The Impact of Flt3 Gene Mutations in Acute Promyelocytic Leukemia: A Meta-Analysis
 ,
,  ,
,
Abstract
:1. Introduction
2. Results
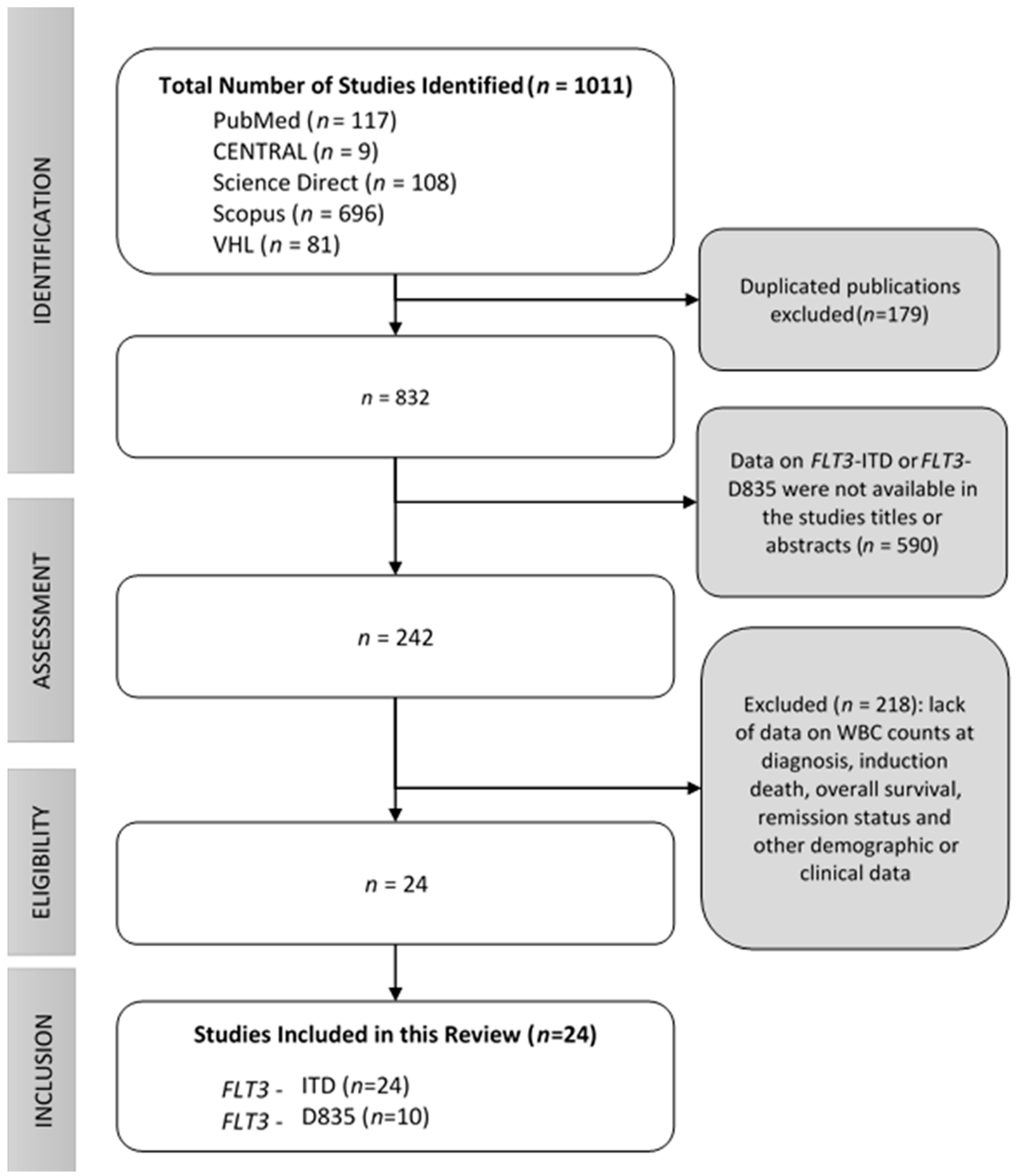
2.1. Search Results
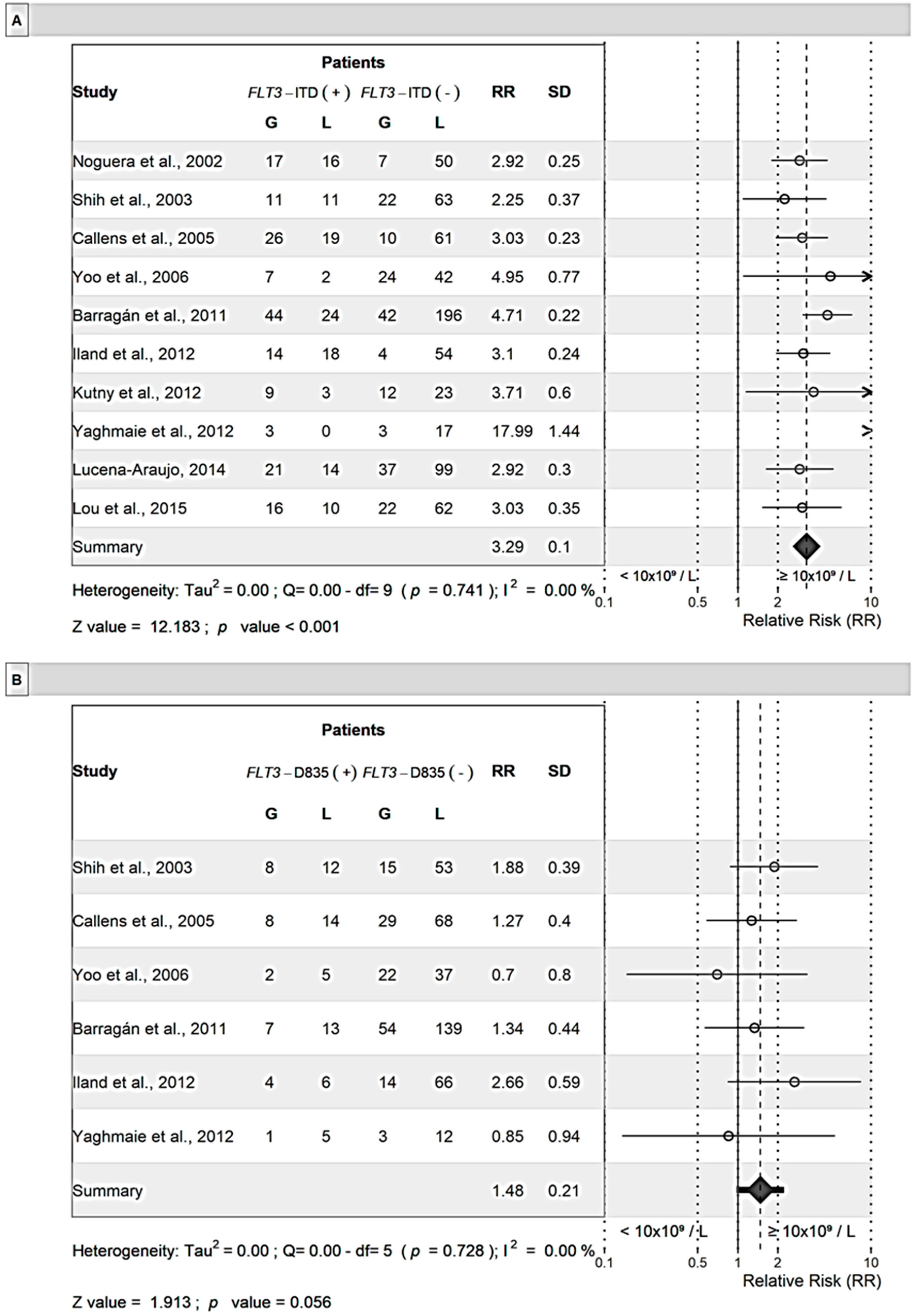
2.2. Sex and WBC Count According to FLT3 Status
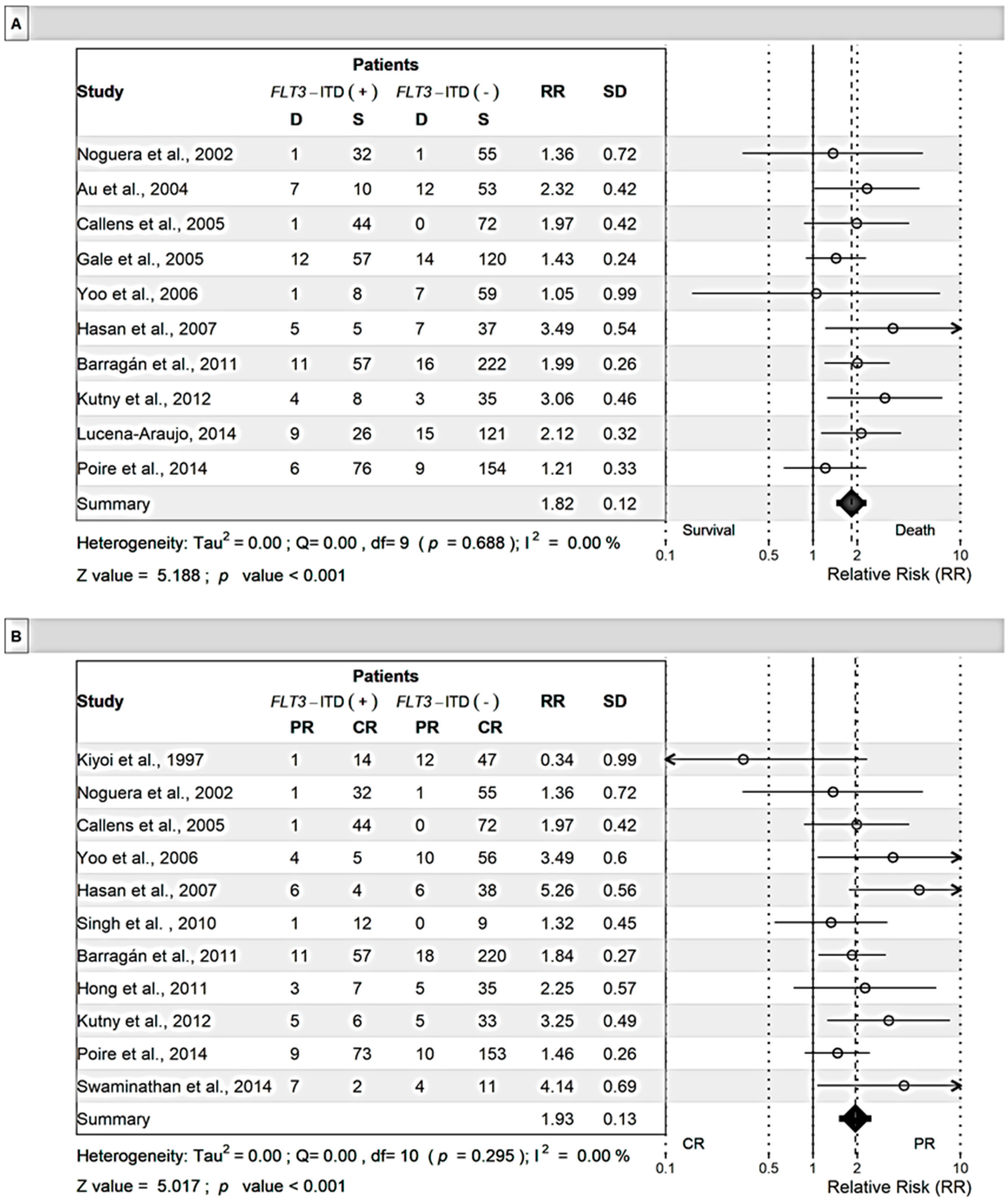
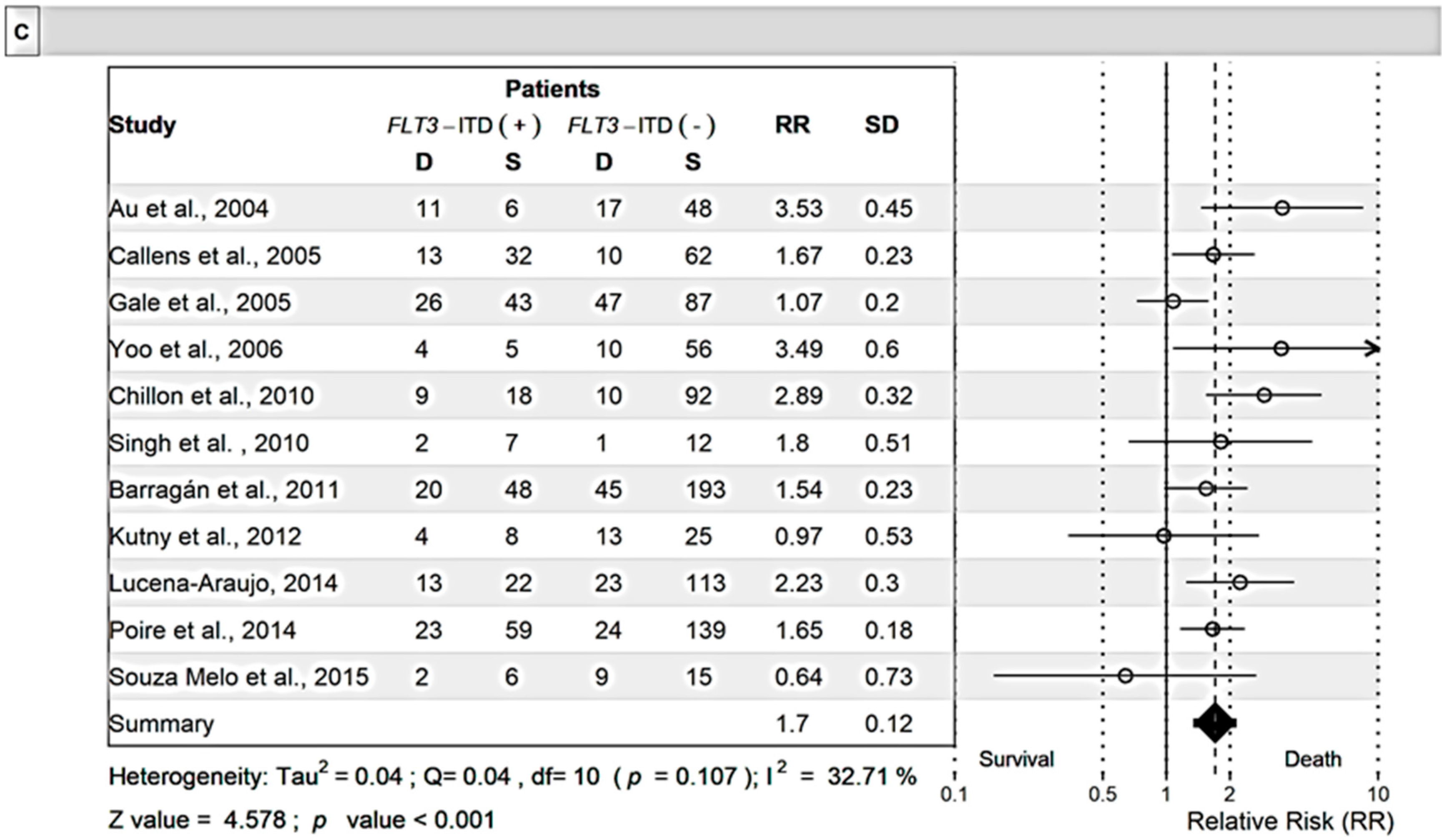
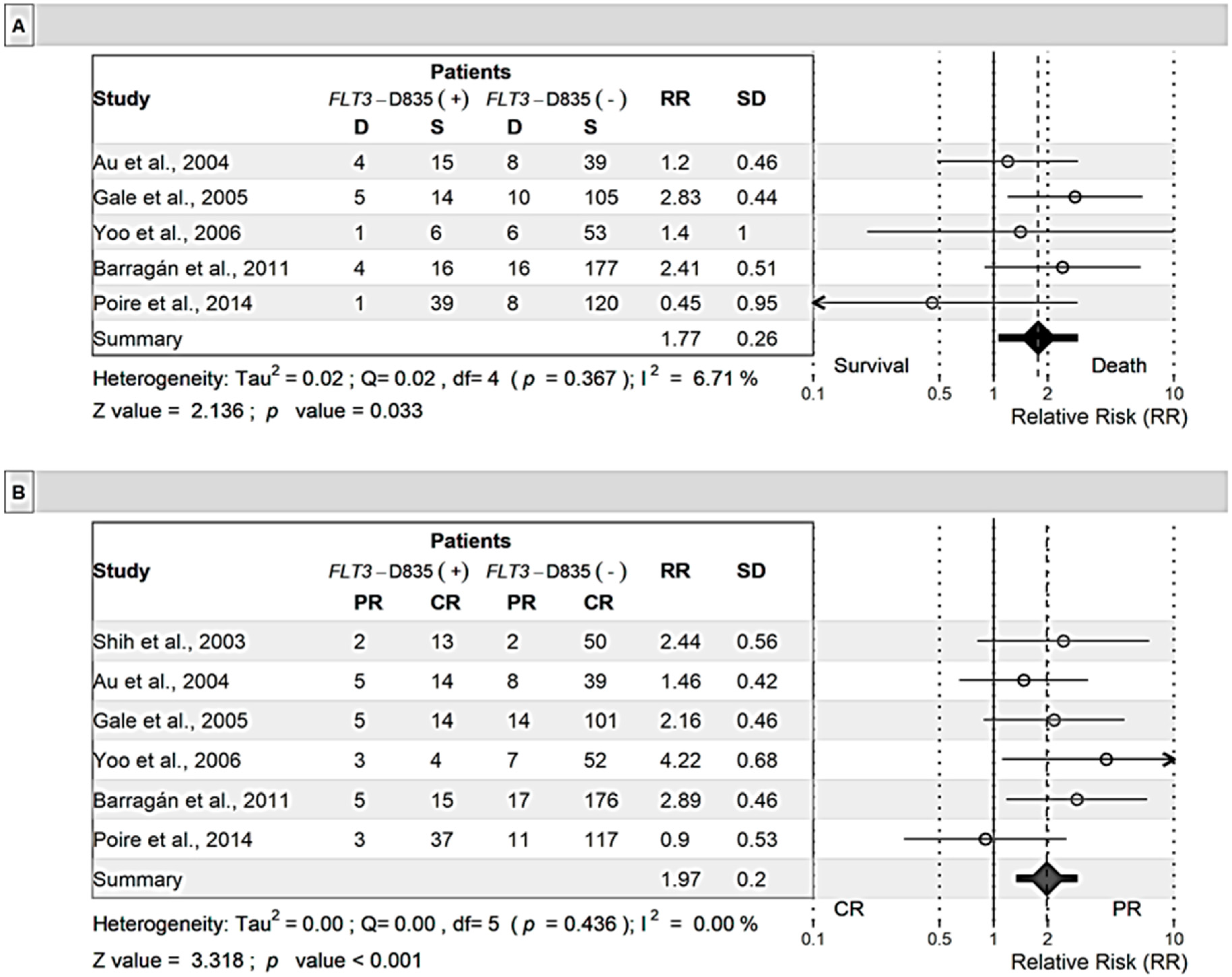
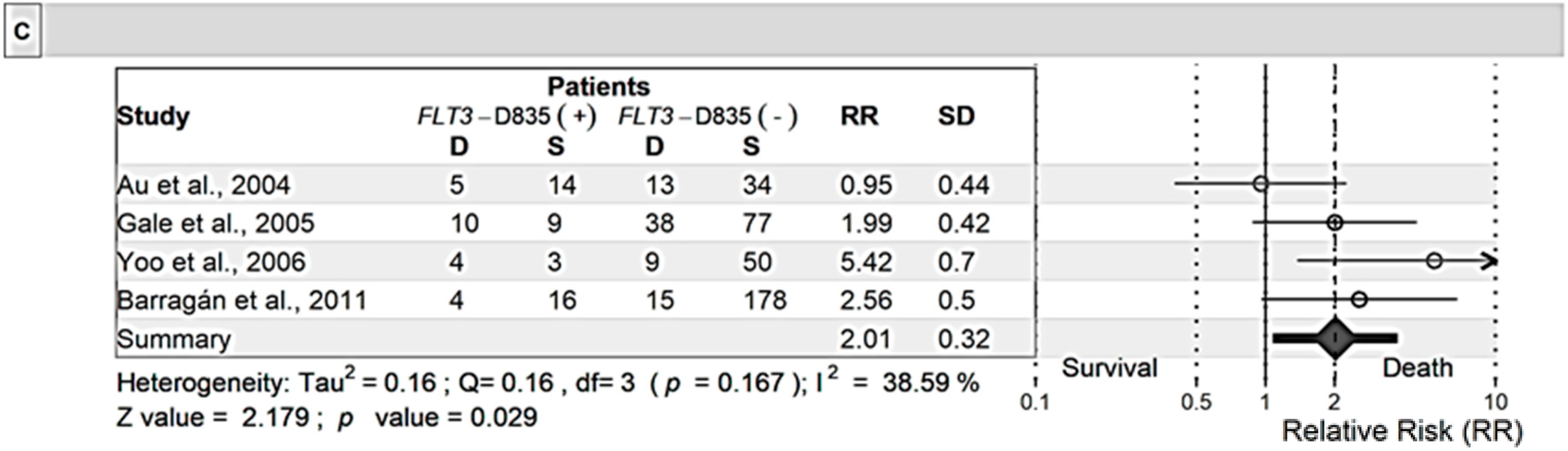
2.3. Outcome According to FLT3 Status
3. Discussion
4. Methods
4.1. Protocol
4.2. Search Strategy and Eligibility Criteria
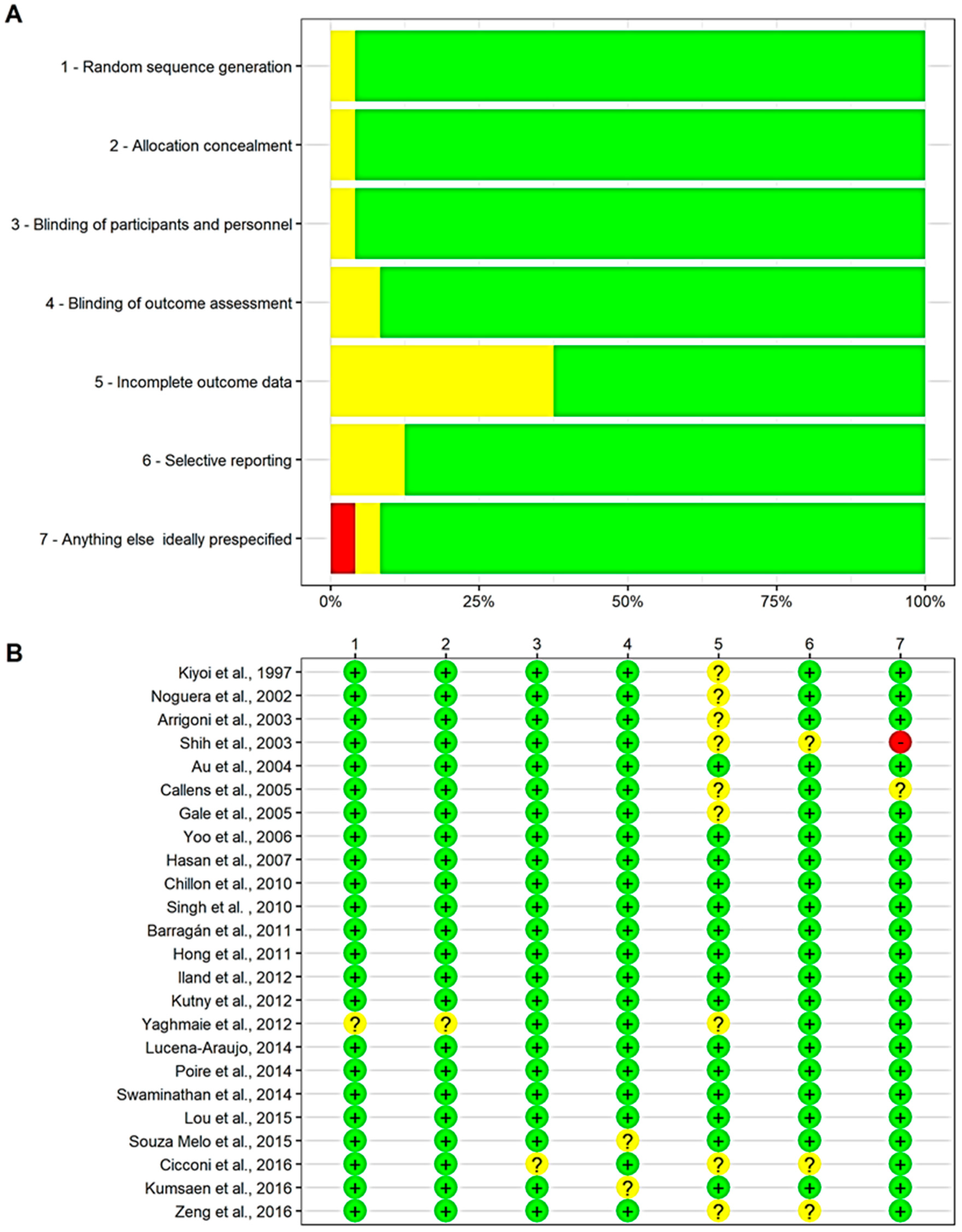
4.3. Selection of Publications, Data Extraction, and Quality Assessment
4.4. Outcome Measures and Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mendez, L.; Chen, M.; Pandolfi, P.P. Molecular Genetics of APL. In Acute Promyelocytic Leukemia: A Clinical Guide; Abla, O.F., Lo-Coco, F., Sanz, M.A., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 41–53. [Google Scholar]
- Elsayed, G.M.; Nassar, H.R.; Zaher, A.; Elnoshokaty, E.H.; Moneer, M.M. Prognostic value of IDH1 mutations identified with PCR-RFLP assay in acute myeloid leukemia patients. J. Egypt. Natl. Cancer Inst. 2014, 26, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Cerver, J.; Sanz, M.A. Revealing the mutational landscape of acute promyelocytic leukemia. Transl. Cancer Res. 2017, 6, S127–S130. [Google Scholar] [CrossRef]
- Breccia, M.; Loglisci, G.; Loglisci, M.G.; Ricci, R.; Diverio, D.; Latagliata, R.; Foà, R.; Lo-Coco, F. FLT3-ITD confers poor prognosis in patients with acute promyelocytic leukemia treated with AIDA protocols: Long-term follow-up analysis. Haematologica 2013, 98, e161–e163. [Google Scholar] [CrossRef]
- Niu, C.; Yan, H.; Yu, T.; Sun, H.P.; Liu, J.X.; Li, X.S.; Wu, W.; Zhang, F.Q.; Chen, Y.; Zhou, L.; et al. Studies on treatment of acute promyelocytic leukemia with arsenic trioxide: Remission induction, follow-up, and molecular monitoring in 11 newly diagnosed and 47 relapsed acute promyelocytic leukemia patients. Blood 2014, 94, 3315–3324. [Google Scholar]
- Beitinjaneh, A.; Jang, S.; Roukoz, H.; Majhail, N.S. Prognostic significance of FLT3 internal tandem duplication and tyrosine kinase domain mutations in acute promyelocytic leukemia: A systematic review. Leuk. Res. 2010, 34, 831–836. [Google Scholar] [CrossRef]
- Li, W.; Zhang, L.; Huang, L.; Mi, Y.; Wang, J. Meta-analysis for the potential application of FLT3-TKD mutations as prognostic indicator in non-promyelocytic AML. Leuk. Res. 2012, 36, 186–191. [Google Scholar] [CrossRef]
- Sanz, M.A.; Fenaux, P.; Tallman, M.S.; Estey, E.H.; Löwenberg, B.; Naoe, T.; Lengfelder, E.; Döhner, H.; Burnett, A.K.; Chen, S.J.; et al. Management of acute promyelocytic leukemia: Updated recommendations from an expert panel of the European LeukemiaNet. Blood 2019, 133, 1630–1643. [Google Scholar] [CrossRef]
- Lo-Coco, F.; Avvisati, G.; Vignetti, M.; Thiede, C.; Orlando, S.M.; Iacobelli, S.; Ferrara, F.; Fazi, P.; Cicconi, L.; Di Bona, E.; et al. Retinoic Acid and Arsenic Trioxide for Acute Promyelocytic Leukemia. N. Engl. J. Med. 2013, 369, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Kutny, M.A.; Alonzo, T.A.; Gerbing, R.B.; Wang, Y.C.; Raimondi, S.C.; Hirsch, B.A.; Fu, C.H.; Meshinchi, S.; Gamis, A.S.; Feusner, J.H.; et al. Arsenic Trioxide Consolidation Allows Anthracycline Dose Reduction for Pediatric Patients with Acute Promyelocytic Leukemia: Report from the Children’s Oncology Group Phase III Historically Controlled Trial AAML0631. J. Clin. Oncol. 2017, 35, 3021–3029. [Google Scholar] [CrossRef]
- Wang, Z.; Chen, Z. Acute promyelocytic leukemia: From highly fatal to highly curable. Blood 2008, 111, 2505–2515. [Google Scholar] [CrossRef]
- Tallman, M.S.; Andersen, J.W.; Schiffer, C.A.; Appelbaum, F.R.; Feusner, J.H.; Woods, W.G.; Ogden, A.; Weinstein, H.; Shepherd, L.; Willman, C.; et al. All-trans retinoic acid in acute promyelocytic leukemia: Long-term outcome and prognostic factor analysis from the North American Intergroup protocol. Blood 2002, 100, 4298–4302. [Google Scholar] [CrossRef]
- Arrigoni, P.; Beretta, C.; Silvestri, D.; Rossi, V.; Rizzari, C.; Valsecchi, M.G.; Cazzaniga, G.; Biondi, A. FLT3 internal tandem duplication in childhood acute myeloid leukaemia: Association with hyperleucocytosis in acute promyelocytic leukaemia. Br. J. Haematol. 2003, 120, 89–92. [Google Scholar] [CrossRef]
- Au, W.Y.; Fung, A.; Chim, C.S.; Lie, A.K.; Liang, R.; Ma, E.S.; Chan, C.H.; Wong, K.F.; Kwong, Y.L. FLT-3 aberrations in acute promyelocytic leukaemia: Clinicopathological associations and prognostic impact. Br. J. Haematol. 2004, 25, 463–469. [Google Scholar] [CrossRef]
- Barragán, E.; Montesinos, P.; Camos, M.; González, M.; Calasanz, M.J.; Román-Gómez, J.; Gómez-Casares, M.T.; Ayala, R.; López, J.; Fuster, Ó.; et al. Prognostic value of FLT3 mutations in patients with acute promyelocytic leukemia treated with all-trans retinoic acid and anthracycline monochemotherapy. Haematologica 2011, 96, 1470–1477. [Google Scholar] [CrossRef] [Green Version]
- Callens, C.; Chevret, S.; Cayuela, J.M.; Cassinat, B.; Raffoux, E.; de Botton, S.; Thomas, X.; Guerci, A.; Fegueux, N.; Pigneux, A.; et al. Prognostic implication of FLT3 and Ras gene mutations in patients with acute promyelocytic leukemia (APL): A retrospective study from the European APL Group. Leukemia 2005, 19, 1153–1160. [Google Scholar] [CrossRef]
- Chillón, M.C.; Santamaría, C.; García-Sanz, R.; Balanzategui, A.; Sarasquete, M.E.; Alcoceba, M.; Marín, L.; Caballero, M.D.; Vidriales, M.B.; Ramos, F.; et al. Long FLT3 internal tandem duplications and reduced PML-RARα expression at diagnosis characterize a high-risk subgroup of acute promyelocytic leukemia patients. Haematologica 2010, 95, 745–751. [Google Scholar] [CrossRef]
- Cicconi, L.; Divona, M.; Ciardi, C.; Ottone, T.; Ferrantini, A.; Lavorgna, S.; Alfonso, V.; Paoloni, F.; Piciocchi, A.; Avvisati, G.; et al. PML-RARα kinetics and impact of FLT3-ITD mutations in newly diagnosed acute promyelocytic leukaemia treated with ATRA and ATO or ATRA and chemotherapy. Leukemia 2016, 30, 1987–1992. [Google Scholar] [CrossRef]
- Gale, R.E.; Hills, R.; Pizzey, A.R.; Kottaridis, P.D.; Swirsky, D.; Gilkes, A.F.; Nugent, E.; Mills, K.I.; Wheatley, K.; Solomon, E.; et al. Relationship between FLT3 mutation status, biologic characteristics, and response to targeted therapy in acute promyelocytic leukemia. Blood 2005, 106, 3768–3776. [Google Scholar] [CrossRef] [Green Version]
- Mathews, V.; Thomas, M.; Srivastava, V.M.; George, A.; Srivastava, V.M.; Chandy, M. Impact of FLT3 mutations and secondary cytogenetic changes on the outcome of patients with newly diagnosed acute promyelocytic leukemia treated with a single agent arsenic trioxide regimen. Haematologica 2007, 92, 994–995. [Google Scholar] [CrossRef] [Green Version]
- Hong, S.D.; Kim, Y.K.; Kim, H.N.; Lee, S.R.; Ahn, J.S.; Yang, D.H.; Lee, J.J.; Lee, I.K.; Shin, M.G.; Kim, H.J. Treatment outcome of all-trans retinoic acid/anthracycline combination chemotherapy and the prognostic impact of FLT3/ITD mutation in acute promyelocytic leukemia patients. Korean J. Hematol. 2011, 46, 24–30. [Google Scholar] [CrossRef]
- Iland, H.; Bradstock, K.; Seymour, J.; Hertzberg, M.; Grigg, A.; Taylor, K.; Catalano, J.; Cannell, P.; Horvath, N.; Deveridge, S.; et al. Results of the APML3 trial incorporating all-trans-retinoic acid and idarubicin in both induction and consolidation as initial therapy for patients with acute promyelocytic leukemia. Haematologica 2012, 97, 27–234. [Google Scholar] [CrossRef]
- Kiyoi, H.; Naoe, T.; Yokota, S.; Nakao, M.; Minami, S.; Kuriyama, K.; Takeshita, A.; Saito, K.; Hasegawa, S.; Shimodaira, S.; et al. Internal tandem duplication of FLT3 associated with leukocytosis in acute promyelocytic leukemia. Leukemia 1997, 11, 1447–1452. [Google Scholar] [CrossRef] [Green Version]
- Kutny, M.A.; Moser, B.K.; Laumann, K.; Feusner, J.H.; Gamis, A.; Gregory, J.; Larson, R.A.; Powell, B.L.; Stock, W.; Willman, C.L.; et al. FLT3 mutation status is a predictor of early death in pediatric acute promyelocytic leukemia: A report from the Children’s Oncology Group. Pediatr. Blood Cancer 2012, 59, 662–667. [Google Scholar] [CrossRef]
- Lou, Y.; Ma, Y.; Suo, S.; Ni, W.; Wang, Y.; Pan, H.; Tong, H.; Qian, W.; Meng, H.; Mai, W.; et al. Prognostic factors of patients with newly diagnosed acute promyelocytic leukemia treated with arsenic trioxide-based frontline therapy. Leuk. Res. 2015, 39, 938–944. [Google Scholar] [CrossRef]
- Lucena-Araujo, A.R.; Kim, H.T.; Jacomo, R.H.; Melo, R.A.; Bittencourt, R.; Pasquini, R.; Pagnano, K.; Fagundes, E.M.; Chauffaille Mde, L.; Chiattone, C.S.; et al. Internal tandem duplication of the FLT3 gene confers poor overall survival in patients with acute promyelocytic leukemia treated with all-trans retinoic acid and anthracycline-based chemotherapy: An International Consortium on Acute Promyelocytic Leukemia. Ann. Hematol. 2014, 93, 2001–2010. [Google Scholar] [CrossRef]
- Noguera, N.I.; Breccia, M.; Divona, M.; Diverio, D.; Costa, V.; De Santis, S.; Avvisati, G.; Pinazzi, M.B.; Petti, M.C.; Mandelli, F.; et al. Alterations of the FLT3 gene in acute promyelocytic leukemia: Association with diagnostic characteristics and analysis of clinical outcome in patients treated with the Italian AIDA protocol. Leukemia 2002, 16, 2185–2189. [Google Scholar] [CrossRef]
- Poiré, X.; Moser, B.K.; Gallagher, R.E.; Laumann, K.; Bloomfield, C.D.; Powell, B.L.; Koval, G.; Gulati, K.; Holowka, N.; Larson, R.A.; et al. Arsenic trioxide in front-line therapy of acute promyelocytic leukemia (C9710): Prognostic significance of FLT3 mutations and complex karyotype. Leuk. Lymphoma 2014, 55, 523–1532. [Google Scholar] [CrossRef]
- Shih, L.Y.; Kuo, M.C.; Liang, D.C.; Huang, C.F.; Lin, T.L.; Wu, J.H.; Wang, P.N.; Dunn, P.; Lai, C.L. Internal tandem duplication and Asp835 mutations of the FMS-like tyrosine kinase 3 (FLT3) gene in acute promyelocytic leukemia. Cancer 2003, 98, 1206–1216. [Google Scholar] [CrossRef]
- Singh, H.; Werner, L.; Deangelo, D.; Ballen, K.; Amrein, P.; Wadleigh, M.; Neuberg, D.; Fox, E.; Stone, R.; Attar, E. Clinical outcome of patients with acute promyelocytic leukemia and FLT3 mutations. Am. J. Hematol. 2010, 85, 956–957. [Google Scholar] [CrossRef] [Green Version]
- Yoo, S.J.; Park, C.J.; Jang, S.; Seo, E.J.; Lee, K.H.; Chi, H.S. Inferior prognostic outcome in acute promyelocytic leukemia with alterations of FLT3 gene. Leuk. Lymphoma 2006, 47, 1788–1793. [Google Scholar] [CrossRef]
- Souza Melo, C.P.; Campos, C.B.; Dutra, Á.P.; Neto, J.C.; Fenelon, A.J.; Neto, A.H.; Carbone, E.K.; Pianovski, M.A.; Ferreira, A.C.; Assumpcão, J.G. Correlation between FLT3–ITD status and clinical, cellular and molecular profiles in promyelocytic acute leukemias. Leuk. Res. 2015, 39, 131–137. [Google Scholar] [CrossRef]
- Swaminathan, S.; Garg, S.; Madkaikar, M.; Gupta, M.; Jijina, F.; Ghosh, K. FLT3 and NPM-1 mutations in a cohort of acute promyelocytic leukemia patients from India. Indian J. Hum. Genet. 2014, 20, 160–165. [Google Scholar] [Green Version]
- Yaghmaie, M.; Alimoghaddam, K.; Mozdarani, H.; Ghavamzadeh, A.; Hajhashemi, M.; Aznab, M.; Ghaffari, S.H. Cytogenetic and FMS-like tyrosine kinase 3 mutation analyses in acute promyelocytic leukemia patients. Iran. Biomed. J. 2012, 16, 10–17. [Google Scholar]
- Zeng, H.; Yin, L.D.; Li, P.; Yuan, Y.H.; Guan, C.Y.; Xie, T.; Zhang, Q.G. The level of peripheral blood circulating CD34+ cells is higher in acute promyelocytic leukemia patients with adverse prognostic factors. Hematology 2016, 21, 513–519. [Google Scholar] [CrossRef] [Green Version]
- Kumsaen, P.; Fucharoen, G.; Sirijerachai, C.; Chainansamit, S.O.; Wisanuyothin, N.; Kuwatjanakul, P.; Wiangnon, S. FLT3-ITD Mutations in Acute Myeloid Leukemia Patients in Northeast Thailand. Asian Pac. J. Cancer Prev. 2016, 17, 4395–4399. [Google Scholar]
- Kumsaen, P.; Fucharoen, G.; Sirijerachai, C.; Chainansamit, S.O.; Wisanuyothin, N.; Kuwatjanakul, P.; Wiangnon, S. Cytogenetic and genetic mutation features of de novo acute myeloid leukemia in elderly Chinese patients. Asian Pac. J. Cancer Prev. 2014, 5, 895–898. [Google Scholar]
- Ablain, J.; De Thé, H. Retinoic acid signaling in cancer: The parable of acute promyelocytic leukemia. Int. J. Cancer 2014, 135, 2262–2272. [Google Scholar] [CrossRef]
- Vickers, M.; Jackson, G.; Taylor, P. The incidence of acute promyelocytic leukemia appears constant over most of a human lifespan, implying only one rate limiting mutation. Leukemia 2000, 14, 722–726. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.N.; Tang, Y.L.; Zhang, Y.C.; Zhang, Z.H.; Liu, X.J.; Ke, Z.Y.; Li, Y.; Tan, H.Z.; Huang, L.B.; Luo, X.Q. Arsenic trioxide and all-trans-retinoic acid selectively exert synergistic cytotoxicity against FLT3-ITD AML cells via co-inhibition of FLT3 signaling pathways. Leuk. Lymphoma 2017, 58, 2426–2438. [Google Scholar] [CrossRef]
- Fleischmann, M.; Schnetzke, U.; Schrenk, K.G.; Schmidt, V.; Sayer, H.G.; Hilgendorf, I.; Hochhaus, A.; Scholl, S. Outcome of FLT3-ITD- positive acute myeloid leukemia: Impact of allogeneic stem cell transplantation and tyrosine kinase inhibitor treatment. J. Cancer Res. Clin. Oncol. 2017, 143, 337–345. [Google Scholar] [CrossRef]
- Thomas, C.M.; Campbell, P. FLT3 inhibitors in acute myeloid leukemia: Current and future. J. Oncol. Pharm. Pract. 2019, 25, 163–171. [Google Scholar] [CrossRef]
- Wu, M.; Li, C.; Zhu, X. FLT3 inhibitors in acute myeloid leukemia. J. Hematol. Oncol. 2018, 11, 33. [Google Scholar] [CrossRef]
- Chauffaille, M.L.; Borri, D.; Proto-Siqueira, R.; Moreira, E.S.; Alberto, F.L. Acute promyelocytic leukemia with t (15;17): Frequency of additional clonal chromosome abnormalities and FLT3 mutations. Leuk. Lymphoma 2008, 49, 2387–2389. [Google Scholar] [CrossRef]
- Wiernik, P.H. Plasma cell dyscrasias and leukemias. Cancer Chemother. Biol. Response Modif. 2005, 22, 343–389. [Google Scholar]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, 1–9. [Google Scholar] [CrossRef]
- R Core Team. R: Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: http://www.R-project.org/ (accessed on 6 July 2019).
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Softw. 2010, 36. [Google Scholar] [CrossRef]
- Stuck, A.E. Bias in meta-analysis detected by a simple, graphical. BMJ 1998, 316, 469. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Kitada, S.; Pedersen, I.M.; Schimmer, A.D.; Reed, J.C. Dysregulation of apoptosis genes in hematopoietic malignancies. Oncogene 2002, 21, 3459–3474. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study [Reference] | n | Male n (%) | WBC ≥ 10 × 109/L n (%) | Early Death n (%) | FLT3-ITD n (%) | FLT3-D835 n (%) |
|---|---|---|---|---|---|---|
| Arrigoni, 2003 [13] | 29 | 16 (55.2%) | - | - | 10 (34.5%) | - |
| Au, 2004 [14] | 82 | 39 (47.6%) | - | 19 (23.2%) | 17 (20.7%) | 19 (23.2%) |
| Barragán, 2011 [15] | 306 | 155 (50.7%) | 86 (28.1%) | 27 (8.8%) | 68 (22.2%) | 20 (9.4%) |
| Callens, 2005 [16] | 117 | 54 (46.2%) | 36 (30.8%) | 1 (0.9%) | 45 (38.5%) | 22 (19.6%) |
| Chillón, 2010 [17] | 129 | - | - | - | 27 (20.9%) | 12 (9.3%) |
| Cicconi, 2016 [18] | 159 | 81 (50.9%) | - | - | 33 (20.8%) | |
| Gale, 2005 [19] | 203 | - | - | 26 (12.8%) | 69(34.0%) | 19 (14.2%) |
| Hasan, 2007 [20] | 54 | 30 (55.6%) | - | 12 (22.2%) | 10 (18.5%) | |
| Hong, 2011 [21] | 50 | 22 (44.0%) | - | - | 10 (20.0%) | |
| Iland, 2012 [22] | 90 | - | 18 (20.0%) | - | 32 (35.6%) | 10 (11.1%) |
| Kiyoi, 1997 [23] | 74 | 39 (52.7%) | - | - | 15 (20.3%) | - |
| Kutny, 2012 [24] | 50 | 32 (64.0%) | 21 (42.0%) | 7 (14.0%) | 12 (24.0%) | - |
| Lou, 2015 [25] | 110 | 61 (55.5%) | 38 (34.5%) | - | 26 (23.6%) | - |
| Lucena, 2014 [26] | 171 | 85 (49.7%) | 58 (33.9%) | 24 (14.0%) | 35 (20.5%) | - |
| Noguera, 2002 [27] | 90 | 43 (47.8%) | 24 (26.7%) | 2 (2.2%) | 33 (36.7%) | - |
| Poiré, 2014 [28] | 245 | 134 (54.7%) | - | 15 (6.1%) | 82 (33.5%) | 40 (23.8%) |
| Shih, 2003 [29] | 107 | 50 (46.7%) | 33 (30.8%) | - | 22 (20.6%) | 20 (22.7%) |
| Singh, 2010 [30] | 22 | 11 (50.0%) | - | - | 9 (40.9%) | - |
| Yoo, 2006 [31] | 75 | 34 (45.3%) | 31 (41.3%) | 8 (10.7%) | 9 (12.0%) | 7 (10.4%) |
| Souza, 2015 [32] | 34 | 18 (52.9%) | - | - | 8 (23.5%) | - |
| Swaminathan, 2014 [33] | 40 | 21 (52.5%) | - | - | 10 (25.0%) | - |
| Yaghmaie, 2012 [34] | 23 | 19 (82.6%) | 6 (26.1%) | - | 3 (13.0%) | 6 (28.6%) |
| Zeng, 2016 [35] | 69 | 33 (48%) | - | - | 50 (72%) | - |
| Kumsaen, 2016 [36] | 52 | 28 (54%) | - | - | 10 (19%) | - |
| Total | 2381 | 1005 | 351 | 141 | 645 | 175 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Picharski, G.L.; Andrade, D.P.; Fabro, A.L.M.R.; Lenzi, L.; Tonin, F.S.; Ribeiro, R.C.; Figueiredo, B.C. The Impact of Flt3 Gene Mutations in Acute Promyelocytic Leukemia: A Meta-Analysis. Cancers 2019, 11, 1311. https://doi.org/10.3390/cancers11091311
Picharski GL, Andrade DP, Fabro ALMR, Lenzi L, Tonin FS, Ribeiro RC, Figueiredo BC. The Impact of Flt3 Gene Mutations in Acute Promyelocytic Leukemia: A Meta-Analysis. Cancers. 2019; 11(9):1311. https://doi.org/10.3390/cancers11091311
Chicago/Turabian StylePicharski, Gledson L., Diancarlos P. Andrade, Ana Luiza M. R. Fabro, Luana Lenzi, Fernanda S. Tonin, Raul C. Ribeiro, and Bonald C. Figueiredo. 2019. "The Impact of Flt3 Gene Mutations in Acute Promyelocytic Leukemia: A Meta-Analysis" Cancers 11, no. 9: 1311. https://doi.org/10.3390/cancers11091311
APA StylePicharski, G. L., Andrade, D. P., Fabro, A. L. M. R., Lenzi, L., Tonin, F. S., Ribeiro, R. C., & Figueiredo, B. C. (2019). The Impact of Flt3 Gene Mutations in Acute Promyelocytic Leukemia: A Meta-Analysis. Cancers, 11(9), 1311. https://doi.org/10.3390/cancers11091311