The Association between the Consumption of Fish/Shellfish and the Risk of Osteoporosis in Men and Postmenopausal Women Aged 50 Years or Older

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Dietary Intake
2.3. Bone Mass
2.4. Risk Factors
2.5. Statistical Analyses
3. Results
3.1. Characteristics of Participants
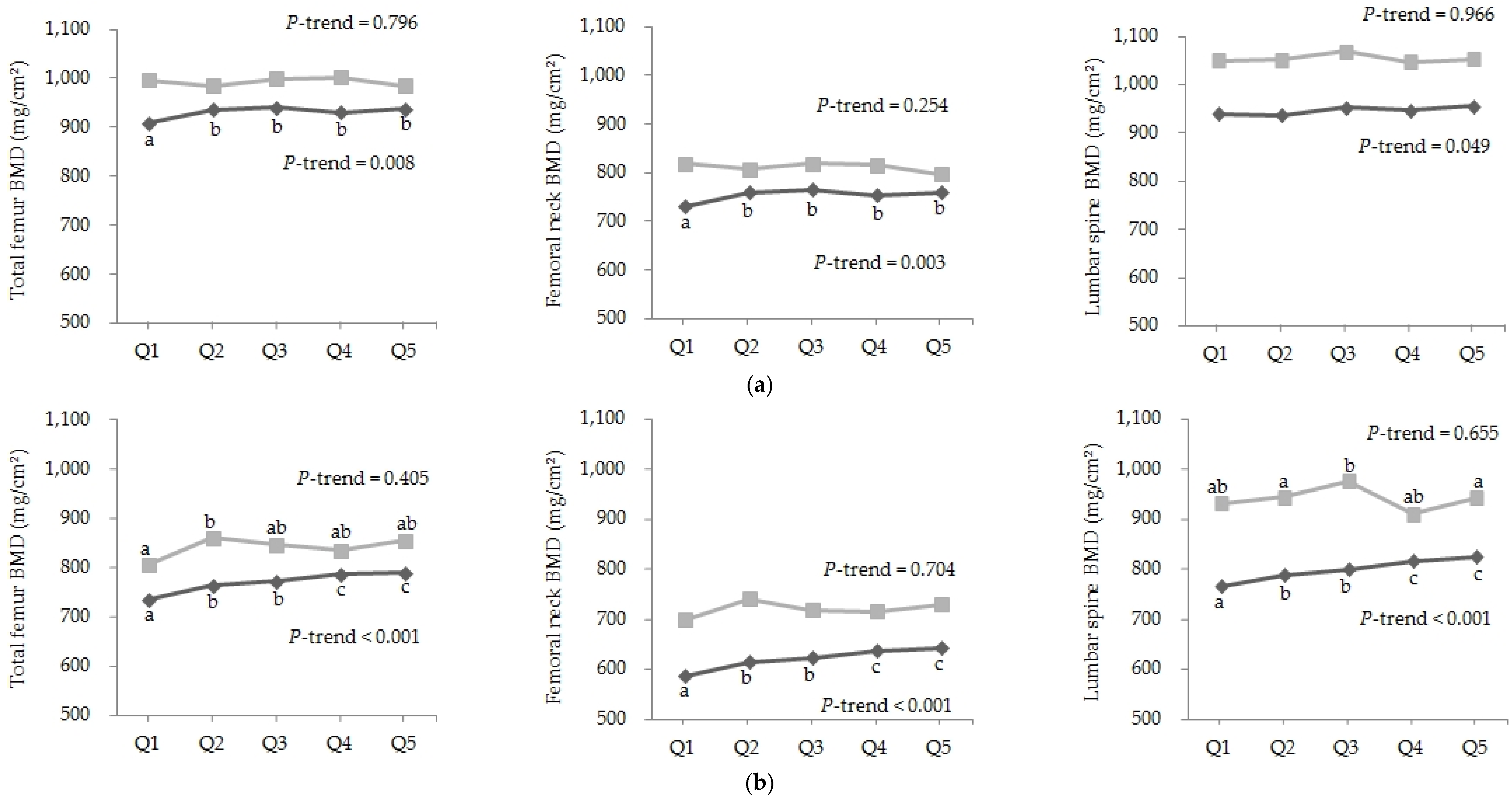
3.2. Association between Consumption of Fish and Shellfish and BMD
3.3. Association between Consumption of Fish and Shellfish and Risk of Osteoporosis
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Riggs, B.L.; Melton, L.J., 3rd. The worldwide problem of osteoporosis: Insights afforded by epidemiology. Bone 1995, 17, 505S–511S. [Google Scholar] [PubMed]
- Cashman, K.D. Diet, nutrition, and bone health. J. Nutr. 2007, 137, 2507S–2512S. [Google Scholar] [PubMed]
- Park, H.; Heo, J.; Park, Y. Calcium from plant sources is beneficial to lowering the risk of osteoporosis in postmenopausal korean women. Nutr. Res. 2011, 31, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Moon, H.; Kim, T.; Byun, D.; Park, Y. Positive correlation between erythrocyte levels of n-3 polyunsaturated fatty acids and bone mass in postmenopausal korean women with osteoporosis. Ann. Nutr. Metab. 2012, 60, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Tartibian, B.; Hajizadeh, M.B.; Kanaley, J.; Sadeghi, K. Long-term aerobic exercise and omega-3 supplementation modulate osteoporosis through inflammatory mechanisms in post-menopausal women: a randomized, repeated measures study. Nutr. Metab. (Lond.) 2011, 8, 71. [Google Scholar]
- Caughey, G.E.; Mantzioris, E.; Gibson, R.A.; Cleland, L.G.; James, M.J. The effect on human tumor necrosis factor alpha and interleukin 1 beta production of diets enriched in n-3 fatty acids from vegetable oil or fish oil. Am. J. Clin. Nutr. 1996, 63, 116–122. [Google Scholar] [PubMed]
- Coetzer, H.; Claassen, N.; van Papendorp, D.H.; Kruger, M.C. Calcium transport by isolated brush border and basolateral membrane vesicles: Role of essential fatty acid supplementation. Prostaglandins Leukot. Essent. Fatty Acids 1994, 50, 257–266. [Google Scholar] [CrossRef]
- Baggio, B.; Budakovic, A.; Nassuato, M.A.; Vezzoli, G.; Manzato, E.; Luisetto, G.; Zaninotto, M. Plasma phospholipid arachidonic acid content and calcium metabolism in idiopathic calcium nephrolithiasis. Kidney Int. 2000, 58, 1278–1284. [Google Scholar] [CrossRef] [PubMed]
- Nawata, K.; Yamauchi, M.; Takaoka, S.; Yamaguchi, T.; Sugimoto, T. Association of n-3 polyunsaturated fatty acid intake with bone mineral density in postmenopausal women. Calcif. Tissue Int. 2013, 93, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Fan, F.; Xue, W.; Wu, B.; He, M.; Xie, H.; Ouyang, W.; Tu, S.; Chen, Y. Higher fish intake is associated with a lower risk of hip fractures in chinese men and women: A matched case-control study. PLoS ONE 2013, 8, e56849. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Ho, S.; Lam, S. Higher sea fish intake is associated with greater bone mass and lower osteoporosis risk in postmenopausal chinese women. Osteoporos. Int. 2010, 21, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, J.; Mozaffarian, D.; Cauley, J.; Mukamal, K.; Robbins, J.; Siscovick, D. Fish consumption, bone mineral density, and risk of hip fracture among older adults: The cardiovascular health study. J. Bone Miner. Res. 2010, 25, 1972–1979. [Google Scholar] [CrossRef] [PubMed]
- Orchard, T.S.; Cauley, J.A.; Frank, G.C.; Neuhouser, M.L.; Robinson, J.G.; Snetselaar, L.; Tylavsky, F.; Wactawski-Wende, J.; Young, A.M.; Lu, B.; et al. Fatty acid consumption and risk of fracture in the women’s health initiative. Am. J. Clin. Nutr. 2010, 92, 1452–1460. [Google Scholar] [PubMed]
- Farina, E.; Kiel, D.; Roubenoff, R.; Schaefer, E.; Cupples, L.; Tucker, K. Dietary intakes of arachidonic acid and α-linolenic acid are associated with reduced risk of hip fracture in older adults. J. Nutr. 2011, 141, 1146–1153. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, J.K.; Mozaffarian, D.; Willett, W.C.; Feskanich, D. Dietary intake of polyunsaturated fatty acids and risk of hip fracture in men and women. Osteoporos. Int. 2012, 23, 2615–2624. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Ramirez, M.J.; Palma, S.; Martinez-Gonzalez, M.A.; Delgado-Martinez, A.D.; de la Fuente, C.; Delgado-Rodriguez, M. Dietary fat intake and the risk of osteoporotic fractures in the elderly. Eur. J. Clin. Nutr. 2007, 61, 1114–1120. [Google Scholar] [CrossRef] [PubMed]
- Benetou, V.; Orfanos, P.; Pettersson-Kymmer, U.; Bergstrom, U.; Svensson, O.; Johansson, I.; Berrino, F.; Tumino, R.; Borch, K.B.; Lund, E.; et al. Mediterranean diet and incidence of hip fractures in a european cohort. Osteoporos. Int. 2013, 24, 1587–1598. [Google Scholar] [CrossRef] [PubMed]
- Farina, E.K.; Kiel, D.P.; Roubenoff, R.; Schaefer, E.J.; Cupples, L.A.; Tucker, K.L. Protective effects of fish intake and interactive effects of long-chain polyunsaturated fatty acid intakes on hip bone mineral density in older adults: The framingham osteoporosis study. Am. J. Clin. Nutr. 2011, 93, 1142–1151. [Google Scholar] [CrossRef] [PubMed]
- Mahaffey, K.R. Fish and shellfish as dietary sources of methylmercury and the ω-3 fatty acids, eicosahexaenoic acid and docosahexaenoic acid: Risks and benefits. Environ. Res. 2004, 95, 414–428. [Google Scholar] [CrossRef] [PubMed]
- Zalloua, P.A.; Hsu, Y.H.; Terwedow, H.; Zang, T.; Wu, D.; Tang, G.; Li, Z.; Hong, X.; Azar, S.T.; Wang, B.; et al. Impact of seafood and fruit consumption on bone mineral density. Maturitas 2007, 56, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Jahns, L.; Raatz, S.; Johnson, L.; Kranz, S.; Silverstein, J.; Picklo, M. Intake of seafood in the us varies by age, income, and education level but not by race-ethnicity. Nutrients 2014, 6, 6060–6075. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Lee, J.; Lee, J.; Park, K.; Kim, S.; Shim, W.; Hong, S.; Im, U.; Giesy, J.; Oh, J. Human exposure to dioxin-like compounds in fish and shellfish consumed in south korea. Hum. Ecol. Risk Assess. 2007, 13, 223–235. [Google Scholar] [CrossRef]
- USDA National Nutrient Database for Standard Reference, Release 22. Available online: http://www.ars.usda.gov/Services/docs.htm?docid=20960 (accessed on 13 December 2015).
- USDA National Nutrient Database for Standard Reference, Release 24. Available online: http://www.ars.usda.gov/Services/docs.htm?docid=22808 (accessed on 13 December 2015).
- National rural resources development institute; Rural developoment administration. Food Composition Tables, 7th ed.; National Rural Resources Development Institute: Suwon, Korea, 2006. [Google Scholar]
- Kanis, J.A.; Delmas, P.; Burckhardt, P.; Cooper, C.; Torgerson, D. Guidelines for diagnosis and management of osteoporosis. The european foundation for osteoporosis and bone disease. Osteoporos. Int. 1997, 7, 390–406. [Google Scholar] [CrossRef] [PubMed]
- Cosman, F.; de Beur, S.; LeBoff, M.; Lewiecki, E.; Tanner, B.; Randall, S.; Lindsay, R. Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos. Int. 2014, 25, 2359–2381. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.; McCloskey, E.; Johansson, H.; Oden, A.; Ström, O.; Borgström, F. Development and use of frax® in osteoporosis. Osteoporos. Int. 2010, 21, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.; Woo, J.; Leung, J. Effects of food groups and dietary nutrients on bone loss in elderly chinese population. J. Nutr. Health Aging 2011, 15, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Korea Centers for Disease Control and Prevention. Korea Health Statistics 2010: Korea National Health and Nutrition Examination Survey (KNHANES V-1); Ministry of Health and Welfare: Seoul, Korea, 2012. [Google Scholar]
- Candela, M.; Astiasaran, I.; Bello, J. Deep-fat frying modifies high-fat fish lipid fraction. J. Agric. Food Chem. 1998, 46, 2793–2796. [Google Scholar] [CrossRef]
- Kim, S.; Moon, S.; Popkin, B.M. The nutrition transition in south korea. Am. J. Clin. Nutr. 2000, 71, 44–53. [Google Scholar] [PubMed]
- Mangano, K.; Kerstetter, J.; Kenny, A.; Insogna, K.; Walsh, S. An investigation of the association between omega 3 fa and bone mineral density among older adults: Results from the national health and nutrition examination survey years 2005–2008. Osteoporos. Int. 2014, 25, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Griel, A.E.; Kris-Etherton, P.M.; Hilpert, K.F.; Zhao, G.; West, S.G.; Corwin, R.L. An increase in dietary n-3 fatty acids decreases a marker of bone resorption in humans. Nutr. J. 2007, 6. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Veit, H.P.; Denbow, D.M. Effects of long-term dietary lipids on mature bone mineral content, collagen, crosslinks, and prostaglandin e2 production in japanese quail. Poult. Sci. 2004, 83, 1876–1883. [Google Scholar] [CrossRef] [PubMed]
- Benetou, V.; Orfanos, P.; Zylis, D.; Sieri, S.; Contiero, P.; Tumino, R.; Giurdanella, M.; Peeters, P.; Linseisen, J.; Nieters, A.; et al. Diet and hip fractures among elderly europeans in the epic cohort. Eur. J. Clin. Nutr. 2011, 65, 132–139. [Google Scholar] [PubMed]
- Park, Y.; Kim, M. Serum 25-hydroxyvitamin D concentrations are associated with erythrocyte levels of n-3 PUFA but not risk of CVD. Br. J. Nutr. 2011, 106, 1529–1534. [Google Scholar] [CrossRef] [PubMed]
 ) and National Health and Nutrition Examination Survey (NHANES,
) and National Health and Nutrition Examination Survey (NHANES,  ). Q1 (4.2), Q2 (10.9), Q3 (19.3), Q4 (30.4), Q5 (49.7) in men of KNHANES; Q1 (0), Q2 (1.5), Q3 (3.5), Q4 (5.8), Q5 (12.2) in men of NHANES; Q1 (3.1), Q2 (8.5), Q3 (16.6), Q4 (28.3), Q5 (49.3) in women of KNHANES; and Q1 (0), Q2 (1.5), Q3 (3.6), Q4 (6.0), Q5 (11.9) in women of NHANES. Values with different letters are significantly different with a p-value < 0.05 (ANCOVA with Bonferroni’s post hoc test).
) and National Health and Nutrition Examination Survey (NHANES, ). Q1 (4.2), Q2 (10.9), Q3 (19.3), Q4 (30.4), Q5 (49.7) in men of KNHANES; Q1 (0), Q2 (1.5), Q3 (3.5), Q4 (5.8), Q5 (12.2) in men of NHANES; Q1 (3.1), Q2 (8.5), Q3 (16.6), Q4 (28.3), Q5 (49.3) in women of KNHANES; and Q1 (0), Q2 (1.5), Q3 (3.6), Q4 (6.0), Q5 (11.9) in women of NHANES. Values with different letters are significantly different with a p-value < 0.05 (ANCOVA with Bonferroni’s post hoc test).
). Q1 (4.2), Q2 (10.9), Q3 (19.3), Q4 (30.4), Q5 (49.7) in men of KNHANES; Q1 (0), Q2 (1.5), Q3 (3.5), Q4 (5.8), Q5 (12.2) in men of NHANES; Q1 (3.1), Q2 (8.5), Q3 (16.6), Q4 (28.3), Q5 (49.3) in women of KNHANES; and Q1 (0), Q2 (1.5), Q3 (3.6), Q4 (6.0), Q5 (11.9) in women of NHANES. Values with different letters are significantly different with a p-value < 0.05 (ANCOVA with Bonferroni’s post hoc test).
) and National Health and Nutrition Examination Survey (NHANES, ). Q1 (4.2), Q2 (10.9), Q3 (19.3), Q4 (30.4), Q5 (49.7) in men of KNHANES; Q1 (0), Q2 (1.5), Q3 (3.5), Q4 (5.8), Q5 (12.2) in men of NHANES; Q1 (3.1), Q2 (8.5), Q3 (16.6), Q4 (28.3), Q5 (49.3) in women of KNHANES; and Q1 (0), Q2 (1.5), Q3 (3.6), Q4 (6.0), Q5 (11.9) in women of NHANES. Values with different letters are significantly different with a p-value < 0.05 (ANCOVA with Bonferroni’s post hoc test).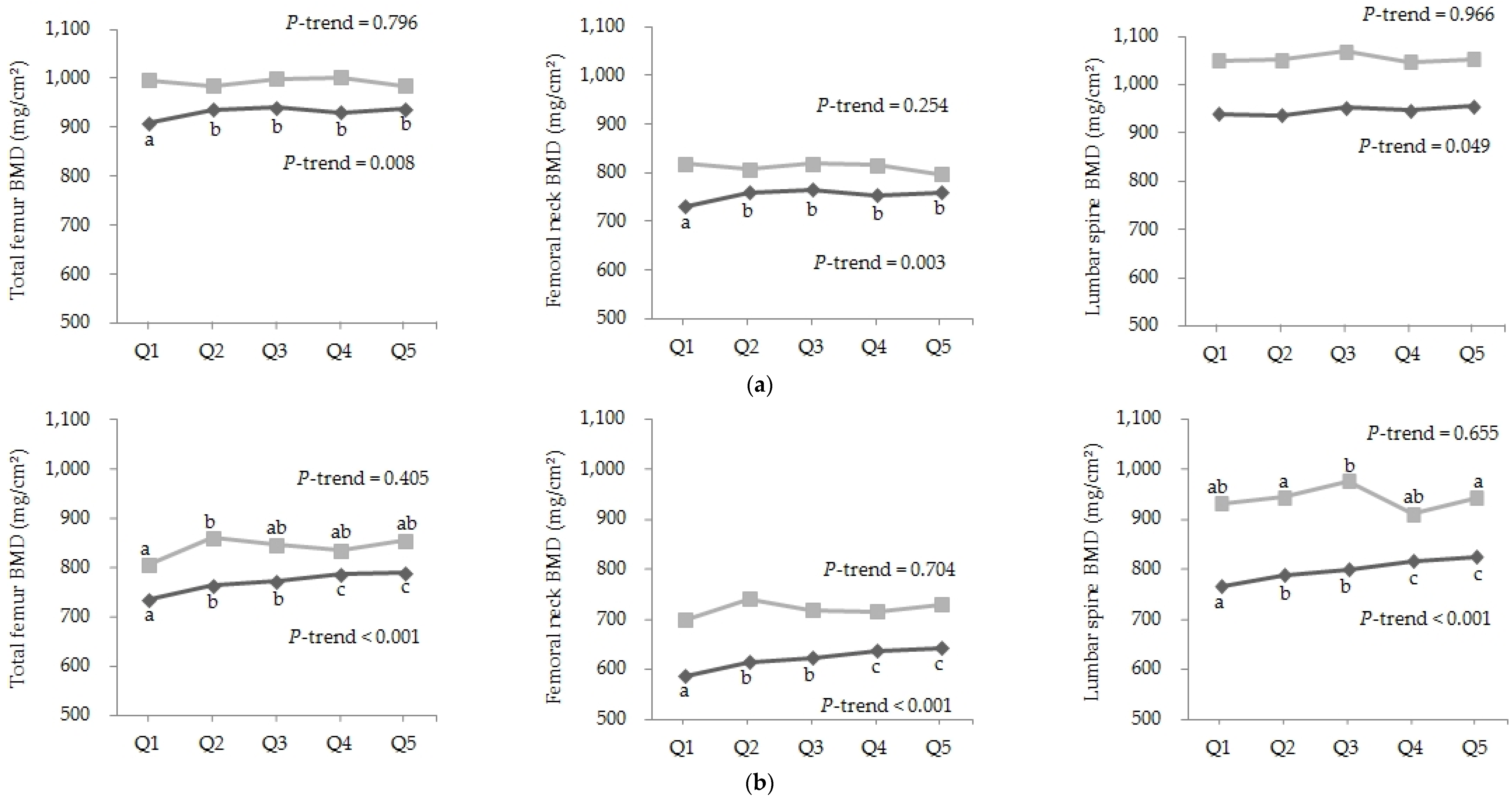

{kind=link}
| Men | p-Value | Women | p-Value | |||
|---|---|---|---|---|---|---|
| KNHANES (N = 3182) | NHANES (N = 1435) | KNHANES (N = 3972) | NHANES (N = 1223) | |||
| Age (year) | 60.94 ± 0.20 | 60.50 ± 0.23 | 0.171 | 63.54 ± 0.20 | 62.59 ± 0.28 | 0.008 |
| BMI (kg/m2) | 23.82 ± 0.07 | 28.40 ± 0.21 | <0.001 | 24.22 ± 0.06 | 27.97 ± 0.20 | <0.001 |
| Alcohol use, n (%) | 2371 (78.0) | 1134 (82.8) | <0.001 | 1736 (45.8) | 671 (63.2) | <0.001 |
| Smoking state, n (%) | 1014 (35.5) | 280 (29.8) | 0.019 | 169 (4.7) | 169 (31.8) | <0.001 |
| Regular exercise, n (%) | 1582 (51.2) | 295 (23.0) | <0.001 | 1467 (37.2) | 141 (13.3) | <0.001 |
| Bone mineral density (mg/cm2) | ||||||
| Total femur | 932.43 ± 2.84 | 1007.68 ± 5.68 | <0.001 | 771.66 ± 2.48 | 843.18 ± 4.80 | <0.001 |
| Femoral neck | 754.94 ± 2.57 | 819.10 ± 4.20 | <0.001 | 621.41 ± 2.24 | 721.84 ± 3.59 | <0.001 |
| Lumbar spine | 945.62 ± 3.30 | 1061.88 ± 6.68 | <0.001 | 799.04 ± 2.76 | 940.97 ± 5.55 | <0.001 |
| Dietary intake | ||||||
| Fish and shellfish (times/month) | 23.90 ± 0.40 | 5.07 ± 0.20 | <0.001 | 22.01 ± 0.41 | 5.29 ± 0.24 | <0.001 |
| Protein (g/day) | 74.96 ± 0.86 | 90.33 ± 1.70 | <0.001 | 51.81 ± 0.57 | 66.42 ± 0.82 | <0.001 |
| Sodium (mg/day) | 5573.56 ± 80.20 | 3781.15 ± 76.47 | <0.001 | 3806.92 ± 56.98 | 2834.24 ± 52.11 | <0.001 |
| Calcium (mg/day) | 559.34 ± 8.46 | 999.35 ± 23.56 | <0.001 | 420.19 ± 7.77 | 869.8 ± 21.72 | <0.001 |
| Family history, n (%) | 372 (13.1) | 135 (13.2) | 0.908 | 637 (16.0) | 179 (20.4) | 0.010 |
| Medical history, n (%) | ||||||
| Thyroid disease | 48 (1.4) | 66 (4.9) | <0.001 | 297 (7.4) | 254 (22.3) | <0.001 |
| Rheumatoid arthritis | 45 (1.2) | 95 (5.2) | <0.001 | 221 (5.5) | 121 (7.3) | 0.054 |
| Osteoporosis | 267 (6.9) | 88 (5.4) | 0.098 | 568 (21.7) | 279 (23.5) | 0.323 |
| Men ≥50 Years Old | Postmenopausal Women ≥50 Years Old | |||
|---|---|---|---|---|
| KNHANES (N = 3182) | NHANES (N = 1435) | KNHANES (N = 3972) | NHANES (N = 1223) | |
| Total femur | 0.0748 *** | -0.0275 | 0.1611 *** | 0.0754 |
| Femoral neck | 0.0768 *** | −0.0002 | 0.1806 *** | 0.0697 |
| Lumbar spine | 0.0465 ** | -0.0124 | 0.1630 *** | 0.0249 |
| Quintiles of Consumption of Fish and Shellfish (Times/Month) | ||||||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | p for Trend 2 | |
| Men ≥50 years old | ||||||
| Average intake in KNHANES | 4.2 | 10.9 | 19.3 | 30.4 | 49.7 | |
| Model 1 | 1.00 | 0.74 (0.49–1.12) | 0.53 (0.33–0.85) | 0.52 (0.32–0.83) | 0.25 (0.15–0.42) | <0.001 |
| Model 2 | 1.00 | 0.92 (0.58–1.45) | 0.68 (0.42–1.12) | 0.69 (0.42–1.15) | 0.35 (0.20–0.59) | <0.001 |
| Model 3 | 1.00 | 0.95 (0.60–1.49) | 0.70 (0.42–1.16) | 0.71 (0.43–1.18) | 0.37 (0.20–0.60) | <0.001 |
| Average intake in NHANES | 0.0 | 1.5 | 3.5 | 5.8 | 12.2 | |
| Model 1 | 1.00 | 0.51 (0.26–1.01) | 0.83 (0.39–1.75) | 1.08 (0.50–2.35) | 0.53 (0.21–1.35) | 0.722 |
| Model 2 | 1.00 | 0.61 (0.30–1.21) | 1.15 (0.52–2.56) | 1.31 (0.55–3.12) | 0.68 (0.27–1.73) | 0.958 |
| Model 3 | 1.00 | 0.43 (0.16–1.16) | 0.90 (0.30–2.72) | 1.12 (0.43–2.89) | 0.57 (0.15–2.12) | 0.999 |
| Postmenopausal women ≥50 years old | ||||||
| Average intake in KNHANES | 3.1 | 8.5 | 16.6 | 28.3 | 49.3 | |
| Model 1 | 1.00 | 0.59 (0.47–0.74) | 0.53 (0.41–0.69) | 0.41 (0.32–0.52) | 0.34 (0.26–0.45) | <0.001 |
| Model 2 | 1.00 | 0.63 (0.49–0.80) | 0.52 (0.40–0.68) | 0.42 (0.32–0.54) | 0.35 (0.26–0.47) | <0.001 |
| Model 3 | 1.00 | 0.63 (0.49–0.80) | 0.55 (0.42–0.71) | 0.43 (0.33–0.56) | 0.36 (0.28–0.50) | <0.001 |
| Average intake in NHANES | 0.0 | 1.5 | 3.6 | 6.0 | 11.9 | |
| Model 1 | 1.00 | 0.87 (0.50–1.51) | 0.57 (0.32–1.03) | 0.69 (0.40–1.17) | 0.57 (0.36–0.90) | 0.025 |
| Model 2 | 1.00 | 0.89 (0.51–1.53) | 0.56 (0.31–1.03) | 0.69 (0.39–1.21) | 0.56 (0.35–0.89) | 0.022 |
| Model 3 | 1.00 | 0.93 (0.48–1.79) | 0.61 (0.34–1.06) | 0.71 (0.35–1.45) | 0.61 (0.38–1.00) | 0.065 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, E.; Park, Y. The Association between the Consumption of Fish/Shellfish and the Risk of Osteoporosis in Men and Postmenopausal Women Aged 50 Years or Older. Nutrients 2016, 8, 113. https://doi.org/10.3390/nu8030113
Choi E, Park Y. The Association between the Consumption of Fish/Shellfish and the Risk of Osteoporosis in Men and Postmenopausal Women Aged 50 Years or Older. Nutrients. 2016; 8(3):113. https://doi.org/10.3390/nu8030113
Chicago/Turabian StyleChoi, Eunjin, and Youngsoon Park. 2016. "The Association between the Consumption of Fish/Shellfish and the Risk of Osteoporosis in Men and Postmenopausal Women Aged 50 Years or Older" Nutrients 8, no. 3: 113. https://doi.org/10.3390/nu8030113
APA StyleChoi, E., & Park, Y. (2016). The Association between the Consumption of Fish/Shellfish and the Risk of Osteoporosis in Men and Postmenopausal Women Aged 50 Years or Older. Nutrients, 8(3), 113. https://doi.org/10.3390/nu8030113