Adherence to the “Mediterranean Diet” in Spain and Its Relationship with Cardiovascular Risk (DIMERICA Study)

 , ,
, ,
Abstract
:1. Introduction
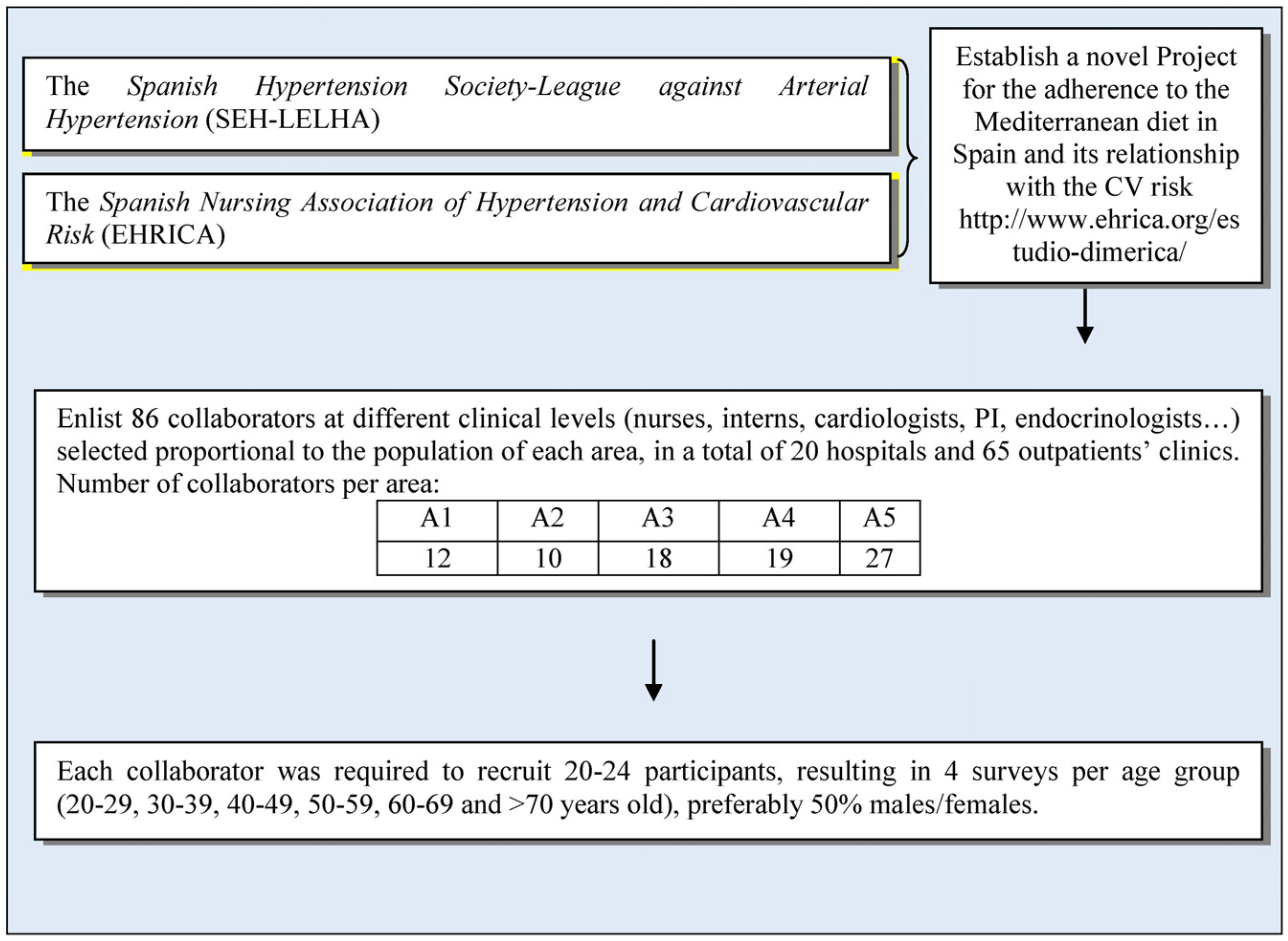
2. Methods
2.1. Study Design and Population
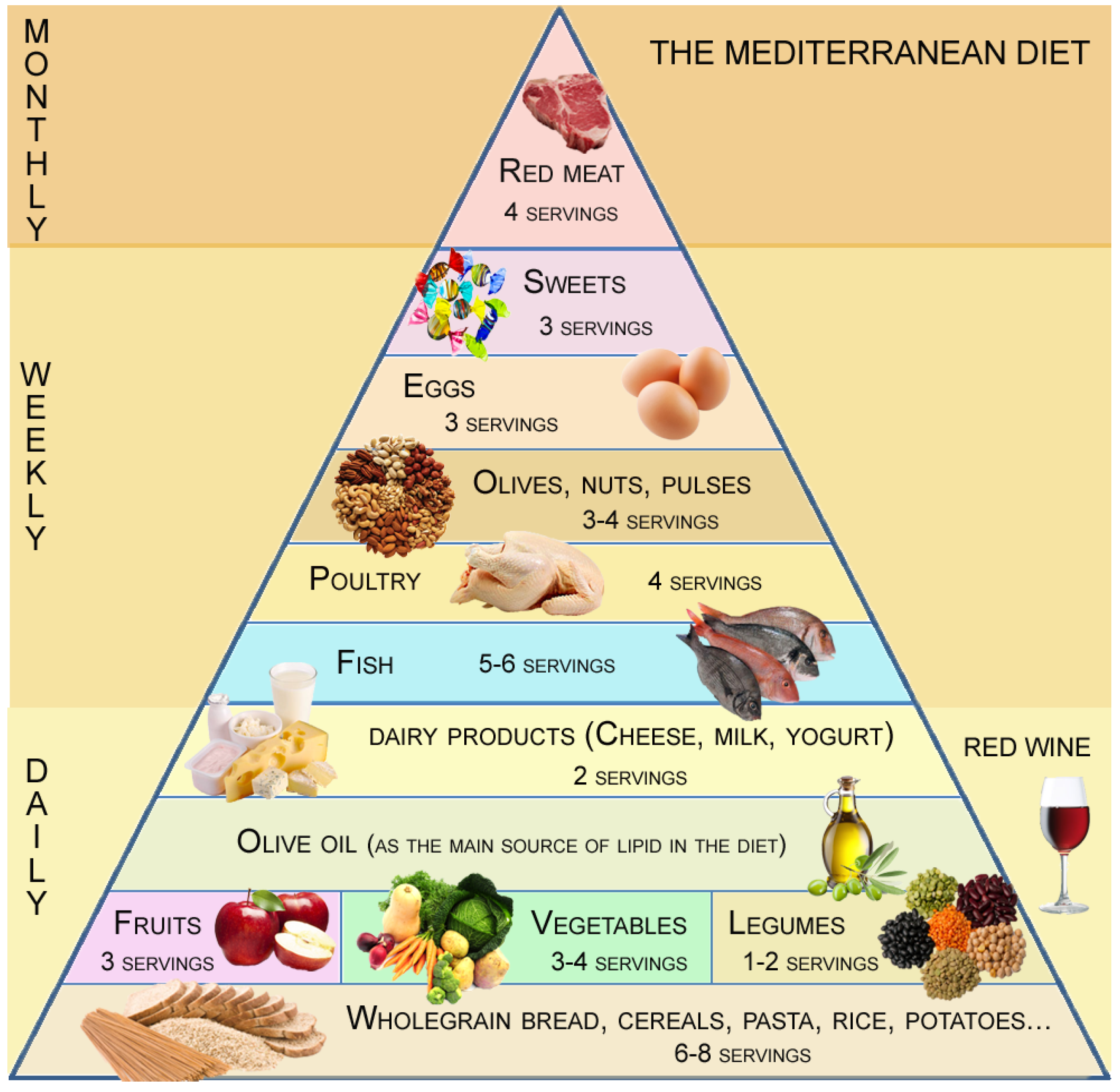
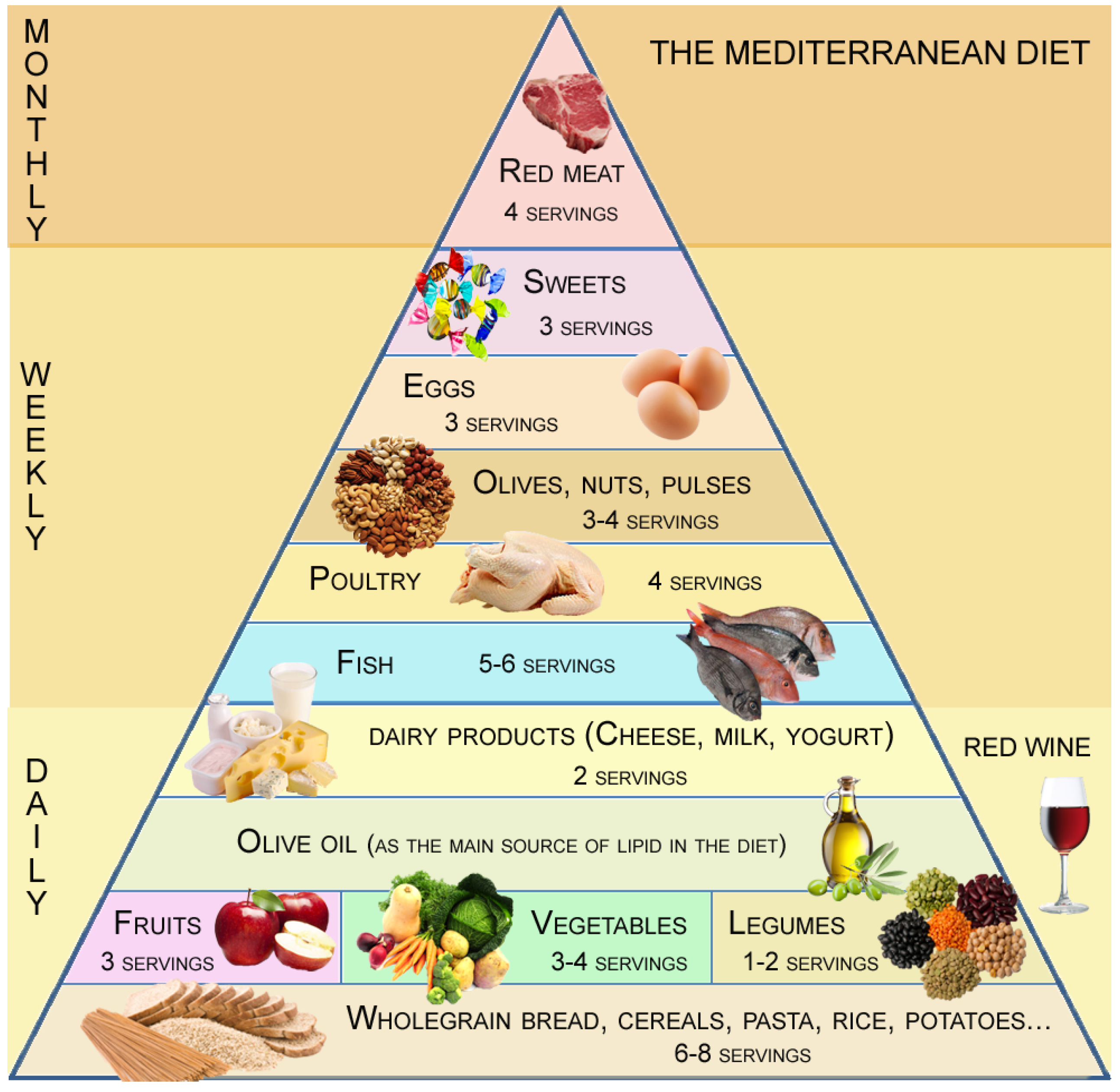
2.2. Survey and MD Score
- Question 1. Consumption of cereals. ≥5 portions per day.
- Question 2. Consumption of fruits. ≥3 portions per day.
- Question 3. Consumption of legumes. ≥2 portions per week.
- Question 4. Consumption of vegetables. ≥2 portions per day.
- Question 5. Consumption of fish. ≥3 portions per week.
- Question 6. Consumption of poultry meat. 1 ≤ portions per week ≤ 4.
- Question 7. Consumption of red meat. 1 ≤ portions per week ≤ 4.
- Question 8. Consumption of dairy products. 3–4 portions per day.
- Question 9. Consumption of different oils. Olive oil as preferred oil.
- Question 10. Use of olive oil for cooking. Daily use.
- Question 11. Consumption of nuts. >1 portion per week.
- Question 12. Consumption of factory-baked products. <1 per week.
- Question 13. Consumption of eggs. < 1 egg per week < 7.
- Question 14. Consumption of cold-meat. <2 per week.
- Question 15. Consumption of red wine. >1 glass per week.
- Score <5: Poor MD adherence, requiring improvement in dietary habits.
- Score 5–7: Average MD adherence, which could be improved with small modifications.
- Score >7: Good MD adherence.
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Cohort and Lifestyle
3.2. Mediterranean Diet in the Total Population
3.3. Mediterranean Diet in the Different Areas Studied
3.4. Dietary Preferences
3.5. MD Adherence and Cardiovascular Risk Factors Prevalence
4. Discussion
4.1. Definition of MD
4.2. Dietary Patterns per Area
4.3. Hypertension and Relationship with MD
4.4. Cardiovascular Risk Factors and MD Score
4.5. Limitations of the Study
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| A1 | Area 1 |
| A2 | Area 2 |
| A3 | Area 3 |
| A4 | Area 4 |
| A5 | Area 5 |
| CV | Cardiovascular |
| CVD | Cardiovascular Disease |
| DIMERICA | Dieta Mediterránea y su relación con el Riesgo Cardiovascular en España (Mediterranean Diet and its relation with Cardiovascular Risk in Spain) |
| EHRICA | Asociación Española de Enfermería de Hipertensión y Riesgo Cardiovascular (Spanish Nursing Association of Hypertension and Cardiovascular Risk) |
| MD | Mediterranean diet |
| SEH-LELHA | Sociedad Española de Hipertensión-Liga Española para la Lucha contra la Hipertensión Arterial (Spanish Hypertension Society-League against Arterial Hypertension) |
References
- Nichols, M.; Townsend, N.; Scarborough, P.; Rayner, M. Cardiovascular disease in Europe 2014: Epidemiological update. Eur. Heart J. 2014, 35, 2950–2959. [Google Scholar] [CrossRef] [PubMed]
- Chiuve, S.E.; Cook, N.R.; Shay, C.M.; Rexrode, K.M.; Albert, C.M.; Manson, J.E.; Willett, W.C.; Rimm, E.B. Lifestyle-based prediction model for the prevention of CVD: The Healthy Heart Score. J. Am. Heart Assoc. 2014, 3, e000954. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean diet and health status: Meta-analysis. BMJ 2008, 337, a1344. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; García-López, M.; Bes-Rastrollo, M.; Toledo, E.; Martínez-Lapiscina, E.H.; Delgado-Rodriguez, M.; Vazquez, Z.; Benito, S.; Beunza, J.J. Mediterranean diet and the incidence of cardiovascular disease: A Spanish cohort. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; de la Fuente-Arrillaga, C.; Nunez-Cordoba, J.M.; Basterra-Gortari, F.J.; Beunza, J.J.; Vazquez, Z.; Benito, S.; Tortosa, A.; Bes-Rastrollo, M. Adherence to Mediterranean diet and risk of developing diabetes: Prospective cohort study. BMJ 2008, 336, 1348–1351. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef] [PubMed]
- Hoevenaar-Blom, M.P.; Nooyens, A.C.; Kromhout, D.; Spijkerman, A.M.; Beulens, J.W.; van der Schouw, Y.T.; Bueno-de-Mesquita, B.; Verschuren, W.M. Mediterranean style diet and 12-year incidence of cardiovascular diseases: The EPIC-NL cohort study. PLoS ONE 2012, 7, e45458. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Domínguez, E.; de la Puerta, R.; Ruiz-Gutiérrez, V. Protective effects upon experimental inflammation models of a polyphenol-supplemented virgin olive oil diet. Inflamm. Res. 2001, 50, 102–106. [Google Scholar] [PubMed]
- Perez-Martinez, P.; Ordovas, J.M.; Garcia-Rios, A.; Delgado-Lista, J.; Delgado-Casado, N.; Cruz-Teno, C.; Camargo, A.; Yubero-Serrano, E.M.; Rodriguez, F.; Perez-Jimenez, F.; et al. Consumption of diets with different type of fat influences triacylglycerols-rich lipoproteins particle number and size during the postprandial state. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Allman-Farinelli, M.A.; Gomes, K.; Favaloro, E.J.; Petocz, P. A diet rich in high-oleic-acid sunflower oil favorably alters low-density lipoprotein cholesterol, triglycerides, and factor VII coagulant activity. J. Am. Diet. Assoc. 2005, 105, 1071–1079. [Google Scholar] [CrossRef] [PubMed]
- Arvaniti, F.; Panagiotakos, D.B.; Pitsavos, C.; Zampelas, A.; Stefanadis, C. Dietary habits in a Greek sample of men and women: The ATTICA study. Cent. Eur. J. Public Health 2006, 14, 74–77. [Google Scholar] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Vecchio, S.; Giuliani, G.; Martinelli, F.; Marcucci, R.; Gori, A.M.; Fedi, S.; Casini, A.; Surrenti, C.; Abbate, R.; et al. Dietary habits, lifestyle and cardiovascular risk factors in a clinically healthy Italian population: The ‘Florence’ diet is not Mediterranean. Eur. J. Clin. Nutr. 2005, 59, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Hulley, S.B.; Cummings, S.R.; Browner, W.S.; Grady, D.G.; Newman, T.B. Planificación de las Mediciones. In Diseño de la Investigación Clínica; Hulley, S.B., Ed.; SRCE: Barcelona, Spain, 1993; pp. 47–58. [Google Scholar]
- Athanasiadou, E.; Kyrkou, C.; Fotiou, M.; Tsakoumaki, F.; Dimitropoulou, A.; Polychroniadou, E.; Menexes, G.; Athanasiadis, A.P.; Biliaderis, C.G.; Michaelidou, A.M.; et al. Development and Validation of a Mediterranean Oriented Culture-Specific Semi-Quantitative Food Frequency Questionnaire. Nutrients 2016, 8, 522. [Google Scholar] [CrossRef] [PubMed]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; a Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [PubMed]
- León-Muñoz, L.M.; Guallar-Castillón, P.; Graciani, A.; López-García, E.; Mesas, A.E.; Aguilera, M.T.; Banegas, J.R.; Rodríguez-Artalejo, F. Adherence to the Mediterranean diet pattern has declined in Spanish adults. J. Nutr. 2012, 142, 1843–1850. [Google Scholar] [CrossRef] [PubMed]
- Valdés, J.; Grau, M.; Subirana, I.; Marrugat, J.; Covas, M.I.; Schröder, H. Secular trends in energy intake and diet quality in a Mediterranean population. Ann. Nutr. Metab. 2009, 54, 177–183. [Google Scholar] [PubMed]
- Rodríguez Artalejo, F.; Banegas, J.R.; Graciani, M.A.; Hernández Vecino, R.; Rey Calero, J. Food and nutrient consumption in Spain in the period 1940–1988. Analysis of its consistency with the Mediterranean diet. Med. Clin. 1996, 106, 161–168. [Google Scholar]
- Tur, J.A.; Romaguera, D.; Pons, A. Food consumption patterns in a mediterranean region: Does the mediterranean diet still exist? Ann. Nutr. Metab. 2004, 48, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Tur, J.A.; Romaguera, D.; Pons, A. Does the diet of the Balearic population, a Mediterranean-type diet, ensure compliance with nutritional objectives for the Spanish population? Public Health Nutr. 2005, 8, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Pitsavos, C.; Matalas, A.L.; Chrysohoou, C.; Stefanadis, C. Geographical influences on the association between adherence to the Mediterranean diet and the prevalence of acute coronary syndromes, in Greece: The CARDIO2000 study. Int. J. Cardiol. 2005, 100, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Tyrovolas, S.; Haro, J.M.; Polychronopoulos, E.; Mariolis, A.; Piscopo, S.; Valacchi, G.; Makri, K.; Zeimbekis, A.; Tyrovola, D.; Bountziouka, V.; et al. Factors associated with components of arterial pressure among older individuals (the multinational MEDIS study): The role of the Mediterranean diet and alcohol consumption. J. Clin. Hypertens. (Greenwich) 2014, 16, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Guallar-Castillón, P.; Rodríguez-Artalejo, F.; Tormo, M.J.; Sánchez, M.J.; Rodríguez, L.; Quirós, J.R.; Navarro, C.; Molina, E.; Martínez, C.; Marín, P.; et al. Major dietary patterns and risk of coronary heart disease in middle-aged persons from a Mediterranean country: The EPIC-Spain cohort study. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Buckland, G.; González, C.A.; Agudo, A.; Vilardell, M.; Berenguer, A.; Amiano, P.; Ardanaz, E.; Arriola, L.; Barricarte, A.; Basterretxea, M.; et al. Adherence to the Mediterranean diet and risk of coronary heart disease in the Spanish EPIC Cohort Study. Am. J. Epidemiol. 2009, 170, 1518–1529. [Google Scholar] [CrossRef] [PubMed]
- Lau, K.K.; Wong, Y.K.; Chan, Y.H.; Li, O.Y.; Lee, P.Y.; Yuen, G.G.; Wong, Y.-K.; Tong, S.; Wong, D.; Chan, K.-H.; et al. Mediterranean-style diet is associated with reduced blood pressure variability and subsequent stroke risk in patients with coronary artery disease. Am. J. Hypertens. 2015, 28, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Hoşcan, Y.; Yiğit, F.; Müderrisoğlu, H. Adherence to Mediterranean diet and its relation with cardiovascular diseases in Turkish population. Int. J. Clin. Exp. Med. 2015, 8, 2860–2866. [Google Scholar] [PubMed]
- Esmaillzadeh, A.; Azadbakht, L. Food intake patterns may explain the high prevalence of cardiovascular risk factors among Iranian women. J. Nutr. 2008, 138, 1469–1475. [Google Scholar] [PubMed]
- D’Alessandro, A.; De Pergola, G. Mediterranean Diet and Cardiovascular Disease: A Critical Evaluation of A Priori Dietary Indexes. Nutrients 2015, 7, 7863–7888. [Google Scholar] [CrossRef] [PubMed]
- Bertomeu, V.; Castillo-Castillo, J. Situación de la enfermedad cardiovascular en España. Rev. Esp. Cardiol. Supl. 2008, 8, 2–9. [Google Scholar]
- Estruch, R.; Ros, E.; Martínez-González, M.A. Mediterranean diet for primary prevention of cardiovascular disease. N. Engl. J. Med. 2013, 369, 676–677. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Artalejo, F.; Graciani, A.; Guallar-Castillón, P.; León-Muñoz, L.M.; Zuluaga, M.C.; López-García, E.; Gutiérrez-Fisac, J.L.; Taboada, J.M.; Aguilera, M.T.; Regidor, E.; et al. Rationale and methods of the study on nutrition and cardiovascular risk in Spain (ENRICA). Rev. Esp. Cardiol. 2011, 64, 876–882. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Total Population (n = 1732) | Area 1 (n = 221) | Area 2 (n = 149) | Area 3 (n = 621) | Area 4 (n = 277) | Area 5 (n = 464) | p Value | |
|---|---|---|---|---|---|---|---|
| Age | 51 (37–65) | 50.0 (36–65) | 49.0 (36–64) | 52.0 (38–66) | 50.0 (36–64) | 51.0 (37–65) | 0.56 |
| Males, % | 47% | 50.0% | 47.4% | 44.8% | 49.5.5% | 46.8% | 0.77 |
| Weight (kg) | 72 (62–82) | 73 (64–84) | 70 (59–80) | 72 (62–82) | 72 (62–84) | 71 (61–81.5) | 0.06 |
| Height (cm) | 166 (160–173) | 166 (161–173) | 167 (160–174) | 165 (159–172) | 168 (160–174) | 165 (160–173) | 0.07 |
| Body mass index category (kg/m2) | 25.6 (22.7–29.2) | 25.7 (22.8–29.8) | 24.8 (21.9–28.1) | 25.8 (22.8–29.7) | 25.6 (22.8–29.2) | 25.4 (22.3–28.5) | 0.09 |
| Normal weight (18.5–24.9 kg/m2) | 43.8% | 43.8% | 48% | 46% | 42.7% | 45.9% | 0.31 |
| Overweight (25.0–29.9 kg/m2) | 35.2% | 31.6% | 33.5% | 35.5% | 36.7% | 34.9% | 0.31 |
| Obese (BMI ≥ 30.0 kg/m2) | 21% | 24.6% | 18.5% | 14.5% | 20.6% | 19.2% | 0.04 |
| Waist circumference (cm) | 92 (82–101) | 91 (82–103) | 90 (79–99) | 93 (81–103) | 93 (83,–102) | 90 (83–99) | 0.11 |
| Trouser size | 44 (40–48) | 44 (40–48) | 42 (40–46) | 44 (40–48) | 44 (40–48) | 43 (40–48) | 0.07 |
| Smoking, % | 19.2% | 17.9% | 21.7% | 18.2% | 18.5% | 20.7% | 0.005 |
| Dyslipidemia, % | 21.5% | 20.1% | 16.4% | 22.3% | 21.7% | 22.5% | 0.54 |
| Diabetes mellitus, % | 10.4% | 9.8% | 8.6% | 10.1% | 12.1% | 9.8% | 0.95 |
| Hypertension, % | 25.5% | 30.4% | 23.0% | 27.7% | 17.8% | 25.5% | 0.012 |
| University Degree, % | 44.2% | 39.3% | 42.8% | 42.9% | 48% | 45.5% | 0.48 |
| Total (n = 1732) | Area 1 (n = 210) | Area 2 (n = 147) | Area 3 (n = 617) | Area 4 (n = 262) | Area 5 (n = 456) | p Value | |
|---|---|---|---|---|---|---|---|
| Physical activity level, % | |||||||
| Daily, % | 39.5 | 37.5 | 34.9 | 35.8 | 33.5 | 32.4 | NS |
| 4–5 times per week, % | 12.9 | 10.3 | 9.9 | 12.9 | 8.9 | 11.7 | NS |
| 2–3 times per week, % | 24.1 | 20.1 | 16.4 | 20.8 | 20.3 | 24.0 | NS |
| Never (sedentary), % | 23.1 | 18.8 | 26.3 | 16.6 | 24.2 | 21.7 | NS |
| Watching Television, h/day, % | |||||||
| <1, % | 22.9 | 19.2 | 23.1 | 20.6 | 19.6 | 25.0 | NS |
| 1–2, % | 42.6 | 42.9 | 45.4 | 37.5 | 38.4 | 40.7 | NS |
| ≥2, % | 34.2 | 31.7 | 28.5 | 33.4 | 35.2 | 29.4 | NS |
| >7 | 4–6 | 3–4 | 1–2 | None | |
| Cereals per day, % | 3.6 | 10.7 | 39.9 | 44.6 | 1.1 |
| Fruits per day, % | 2.0 | 7.2 | 29.9 | 53.9 | 6.9 |
| >2 | 2 | 1 | <1 | none | |
| Vegetables per day, % | 9.5 | 29.8 | 45.2 | 14.2 | 1.2 |
| >4 | 3–4 | 1–2 | <1 | none | |
| Legumes weekly, % | 2.0 | 20.1 | 62.0 | 12.8 | 2.4 |
| Fish weekly, % | 5.5 | 30.2 | 54.0 | 8.7 | 1.7 |
| White meat weekly, % | 5.6 | 31.6 | 54.7 | 6.0 | 2.1 |
| Other meat weekly, % | 4.4 | 18.7 | 55.9 | 15.8 | 5.2 |
| Dairy products daily, % | 4.5 | 28.5 | 63.9 | 1.9 | 1.0 |
| >7 | 4–7 | 1–3 | <1 | none | |
| Red wine (in moderation), weekly,% | 5.8 | 9.0 | 13.6 | 22.9 | 48.4 |
| Daily | 3–5 | 1–2 | <1 | none | |
| Olive oil for cooking weekly, % | 89.9 | 4.4 | 2.6 | 1.5 | 1.6 |
| Factory-baked products weekly, % | 5.2 | 7.1 | 17.7 | 34.7 | 35.2 |
| >5 | 3–4 | 1–2 | <1 | none | |
| Nuts weekly, % | 6.2 | 10.0 | 25.9 | 38.8 | 19.1 |
| Cold-meat weekly, % | 9.5 | 24.7 | 36.1 | 19.5 | 10.2 |
| Area 1 (n = 221) | Area 2 (n = 149) | Area 3 (n = 621) | Area 4 (n = 227) | Area 5 (n = 464) | p Value | |
|---|---|---|---|---|---|---|
| Cereals, >5/day, % | 21.9 | 15.1 | 13.4 | 14.5 | 13.1 | <0.001 |
| Fruits, >3/day, % | 40.4 | 36.1 | 42.6 | 40.4 | 30.5 | <0.05 |
| Legumes, 3–4/week, % | 33.2 | 23.2 | 16.1 | 24.5 | 16.6 | <0.001 |
| Red meat, <1/week, % | 22.6 | 13.4 | 20.7 | 35.5 | 26.2 | <0.001 |
| Poultry, 3–4/week, % | 29.8 | 27.7 | 28.9 | 34.1 | 35.9 | 0.39 |
| Eggs, >3 week, % | 49.0 | 48.9 | 29.6 | 40.5 | 27.9 | <0.001 |
| Fish, >3 week, % | 35.6 | 35.5 | 41.2 | 36.9 | 27.2 | <0.001 |
| Dairy products, daily, % | 61.9 | 66.0 | 63.4 | 59.5 | 68.1 | 0.062 |
| Area 1 (n = 221) | Area 2 (n = 149) | Area 3 (n = 621) | Area 4 (n = 277) | Area 5 (n = 464) | p Value | |
|---|---|---|---|---|---|---|
| Score | 5.3 (4.0, 6.0) *,† | 5.3 (4.0, 6.0) *,† | 4.6 (3.3, 6.0) | 5.3 (4.0, 6.0) *,† | 4.6 (3.3, 4.6) | <0.001 |
| Hypertension (n = 462) | No Hypertension (n = 1239) | p Value | |
|---|---|---|---|
| Diabetes mellitus, % | 22.8 | 6.3 | <0.05 |
| Dyslipidemia, % | 44.1 | 19.4 | <0.05 |
| Smoking, % | 19.2 | 28.3 | <0.05 |
| Overweight, % | 81.6 | 44.6 | <0.05 |
| Adherence score | 4.6 (3.3–6.0) | 5.3 (4.0–6.0) | 0.017 † |
| Adherence score ≥ 7, % | 7.9 | 11.5 | <0.05 |
| Poultry, 3–4/week, % | 30.3 | 35.9 | <0.05 |
| Red meat, 3–4/week, % | 27.2 | 19.2 | <0.05 |
| Fish, >3 week, % | 28.5 | 35.5 | <0.05 |
| Fruits, 3–4/daily, % | 27.9 | 34.3 | <0.05 |
| Covariate | Unadjusted OR (95% CI) | Adjusted OR a (95% CI) | Adjusted OR b (95% CI) |
|---|---|---|---|
| Adherence score ≥ 7 | 0.66 (0.47–0.94) * | 1.02 (0.63–1.61) | 0.84 (0.58–1.13) |
| Fruits, 3–4/daily | 1.03 (0.76–1.28) | 0.84 (0.63–1.13) | |
| Poultry, 3–4/week | 0.82 (0.66–1.02) | 0.77 (0.57–1.03) | |
| Fish, >3 week | 0.78 (0.63–0.98) * | 0.71 (0.52–0.97) * | |
| Red meat, <3–4/week | 0.68 (0.53–0.87) * | 0.68 (0.49–0.96) * |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abellán Alemán, J.; Zafrilla Rentero, M.P.; Montoro-García, S.; Mulero, J.; Pérez Garrido, A.; Leal, M.; Guerrero, L.; Ramos, E.; Ruilope, L.M. Adherence to the “Mediterranean Diet” in Spain and Its Relationship with Cardiovascular Risk (DIMERICA Study). Nutrients 2016, 8, 680. https://doi.org/10.3390/nu8110680
Abellán Alemán J, Zafrilla Rentero MP, Montoro-García S, Mulero J, Pérez Garrido A, Leal M, Guerrero L, Ramos E, Ruilope LM. Adherence to the “Mediterranean Diet” in Spain and Its Relationship with Cardiovascular Risk (DIMERICA Study). Nutrients. 2016; 8(11):680. https://doi.org/10.3390/nu8110680
Chicago/Turabian StyleAbellán Alemán, José, María Pilar Zafrilla Rentero, Silvia Montoro-García, Juana Mulero, Alfonso Pérez Garrido, Mariano Leal, Lucía Guerrero, Elena Ramos, and Luis Miguel Ruilope. 2016. "Adherence to the “Mediterranean Diet” in Spain and Its Relationship with Cardiovascular Risk (DIMERICA Study)" Nutrients 8, no. 11: 680. https://doi.org/10.3390/nu8110680