Analysis of Body Composition and Food Habits of Spanish Celiac Women


Abstract
:1. Introduction
2. Experimental Section
2.1. Participants and Procedure
2.2. Anthropometric Measurements
2.3. Body Composition and Energy Expenditure
2.4. Dietary Assessment
2.5. Mediterranean-Diet Score
2.6. Statistical Analysis
3. Results
3.1. Anthropometric and Body Composition Measurements

{kind=link}
{kind=link}
{kind=link}
| Characteristic | Women |
|---|---|
| n | 54 |
| Age (year) | 34.4 ± 12.9 |
| Mean duration of GFD ( year) | 10.9 ± 8.5 |
| Height (cm) | 164 ± 6 |
| Weight (kg) | 57.9 ± 7.3 |
| Body Fat % | 27.1 ± 6.9 |
| Body-mass index | |
| Mean (kg/m2) | 21.4 ± 27 |
| Underweight <18.5—no. (%) | 6 (11.1) |
| Normal 18.5–24.9—no. (%) | 44 (81.5) |
| Overweight 25–30—no. (%) | 4 (7.4) |
3.2. Dietary Intakes
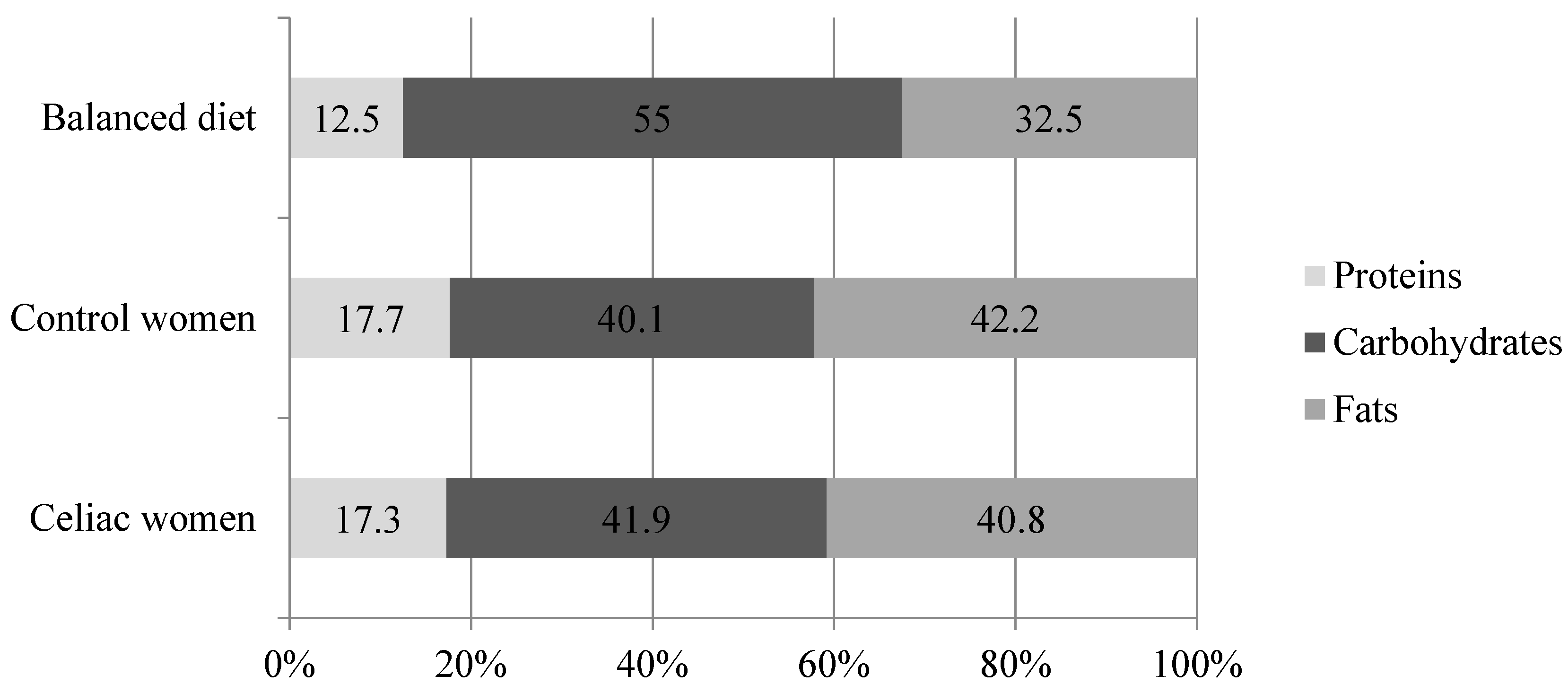
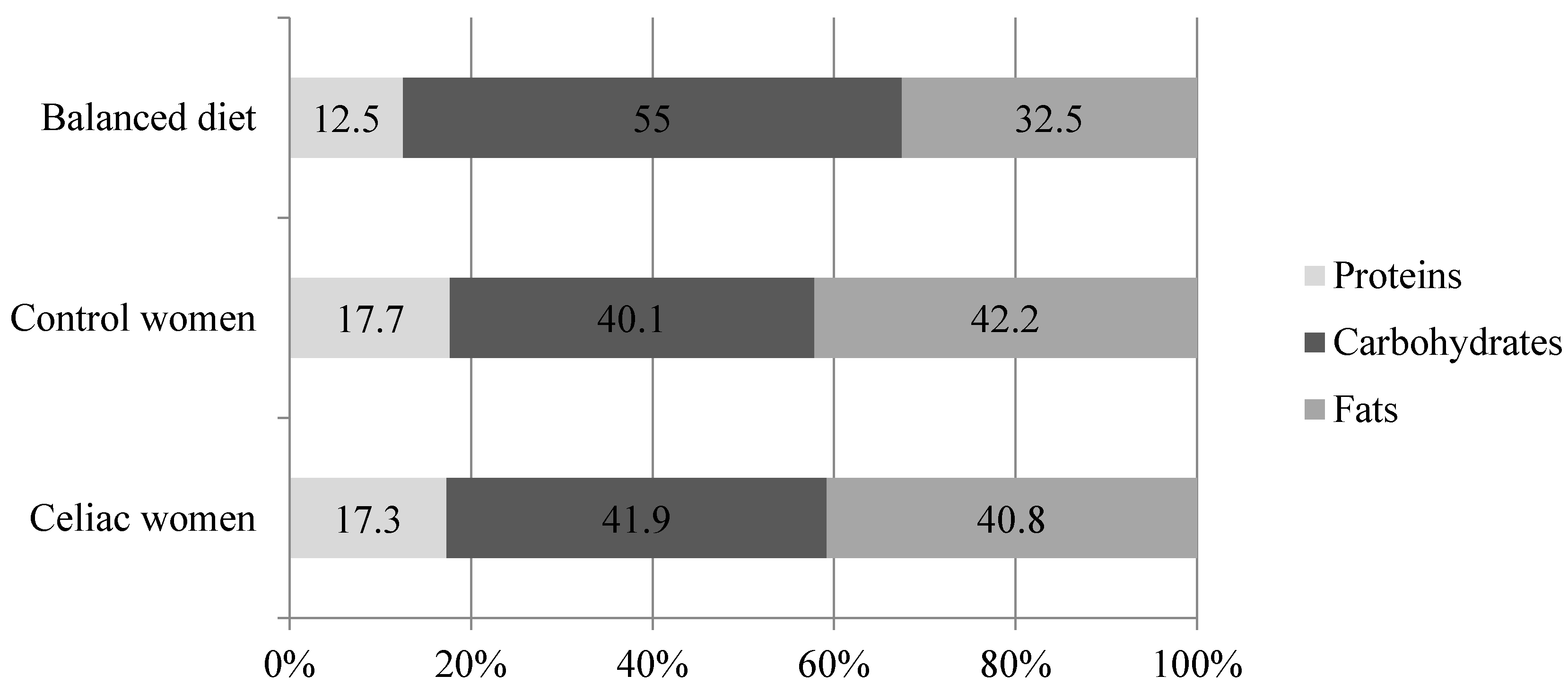
3.2.1. Energy, Macronutrients and Fiber
| Celiac Women ( n = 54) | Spanish Women—Control Women (n = 1734) | p | |
|---|---|---|---|
| Energy (kcal) | 1847 ± 362 | 2038 ± 655 | 0.003 |
| Protein (g) | 79.2 ± 16.6 | 88.0 ± 37.8 | < 0.001 |
| Carbohydrate (g) | 192.3 ± 40.7 | 199.7 ± 75.9 | 0.002 |
| Fat (g) | 84.6 ± 23.0 | 93.2 ± 35.6 | 0.022 |
| (PUFA+MUFA)/SFA | 2.1 | 2.0 | - |
| PUFA/SFA | 0.49 | 0.49 | - |
| Cholesterol (mg) | 324 ± 137 | 336 ± 151 | 0.544 |
| Fiber (g) | 16.4 ± 5.6 | 18.9 ± 10.1 | 0.002 |
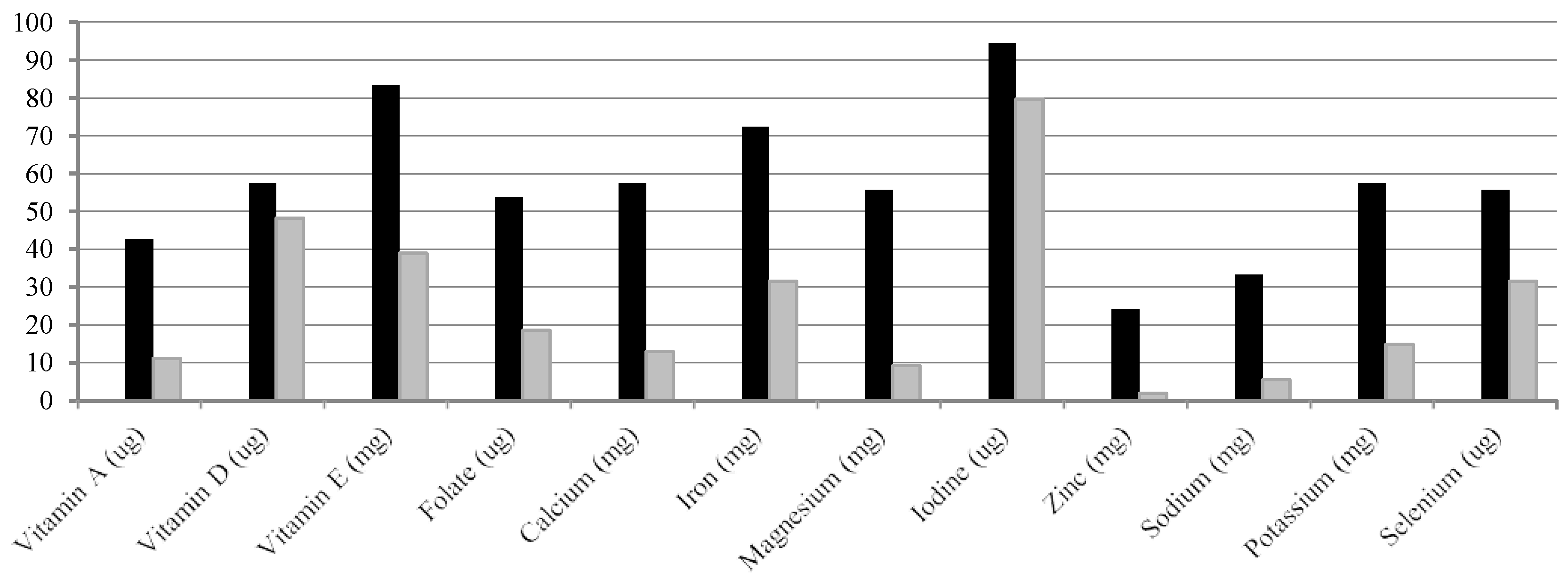
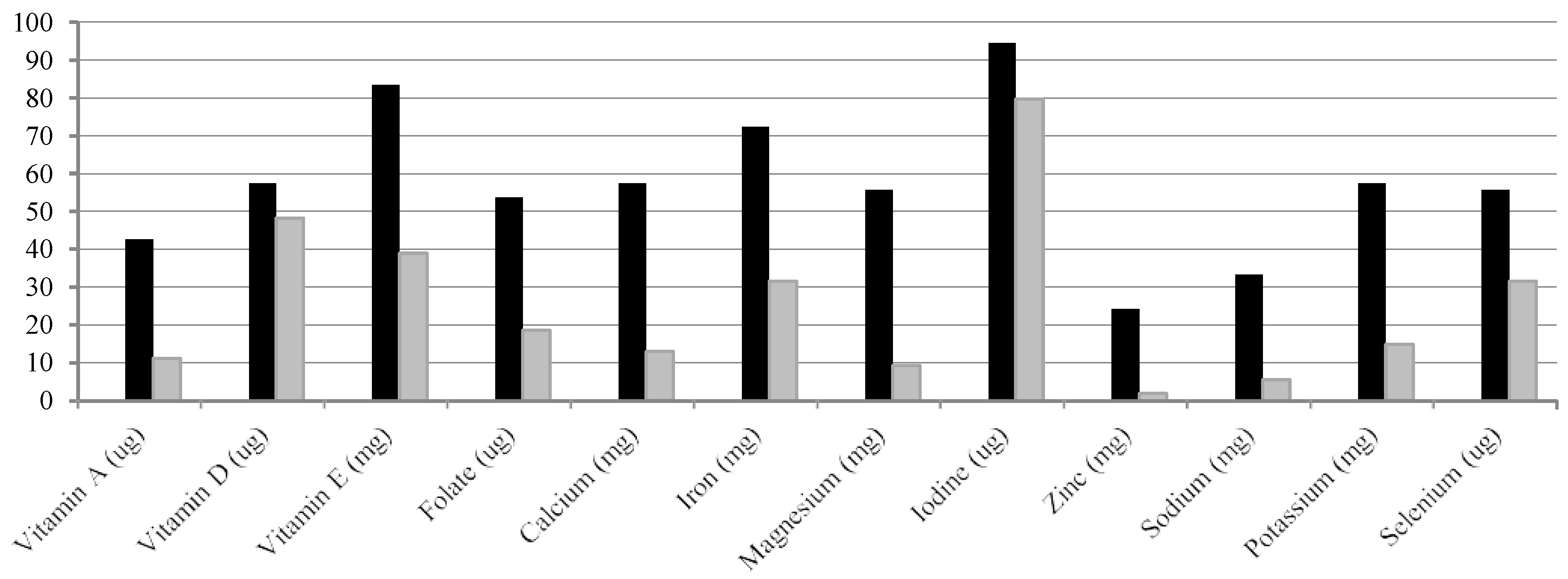
3.2.2. Micronutrients
| Celiac Women (n = 54) | Spanish Women—Control Women (n = 1734) | p | DRI FESNAD (2010) [14] | DRI: RDA and AI IoM (2011) [15] | |
|---|---|---|---|---|---|
| Vitamin A (μg) | 819 ± 556 | 723 ± 323 | 0.001 | 600 | 700 |
| Thiamin (mg) | 2.1 ± 3.5 | 1.8 ± 4.9 | 0.056 | 1 | 1.1 k |
| Riboflavin (mg) | 2.1 ± 1.5 | 1.4 ± 3.2 | 0.001 | 1.3 a | 1.1 k |
| Vitamin B6 (mg) | 2.1 ± 0.8 | 1.7 ± 3.7 | < 0.001 | 1.2 b | 1.3 b |
| Vitamin B12 (μg) | 8.1 ± 5.6 | 6.1 ± 4.9 | 0.230 | 2 | 2.4 |
| Vitamin C (mg) | 153 ± 65 | 133 ± 80 | 0.180 | 60 c | 75 |
| Vitamin D (μg) | 4.9 ± 4.0 | 3.7 ± 3.7 | 0.331 | 5 | 15 |
| Vitamin E (mg) | 11.2 ± 3.8 | 13.4 ± 7.0 | 0.003 | 15 | 15 |
| Niacin (mg) | 26.4 ± 11.4 | 39.4 ± 39.7 | < 0.001 | 14 | 14 |
| Folate (μg) | 373 ± 556 | 266 ± 113 | < 0.001 | 300 | 400 j |
| Calcium (mg) | 897 ± 264 | 835 ± 293 | 0.274 | 900 d | 1000 d |
| Iron (mg) | 14.5 ± 5.0 | 13.7 ± 6.2 | 0.162 | 18 e | 18 e |
| Magnesium (mg) | 297 ± 92 | 354 ± 126 | 0.011 | 300 f | 320 f |
| Iodine (μg) | 78.7 ± 38.7 | 84.8 ± 47.3 | 0.187 | 150 | 150 |
| Phosphorus (mg) | 1223 ± 314 | 1295 ± 380 | 0.191 | 700 g | 700 g |
| Zinc (mg) | 9.2 ± 4.0 | 8.7 ± 3.3 | 0.156 | 7 g | 8 |
| Sodium (mg) | 1916 ± 802 | 2349 ± 810 | 0.505 | 1500 | 1500 l |
| Potassium (mg) | 2950 ± 806 | 2858 ± 827 | 0.485 | 3100 h | 4700 |
| Selenium (μg) | 48.2 ± 19.3 | 53.7 ± 28.9 | 0.031 | 55 i | 55 |
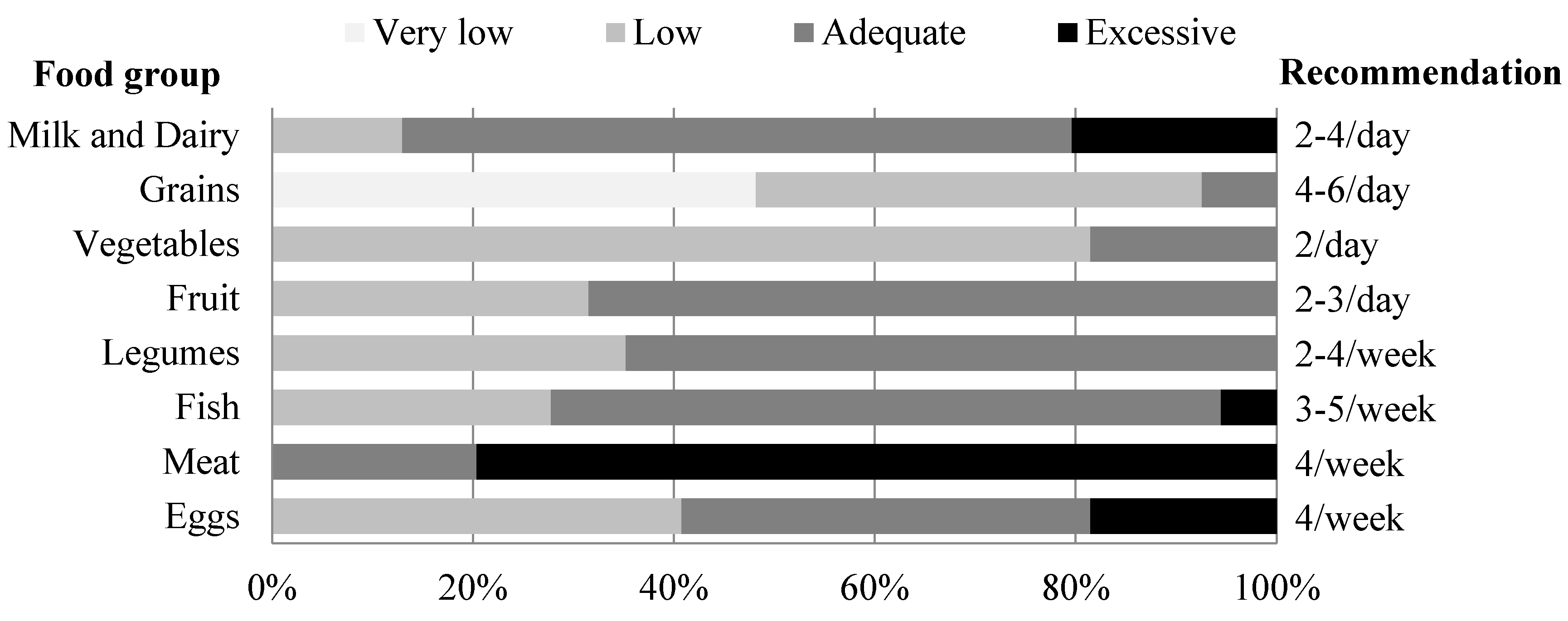
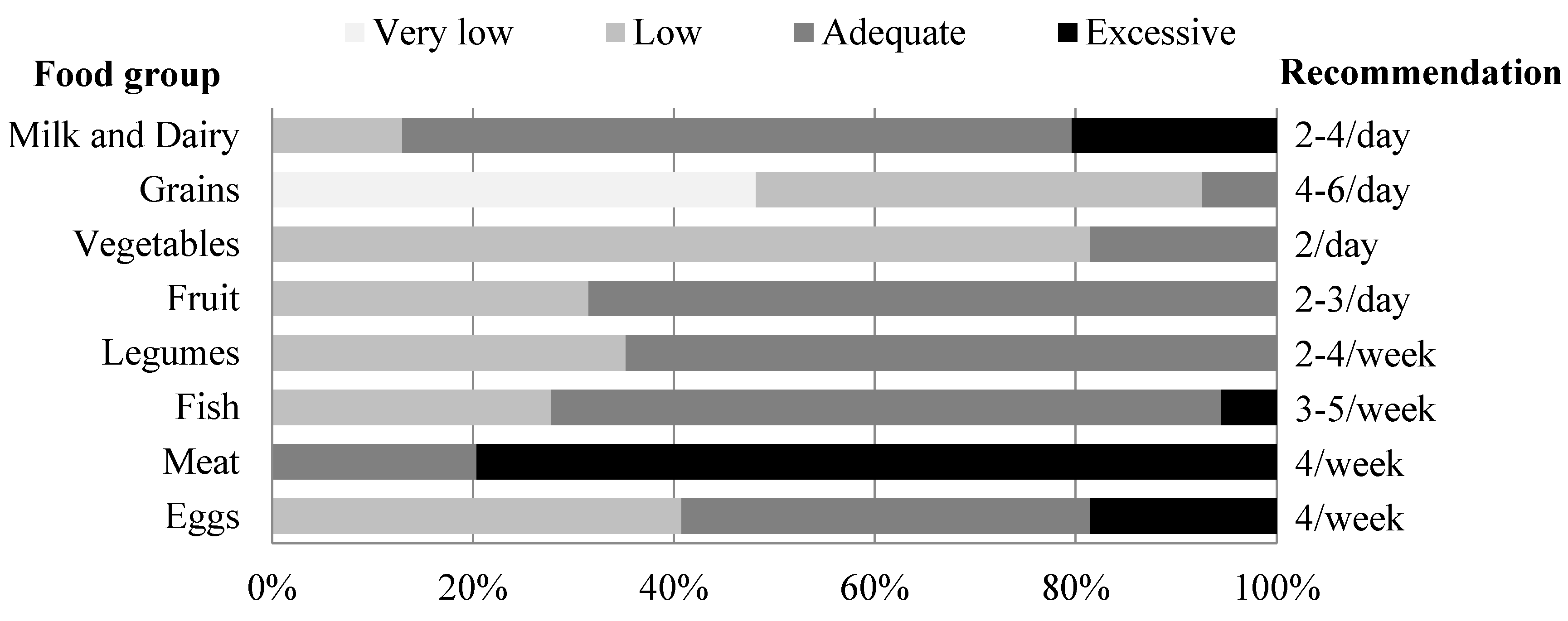
3.3. Food Consumption Frequency
3.4. Score for Adherence to Mediterranean Diet
4. Discussion
| Compliance/Suggestion | ||
|---|---|---|
| Celiac Women | Spanish Women—Control Women | |
| Energy intake (kcal) | √ | |
| Obese and overweight (%) | √ | ×/↓ |
| Macronutrient distribution | ||
| Protein (%) | ×/↓ | |
| Carbohydrate (%) | ×/↑ | |
| Fat (%) | ×/↓ | |
| Fiber (g) | ×/↑↑ | ×/↑ |
| Micronutrient intake | ||
| Vitamin D (μg) | ×/↑ | |
| Vitamin E (mg) | ×/↑ | |
| Folate (μg) | ×/↑ | |
| Calcium (mg) | ×/↑ | |
| Iron (mg) | ×/↑ | |
| Iodine (μg) | ×/↑ | |
| Selenium (μg) | ×/↑ | |
| Food consumption frequency | ||
| Grains | ×/↑ | √/= |
| Legumes | √/= | ×/↑ |
| Vegetables | ×/↑ | |
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ludvigsson, J.F.; Green, P.H. Clinical management of coeliac disease. J. Int. Med. 2011, 269, 560–571. [Google Scholar] [CrossRef] [PubMed]
- Catassi, C.; Gatti, S.; Fasano, A. The new epidemiology of celiac disease. J Pediatr. Gastroenterol. Nutr. 2014, 59, S7–S9. [Google Scholar] [CrossRef] [PubMed]
- Catassi, C.; Fabiani, E.; Iacono, G.; D’Agate, C.; Francavilla, R.; Biagi, F.; Volta, U.; Accomando, S.; Picarelli, A.; de Vitis, I.; et al. A prospective, double-blind, placebo-controlled trial to establish a safe gluten threshold for patients with celiac disease. Am. J. Clin. Nutr. 2007, 85, 160–166. [Google Scholar] [PubMed]
- Rajpoot, P.; Makharia, G.K. Problems and challenges to adaptation of gluten free diet by Indian patients with celiac disease. Nutrients 2013, 5, 4869–4879. [Google Scholar] [CrossRef] [PubMed]
- Gibert, A.; Kruizinga, A.G.; Neuhold, S.; Houben, G.F.; Canela, M.A.; Fasano, A.; Catassi, C. Might gluten traces in wheat substitutes pose a risk in patients with celiac disease? A population-based probabilistic approach to risk estimation. Am. J. Clin. Nutr. 2013, 97, 109–116. [Google Scholar] [CrossRef] [PubMed]
- American-Dietetic-Association. Celiac disease. In Evidence Based Nutrition Practice Guideline; American-Dietetic-Association: Chicago, IL, USA, 2009. [Google Scholar]
- Saturni, L.; Ferretti, G.; Bacchetti, T. The gluten-free diet: Safety and nutritional quality. Nutrients 2010, 2, 16–34. [Google Scholar] [CrossRef] [PubMed]
- Pietzak, M.M. Follow-up of patients with celiac disease: Achieving compliance with treatment. Gastroenterology 2005, 128, S135–S141. [Google Scholar] [CrossRef] [PubMed]
- Valdimarsson, T.; Toss, G.; Löfman, O.; Ström, M. Three years’ follow-up of bone density in adult coeliac disease: Significance of secondary hyperparathyroidism. Scand. J. Gastroenterol. 2000, 35, 274–280. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Obesity: Preventing and managing the global epidemic. In Report of a WHO Consultation on Obesity; World Health Organization: Geneva, Switzerland, 1997; p. 276. [Google Scholar]
- Gallagher, D.; Heymsfield, S.B.; Heo, M.; Jebb, S.A.; Murgatroyd, P.R.; Sakamoto, Y. Healthy percentage body fat ranges: An approach for developing guidelines based on body mass index. Am. J. Clin. Nutr. 2000, 72, 694–701. [Google Scholar] [PubMed]
- Miranda, J.; Lasa, A.; Bustamante, M.A.; Churruca, I.; Simon, E. Nutritional differences between a gluten-free diet and a diet containing equivalent products with gluten. Plant. Foods. Hum. Nutr. 2014, 69, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Russolillo, G.; Marques, I. Food Portion Sizes Album; Imagen Comunicación Multimedia: Madrid, Spain, 2008; p. 186. [Google Scholar]
- Federation of Spanish Societies of Nutrition and Dietetics (FESNAD). Dietary reference intakes (DRI) for spanish population, 2010. Act Diet. 2010, 14, 196–197. [Google Scholar]
- Ross, C.; Taylor, C.; Yaktine, A.; del Valle, H. Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Press: Washington, DC, USA, 2011; p. 1132. [Google Scholar]
- Aranceta, J.; Serra-Majem, L. Dietary guidelines for the Spanish population. Public. Health. Nutr. 2001, 4, 1403–1408. [Google Scholar] [CrossRef] [PubMed]
- Nutritional Assessment Studies: Spanish Population Dietary Intakes. National Health Survey. ENIDE. Available online: http://aesan.msssi.gob.es/AESAN/web/evaluacion_riesgos/seccion/estudios_evaluacion_nutricional.shtml (accessed on 25 May 2015).
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Aranceta, J. Nutritional objectives for the Spanish population: Consensus from the Spanish Society of Community Nutrition. Public Health Nutr. 2001, 4, 1409–1413. [Google Scholar] [CrossRef] [PubMed]
- Bardella, M.T.; Fredella, C.; Prampolini, L.; Molteni, N.; Giunta, A.M.; Bianchi, P.A. Body composition and dietary intakes in adult celiac disease patients consuming a strict gluten-free diet. Am. J. Clin. Nutr. 2000, 72, 937–939. [Google Scholar] [PubMed]
- Pedrera-Zamorano, J.D.; Roncero-Martin, R.; Lavado-Garcia, J.M.; Calderon-Garcia, J.F.; Rey-Sanchez, P.; Vera, V.; Martinez, M.; Moran, J.M. Segmental fat-free and fat mass measurements by bioelectrical impedance analysis in 2224 healthy Spanish women aged 18–85 years. Am. J. Hum. Biol. 2014. [Google Scholar] [CrossRef]
- Wierdsma, N.J.; van Bokhorst-de van der Schueren, M.A.; Berkenpas, M.; Mulder, C.J.; van Bodegraven, A.A. Vitamin and mineral deficiencies are highly prevalent in newly diagnosed celiac disease patients. Nutrients 2013, 5, 3975–3992. [Google Scholar] [CrossRef] [PubMed]
- Lanzini, A.; Lanzarotto, F.; Villanacci, V.; Mora, A.; Bertolazzi, S.; Turini, D.; Carella, G.; Malagoli, A.; Ferrante, G.; Cesana, B.M.; et al. Complete recovery of intestinal mucosa occurs very rarely in adult coeliac patients despite adherence to gluten-free diet. Aliment. Pharmacol. Ther. 2009, 29, 1299–1308. [Google Scholar] [CrossRef] [PubMed]
- Hallert, C.; Grant, C.; Grehn, S.; Grännö, C.; Hultén, S.; Midhagen, G.; Ström, M.; Svensson, H.; Valdimarsson, T. Evidence of poor vitamin status in coeliac patients on a gluten-free diet for 10 years. Aliment. Pharmacol. Ther. 2002, 16, 1333–1339. [Google Scholar] [CrossRef] [PubMed]
- Zipser, R.D.; Patel, S.; Yahya, K.Z.; Baisch, D.W.; Monarch, E. Presentations of adult celiac disease in a nationwide patient support group. Dig. Dis. Sci. 2003, 48, 761–764. [Google Scholar] [CrossRef] [PubMed]
- Ukkola, A.; Mäki, M.; Kurppa, K.; Collin, P.; Huhtala, H.; Kekkonen, L.; Kaukinen, K. Changes in body mass index on a gluten-free diet in coeliac disease: A nationwide study. Eur. J. Int. Med. 2012, 23, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, N.; Agostoni, C. Nutritional aspects of gluten-free products. J. Sci Food. Agric. 2015, in press. [Google Scholar]
- Martin, J.; Geisel, T.; Maresch, C.; Krieger, K.; Stein, J. Inadequate nutrient intake in patients with celiac disease: Results from a German dietary survey. Digestion 2013, 87, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Zuccotti, G.; Fabiano, V.; Dilillo, D.; Picca, M.; Cravidi, C.; Brambilla, P. Intakes of nutrients in Italian children with celiac disease and the role of commercially available gluten-free products. J. Hum. Nutr. Diet. 2013, 26, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Varela-Moreiras, G.; Avila, J.M.; Cuadrado, C.; del Pozo, S.; Ruiz, E.; Moreiras, O. Evaluation of food consumption and dietary patterns in Spain by the Food Consumption Survey: Updated information. Eur. J. Clin. Nutr. 2010, 64, S37–S43. [Google Scholar] [CrossRef] [PubMed]
- Subar, A.F.; Krebs-Smith, S.M.; Cook, A.; Kahle, L.L. Dietary sources of nutrients among US adults, 1989 to 1991. J. Am. Diet. Assoc. 1998, 98, 537–547. [Google Scholar] [CrossRef]
- Gallagher, E.; Gormley, T.R.; Arendt, E.K. Recent advances in the formulation of gluten-free cereal-based products. Trends Food. Sci. Technol. 2004, 15, 143–152. [Google Scholar] [CrossRef]
- Martin, U.; Mercer, S.W. A comparison of general practitioners prescribing of gluten-free foods for the treatment of coeliac disease with national prescribing guidelines. J. Hum. Nutr. Diet. 2014, 27, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Roso Calvo de Mora, B.; Perez-Olleros Conde, L. Preliminary results on dietary fibre intake in Spain and health benefits associated to soluble fiber intake. Res. Esp Nutr. Comunitaria 2010, 16, 147–153. [Google Scholar] [CrossRef]
- Yoshida, T.; Stern, P.H. How vitamin D works on bone. Endocrinol. Metab. Clin. North. Am. 2012, 41, 557–569. [Google Scholar] [CrossRef] [PubMed]
- Cellier, C.; Flobert, C.; Cormier, C.; Roux, C.; Schmitz, J. Severe osteopenia in symptom-free adults with a childhood diagnosis of coeliac disease. Lancet 2000. [Google Scholar] [CrossRef]
- Kalayci, A.G.; Kansu, A.; Girgin, N.; Kucuk, O.; Aras, G. Bone mineral density and importance of a gluten-free diet in patients with celiac disease in childhood. Pediatrics 2001, 108, E89. [Google Scholar] [CrossRef] [PubMed]
- Lucendo, A.J.; García-Manzanares, A. Bone mineral density in adult coeliac disease: An updated review. Rev. Esp. Enferm. Dig. 2013, 105, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, B.; Michaëlsson, K.; Green, P.H.; Ludvigsson, J.F. Persistent mucosal damage and risk of fracture in celiac disease. J. Clin. Endocrinol. Metab. 2014, 99, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Andersson, M. Prevalence of iodine deficiency in Europe in 2010. Ann. Endocrinol. 2011, 72, 164–166. [Google Scholar] [CrossRef] [PubMed]
- Kalyoncu, D.; Urganci, N. Antithyroid antibodies and thyroid function in pediatric patients with celiac disease. Int. J. Endocrinol. 2015. [Google Scholar] [CrossRef] [PubMed]
- Hadithi, M.; Mulder, C.J.; Stam, F.; Azizi, J.; Crusius, J.B.; Peña, A.S.; Stehouwer, C.D.; Smulders, Y.M. Effect of B vitamin supplementation on plasma homocysteine levels in celiac disease. World. J. Gastroenterol. 2009, 15, 955–960. [Google Scholar] [CrossRef] [PubMed]
- Thompson, T. Folate, iron, and dietary fiber contents of the gluten-free diet. J. Am. Diet. Assoc. 2000, 100, 1389–1396. [Google Scholar] [CrossRef]
- Mlynekov, Z.; Chrenkov, Mr.; Formelov, Z. Cereals and Legumes in Nutrition of People with Celiac Disease. Int. J. Celiac Dis. 2014, 2, 105–109. [Google Scholar]
- Martínez-González, M.A.; Salas-Salvadó, J.; Estruch, R.; Corella, D.; Fitó, M.; Ros, E. Benefits of the Mediterranean Diet: Insights from the PREDIMED Study. Prog. Cardiovasc. Dis. 2015, 58, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Sayón-Orea, C.; Santiago, S.; Cuervo, M.; Martínez-González, M.A.; Garcia, A.; Martínez, J.A. Adherence to Mediterranean dietary pattern and menopausal symptoms in relation to overweight/obesity in Spanish perimenopausal and postmenopausal women. Menopause 2014, 22, 750–757. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Churruca, I.; Miranda, J.; Lasa, A.; Bustamante, M.; Larretxi, I.; Simon, E. Analysis of Body Composition and Food Habits of Spanish Celiac Women. Nutrients 2015, 7, 5515-5531. https://doi.org/10.3390/nu7075234
Churruca I, Miranda J, Lasa A, Bustamante M, Larretxi I, Simon E. Analysis of Body Composition and Food Habits of Spanish Celiac Women. Nutrients. 2015; 7(7):5515-5531. https://doi.org/10.3390/nu7075234
Chicago/Turabian StyleChurruca, Itziar, Jonatan Miranda, Arrate Lasa, María Bustamante, Idoia Larretxi, and Edurne Simon. 2015. "Analysis of Body Composition and Food Habits of Spanish Celiac Women" Nutrients 7, no. 7: 5515-5531. https://doi.org/10.3390/nu7075234