Micronutrient Fortified Condiments and Noodles to Reduce Anemia in Children and Adults—A Literature Review and Meta-Analysis

Abstract
:1. Introduction
2. Experimental Section
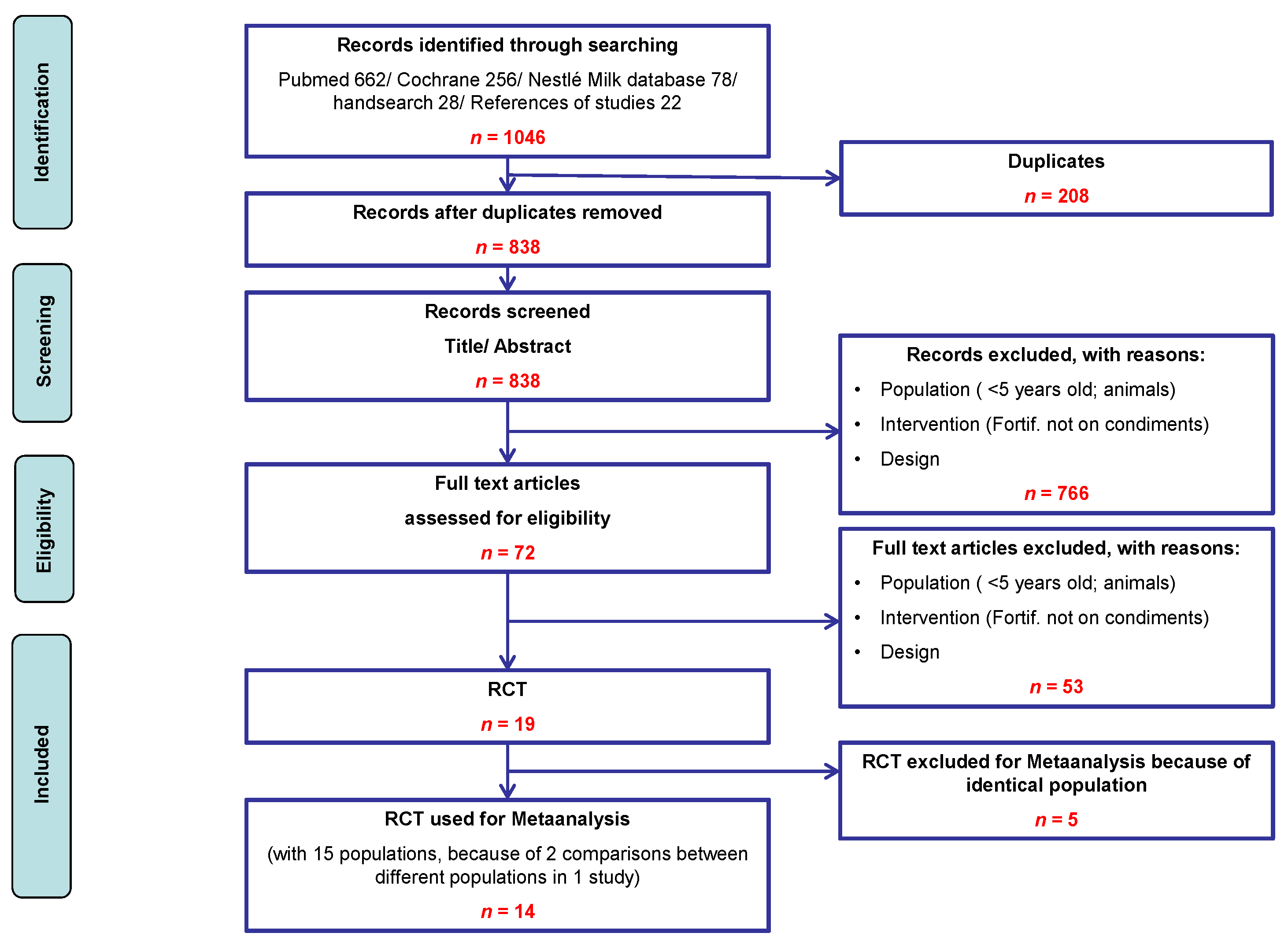
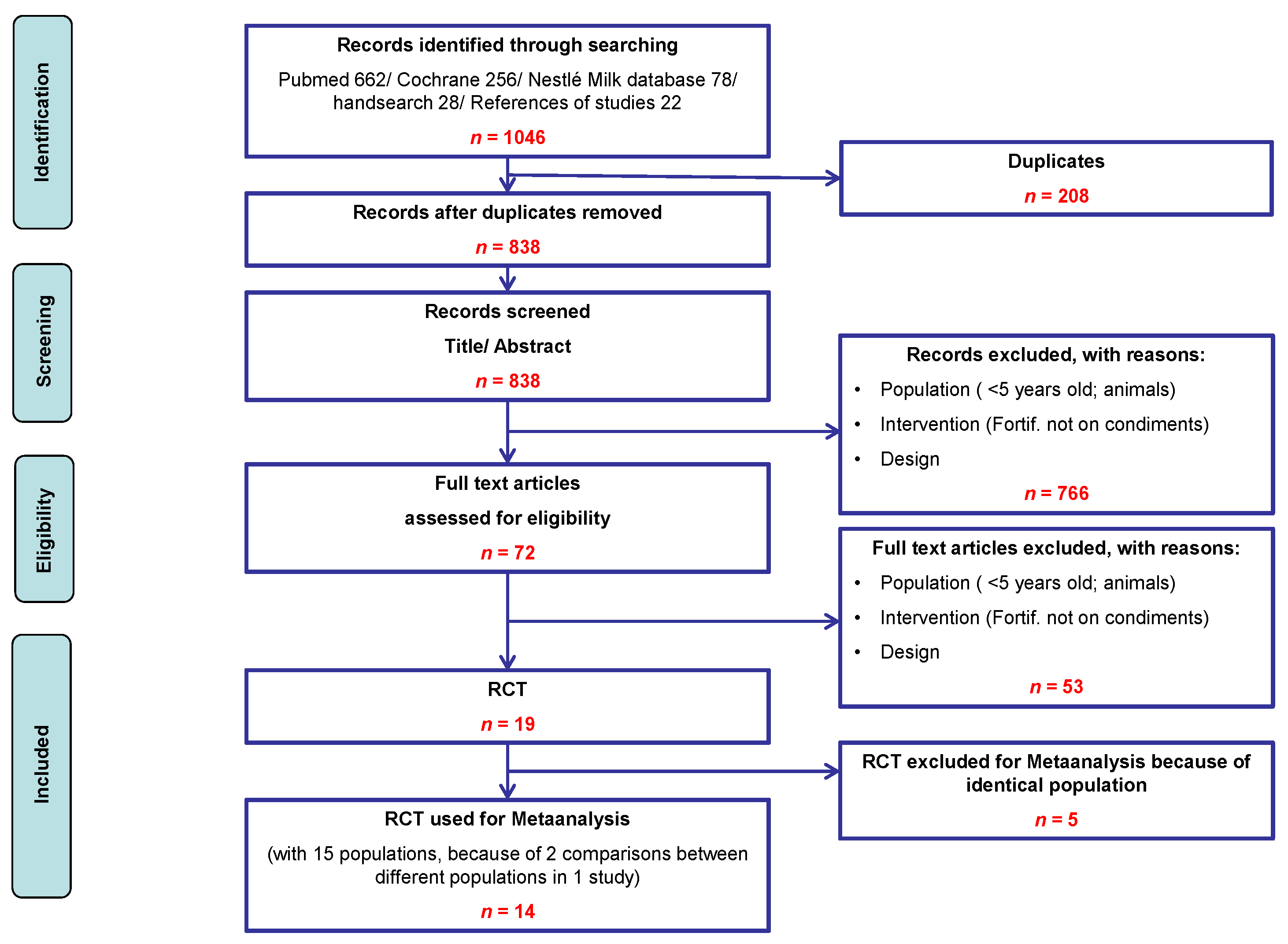
2.1. Search Strategy

{kind=link}
{kind=link}
{kind=link}
| Step | Search Pubmed |
|---|---|
| 1 | Fortif * |
| 2 | Condiments [MesH] OR Seasoned OR Seasoning OR Bouillon * OR Sprinkle * OR Soy sauce * |
| 3 | OR Fish sauce* OR Powder */NOT milk powder * OR Noodle * |
| 4 | 1 AND 2 Fortified salt * |
2.2. Inclusion/Exclusion Criteria
2.3. Study Selection and Data Extraction
2.4. Analysis
3. Results
3.1. Description of Included Studies
| Author; Year | Population | Intervention | Control | Outcome Parameters (Including Surrogate Parameters) |
|---|---|---|---|---|
| Andersson; 2008 [25] Design: RCT | Country: India Age in years (mean (range)): 12 (5 to15) Males in %: 52 Exclusion criteria : Hb < 8 g/dL | n = 130 Dual fortified salt providing iron and iodine (potassium iodate (KIO3; 30 µg/g salt) and MGFePP (2 mg/g salt)) MN strategy: dual MN strategy | n = 131 (Mono) iodized salt providing potassium iodate (KIO3; 30 µg/g salt) | After 0.8 years: Anemia rate, Hb, ferritin, transferrin, body iron, zinc protoporphyrin, acceptability |
| Asibey-Berko; 2007 [21] Design: RCT | Country: Ghana Age in years (mean (range)): 29 Males in %: 0 Exclusion criteria : pregnant women, unwilling to take fortified salt, Hb < 100 g/L | n = 65 Dual fortified salt providing iron and iodine (potassium iodide (50 mg/kg salt) and ferrous furamate (1 g/kg salt)) MN strategy: dual MN strategy | n = 58 (Mono) iodized salt providing potassium iodate (50 mg/kg salt) and placebo | After 0.7 years: Anemia rate, urinary iodine |
| Ballot; 1989 [20] Design: cluster RCT (264 clusters: families) | Country: South Africa Age in years (mean (range)): no info Males in %: 45.6 Exclusion criteria : age < 10 year, Hb ≤ 90 g/L | n = 298 Fortified masala powder providing iron (NaFeEDTA (25 µg/g masala)) MN strategy: single MN strategy | n = 300 Non fortified masala powder | After 2 years: Hb, ferritin, transferrin saturation, body iron |
| Chen; 2005 [33] Design: cluster RCT (9 clusters: villages) | Country: China Age in years (mean (range)): no info (3 to 55+) Males in %: no info Exclusion criteria : no info | n = 2020 Fortified soy sauce providing iron (NaFeEDTA (29.6 mg/100 mL soy sauce )) MN strategy: single MN strategy | n = 2007 Non fortified soy sauce | After 1.5 years: Hb, ferritin, serum retinol, W/H, food consumption, anemia rate |
| Author; year | Population | Intervention | Control | Outcome parameters (including surrogate parameters) |
| Huo; 2002 [32] Design: RCT | Country: China Age in years (range): 11 to 17 Males in %: 51 Exclusion criteria : no anemia | n = 77 Fortified soy sauce providing iron (high-NaFeEDTA (4 mg Fe/mL soy sauce)) MN strategy: single MN strategy | n = 81 Non fortified soy sauce | After 0.2 years: Anemia rate, Hb, ferritin, transferrin, iron, free erythrocyte protoporphyrin, total iron binding capapility |
| Le; 2007 [18] Design: RCT | Country: Vietnam Age in years (mean (range)): 7.3 Males in %: IG:51.2 CG:48.8 Exclusion criteria : Hb < 70g /L | n = 86 Fortified noodles providing iron (NaFeEDTA (10.7 mg/52 g noodles)) MN strategy: single MN strategy | n = 82 Non fortified noodles with placebo | After 0.5 years: Anemia rate, Hb, ferritin, serum transferrin rezeptor, body iron |
| Le; 2007 [18] Design: RCT | Country: Vietnam Age in years (mean (range)): 7.3 Males in %:48.7 Exclusion criteria : Hb < 70 g/L | n = 79 Fortified noodles providing iron (NaFeEDTA (10.7 mg/52 g noodles)) with mebendazole MN strategy: single MN strategy | n = 79 Non fortified noodles with mebendazole | After 0.5 years: Anemia rate, Hb, ferritin, serum transferrin rezeptor, body iron |
| Longfils; 2008 [15] Design: RCT | Country: Cambodia Age in years (mean (range)): 13.6 (6 to 21) Males in %: 40 Exclusion criteria : acute malnutrition below 80% weight or height score, Hb < 70 g/L, chronic diseases, iron supplementation, lack of parental approval | n = 46 Fortified fish sauce providing iron (NaFe-EDTA (1 mg Fe/mL fish sauce)) MN strategy: single MN strategy | n = 44 Non fortified fish sauce (endogenous iron content of 86 mg Fe/L) | After 0.4 years: Hb, ferritin, CRP, W/H, BMI, infections (vomiting, diarrhea, acute respiratory infection) |
| Rajagopalan; 2000 [26] Design: cluster RCT (20 clusters: housing areas) | Country: India Age in years (mean (range)): no info (18 to 45) Males in %: 39 Exclusion criteria : casual workers | n = 385 Dual fortified salt providing iron and iodine (no info about MN dosage) MN strategy: dual MN strategy | n = 408 (Mono) iodized salt | After 1 year: Hb, productivity in tea leaf picking |
| Thuy; 2003 [17] Design: RCT | Country: Vietnam Age in years (mean (range)): 34 (19 to 49) Males in %: 0 Exclusion criteria : women with gastrointestinal or metabolic disorders, pregnant women | n = 64 Fortified fish sauce providing iron (NaFeEDTA (1 mg Fe/mL fish sauce)) MN strategy: single MN strategy | n = 72 Non fortified fish sauce | After 0.5 years: Anemia rate, Hb, ferritin, transferrin |
| Thuy; 2005 [16] Design: cluster RCT (21 clusters: villages) | Country: Vietnam Age in years (mean (range)): 32 (16 to 49) Males in %: 0 Exclusion criteria : no info | n = 199 Fortified fish sauce providing iron (NaFeEDTA (9 mmol Fe/L fish sauce)) MN strategy: single MN strategy | n = 190 Non fortified fish sauce | After 1.5 years: Anemia rate, Hb, ferritin, CRP, serum retinol, intestinal parasites (eggs counts) |
| Vinodkumar; 2007 [27] Design: cluster RCT (7 clusters: communities) | Country: India Age in years (mean (range)): no info Males in %: 39 Exclusion criteria : no info | n = 393 Dual fortified salt providing iron and iodine (potassium iodate (40 µg/g salt), ferrous sulfate monohydrate (1 mg/g salt)) MN strategy: dual MN strategy | n = 436 (Mono) iodized salt providing potassium iodate | After 1 year: Hb, urinary iodine |
| Vinodkumar; 2009 [28] Design: cluster RCT (6 clusters: schools) | Country: India Age in years (mean (range)): 12.3 (5 to 18) Males in %: no info Exclusion criteria : schools where children go home more than once a year | n = 213 Multimicronutrient fortified salt providing iron, zinc, vitamin A, other vitamins, folate, other MN (10 g salt contained the RDA of MN. Iron 1 mg/g salt.) MN strategy: Multimicronutrient strategy | n = 18 (Mono) iodized salt providing potassium iodate | After 0.75 years: Anemia rate, Hb, ferritin, serum transferrin rezeptor, body iron stores, CRP, alkaline granulocytes phosphatase, serum Vit.A, serum Vit. B12, serum folic acid, serum zinc, angular stomatitis, memory Test |
| Winichagoon; 2006 [30] Design: cluster RCT (10 cluster: schools) | Country: Thailand Age in years (mean (range)): 9.2 (5.5 to 13.4) Males in %: 49.5 Exclusion criteria : acute or chronic illnesses, Hb < 80 g/L | n = 278 Multimicronutrient fortified seasoning providing iron, zinc, iodine, vitamin A (per serving (lunch): 5 mg H-reduced elemental iron, 270 µg palmitate, 50 µg potassium idodine, 5 mg zinc sulfate) MN strategy: Multimicronutrient strategy | n = 277 Non fortified seasoning powder | After 0.6 years: Anemia rate, Hb, ferritin, urinary iodine, serum retinol, mean corpuscular volume, W/H, BMI, arm circumfences infection status, short-term learning, memory, attention span |
| Zimmermann; 2004 [24] Design: cluster RCT (clusters: households; no information about number of clusters) | Country: Morocco Age in years (mean (range)): 10.7 (6 to 15) Males in %: 53 Exclusion criteria : no info | n = 75 Dual fortified salt providing iron and iodine (potassium iodate (25 µg iodine/g salt) and FePP (2 mg Fe/g salt)) MN strategy: dual MN strategy | n = 83 (Mono) iodized salt providing potassium iodate (25 µg iodine/g salt) | After 0.8 years: Anemia rate, Hb, ferritin, transferrin, CRP, zinc, urinary iodine, thyroid volume, goiter, color, taste acceptability, satisfaction with salt, sensory changes |
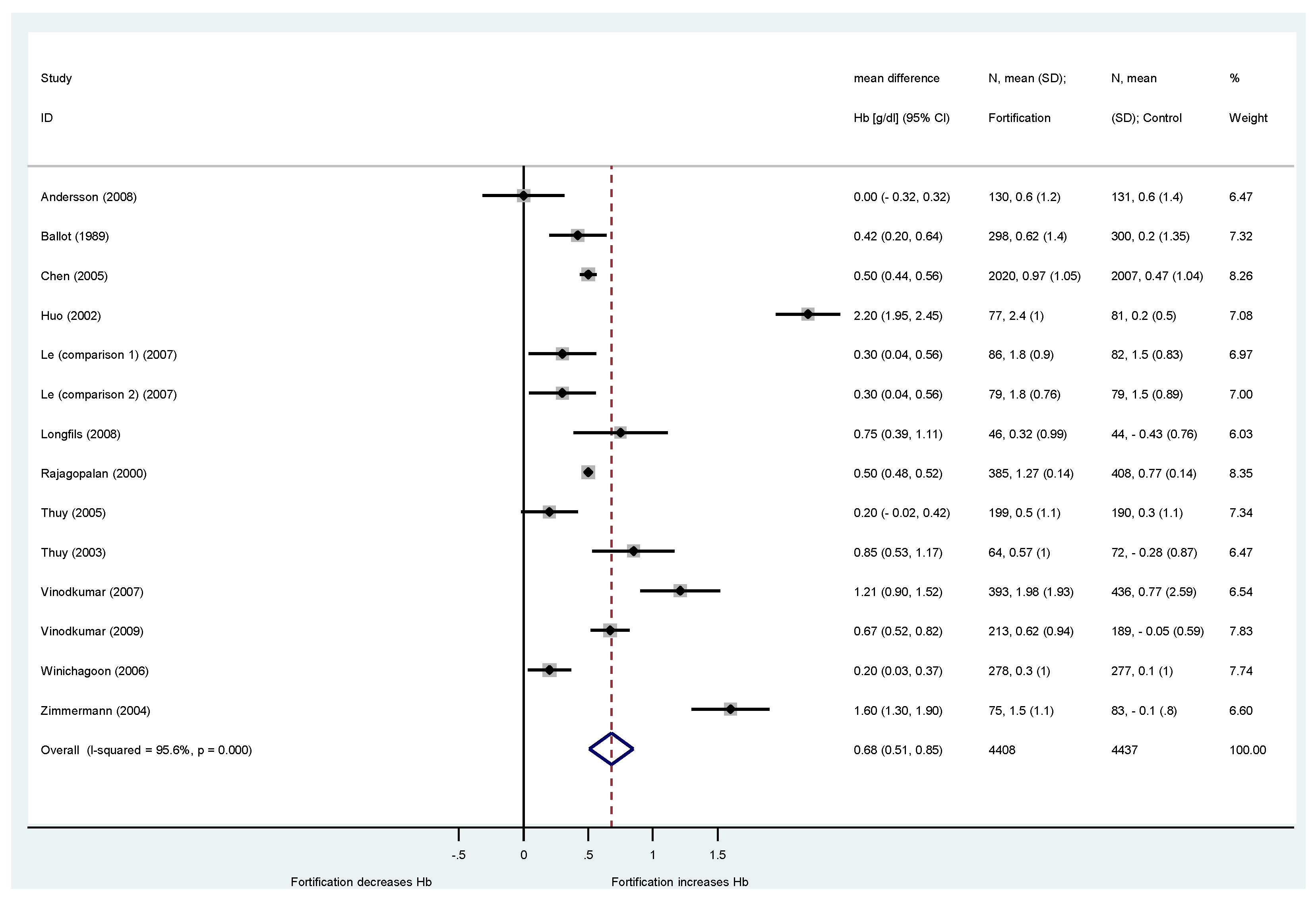
3.2. Effects on Hemoglobin Concentrations

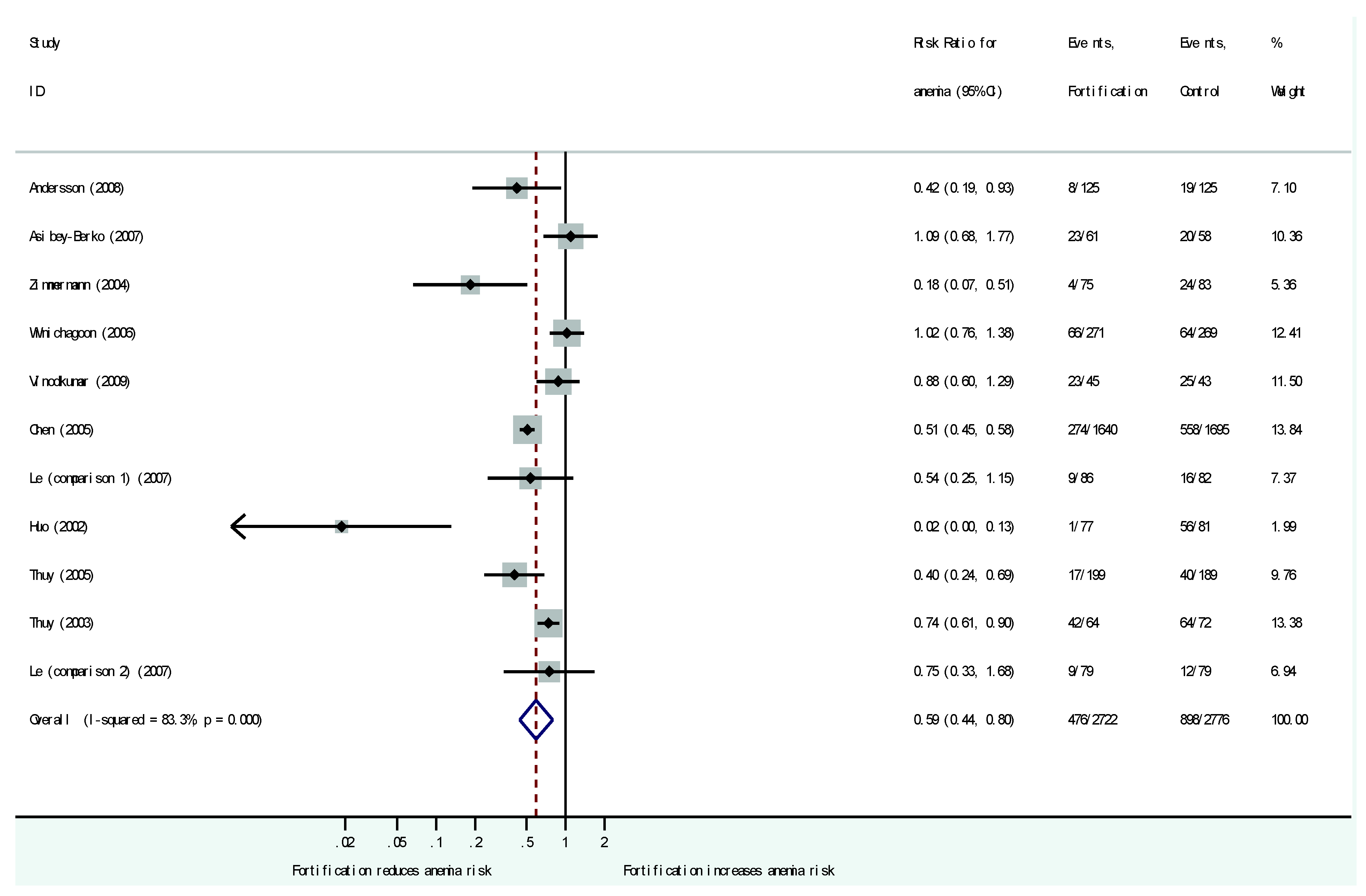
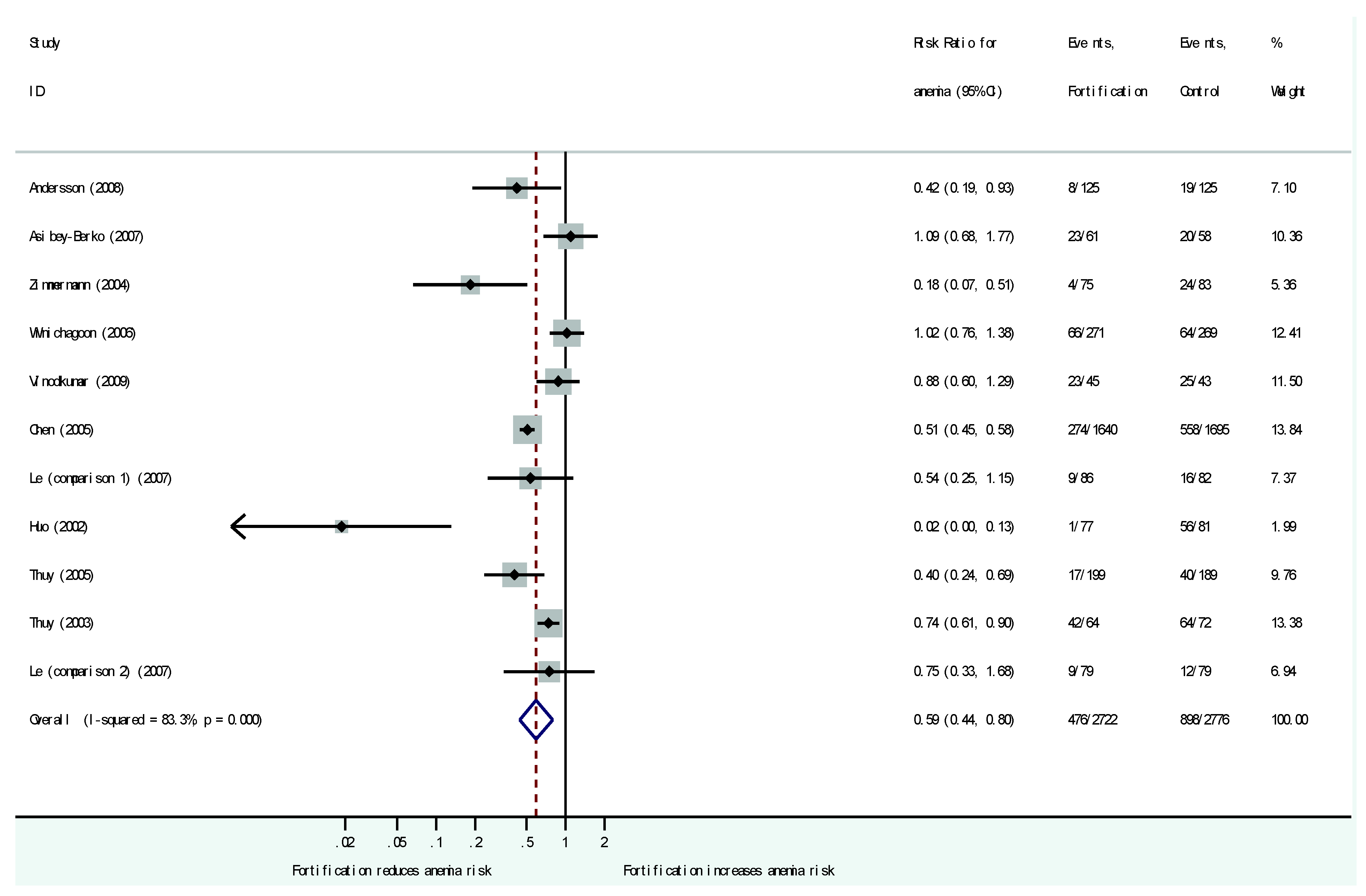
3.3. Effects on Anemia Prevalence
3.4. Effect on Ferritin Concentrations
3.5. Other Reported Effects
3.6. Results of Meta-Regression
3.7. Risk of Bias Assessment
| Reference | Author | Year | Adequate Sequence Generation? | Allocation Concealment? | Blinding? | Incomplete Outcome Data Addressed? | Are typical Outcomes Reported? (No Selective Outcome Reporting) |
|---|---|---|---|---|---|---|---|
| [25] | Andersson | 2008 | ? | ? | YES | YES | YES |
| [21] | Asibey-Berko | 2007 | ? | YES | YES | NO | YES |
| [20] | Ballot | 1989 | ? | ? | YES | NO | NO |
| [33] | Chen | 2005 | ? | ? | YES | YES | YES |
| [32] | Huo | 2002 | ? | ? | ? | NO | YES |
| [18] | Le | 2007 | YES | YES | YES | YES | YES |
| [15] | Longfis | 2008 | ? | ? | YES | YES | YES |
| [26] | Rajagopalan | 2000 | YES | YES | YES | NO | YES |
| [16] | Thuy | 2005 | ? | ? | YES | NO | YES |
| [17] | Thuy | 2003 | ? | ? | YES | YES | YES |
| [27] | Vinodkumar | 2007 | ? | ? | YES | YES | NO |
| [28] | Vinodkumar | 2009 | ? | ? | YES | YES | YES |
| [30] | Winichagoon | 2006 | YES | ? | ? | YES | YES |
| [24] | Zimmermann | 2004 | ? | ? | YES | YES | YES |
4. Discussion
4.1. Existing Systematic Reviews and Research Needs
4.2. Implications for Decision Makers
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- World Health Organisation. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Allen, L.; de Benoist, B.; Dary, O.; Hurrell, R. Guidelines on Food Fortification with Micronutrients; World Health Organization and Food and Agriculture Organization of the United Nations: Geneva, Switzerland, 2006. [Google Scholar]
- Bhutta, Z.A.; Ahmed, T.; Black, R.E.; Cousens, S.; Dewey, K.; Giugliani, E.; Haider, B.A.; Kirkwood, B.; Morris, S.S.; Sachdev, H.P.; et al. What works? Interventions for maternal and child undernutrition and survival. Lancet 2008, 371, 417–440. [Google Scholar] [PubMed]
- World Health Organization. Conclusions and recommendations of the WHO consultation on prevention and control of iron deficiency in infants and young children in malaria-endemic areas. Food Nutr. Bull. 2007, 28, S621–S631. [Google Scholar]
- Das, J.K.; Salam, R.; Kumar, R.; Bhutta, Z.A. Micronutrient fortification of food and its impact on woman and child health: A systematic review. BioMed Central 2013, 2, 2–24. [Google Scholar] [CrossRef] [PubMed]
- Eichler, K.; Wieser, S.; Ruthemann, I.; Brugger, U. Effects of micronutrient fortified milk and cereal food for infants and children: A systematic review. BMC Public Health 2012, 12, 506. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.H.; Peerson, J.M.; Olney, D.K. Provision of multiple rather than two or fewer micronutrients more effectively improves growth and other outcomes in micronutrient-deficient children and adults. J. Nutr. 2009, 139, 1022–1030. [Google Scholar] [CrossRef] [PubMed]
- De-Regil, L.M.; Suchdev, P.S.; Vist, G.E.; Walleser, S.; Pena-Rosas, J.P. Home fortification of foods with multiple micronutrient powders for health and nutrition in children under two years of age. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef]
- Gera, T.; Sachdev, H.S.; Boy, E. Effect of iron-fortified foods on hematologic and biological outcomes: systematic review of randomized controlled trials. Am. J. Clin. Nutr. 2012, 96, 309–324. [Google Scholar] [CrossRef] [PubMed]
- Haider, B.A.; Bhutta, Z.A. Neonatal vitamin A supplementation for the prevention of mortality and morbidity in term neonates in developing countries. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef]
- Hess, S.Y.; Brown, K.H. Impact of zinc fortification on zinc nutrition. Food Nutr. Bull. 2009, 30, 79S–107S. [Google Scholar] [CrossRef]
- NHS Centre for Reviews and Dissemination. CRD’s Guidance for Undertaking Reviews in Health Care; University of York: York, UK, 2008. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Longfils, P.; Monchy, D.; Weinheimer, H.; Chavasit, V.; Nakanishi, Y.; Schumann, K. A comparative intervention trial on fish sauce fortified with NaFe-EDTA and FeSO4+ citrate in iron deficiency anemic school children in Kampot, Cambodia. Asia Pac. J. Clin. Nutr. 2008, 17, 250–257. [Google Scholar] [PubMed]
- Thuy, P.V.; Berger, J.; Nakanishi, Y.; Khan, N.C.; Lynch, S.; Dixon, P. The Use of NaFeEDTA-Fortified Fish Sauce Is an Effective Tool for Controlling Iron Deficiency in Women of Childbearing Age in Rural Vietnam. J. Nutr. 2005, 135, 2596–2601. [Google Scholar] [PubMed]
- Thuy, P.V.; Berger, J.; Davidsson, L.; Khan, N.C.; Lam, N.T.; Cook, J.D.; Hurrell, R.F.; Khoi, H.H. Regular consumption of NaFeEDTA-fortified fish sauce improves iron status and reduces the prevalence of anemia in anemic Vietnamese women. Am. J. Clin. Nutr. 2003, 78, 284–290. [Google Scholar] [PubMed]
- Le, H.T.; Brouwer, I.D.; Nguyen, K.C.; Burema, J.; Kok, F.J. The effect of iron fortification and de-worming on anaemia and iron status of Vietnamese schoolchildren. Br. J. Nutr. 2007, 97, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Thi Le, H.; Brouwer, I.D.; Burema, J.; Nguyen, K.C.; Kok, F.J. Efficacy of iron fortification compared to iron supplementation among Vietnamese schoolchildren. Nutr. J. 2006, 5, 32. [Google Scholar] [CrossRef] [PubMed]
- Ballot, D.E.; MacPhail, A.P.; Bothwell, T.H.; Gillooly, M.; Mayet, F.G. Fortification of curry powder with NaFe(111)EDTA in an iron-deficient population: Report of a controlled iron-fortification trial. Am. J. Clin. Nutr. 1989, 49, 162–169. [Google Scholar] [PubMed]
- Asibey-Berko, E.; Zlotkin, S.H.; Yeung, G.S.; Nti-Nimako, W.; Ahunu, B.; Kyei-Faried, S.; Johnston, J.L.; Tondeur, M.C.; Mannar, V. Dual fortification of salt with iron and iodine in women and children in rural Ghana. East Afr. Med. J. 2007, 84, 473–480. [Google Scholar] [PubMed]
- Zimmermann, M.B.; Zeder, C.; Chaouki, N.; Saad, A.; Torresani, T.; Hurrell, R.F. Dual fortification of salt with iodine and microencapsulated iron: A randomized, double-blind, controlled trial in Moroccan schoolchildren. Am. J. Clin. Nutr. 2003, 77, 425–432. [Google Scholar] [PubMed]
- Zimmermann, M.B.; Zeder, C.; Chaouki, N.; Torresani, T.; Saad, A.; Hurrell, R.F. Addition of microencapsulated iron to iodized salt improves the efficacy of iodine in goitrous, iron-deficient children: A randomized, double-blind, controlled trial. Eur. J. Endocrinol. 2002, 147, 747–753. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Wegmueller, R.; Zeder, C.; Chaouki, N.; Rohner, F.; Saissi, M.; Torresani, T.; Hurrell, R.F. Dual fortification of salt with iodine and micronized ferric pyrophosphate: A randomized, double-blind, controlled trial. Am. J. Clin. Nutr. 2004, 80, 952–959. [Google Scholar] [PubMed]
- Andersson, M.; Thankachan, P.; Muthayya, S.; Goud, R.B.; Kurpad, A.V.; Hurrell, R.F.; Zimmermann, M.B. Dual fortification of salt with iodine and iron: A randomized, double-blind, controlled trial of micronized ferric pyrophosphate and encapsulated ferrous fumarate in southern India. Am. J. Clin. Nutr. 2008, 88, 1378–1387. [Google Scholar] [PubMed]
- Rajagopalan, S.; Vinodkumar, M. Effects of salt fortified with iron and iodine on the hamoglobin levels and productivity of tea pickers. Food Nutr. Bull. 2000, 21, 323–329. [Google Scholar] [CrossRef]
- Vinodkumar, M.; Rajagopalan, S.; Bhagwat, I.P.; Singh, S.; Parmar, B.S.; Mishra, O.P.; Upadhyay, S.S.; Bhalia, N.B.; Deshpande, S.R. A multicenter community study on the efficacy of double-fortified salt. Food Nutr. Bull. 2007, 28, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Vinodkumar, M.; Erhardt, J.G.; Rajagopalan, S. Impact of a multiple-micronutrient fortified salt on the nutritional status and memory of schoolchildren. Int. J. Vitam. Nutr. Res. 2009, 79, 348–361. [Google Scholar] [CrossRef] [PubMed]
- Manger, M.S.; McKenzie, J.E.; Winichagoon, P.; Gray, A.; Chavasit, V.; Pongcharoen, T.; Gowachirapant, S.; Ryan, B.; Wasantwisut, E.; Gibson, R.S. A micronutrient-fortified seasoning powder reduces morbidity and improves short-term cognitive function, but has no effect on anthropometric measures in primary school children in northeast Thailand: A randomized controlled trial. Am. J. Clin. Nutr. 2008, 87, 1715–1722. [Google Scholar] [PubMed]
- Winichagoon, P.; McKenzie, J.E.; Chavasit, V.; Pongcharoen, T.; Gowachirapant, S.; Boonpraderm, A.; Manger, M.S.; Bailey, K.B.; Wasantwisut, E.; Gibson, R.S. A multimicronutrient-fortified seasoning powder enhances the hemoglobin, zinc, and iodine status of primary school children in North East Thailand: A randomized controlled trial of efficacy. J. Nutr. 2006, 136, 1617–1623. [Google Scholar] [PubMed]
- Huo, J.; Sun, J.; Miao, H.; Yu, B. Effect of NaFeEDTA fortified soy sauce on iron deficiency anemia in students. Wei Sheng Yan Jiu 2001, 30, 296–298. [Google Scholar] [PubMed]
- Huo, J.; Sun, J.; Miao, H.; Yu, B.; Yang, T.; Liu, Z.; Lu, C.; Chen, J.; Zhang, D.; Ma, Y.; et al. Therapeutic effects of NaFeEDTA-fortified soy sauce in anaemic children in China. Asia Pac. J. Clin. Nutr. 2002, 11, 123–127. [Google Scholar] [PubMed]
- Chen, J.; Zhao, X.; Zhang, X.; Yin, S.; Piao, J.; Huo, J.; Yu, B.; Qu, N.; Lu, Q.; Wang, S.; et al. Studies on the effectiveness of NaFeEDTA-fortified soy sauce in controlling iron deficiency: A population-based intervention trial. Food Nutr. Bull. 2005, 26, 177–186. [Google Scholar] [PubMed]
- Lee, Y.M.; Skurk, T.; Hennig, M.; Hauner, H. Effect of a milk drink supplemented with whey peptides on blood pressure in patients with mild hypertension. Eur. J. Nutr. 2007, 46, 21–27. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. In Vitamin and Mineral Nutrition Information System; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Best, C.; Neufingerl, N.; Del Rosso, J.M.; Transler, C.; van den Briel, T.; Osendarp, S. Can multi-micronutrient food fortification improve the micronutrient status, growth, health, and cognition of schoolchildren? A systematic review. Nutr. Rev. 2011, 69, 186–204. [Google Scholar] [PubMed]
- Jiang, T.; Xue, Q. Fortified salt for preventing iodine deficiency disorders: A systematic review Chin. J. Evid. Based Med. 2010, 10, 857–861. [Google Scholar]
- Vucic, V.; Berti, C.; Vollhardt, C.; Fekete, K.; Cetin, I.; Koletzko, B.; Gurinovic, M.; van't Veer, P. Effect of iron intervention on growth during gestation, infancy, childhood, and adolescence: A systematic review with meta-analysis. Nutr. Rev. 2013, 71, 386–401. [Google Scholar] [CrossRef] [PubMed]
- Casgrain, A.; Collings, R.; Harvey, L.J.; Hooper, L.; Fairweather-Tait, S.J. Effect of iron intake on iron status: A systematic review and meta-analysis of randomized controlled trials Am. J. Clin. Nutr. 2012, 96, 768–780. [Google Scholar] [CrossRef] [PubMed]
- Van den Wijngaart, A.; Begin, F.; Codling, K.; Randall, P.; Johnson, Q.W. Regulatory monitoring systems of fortified salt and wheat flour in selected ASEAN countries. Food Nutr. Bull. 2013, 34, S102–S111. [Google Scholar] [CrossRef] [PubMed]
- Pena-Rosas, J.P.; De-Regil, L.M.; Rogers, L.M.; Bopardikar, A.; Panisset, U. Translating research into action: WHO evidence-informed guidelines for safe and effective micronutrient interventions. J. Nutr. 2012, 142, 197S–204S. [Google Scholar] [CrossRef] [PubMed]
- The Working Group. Use of common salt fortified with iron in the control and prevention of anemia—A collaborative study. Report of the Working Group on Fortification of Salt with Iron. Am. J. Clin. Nutr. 1982, 35, 1442–1451. [Google Scholar]
- Liu, P.; Bhatia, R.; Pachon, H. Food fortification in India. Indian J. Community Health 2014, 26, 59–74. [Google Scholar]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hess, S.; Tecklenburg, L.; Eichler, K. Micronutrient Fortified Condiments and Noodles to Reduce Anemia in Children and Adults—A Literature Review and Meta-Analysis. Nutrients 2016, 8, 88. https://doi.org/10.3390/nu8020088
Hess S, Tecklenburg L, Eichler K. Micronutrient Fortified Condiments and Noodles to Reduce Anemia in Children and Adults—A Literature Review and Meta-Analysis. Nutrients. 2016; 8(2):88. https://doi.org/10.3390/nu8020088
Chicago/Turabian StyleHess, Sascha, Linda Tecklenburg, and Klaus Eichler. 2016. "Micronutrient Fortified Condiments and Noodles to Reduce Anemia in Children and Adults—A Literature Review and Meta-Analysis" Nutrients 8, no. 2: 88. https://doi.org/10.3390/nu8020088
APA StyleHess, S., Tecklenburg, L., & Eichler, K. (2016). Micronutrient Fortified Condiments and Noodles to Reduce Anemia in Children and Adults—A Literature Review and Meta-Analysis. Nutrients, 8(2), 88. https://doi.org/10.3390/nu8020088