Radiomics and Texture Analysis in Laryngeal Cancer. Looking for New Frontiers in Precision Medicine through Imaging Analysis

 , ,
, ,
Abstract
:1. Introduction
1.1. Radiomics and Texture Analysis Software Available
1.1.1. Open-Source Software
- IBEX (Imaging Biomarker Explorer): developed by Zhang et al., described as an “open infrastructure software platform that flexibly supports common radiomics workflow tasks such as multimodality image data import and review, development of feature extraction algorithms, model validation, and consistent data sharing among multiple institutions.” [39]. IBEX is compatible with CT, PET, and MRI modalities.
- MazDa is another open-source solution for texture analysis that has been validated through multi-institutional studies [40]. This software is built primarily for MRI texture analysis and supports various feature selection methods for model generation.
- Chang-Gung Image Texture Analysis (CGITA) is yet another open-source texture analysis tool, built in the MATLAB environment. The software supports numerous heterogeneity indices, user-defined calculations, and batch processing with a focus on molecular imaging. CGITA supports CT, PET, and MRI images [41].
1.1.2. In-House Development of Radiomic Analysis
1.1.3. Commercial Solutions Software for Radiomic Analysis
- TexRAD is a commercial software that uses a LoG special filter to delineate fine, intermediate, and coarse textures in a ROI for subsequent analysis. This software contains various decision support tools for thoracic and gastrointestinal imaging and has also demonstrated applicability in head and neck cancer textural analysis [46].
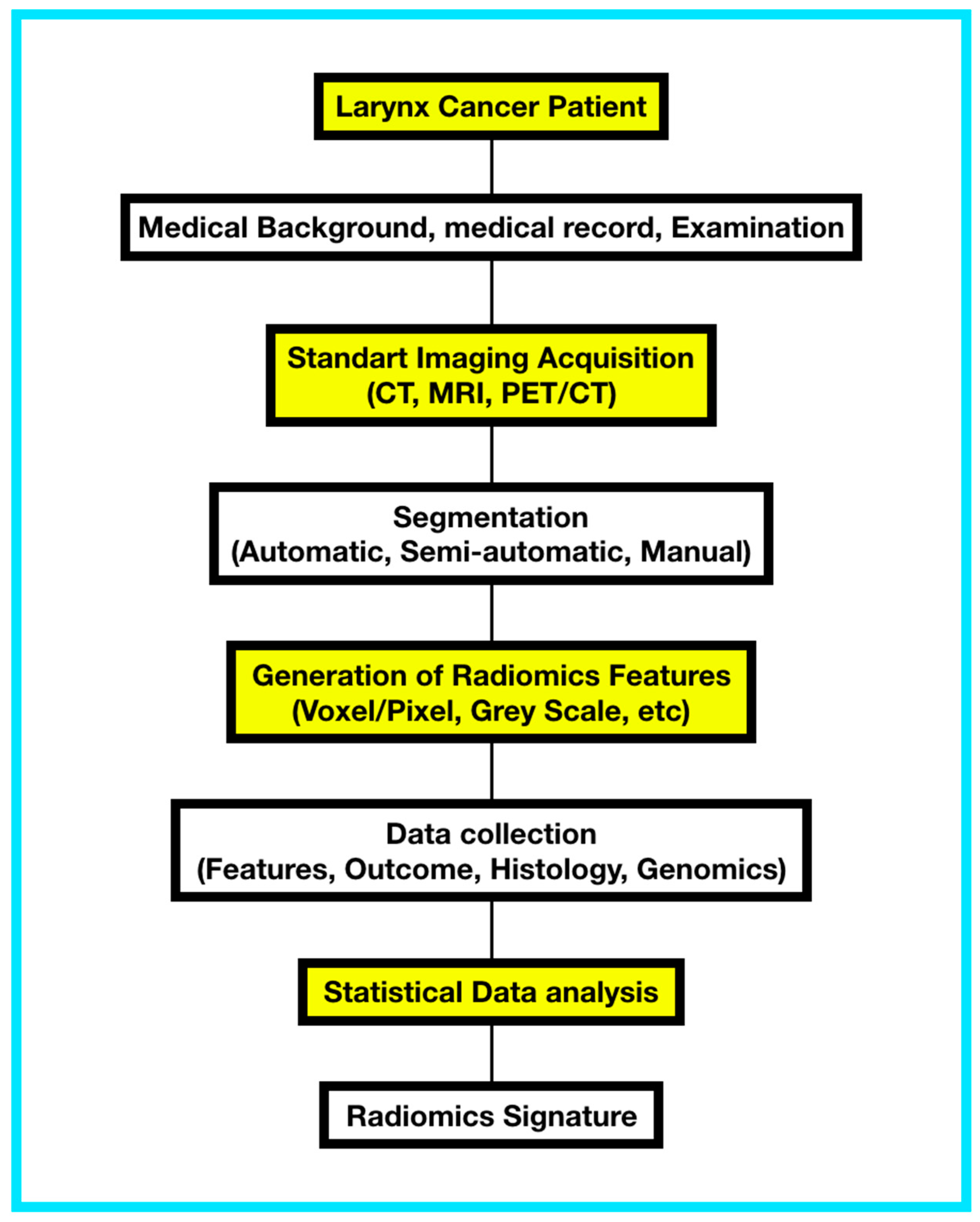
1.2. Radiomics Workflow
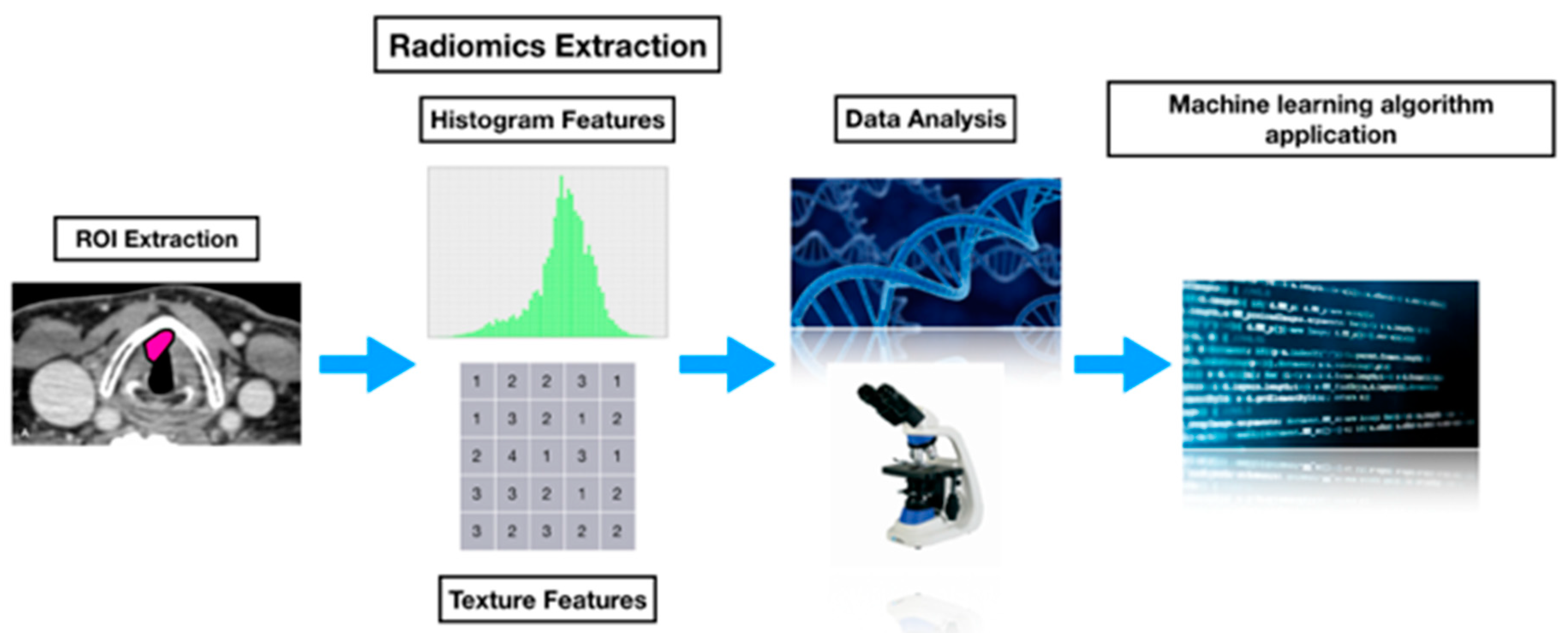
- High-quality, standardized imaging data must be acquired. The region of interest (ROI), represented by the tumor, metastasis, or parts of it is manually/automatically identified, and the volume of interest (VOI) is defined.
- Collections of datasets from clinical practice can be gathered to perform retrospective analysis in order to obtain the basic radiomic feature extraction and statistical and predictive systems for prospective analysis.
- Definition and segmentation of the ROI: In each subject, capture of radiomic imaging data can be performed using a manual, semiautomatic or automatic approach.
- Radiomic feature extraction: These features are extracted from the tumor ROI concerning information about image shape, intensity, and texture. Features can be constructed by statistical means, such as co-occurrence matrices, or by selecting the coefficients of image transformations, such as wavelet-based image decomposition and analysis.
- Multi-source fusion data analysis: Defining associations between radiomic features and clinical data, outcome, treatment responses, histopathological data. Mixed analysis, e.g., including gene expression (“radiogenomics”) is achieved through data fusion schemes like canonical correlation analysis (CCA).
- Machine learning algorithm application: Predictive/discriminant functions can be trained and validated over the radiomic feature collected from retrospective data in order to be refined and applied in prospective studies. Model building procedures include logistic regression, support vector machines (SVM), random forests (RF), and artificial neural networks including deep learning approaches. Radiomics can be fused with survival analysis for prognostic studies. [8,47,48,49]. (Figure 1)
2. Radiomics and Laryngeal Cancer
- Tumor segmentation and pathologic classification in surgical and non-surgical patients.
- Anatomical extension: Paraglottic space, thyroid cartilage, cryco-aritenoid joint, cryco-thyroid membrane.
- Risk stratification.
- Prognostic or predictive biomarker.
- Monitorization of alterations in normal tissue as a sequelae of radiotherapy dose deposition.
3. Precision Medicine, Big Data, and Machine Learning in Larynx Cancer
4. Radiomics Limitations
4.1. Imaging Acquisition
4.2. Image Segmentation
4.3. Feature Extraction
4.4. Image Processing
5. Future Direction
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Allen, C.; Barber, R.M.; Barregard, L.; Bhutta, Z.A.; Brenner, H.; Dicker, D.J.; Chimed-Orchir, O.; Dandona, R.; et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: A systematic analysis for the global burden of disease study. JAMA Oncol. 2017, 3, 524–548. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Scheckenbach, K. Radiomics: Big Data Instead of Biopsies in the Future? Laryngorhinootologie 2018, 97, S114–S141. [Google Scholar] [PubMed]
- Ulrich, E.J.; Menda, Y.; Ponto, L.L.; Anderson, C.M.; Smith, B.J.; Sunderland, J.J.; Graham, M.M.; Buatti, J.M.; Beichel, R.R. FLT PET Radiomics for Response Prediction to Chemoradiation Therapy in Head and Neck Squamous Cell Cancer. Tomography 2019, 5, 161–169. [Google Scholar] [PubMed]
- Guezennec, C.; Robin, P.; Orlhac, F.; Bourhis, D.; Delcroix, O.; Gobel, Y.; Rousset, J.; Schick, U.; Salaün, P.Y.; Abgral, R. Prognostic value of textural indices extracted from pretherapeutic 18-F FDG-PET/CT in head and neck squamous cell carcinoma. Head Neck 2019, 41, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, V.; Gu, Y.; Basu, S.; Berglund, A.; Eschrich, S.A.; Schabath, M.B.; Forster, K.; Aerts, H.J.; Dekker, A.; Fenstermacher, D.; et al. Radiomics: The process and the challenges. Magn. Reson. Imaging 2012, 30, 1234–1248. [Google Scholar] [CrossRef] [PubMed]
- Aerts, H.J.; Velazquez, E.R.; Leijenaar, R.T.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006, Erratum in: Nat. Commun. 2014, 5, 4644. [Google Scholar] [CrossRef]
- Alic, L.; Niessen, W.J.; Veenland, J.F. Quantification of heterogeneity as a biomarker in tumor imaging: A systematic review. PLoS ONE 2014, 9, e110300. [Google Scholar] [CrossRef]
- Carvalho, S.; Leijenaar, R.T.; Velazquez, E.R.; Oberije, C.; Parmar, C.; Van Elmpt, W.; Reymen, B.; Troost, E.G.; Oellers, M.; Dekker, A.; et al. Prognostic value of metabolic metrics extracted from baseline positron emission tomography images in non-small cell lung cancer. Acta Oncol. 2013, 52, 1398–1404. [Google Scholar] [CrossRef]
- Gevaert, O.; Mitchell, L.A.; Achrol, A.S.; Xu, J.; Echegaray, S.; Steinberg, G.K.; Cheshier, S.H.; Napel, S.; Zaharchuk, G.; Plevritis, S.K. Glioblastoma multiforme: Exploratory radiogenomic analysis by using quantitative image features. Radiology 2014, 273, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Hatt, M.; Tixier, F.; Le Rest, C.C.; Pradier, O.; Visvikis, D. Robustness of intratumour 18F-FDG PET uptake heterogeneity quantification for therapy response prediction in oesophageal carcinoma. Eur. J. Nucl. Med. Mol Imaging 2013, 40, 1662–1671. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Poisson, L.M.; Gutman, D.; Scarpace, L.; Hwang, S.N.; Holder, C.A.; Wintermark, M.; Rao, A.; Colen, R.R.; Kirby, J.; et al. Outcome prediction in patients with glioblastoma by using imaging, clinical, and genomic biomarkers: Focus on the nonenhancing component of the tumor. Radiology 2014, 272, 484–493. [Google Scholar] [CrossRef] [PubMed]
- Leijenaar, R.T.; Carvalho, S.; Velazquez, E.R.; Van Elmpt, W.J.; Parmar, C.; Hoekstra, O.S.; Hoekstra, C.J.; Boellaard, R.; Dekker, A.L.; Gillies, R.J.; et al. Stability of FDG-PET radiomics features: An integrated analysis of test-retest and inter-observer variability. Acta Oncol. 2013, 52, 1391–1397. [Google Scholar] [CrossRef] [PubMed]
- Parmar, C.; Velazquez, E.R.; Leijenaar, R.; Jermoumi, M.; Carvalho, S.; Mak, R.H.; Mitra, S.; Shankar, B.U.; Kikinis, R.; Haibe-Kains, B.; et al. Robust radiomics feature quantification using semiautomatic volumetric segmentation. PLoS ONE 2014, 9, e102107. [Google Scholar] [CrossRef]
- Hunter, L.A.; Krafft, S.; Stingo, F.; Choi, H.; Martel, M.K.; Kry, S.F. High quality machine-robust image features: Identification in nonsmall cell lung cancer computed tomography images. Med. Phys. 2013, 40, 121916. [Google Scholar] [CrossRef]
- Basu, S.; Hall, L.O.; Goldgof, D.B.; Gu, Y.; Kumar, V.; Choi, J.; Gillies, R.J.; Gatenby, R.A. Developing a classifier model for lung tumors in CT-scan images. In Proceedings of the 2011 IEEE International Conference on Systems, Man, and Cybernetics, Anchorage, AK, USA, 9–12 October 2011; pp. 1306–1312. [Google Scholar]
- Parmar, C.; Leijenaar, R.T.; Grossmann, P.; Velazquez, E.R.; Bussink, J.; Rietveld, D.; Rietbergen, M.M.; Haibe-Kains, B.; Lambin, P.; Aerts, H.J. Radiomic feature clusters and prognostic signatures specific for lung and head & neck cancer. Sci. Rep. 2015, 5, 11044. [Google Scholar]
- Ganeshan, B.; Goh, V.; Mandeville, H.C.; Ng, Q.S.; Hoskin, P.J.; Miles, K.A. Non-small cell lung cancer: Histopathologic correlates for texture parameters at CT. Radiology 2013, 266, 326–336. [Google Scholar] [CrossRef]
- Cistaro, A.; Quartuccio, N.; Mojtahedi, A.; Fania, P.; Filosso, P.L.; Campenni, A.; Ficola, U.; Baldari, S. Prediction of 2 years-survival in patients with stage I and II non-small cell lung cancer utilizing 18F-FDG PET/CT SUV quantifica. Radiol. Oncol. 2013, 47, 219–223. [Google Scholar] [CrossRef]
- Cook, G.J.; Yip, C.; Siddique, M.; Goh, V.; Chicklore, S.; Roy, A.; Marsden, P.; Ahmad, S.; Landau, D. Are pretreat- ment 18F-FDG PET tumor textural features in non-small cell lung cancer associated with response and survival after chemoradiotherapy? J. Nucl. Med. 2013, 541, 19–26. [Google Scholar] [CrossRef]
- Hawkins, S.H.; Korecki, J.N.; Balagurunathan, Y.; Gu, Y.; Kumar, V.; Basu, S.; Hall, L.O.; Goldgof, D.B.; Gatenby, R.A.; Gillies, R.J. Predicting Outcomes of Nonsmall Cell Lung Cancer Using CT Image Features. IEEE Access 2014, 2, 1418–1426. [Google Scholar] [CrossRef]
- Ganeshan, B.; Abaleke, S.; Young, R.C.; Chatwin, C.R.; Miles, K.A. Texture analysis of non-small cell lung cancer on unenhanced computed tomography: Initial evidence for a relationship with tumour glucose metabolism and stage. Cancer Imaging 2010, 10, 137. [Google Scholar] [CrossRef]
- Coroller, T.P.; Grossmann, P.; Hou, Y.; Velazquez, E.R.; Leijenaar, R.T.; Hermann, G.; Lambin, P.; Haibe-Kains, B.; Mak, R.H.; Aerts, H.J. CT-based radiomic signature predicts distant metastasis in lung adenocarcinoma. Radiother. Oncol. 2015, 114, 345–350. [Google Scholar] [CrossRef]
- Pickles, M.D.; Manton, D.J.; Lowry, M.; Turnbull, L.W. Prognostic value of pre-treat- ment DCE-MRI parameters in predicting disease free and overall survival for breast cancer patients undergoing neoadjuvant chemotherapy. Eur. J. Radiol. 2009, 71, 498–505. [Google Scholar] [CrossRef]
- Segal, E.; Sirlin, C.B.; Ooi, C.; Adler, A.S.; Gollub, J.; Chen, X.; Chan, B.K.; Matcuk, G.R.; Barry, C.T.; Chang, H.Y.; et al. Decoding global gene expression programs in liver cancer by noninvasive imaging. Nat. Biotechnol. 2007, 25, 675–680. [Google Scholar] [CrossRef]
- Nicolasjilwan, M.; Hu, Y.; Yan, C.; Meerzaman, D.; Holder, C.A.; Gutman, D.; Jain, R.; Colen, R.; Rubin, D.L.; Zinn, P.O.; et al. Addition of MR imaging features and genetic biomarkers strengthens glioblastoma survival prediction in TCGA patients. J. Neuroradiol. 2015, 42, 212–221. [Google Scholar] [CrossRef]
- Lambin, P.; Van Stiphout, R.G.; Starmans, M.H.; Rios-Velazquez, E.; Nalbantov, G.; Aerts, H.J.; Roelofs, E.; Van Elmpt, W.; Boutros, P.C.; Granone, P.; et al. Predicting outcomes in radiation oncology—Multifactorial decision support systems. Nat. Rev. Clin. Oncol. 2013, 10, 27–40. [Google Scholar] [CrossRef]
- Haralick, R.M.; Shanmugam, K.; Dinstein, I. Textural Features for Image Classification. IEEE Trans. Syst. Man Cybern. 1973, SMC–3, 610–621. [Google Scholar] [CrossRef]
- Castellano, G.; Bonilha, L.; Li, L.M.; Cendes, F. Texture analysis of medical images. Clin. Radiol. 2004, 59, 1061–1069. [Google Scholar] [CrossRef]
- Tang, X. Texture information in run-length matrices. IEEE Trans. Image Process. 1998, 7, 1602–1609. [Google Scholar] [CrossRef] [Green Version]
- Soh, L.K. Texture analysis of SAR sea ice imagery using gray level co-occurrence matrices. IEEE Trans. Geosci. Remote Sens. 1999, 37, 780–795. [Google Scholar] [CrossRef] [Green Version]
- Galloway, M.M. Texture analysis using gray level run lengths. Comput. Graph. Image Process. 1975, 4, 172–179. [Google Scholar] [CrossRef]
- Lam, S.W. Texture feature extraction using gray level gradient based co-occurence matrices. In Proceedings of the 1996 IEEE International Conference on Systems, Man and Cybernetics, Information Intelligence and Systems (Cat. No.96CH35929). Beijing, China, 14–17 October 1996; Volume 1, pp. 267–271. [Google Scholar]
- Miles, K.A.; Ganeshan, B.; Hayball, M.P. CT texture analysis using the filtration-histogram method: What do the measurements mean? Cancer Imaging 2013, 13, 400–406. [Google Scholar] [CrossRef]
- Zhang, X.; Stockel, J.; Wolf, M.; Cathier, P.; McLennan, G.; Hoffman, E.A.; Sonka, M. A new method for spherical object detection and its application to computer aided detection of pulmonary nodules in CT images. Med. Image Comput. Comput. Assist. Interv. 2007, 10, 842–849. [Google Scholar]
- Guo, X.; Liu, X.; Wang, H.; Liang, Z.; Wu, W.; He, Q.; Li, K.; Wang, W. Enhanced CT images by the wavelet transform improving diagnostic accuracy of chest nodules. J. Digit. Imaging 2011, 24, 44–49. [Google Scholar] [CrossRef]
- Bastawrous, H.A. Detection of Ground Glass Opacities in Lung CT Images Using Gabor Filters and Neural Networks. In Proceedings of the 2005 IEEE Instrumentation and Measurement Technology Conference Proceedings, Ottawa, ON, Canada, 16–19 May 2005; Volume 1, pp. 251–256. [Google Scholar]
- Zhang, L.; Fried, D.V.; Fave, X.J.; Hunter, L.A.; Yang, J.; Court, L.E. IBEX: An open infrastructure software platform to facilitate collaborative work in radiomics. Med. Phys. 2015, 42, 1341–1353. [Google Scholar] [CrossRef]
- Brown, A.M.; Nagala, S.; McLean, M.A.; Lu, Y.; Scoffings, D.; Apte, A.; Gonen, M.; Stambuk, H.E.; Shaha, A.R.; Tuttle, R.M.; et al. Multi-institutional validation of a novel textural analysis tool for preoperative stratification of suspected thyroid tumors on diffusion-weighted MRI. Magn. Reson. Med. 2016, 75, 1708–1716. [Google Scholar] [CrossRef]
- Fang, Y.H.; Lin, C.Y.; Shih, M.J.; Wang, H.M.; Ho, T.Y.; Liao, C.T.; Yen, T.C. Development and evaluation of an open-source software package “CGITA” for quantifying tumor heterogeneity with molecular images. Biomed. Res. Int. 2014, 2014, 248505. [Google Scholar] [CrossRef]
- Buch, K.; Fujita, A.; Li, B.; Kawashima, Y.; Qureshi, M.M.; Sakai, O. Using Texture Analysis to Determine Human Papillomavirus Status of Oropharyngeal Squamous Cell Carcinomas on CT. AJNR Am. J. Neuroradiol. 2015, 36, 1343–1348. [Google Scholar] [CrossRef] [Green Version]
- Alobaidli, S.; McQuaid, S.; South, C.; Prakash, V.; Evans, P.; Nisbet, A. The role of texture analysis in imaging as an outcome predictor and potential tool in radiotherapy treatment planning. Br. J. Radiol. 2014, 87, 20140369. [Google Scholar] [CrossRef] [Green Version]
- El Naqa, I.; Grigsby, P.W.; Apte, A.; Kidd, E.; Donnelly, E.; Khullar, D.; Chaudhari, S.; Yang, D.; Schmitt, M.; Laforest, R.; et al. Exploring feature- based approaches in PET images for predicting cancer treatment outcomes. Pattern Recognit. 2009, 42, 1162–1171. [Google Scholar] [CrossRef]
- Jansen, J.F.; Lu, Y.; Gupta, G.; Lee, N.Y.; Stambuk, H.E.; Mazaheri, Y.; Deasy, J.O.; Shukla-Dave, A. Texture analysis on parametric maps derived from dynamic contrast-enhanced magnetic resonance imaging in head and neck cancer. World J. Radiol. 2016, 8, 90–97. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Graham, C.M.; Elci, O.; Griswold, M.E.; Zhang, X.; Khan, M.A.; Pitman, K.; Caudell, J.J.; Hamilton, R.D.; Ganeshan, B.; et al. Locally advanced squamous cell carcinoma of the head and neck: CT texture and histogram analysis allow independent prediction of overall survival in patients treated with induction chemotherapy. Radiology 2013, 269, 801–809. [Google Scholar] [CrossRef]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; Van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Sala, E.; Mema, E.; Himoto, Y.; Veeraraghavan, H.; Brenton, J.D.; Snyder, A.; Weigelt, B.; Vargas, H.A. Unravelling tumour heterogeneity using next-generation imaging: Radiomics, radiogenomics, and habitat imaging. Clin. Radiol. 2017, 72, 3–10. [Google Scholar] [CrossRef]
- Lefebvre, J.L.; Ang, K.K. Larynx preservation clinical trial design: Key issues and recommendations-a consensus panel summary. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 1293–1303. [Google Scholar] [CrossRef]
- Riga, M.; Chelis, L.; Danielides, V.; Vogiatzaki, T.; Pantazis, T.L.; Pantazis, D. Systematic review on T3 laryngeal squamous cell carcinoma; still far from a consensus on the optimal organ preserving treatment. Eur. J. Surg. Oncol. 2017, 43, 20–31. [Google Scholar] [CrossRef]
- Forastiere, A.A.; Goepfert, H.; Maor, M.; Pajak, T.F.; Weber, R.; Morrison, W.; Glisson, B.; Trotti, A.; Ridge, J.A.; Chao, C.; et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N. Engl. J. Med. 2003, 349, 2091–2098. [Google Scholar] [CrossRef]
- Lefebvre, J.L.; Andry, G.; Chevalier, D.; Luboinski, B.; Collette, L.; Traissac, L.; De Raucourt, D.; Langendijk, J.A.; EORTC Head and Neck Cancer Group. Laryngeal preservation with induction chemotherapy for hypopharyngeal squamous cell carcinoma: 10-year results of EORTC trial 24891. Ann. Oncol. 2012, 23, 2708–2714. [Google Scholar] [CrossRef]
- Forastiere, A.A.; Zhang, Q.; Weber, R.S.; Maor, M.H.; Goepfert, H.; Pajak, T.F.; Morrison, W.; Glisson, B.; Trotti, A.; Ridge, J.A.; et al. Long-term results of RTOG 91-11: A comparison of three nonsurgical treatment strategies to preserve the larynx in patients with locally advanced larynx cancer. J. Clin. Oncol. 2013, 31, 845–852. [Google Scholar] [CrossRef]
- Siegel, R.L.M.K.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef]
- Fisher, R.; Pusztai, L.; Swanton, C. Cancer heterogeneity: Implications for targeted therapeutics. Br. J. Cancer 2013, 108, 479–485. [Google Scholar] [CrossRef]
- Longo, D.L. Tumor heterogeneity and personalized medicine. N. Engl. J. Med. 2012, 366, 956–957. [Google Scholar] [CrossRef]
- Bogowicz, M.; Leijenaar, R.T.; Tanadini-Lang, S.; Riesterer, O.; Pruschy, M.; Studer, G.; Unkelbach, J.; Guckenberger, M.; Konukoglu, E.; Lambin, P. Post-radiochemotherapy PET radiomics in head and neck cancer—The influence of radiomics implementation on the reproducibility of local control tumor models. Radiother. Oncol. 2017, 125, 385–391. [Google Scholar] [CrossRef]
- Bogowicz, M.; Riesterer, O.; Ikenberg, K.; Stieb, S.; Moch, H.; Studer, G.; Guckenberger, M.; Tanadini-Lang, S. Computed Tomography Radiomics Predicts HPV Status and Local Tumor Control after Definitive Radiochemotherapy in Head and Neck Squamous Cell Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 921–928. [Google Scholar] [CrossRef]
- Bogowicz, M.; Riesterer, O.; Stark, L.S.; Studer, G.; Unkelbach, J.; Guckenberger, M.; Tanadini-Lang, S. Comparison of PET and CT radiomics for prediction of local tumor control in head and neck squamous cell carcinoma. Acta Oncol. 2017, 56, 1531–1536. [Google Scholar] [CrossRef] [Green Version]
- Ou, D.; Blanchard, P.; Rosellini, S.; Levy, A.; Nguyen, F.; Leijenaar, R.T.; Garberis, I.; Gorphe, P.; Bidault, F.; Ferté, C.; et al. Predictive and prognostic value of CT based radiomics signature in locally advanced head and neck cancers patients treated with concurrent chemoradiotherapy or bioradiotherapy and its added value to Human Papillomavirus status. Oral Oncol. 2017, 71, 150–155. [Google Scholar] [CrossRef]
- Kuno, H.; Qureshi, M.M.; Chapman, M.N.; Li, B.; Andreu-Arasa, V.C.; Onoue, K.; Truong, M.T.; Sakai, O. CT Texture Analysis Potentially Predicts Local Failure in Head and Neck Squamous Cell Carcinoma Treated with Chemoradiotherapy. AJNR Am. J. Neuroradiol. 2017, 38, 2334–2340. [Google Scholar] [CrossRef] [Green Version]
- Yip, S.S.F.; Aerts, H.J.W.L. Applications and limitations of radiomics. Phys. Med. Biol. 2016, 61, R150–R166. [Google Scholar] [CrossRef] [Green Version]
- European Commission satellite workshop ‘Big data in Health Research: An EU Action Plan’. Available online: http://bigdata2015.uni.lu/eng/European-Commission-satellite-workshop (accessed on 7 June 2015).
- Parmar, C.; Grossmann, P.; Rietveld, D.; Rietbergen, M.M.; Lambin, P.; Aerts, H.J. Radiomic Machine-Learning Classifiers for Prognostic Biomarkers of Head and Neck Cancer. Front. Oncol. 2015, 5, 272. [Google Scholar] [CrossRef] [Green Version]
- Leger, S.; Zwanenburg, A.; Pilz, K.; Lohaus, F.; Linge, A.; Zöphel, K.; Kotzerke, J.; Schreiber, A.; Tinhofer, I.; Budach, V.; et al. A comparative study of machine learning methods for time-to-event survival data for radiomics risk modelling. Sci. Rep. 2017, 7, 13206. [Google Scholar] [CrossRef]
- Resteghini, C.; Trama, A.; Borgonovi, E.; Hosni, H.; Corrao, G.; Orlandi, E.; Calareso, G.; De Cecco, L.; Piazza, C.; Mainardi, L.; et al. Big Data in Head and Neck Cancer. Curr. Treat. Options Oncol. 2018, 19, 62. [Google Scholar] [CrossRef]
- Giraud, P.; Giraud, P.; Gasnier, A.; El Ayachy, R.; Kreps, S.; Foy, J.P.; Durdux, C.; Huguet, F.; Burgun, A.; Bibault, J.E. Radiomics and Machine Learning for Radiotherapy in Head and Neck Cancers. Front. Oncol. 2019, 9, 174. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Ref. | Number of Patients | Image Acquisition | Treatment | Significant Features | Study Objective |
|---|---|---|---|---|---|
| [5] | 32 | Fluorodeoxyglucose (FDG) positron emission tomography (PET)/computed tomography (CT) | Surgery, radiochemotherapy (RCT), Radiotherapy (RT), palliative (not specified by localization) | Metabolic tumor volume, correlation, entropy, energy, and coarseness. | Prognostic value of texture indices over overall survival (OS). |
| [4] | 2 | F-fluorothymidine positron emission tomography (FLT PET) | RCT | Nine features were considered significant. Their results suggested that homogenous lesions at baseline were associated with better prognosis. | Evaluate the utility of radiomic feature analysis from FLT PET obtained at baseline in prediction of treatment response in patients with head and neck cancer. |
| [57] | 11 | FDG PET/CT | RCT | 80 PET radiomic features yielded intraclass correlation coefficient >0.8 in the comparison between the implementations. The change of implementation caused high variability of concordance index (CI) in the univariable analysis. However, both final multivariable models performed equally well in the training and validation cohorts (CI > 0.7) independent of radiomics implementation. | Association of post (RCT) PET radiomics with local tumor control. |
| [60] | Not specified | CT | RCT/Bio-Radiotherapy (BRT) | 544 radiomics image features were defined and were divided in four groups: (I) tumor intensity, (II) shape, (III) texture, and (IV) wavelet features. | Develop a radiomics signature to estimate OS in patients with locally advanced head & neck squamous cell carcinoma (HNSCC) treated with concurrent RCT or BRT and assess its incremental value to Human Papilloma Virus (HPV) and clinical risk factors for individual OS estimation and also to explore its predictive value. |
| [46] | 21 | CT | Cisplatin, 5-fluorouracil, and docetaxel (TPF) Induction Chemotherapy (ICT) | Primary mass entropy and skewness measurements with multiple spatial filters were associated with OS. Multivariate Cox regression analysis incorporating clinical and imaging variables indicated that primary mass size, N stage, primary mass entropy and skewness measurements with the 1.0 spatial filter were independently associated with OS. | Examine the association between overall survival and the baseline CT imaging measurements and clinical variables. |
| [61] | 19 | CT | Not specified | Multivariate analysis revealed that three histogram features (geometric mean, harmonic mean, and fourth moment) and four gray-level run-length features, (short-run emphasis, gray-level nonuniformity, run-length nonuniformity, and short-run low gray-level emphasis) were significant predictors of outcome after adjusting for clinical variables. | Assess the utility of texture analysis for the prediction of treatment failure in primary HNSCC treated with RCT. |
| [58] | 4 | CT | RCT | A radiomic signature, comprising three features, was significantly associated with local control showing that tumors with the most heterogeneous CT density distribution are at risk for decreased local control. | This study aimed to predict local tumor control (LC) after RCT of HNSCC and HPV status using CT radiomics. |
| [59] | 10 | CT/18F-FDGPET/CT | RCT | 569 radiomic features were extracted from both contrast-enhanced CT and 18F-FDG PET. The most homogenous tumors in CT density with a focused region of high FDG uptake indicated better prognosis. However, the CT radiomics-based model overestimated the probability of tumor control in the poor prognostic group. | Comparison of PET and CT radiomics for prediction of local tumor control in HNSCC. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiesa-Estomba, C.M.; Echaniz, O.; Larruscain, E.; Gonzalez-Garcia, J.A.; Sistiaga-Suarez, J.A.; Graña, M. Radiomics and Texture Analysis in Laryngeal Cancer. Looking for New Frontiers in Precision Medicine through Imaging Analysis. Cancers 2019, 11, 1409. https://doi.org/10.3390/cancers11101409
Chiesa-Estomba CM, Echaniz O, Larruscain E, Gonzalez-Garcia JA, Sistiaga-Suarez JA, Graña M. Radiomics and Texture Analysis in Laryngeal Cancer. Looking for New Frontiers in Precision Medicine through Imaging Analysis. Cancers. 2019; 11(10):1409. https://doi.org/10.3390/cancers11101409
Chicago/Turabian StyleChiesa-Estomba, Carlos Miguel, Oier Echaniz, Ekhiñe Larruscain, Jose Angel Gonzalez-Garcia, Jon Alexander Sistiaga-Suarez, and Manuel Graña. 2019. "Radiomics and Texture Analysis in Laryngeal Cancer. Looking for New Frontiers in Precision Medicine through Imaging Analysis" Cancers 11, no. 10: 1409. https://doi.org/10.3390/cancers11101409