Metastases: Results of Esope (European Standard Operating Procedures of Electrochemotherapy) Study. EJC Suppl. 2006, 4, 3–13. [Google Scholar] [CrossRef]
- Edhemovic, I.; Brecelj, E.; Gasljevic, G.; Marolt Music, M.; Gorjup, V.; Mali, B.; Jarm, T.; Kos, B.; Pavliha, D.; Grcar Kuzmanov, B.; et al. Intraoperative Electrochemotherapy of Colorectal Liver Metastases. J. Surg. Oncol. 2014, 110, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Kis, E.G.; Baltas, E.; Ocsai, H.; Vass, A.; Nemeth, I.B.; Varga, E.; Olah, J.; Kemeny, L.; Toth-Molnar, E. Electrochemotherapy in the Treatment of Locally Advanced or Recurrent Eyelid-Periocular Basal Cell Carcinomas. Sci. Rep. 2019, 9, 4285. [Google Scholar] [CrossRef] [PubMed]
- Jaroszeski, M.J.; Dang, V.; Pottinger, C.; Hickey, J.; Gilbert, R.; Heller, R. Toxicity of Anticancer Agents Mediated by Electroporation in Vitro. Anticancer Drugs 2000, 11, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Probst, U.; Fuhrmann, I.; Beyer, L.; Wiggermann, P. Electrochemotherapy as a New Modality in Interventional Oncology: A Review. Technol. Cancer Res. Treat. 2018, 17, 1533033818785329. [Google Scholar] [CrossRef] [PubMed]
- Fiorentzis, M.; Kalirai, H.; Katopodis, P.; Seitz, B.; Viestenz, A.; Coupland, S.E. Electrochemotherapy with Bleomycin and Cisplatin Enhances Cytotoxicity in Primary and Metastatic Uveal Melanoma Cell Lines in Vitro. Neoplasma 2018, 65, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Brun, P.; Dettin, M.; Campana, L.G.; Dughiero, F.; Sgarbossa, P.; Bernardello, C.; Tosi, A.L.; Zamuner, A.; Sieni, E. Cell-Seeded 3d Scaffolds as in Vitro Models for Electroporation. Bioelectrochemistry 2019, 125, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Ravi, M.; Ramesh, A.; Pattabhi, A. Contributions of 3d Cell Cultures for Cancer Research. J. Cell Physiol. 2017, 232, 2679–2697. [Google Scholar] [CrossRef] [PubMed]
- Stei, M.M.; Loeffler, K.U.; Holz, F.G.; Herwig, M.C. Animal Models of Uveal Melanoma: Methods, Applicability, and Limitations. Biomed. Res. Int. 2016, 2016, 4521807. [Google Scholar] [CrossRef] [PubMed]
- Kalirai, H.; Shahidipour, H.; Coupland, S.E.; Luyten, G. Use of the Chick Embryo Model in Uveal Melanoma. Ocul. Oncol. Pathol. 2015, 1, 133–140. [Google Scholar] [CrossRef]
- Luyten, G.P.; Mooy, C.M.; De Jong, P.T.; Hoogeveen, A.T.; Luider, T.M. A Chicken Embryo Model to Study the Growth of Human Uveal Melanoma. Biochem. Biophys. Res. Commun. 1993, 192, 22–29. [Google Scholar] [CrossRef]
- Sersa, G.; Miklavcic, D.; Cemazar, M.; Rudolf, Z.; Pucihar, G.; Snoj, M. Electrochemotherapy in Treatment of Tumours. Eur. J. Surg. Oncol. 2008, 34, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Mir, L.M.; Orlowski, S. The Basis of Electrochemotherapy. Methods Mol. Med. 2000, 37, 99–117. [Google Scholar] [CrossRef] [PubMed]
- Silve, A.; Leray, I.; Mir, L.M. Demonstration of Cell Membrane Permeabilization to Medium-Sized Molecules Caused by a Single 10 Ns Electric Pulse. Bioelectrochemistry 2012, 87, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Pucihar, G.; Kotnik, T.; Teissie, J.; Miklavcic, D. Electropermeabilization of Dense Cell Suspensions. Eur. Biophys J. 2007, 36, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Rols, M.P.; Teissie, J. Electropermeabilization of Mammalian Cells to Macromolecules: Control by Pulse Duration. Biophys J. 1998, 75, 1415–1423. [Google Scholar] [CrossRef]
- Pyrhonen, S.; Hahka-Kemppinen, M.; Muhonen, T.; Nikkanen, V.; Eskelin, S.; Summanen, P.; Tarkkanen, A.; Kivela, T. Chemoimmunotherapy with Bleomycin, Vincristine, Lomustine, Dacarbazine (Bold), and Human Leukocyte Interferon for Metastatic Uveal Melanoma. Cancer 2002, 95, 2366–2372. [Google Scholar] [CrossRef] [PubMed]
- Gehl, J. Electroporation: Theory and Methods, Perspectives for Drug Delivery, Gene Therapy and Research. Acta Physiol. Scand. 2003, 177, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Kotnik, T.; Kramar, P.; Pucihar, G.; Miklavcic, D.; Tarek, M. Cell Membrane Electroporation-Part 1: The Phenomenon. IEEE Electr. Insul. Mag. 2012, 28, 14–23. [Google Scholar] [CrossRef]
- Jager, M.J.; Magner, J.A.; Ksander, B.R.; Dubovy, S.R. Uveal Melanoma Cell Lines: Where Do They Come From? (An American Ophthalmological Society Thesis). Trans. Am. Ophthalmol. Soc. 2016, 114, T5. [Google Scholar]
- Dogrusoz, M.; Jager, M.J.; Damato, B. Uveal Melanoma Treatment and Prognostication. Asia Pac. J. Ophthalmol. 2017, 6, 186–196. [Google Scholar] [CrossRef]
- Hamburger, V.; Hamilton, H.L. A Series of Normal Stages in the Development of the Chick Embryo. J. Morphol 1951, 88, 49–92. [Google Scholar] [CrossRef] [PubMed]
- Hagedorn, M.; Javerzat, S.; Gilges, D.; Meyre, A.; de Lafarge, B.; Eichmann, A.; Bikfalvi, A. Accessing Key Steps of Human Tumor Progression in Vivo by Using an Avian Embryo Model. Proc. Natl. Acad. Sci. USA 2005, 102, 1643–1648. [Google Scholar] [CrossRef] [PubMed]
- Conn, E.M.; Botkjaer, K.A.; Kupriyanova, T.A.; Andreasen, P.A.; Deryugina, E.I.; Quigley, J.P. Comparative Analysis of Metastasis Variants Derived from Human Prostate Carcinoma Cells: Roles in Intravasation of Vegf-Mediated Angiogenesis and Upa-Mediated Invasion. Am. J. Pathol. 2009, 175, 1638–1652. [Google Scholar] [CrossRef] [PubMed]
- Subauste, M.C.; Kupriyanova, T.A.; Conn, E.M.; Ardi, V.C.; Quigley, J.P.; Deryugina, E.I. Evaluation of Metastatic and Angiogenic Potentials of Human Colon Carcinoma Cells in Chick Embryo Model Systems. Clin. Exp. Metastasis 2009, 26, 1033–1047. [Google Scholar] [CrossRef] [PubMed]
- Fergelot, P.; Bernhard, J.C.; Soulet, F.; Kilarski, W.W.; Leon, C.; Courtois, N.; Deminiere, C.; Herbert, J.M.; Antczak, P.; Falciani, F.; et al. The Experimental Renal Cell Carcinoma Model in the Chick Embryo. Angiogenesis 2013, 16, 181–194. [Google Scholar] [CrossRef] [PubMed]
- Lokman, N.A.; Elder, A.S.; Ricciardelli, C.; Oehler, M.K. Chick Chorioallantoic Membrane (Cam) Assay as an in Vivo Model to Study the Effect of Newly Identified Molecules on Ovarian Cancer Invasion and Metastasis. Int. J. Mol. Sci. 2012, 13, 9959–9970. [Google Scholar] [CrossRef]
- Wan, J.; Chai, H.; Yu, Z.; Ge, W.; Kang, N.; Xia, W.; Che, Y. Hif-1alpha Effects on Angiogenic Potential in Human Small Cell Lung Carcinoma. J. Exp. Clin. Cancer Res. 2011, 30, 77. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.D.; Kivela, T. The Collaborative Ocular Melanoma Study. Ophthalmol. Clin. North. Am. 2005, 18, 129–142. [Google Scholar] [CrossRef]
- Griewank, K.G.; Yu, X.; Khalili, J.; Sozen, M.M.; Stempke-Hale, K.; Bernatchez, C.; Wardell, S.; Bastian, B.C.; Woodman, S.E. Genetic and Molecular Characterization of Uveal Melanoma Cell Lines. Pigment Cell Melanoma Res. 2012, 25, 182–187. [Google Scholar] [CrossRef]
- Rueden, C.T.; Schindelin, J.; Hiner, M.C.; DeZonia, B.E.; Walter, A.E.; Arena, E.T.; Eliceiri, K.W. Imagej2: Imagej for the Next Generation of Scientific Image Data. BMC Bioinformatics 2017, 18, 529. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cell line | Average Differences Compared to Untreated Controls (in %) | ||
|---|---|---|---|
| EP | Chemotherapy | ECT | |
| Primary UM cell lines | |||
| MP46 | −3.0 | 19.8 | 18.3 |
| 92.1 | 6.8 | 2.9 | 14.4 |
| Mel270 | −0.7 | 17.5 | 25.4 |
| Mean differences | 1.1 | 13.4 | 19.4 |
| Metastatic UM cell lines | |||
| MM28 | 13.9 | 33.0 | 79.9 |
| OMM1 | 10.9 | 14.0 | 32.6 |
| Mean differences | 12.4 | 23.5 | 56.2 |
| Cell line | Average Differences Compared to Untreated Controls (in %) | ||
|---|---|---|---|
| EP | Chemotherapy | ECT | |
| Primary UM cell lines | |||
| MP46 | −1.5 | 12.8 | 49.3 |
| 92.1 | 5.7 | 5.7 | 29.4 |
| Mel270 | 4.8 | −3.0 | 1.9 |
| Mean differences | −0.2 | 5.2 | 26.8 |
| Metastatic UM cell lines | |||
| MM28 | 7.0 | 8.3 | 58.1 |
| OMM1 | −2.4 | 26.7 | 25.0 |
| Mean differences | 2.3 | 17.5 | 41.5 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiorentzis, M.; Viestenz, A.; Siebolts, U.; Seitz, B.; Coupland, S.E.; Heinzelmann, J. The Potential Use of Electrochemotherapy in the Treatment of Uveal Melanoma: In Vitro Results in 3D Tumor Cultures and In Vivo Results in a Chick Embryo Model. Cancers 2019, 11, 1344. https://doi.org/10.3390/cancers11091344
Fiorentzis M, Viestenz A, Siebolts U, Seitz B, Coupland SE, Heinzelmann J. The Potential Use of Electrochemotherapy in the Treatment of Uveal Melanoma: In Vitro Results in 3D Tumor Cultures and In Vivo Results in a Chick Embryo Model. Cancers. 2019; 11(9):1344. https://doi.org/10.3390/cancers11091344
Chicago/Turabian StyleFiorentzis, Miltiadis, Arne Viestenz, Udo Siebolts, Berthold Seitz, Sarah E. Coupland, and Joana Heinzelmann. 2019. "The Potential Use of Electrochemotherapy in the Treatment of Uveal Melanoma: In Vitro Results in 3D Tumor Cultures and In Vivo Results in a Chick Embryo Model" Cancers 11, no. 9: 1344. https://doi.org/10.3390/cancers11091344
APA StyleFiorentzis, M., Viestenz, A., Siebolts, U., Seitz, B., Coupland, S. E., & Heinzelmann, J. (2019). The Potential Use of Electrochemotherapy in the Treatment of Uveal Melanoma: In Vitro Results in 3D Tumor Cultures and In Vivo Results in a Chick Embryo Model. Cancers, 11(9), 1344. https://doi.org/10.3390/cancers11091344