Predictors of Outcomes in Patients with EGFR-Mutated Non-Small Cell Lung Cancer Receiving EGFR Tyrosine Kinase Inhibitors: A Systematic Review and Meta-Analysis

 , , ,
, , , 
Abstract
1. Introduction
2. Results
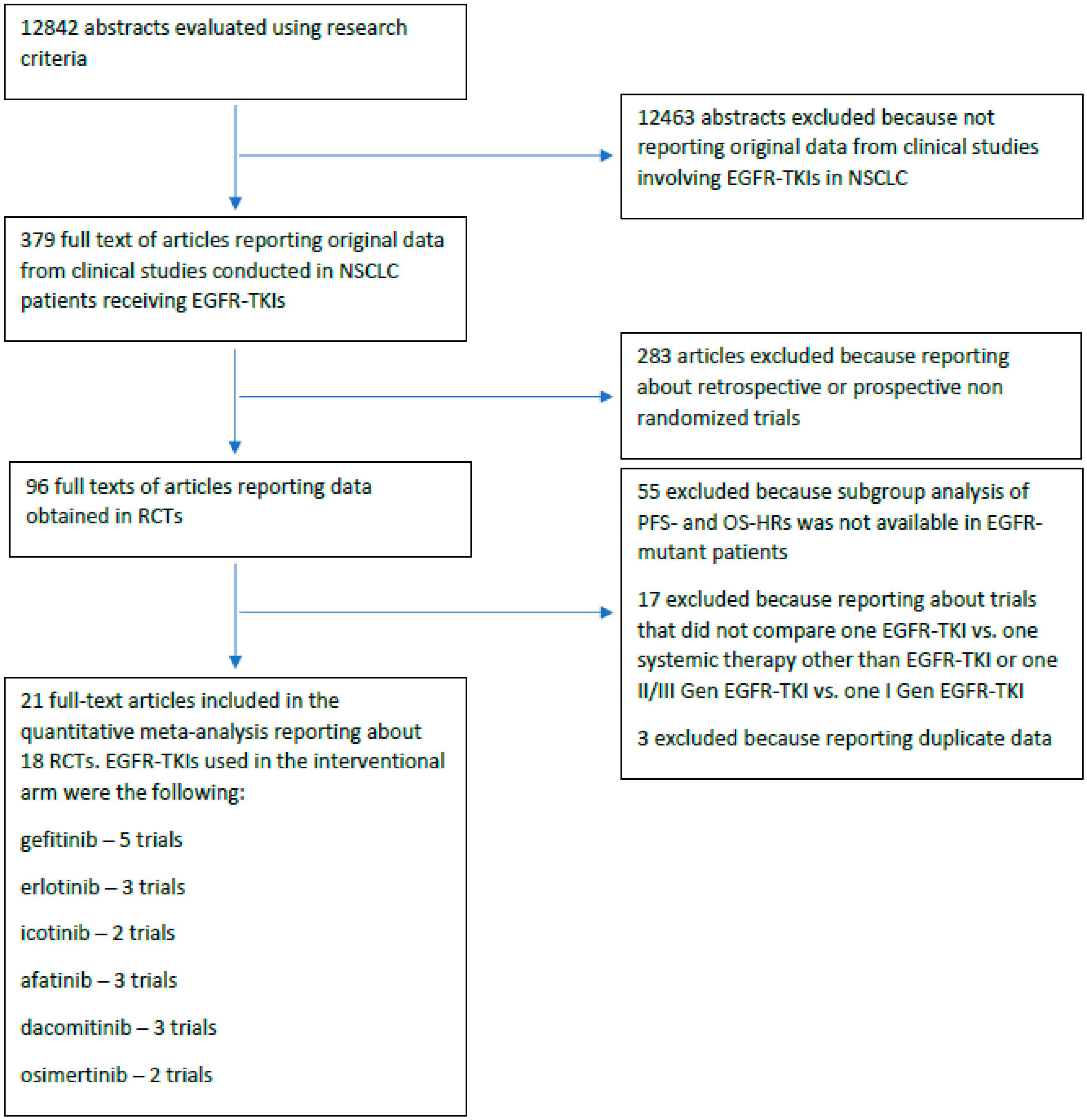
2.1. Eligible Articles
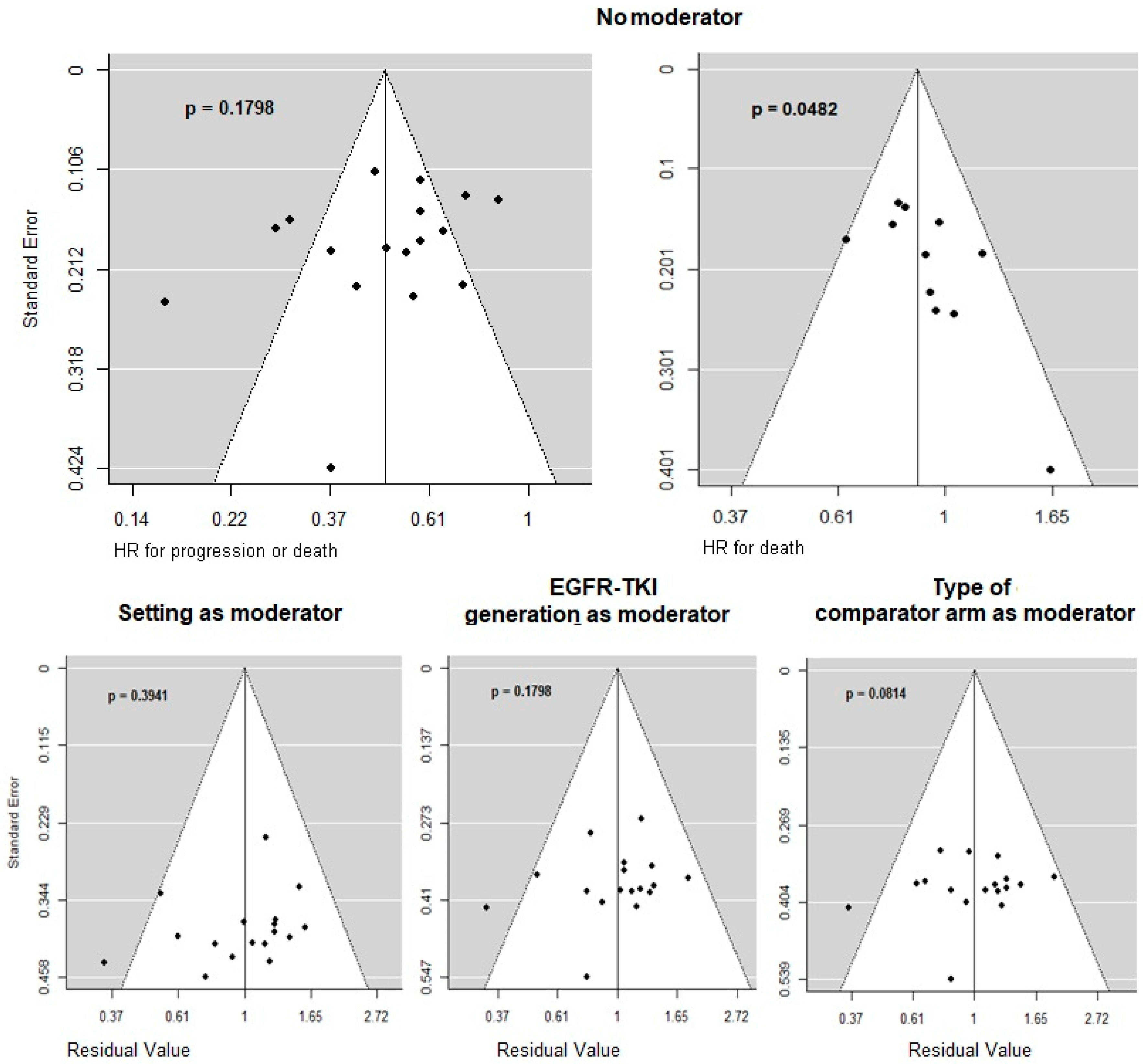
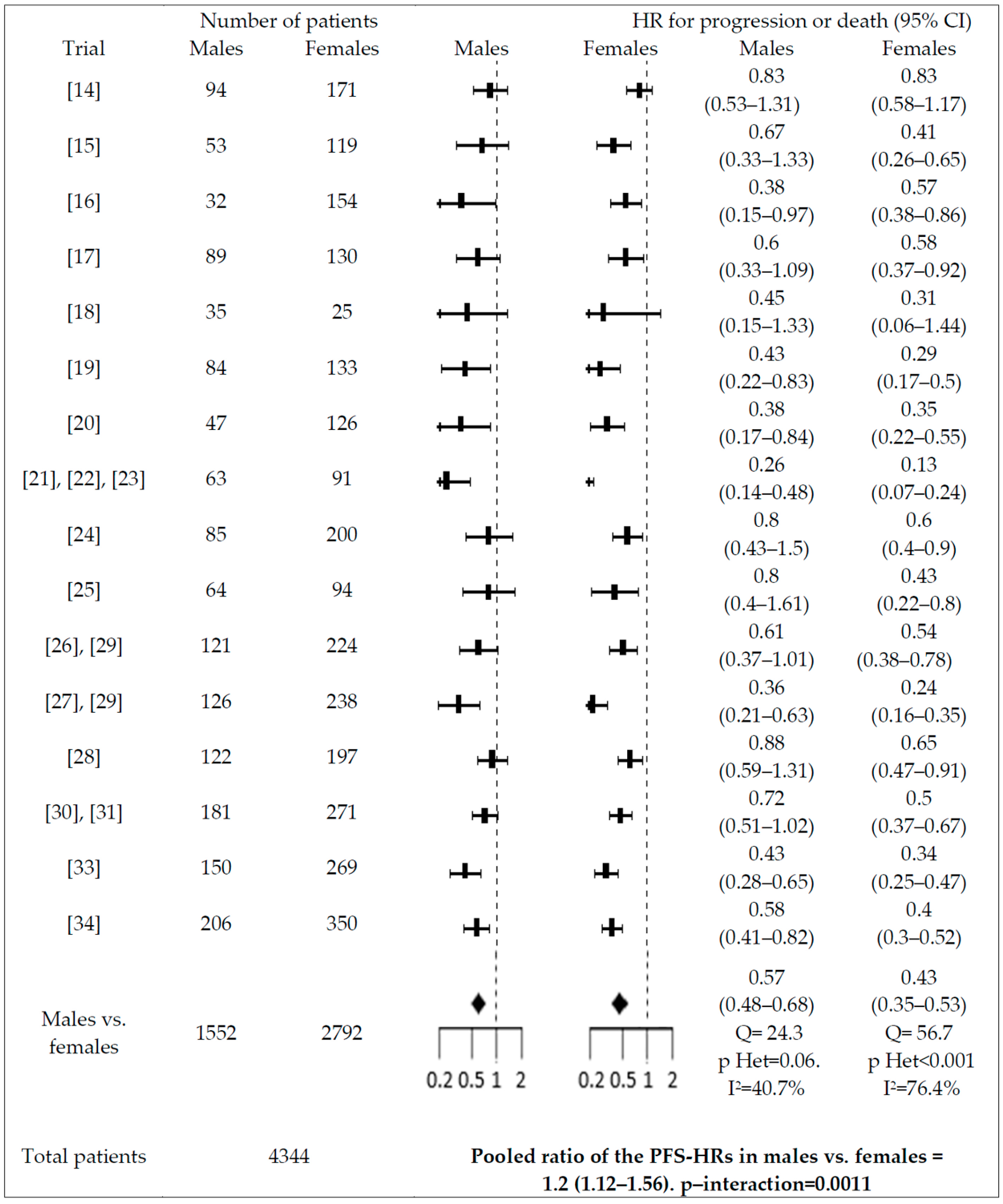
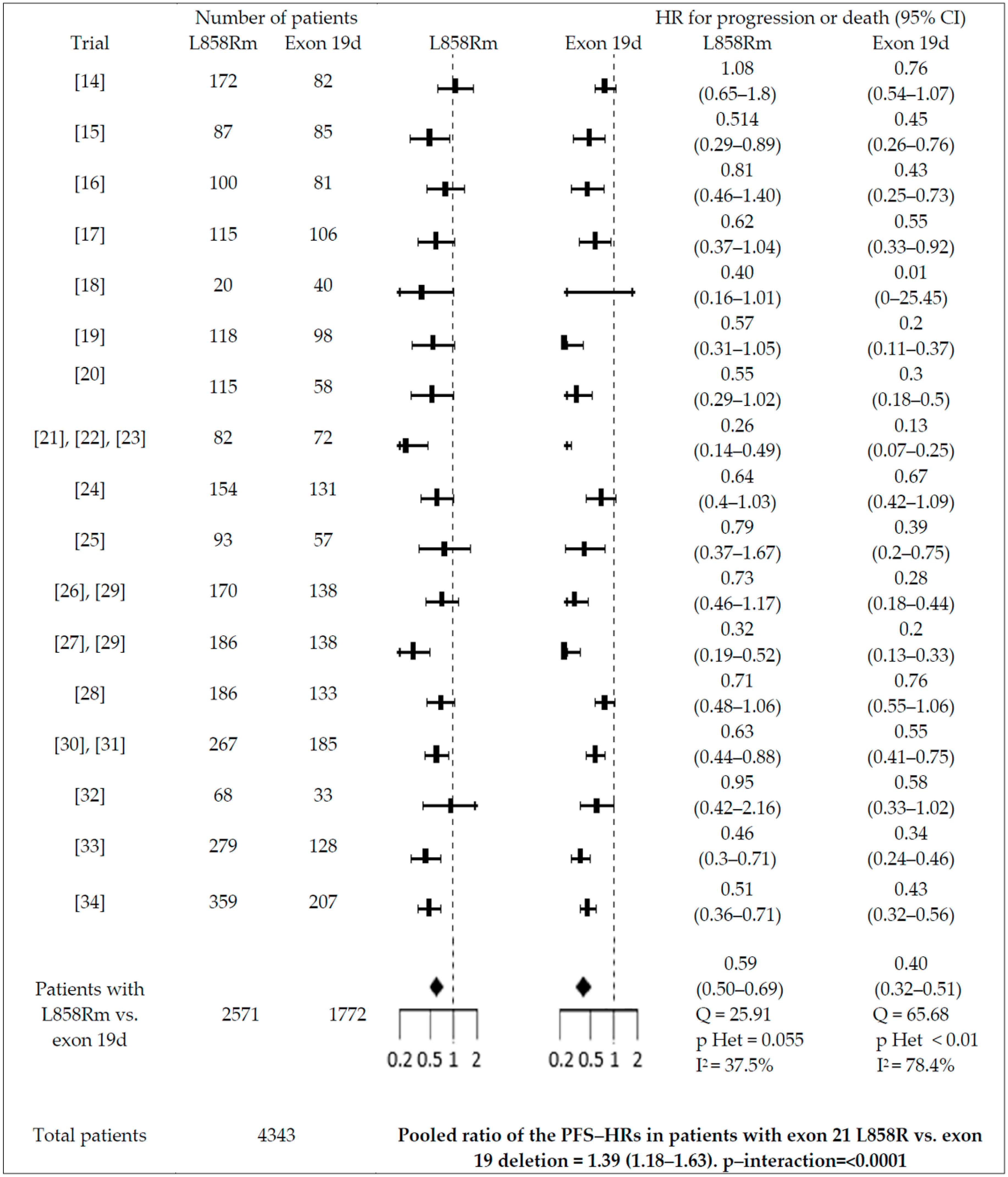
2.2. Quantitative Synthesis
3. Discussion
4. Methods
4.1. Search Strategy
4.2. Data Analysis
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Schiller, J.H.; Harrington, D.; Belani, C.P.; Langer, C.; Sandler, A.; Krook, J.; Zhu, J.; Johnson, D.H. Comparison of four chemotherapy regimens for advanced non–small-cell lung cancer. N. Engl. J. Med. 2002, 346, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Proto, C.; Ferrara, R.; Signorelli, D.; Lo Russo, G.; Galli, G.; Imbimbo, M.; Prelaj, A.; Zilembo, N.; Ganzinelli, M.; Pallavicini, L.M.; et al. Choosing wisely first line immunotherapy in non-small cell lung cancer (NSCLC): What to add and what to leave out. Cancer Treat. Rev. 2019, 75, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Castellanos, E.; Feld, E.; Horn, L. Driven by Mutations: The Predictive Value of Mutation Subtype in EGFR-Mutated Non–Small Cell Lung Cancer. J. Thorac. Oncol. 2017, 12, 612–623. [Google Scholar] [CrossRef] [PubMed]
- Le, T.; Gerber, D.E. Newer-generation egfr inhibitors in lung cancer: How are they best used? Cancers (Basel). 2019, 11, 366. [Google Scholar] [CrossRef] [PubMed]
- Inoue, A.; Yoshida, K.; Morita, S.; Imamura, F.; Seto, T.; Okamoto, I.; Nakagawa, K.; Yamamoto, N.; Muto, S.; Fukuoka, M. Characteristics and overall survival of EGFR mutation-positive non-small cell lung cancer treated with EGFR tyrosine kinase inhibitors: A retrospective analysis for 1660 Japanese patients. Jpn. J. Clin. Oncol. 2016, 46, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Pilotto, S.; Di Maio, M.; Peretti, U.; Kinspergher, S.; Brunelli, M.; Massari, F.; Sperduti, I.; Giannarelli, D.; De Marinis, F.; Tortora, G.; et al. Predictors of outcome for patients with lung adenocarcinoma carrying the epidermal growth factor receptor mutation receiving 1st-line tyrosine kinase inhibitors: Sensitivity and meta-regression analysis of randomized trials. Crit. Rev. Oncol. Hematol. 2014, 90, 134–145. [Google Scholar] [CrossRef] [PubMed]
- Stanic, K.; Zwitter, M.; Hitij, N.T.; Kern, I.; Sadikov, A.; Cufer, T. Brain metastases in lung adenocarcinoma: Impact of EGFR mutation status on incidence and survival. Radiol. Oncol. 2014, 48, 173–183. [Google Scholar] [CrossRef]
- Zhang, Y.; Sheng, J.; Kang, S.; Fang, W.; Yan, Y.; Hu, Z.; Hong, S.; Wu, X.; Qin, T.; Liang, W.; et al. Patients with exon 19 deletion were associated with longer progression-free survival compared to those with L858R mutation after first-line EGFR-TKIs for advanced non-small cell lung cancer: A meta-analysis. PLoS One 2014, 9, e107161. [Google Scholar] [CrossRef]
- Pinto, J.A.; Vallejos, C.S.; Raez, L.E.; Mas, L.A.; Ruiz, R.; Torres-Roman, J.S.; Morante, Z.; Araujo, J.M.; Gómez, H.L.; Aguilar, A.; et al. Gender and outcomes in non-small cell lung cancer: An old prognostic variable comes back for targeted therapy and immunotherapy? ESMO Open 2018, 3, e000344. [Google Scholar] [CrossRef]
- Hasegawa, Y.; Ando, M.; Maemondo, M.; Yamamoto, S.; Isa, S.-i.; Saka, H.; Kubo, A.; Kawaguchi, T.; Takada, M.; Rosell, R.; et al. The role of smoking status on the progression-free survival of non-small cell lung cancer patients harboring activating epidermal growth factor receptor (EGFR) mutations receiving first-line EGFR tyrosine kinase inhibitor versus platinum doublet chemother. Oncologist 2015, 20, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.K.; Davies, L.; Wu, Y.L.; Mitsudomi, T.; Inoue, A.; Rosell, R.; Zhou, C.; Nakagawa, K.; Thongprasert, S.; Fukuoka, M.; et al. Gefitinib or erlotinib vs chemotherapy for EGFR mutation-positive lung cancer: Individual patient data meta-analysis of overall survival. J. Natl. Cancer Inst. 2017. [Google Scholar] [CrossRef] [PubMed]
- Fisher, D.J.; Carpenter, J.R.; Morris, T.P.; Freeman, S.C.; Tierney, J.F. Meta-analytical methods to identify who benefits most from treatments: Daft, deluded, or deft approach? BMJ 2017, 356, j573. [Google Scholar] [CrossRef] [PubMed]
- Soria, J.C.; Wu, Y.L.; Nakagawa, K.; Kim, S.W.; Yang, J.J.; Ahn, M.J.; Wang, J.; Yang, J.C.H.; Lu, Y.; Atagi, S.; et al. Gefitinib plus chemotherapy versus placebo plus chemotherapy in EGFR-mutation-positive non-small-cell lung cancer after progression on first-line gefitinib (IMPRESS): A phase 3 randomised trial. Lancet Oncol. 2015, 16, 990–998. [Google Scholar] [CrossRef]
- Mitsudomi, T.; Morita, S.; Yatabe, Y.; Negoro, S.; Okamoto, I.; Tsurutani, J.; Seto, T.; Satouchi, M.; Tada, H.; Hirashima, T.; et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): An open label, randomised phase 3 trial. Lancet Oncol. 2010, 11, 121–128. [Google Scholar] [CrossRef]
- Wu, Y.L.; Saijo, N.; Thongprasert, S.; Yang, J.C.H.; Han, B.; Margono, B.; Chewaskulyong, B.; Sunpaweravong, P.; Ohe, Y.; Ichinose, Y.; et al. Efficacy according to blind independent central review: Post-hoc analyses from the phase III, randomized, multicenter, IPASS study of first-line gefitinib versus carboplatin/paclitaxel in Asian patients with EGFR mutation-positive advanced NSCLC. Lung Cancer 2017, 104, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Zhong, W.Z.; Wang, Q.; Mao, W.M.; Xu, S.T.; Wu, L.; Shen, Y.; Liu, Y.Y.; Chen, C.; Cheng, Y.; Xu, L.; et al. Gefitinib versus vinorelbine plus cisplatin as adjuvant treatment for stage II–IIIA (N1–N2) EGFR-mutant NSCLC (ADJUVANT/CTONG1104): A randomised, open-label, phase 3 study. Lancet Oncol. 2018, 19, 139–148. [Google Scholar] [CrossRef]
- Li, N.; Ou, W.; Ye, X.; Sun, H.B.; Zhang, L.; Fang, Q.; Zhang, S.L.; Wang, B.X.; Wang, S.Y. Pemetrexed-carboplatin adjuvant chemotherapy with or without gefitinib in resected stage IIIA-N2 non-small cell lung cancer harbouring EGFR mutations: A randomized, phase II study. Ann. Surg. Oncol. 2014, 21, 2091–2096. [Google Scholar] [CrossRef]
- Wu, Y.L.; Zhou, C.; Liam, C.K.; Wu, G.; Liu, X.; Zhong, Z.; Lu, S.; Cheng, Y.; Han, B.; Chen, L.; et al. First-line erlotinib versus gemcitabine/cisplatin in patients with advanced EGFR mutation-positive non-small-cell lung cancer: Analyses from the phase III, randomized, open-label, ENSURE study. Ann. Oncol. 2015, 26, 1883–1889. [Google Scholar] [CrossRef]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Zhou, C.; Wu, Y.L.; Chen, G.; Feng, J.; Liu, X.Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): A multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011, 12, 735–742. [Google Scholar] [CrossRef]
- Chen, G.; Feng, J.; Zhou, C.; Wu, Y.L.; Liu, X.Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Quality of life (QoL) analyses from optimal (CTONG-0802), a phase III, randomised, open-label study of first-line erlotinib versus chemotherapy in patients with advanced EGFR mutation-positive non-small-cell lung cancer (NSCLC). Ann. Oncol. 2013, 24, 1615–1622. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Wu, Y.L.; Chen, G.; Feng, J.; Liu, X.Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Final overall survival results from a randomised, phase III study of erlotinib versus chemotherapy as first-line treatment of EGFR mutation-positive advanced non-small-cell lung cancer (OPTIMAL, CTONG-0802). Ann. Oncol. 2015, 26, 1877–1883. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.K.; Wang, L.; Han, B.H.; Li, W.; Yu, P.; Liu, Y.P.; Ding, C.M.; Song, X.; Ma, Z.Y.; Ren, X.L.; et al. First-line icotinib versus cisplatin/pemetrexed plus pemetrexed maintenance therapy for patients with advanced EGFR mutation-positive lung adenocarcinoma (CONVINCE): A phase 3, open-label, randomized study. Ann. Oncol. 2017, 28, 2443–2450. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.J.; Zhou, C.; Huang, Y.; Feng, J.; Lu, S.; Song, Y.; Huang, C.; Wu, G.; Zhang, L.; Cheng, Y.; et al. Icotinib versus whole-brain irradiation in patients with EGFR-mutant non-small-cell lung cancer and multiple brain metastases (BRAIN): A multicentre, phase 3, open-label, parallel, randomised controlled trial. Lancet Respir. Med. 2017. [Google Scholar] [CrossRef]
- Sequist, L.V.; Yang, J.C.H.; Yamamoto, N.; O’Byrne, K.; Hirsh, V.; Mok, T.; Geater, S.L.; Orlov, S.; Tsai, C.M.; Boyer, M.; et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J. Clin. Oncol. 2013, 31, 3327–3334. [Google Scholar] [CrossRef]
- Wu, Y.L.; Zhou, C.; Hu, C.P.; Feng, J.; Lu, S.; Huang, Y.; Li, W.; Hou, M.; Shi, J.H.; Lee, K.Y.; et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): An open-label, randomised phase 3 trial. Lancet Oncol. 2014, 15, 213–222. [Google Scholar] [CrossRef]
- Park, K.; Tan, E.H.; O’Byrne, K.; Zhang, L.; Boyer, M.; Mok, T.; Hirsh, V.; Yang, J.C.H.; Lee, K.H.; Lu, S.; et al. Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7): A phase 2B, open-label, randomised controlled trial. Lancet Oncol. 2016, 17, 577–589. [Google Scholar] [CrossRef]
- Yang, J.C.-H.; Wu, Y.-L.; Schuler, M.; Sebastian, M.; Popat, S.; Yamamoto, N.; Zhou, C.; Hu, C.-P.; O’Byrne, K.; Feng, J.; et al. Afatinib versus cisplatin-based chemotherapy for EGFR mutation-positive lung adenocarcinoma (LUX-Lung 3 and LUX-Lung 6): Analysis of overall survival data from two randomised, phase 3 trials. Lancet. Oncol. 2015, 16, 141–151. [Google Scholar] [CrossRef]
- Wu, Y.L.; Cheng, Y.; Zhou, X.; Lee, K.H.; Nakagawa, K.; Niho, S.; Tsuji, F.; Linke, R.; Rosell, R.; Corral, J.; et al. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): A randomised, open-label, phase 3 trial. Lancet Oncol. 2017, 8, 1454–1466. [Google Scholar] [CrossRef]
- Mok, T.S.; Cheng, Y.; Zhou, X.; Lee, K.H.; Nakagawa, K.; Niho, S.; Lee, M.; Linke, R.; Rosell, R.; Corral, J.; et al. Improvement in overall survival in a randomized study that compared dacomitinib with gefitinib in patients with advanced non–small-cell lung cancer and EGFR-activating mutations. J. Clin. Oncol. 2018, 36, 2244–2250. [Google Scholar] [CrossRef] [PubMed]
- Ramalingam, S.S.; O’Byrne, K.; Boyer, M.; Mok, T.; Jänne, P.A.; Zhang, H.; Liang, J.; Taylor, I.; Sbar, E.I.; Paz-Ares, L. Dacomitinib versus erlotinib in patients with EGFR-mutated advanced nonsmall-cell lung cancer (NSCLC): Pooled subset analyses from two randomized trials. Ann. Oncol. 2016, 27, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.-L.; Ahn, M.-J.; Garassino, M.C.; Kim, H.R.; Ramalingam, S.S.; Shepherd, F.A.; He, Y.; Akamatsu, H.; Theelen, W.S.M.E.; et al. Osimertinib or Platinum-Pemetrexed in EGFR T790M-Positive Lung Cancer. N. Engl. J. Med. 2017, 376, 629–640. [Google Scholar] [CrossRef] [PubMed]
- Soria, J.-C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in untreated EGFR-mutated advanced non–small-cell lung cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.I.; Lim, H.; Moon, A. Sex differences in cancer: Epidemiology, genetics and therapy. Biomol. Ther. 2018, 26, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Gabriele, L.; Buoncervello, M.; Ascione, B.; Bellenghi, M.; Matarrese, P.; Caré, A. The gender perspective in cancer research and therapy: Novel insights and on-going hypotheses. Ann. Ist. Super. Sanita 2016, 52, 213–222. [Google Scholar] [PubMed]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Tseng, C.-H.; Chiang, C.-J.; Tseng, J.-S.; Yang, T.-Y.; Hsu, K.-H.; Chen, K.-C.; Wang, C.-L.; Chen, C.-Y.; Yen, S.-H.; Tsai, C.-M.; et al. EGFR mutation, smoking, and gender in advanced lung adenocarcinoma. Oncotarget 2017, 8, 98384–98393. [Google Scholar] [CrossRef]
- Wang, L.; Cao, Y.; Ren, M.; Chen, A.; Cui, J.; Sun, D.J.; Gu, W. Sex Differences in Hazard Ratio During Drug Treatment of Non–small-cell Lung Cancer in Major Clinical Trials: A Focused Data Review and Meta-analysis. Clin. Ther. 2017, 39, 34–54. [Google Scholar] [CrossRef][Green Version]
- Conforti, F.; Pala, L.; Bagnardi, V.; De Pas, T.; Martinetti, M.; Viale, G.; Gelber, R.D.; Goldhirsch, A. Cancer immunotherapy efficacy and patients’ sex: A systematic review and meta-analysis. Lancet Oncol. 2018, 19, 737–746. [Google Scholar] [CrossRef]
- Des Guetz, G.; Landre, T.; Uzzan, B.; Chouahnia, K.; Nicolas, P.; Morere, J.F. Is there a survival benefit of first-line epidermal growth factor receptor tyrosine-kinase inhibitor monotherapy versus chemotherapy in patients with advanced non-small-cell lung cancer?: A meta-analysis. Target. Oncol. 2016, 11, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Gettinger, S.; Hellmann, M.D.; Chow, L.Q.M.; Borghaei, H.; Antonia, S.; Brahmer, J.R.; Goldman, J.W.; Gerber, D.E.; Juergens, R.A.; Shepherd, F.A.; et al. Nivolumab Plus Erlotinib in Patients With EGFR-Mutant Advanced NSCLC. J. Thorac. Oncol. 2018, 13, 1363–1372. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trial | Phase | Setting (0 = Adjuvant; 1 = First Line; 2 = Second or Subsequent Lines) | Jadad Score (0–5) | No. Evaluable pts | Age in Years (Range) | Median Follow-up in Months | Intervention | Control | HR for Progression—95% CI | HR for Death—95% CI | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [14] | 3 | 2 | 5 | 265 | 59 (33–79) | GEFITINIB + CISPLATIN + PEMETREXED | PLACEBO + CISPLATIN + PEMETREXED | 0.86 (0.65–1.13) | ||||
| [15] | 3 | 1 | 3 | 172 | 64 (34–75) | 2.7 | GEFITINIB | CISPLATIN + DOCETAXEL | 0.48 (0.33–0.71) | 1.63 (0.75–3.58) | ||
| [16] | 3 | 1 | 3 | 186 | GEFITINIB | CARBOPLATIN + PACLITAXEL | 0.54 (0.38–0.79) | |||||
| [17] | 3 | 0 | 3 | 219 | 59 (26–76) | 36.5 | GEFITINIB | VINORELBINE + CISPLATIN | 0.58 (0.4–0.83) | |||
| [18] | 2 | 0 | 3 | 60 | 57 (32–78) | 30.6 | GEFITINIB | PEMETREXED + CARBOPLATIN | 0.37 (0.16–0.85) | |||
| [19] | 3 | 1 | 3 | 217 | 56 (30–79) | 28.9/27.1 | ERLOTINIB | GEMCITABINE + CISPLATIN | 0.42 (0.27–0.66) | 0.91 (0.63–1.31) | ||
| [20] | 3 | 1 | 3 | 173 | 65 (24–72) | 18.9/14.4 | ERLOTINIB | PLATINUM + DOCETAXEL/GEMCITABINE | 0.37 (0.25–0.54) | 1.04 (0.65–1.68) | ||
| [21,22,23] | 3 | 1 | 3 | 154 | 54 (31–78) | ERLOTINIB | GEMCITABINE + CARBOPLATIN | 0.16 (0.11–0.26) | 1.19 (0.83–1.71) | |||
| [24] | 3 | 1 | 3 | 285 | 56 (30–76) | 18 | ICOTINIB | CISPLATIN + PEMETREXED | 0.65 (0.46–0.91) | 0.97 (0.72–1.31) | ||
| [25] | 3 | 1 | 3 | 158 | 58 (48–64) | 16.5 | ICOTINIB | WBI | 0.56 (0.36–0.9) | 0.93 (0.6–1.44) | ||
| [26,29] | 3 | 1 | 3 | 345 | 61 (28–86) | 16.4 | AFATINIB | CISPLATIN + PEMETREXED | 0.58 (0.43–0.78) | 0.78 (0.58–1.06) | ||
| [27,29] | 3 | 1 | 3 | 364 | 58 (49–65) | 16 | AFATINIB | GEMCITABINE + CISPLATIN | 0.28 (0.2–0.39) | 0.83 (0.63–1.09) | ||
| [28] | 2 | 1 | 3 | 319 | 63 (30–89) | AFATINIB | GEFITINIB | 0.73 (0.57–0.95) | ||||
| [30,31] | 3 | 1 | 3 | 452 | 61 (53–68) | 22.1 (PFS) 31.3 (OS) | DACOMITINIB | GEFITINIB | 0.58 (0.4–0.73) | 0.80 (0.61–1.04) | ||
| [32] ARCHER 1009 | 3 | 2 | 5 | 121 | 61 (32–84) | DACOMITINIB | ERLOTINIB | 0.71 (0.45–1.12) | 0.95 (0.59–1.53) | |||
| [32] A7471028 | 2 | 2 | 3 | 62 (34–79) | ||||||||
| [33] | 3 | 2 | 3 | 419 | 62 (20–90) | 8.3 | OSIMERTINIB | PLATINUM + PEMETREXED | 0.3 (0.23–0.41) | |||
| [34] | 3 | 1 | 5 | 556 | 64 (26–93) | 15 | OSIMERTINIB | GEFITINIB OR ERLOTINIB | 0.46 (0.37–0.57) | 0.63 (0.45–0.88) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buonerba, C.; Iaccarino, S.; Dolce, P.; Pagliuca, M.; Izzo, M.; Scafuri, L.; Costabile, F.; Riccio, V.; Ribera, D.; Mucci, B.; et al. Predictors of Outcomes in Patients with EGFR-Mutated Non-Small Cell Lung Cancer Receiving EGFR Tyrosine Kinase Inhibitors: A Systematic Review and Meta-Analysis. Cancers 2019, 11, 1259. https://doi.org/10.3390/cancers11091259
Buonerba C, Iaccarino S, Dolce P, Pagliuca M, Izzo M, Scafuri L, Costabile F, Riccio V, Ribera D, Mucci B, et al. Predictors of Outcomes in Patients with EGFR-Mutated Non-Small Cell Lung Cancer Receiving EGFR Tyrosine Kinase Inhibitors: A Systematic Review and Meta-Analysis. Cancers. 2019; 11(9):1259. https://doi.org/10.3390/cancers11091259
Chicago/Turabian StyleBuonerba, Carlo, Simona Iaccarino, Pasquale Dolce, Martina Pagliuca, Michela Izzo, Luca Scafuri, Ferdinando Costabile, Vittorio Riccio, Dario Ribera, Brigitta Mucci, and et al. 2019. "Predictors of Outcomes in Patients with EGFR-Mutated Non-Small Cell Lung Cancer Receiving EGFR Tyrosine Kinase Inhibitors: A Systematic Review and Meta-Analysis" Cancers 11, no. 9: 1259. https://doi.org/10.3390/cancers11091259
APA StyleBuonerba, C., Iaccarino, S., Dolce, P., Pagliuca, M., Izzo, M., Scafuri, L., Costabile, F., Riccio, V., Ribera, D., Mucci, B., Carrano, S., Picozzi, F., Bosso, D., Formisano, L., Bianco, R., De Placido, S., & Di Lorenzo, G. (2019). Predictors of Outcomes in Patients with EGFR-Mutated Non-Small Cell Lung Cancer Receiving EGFR Tyrosine Kinase Inhibitors: A Systematic Review and Meta-Analysis. Cancers, 11(9), 1259. https://doi.org/10.3390/cancers11091259