Associations between Vitamin D Status, Supplementation, Outdoor Work and Risk of Parkinson’s Disease: A Meta-Analysis Assessment

Abstract
:1. Introduction
2. Methods
2.1. Literature Search and Inclusion Criteria
2.2. Data Extraction and Statistical Analysis
3. Results
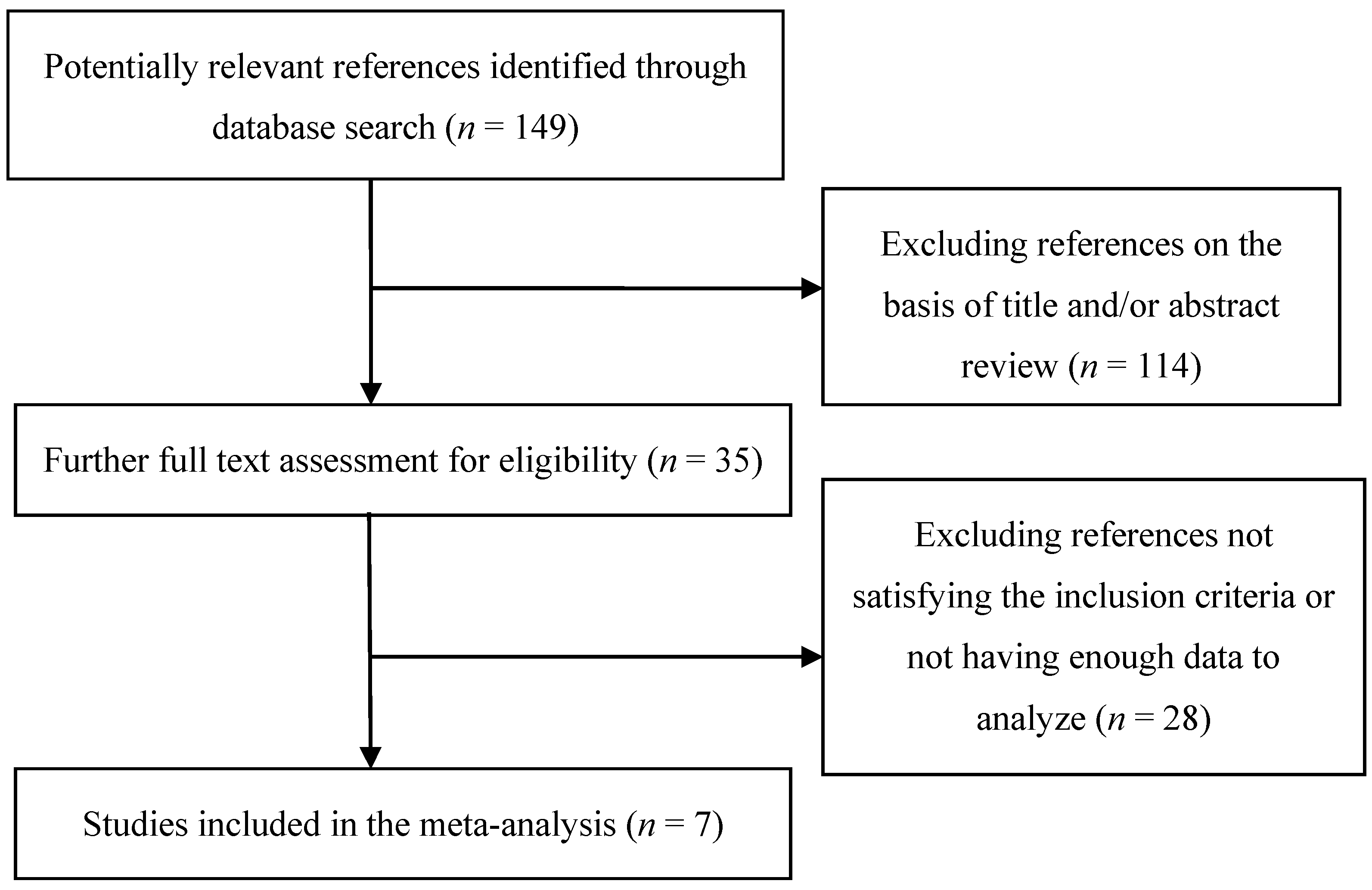
3.1. Results of the Literature Search
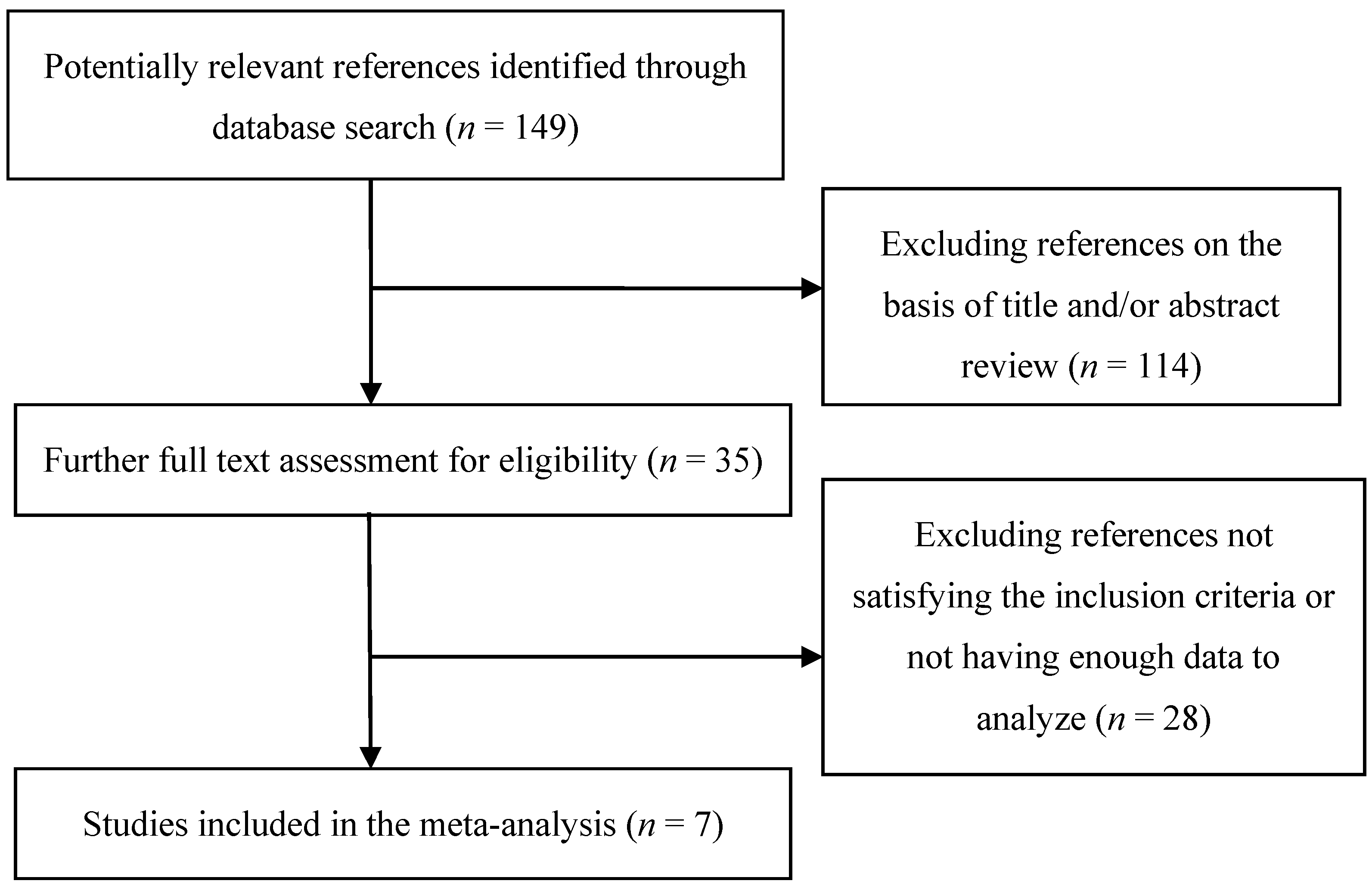
3.2. Results of Meta-analysis
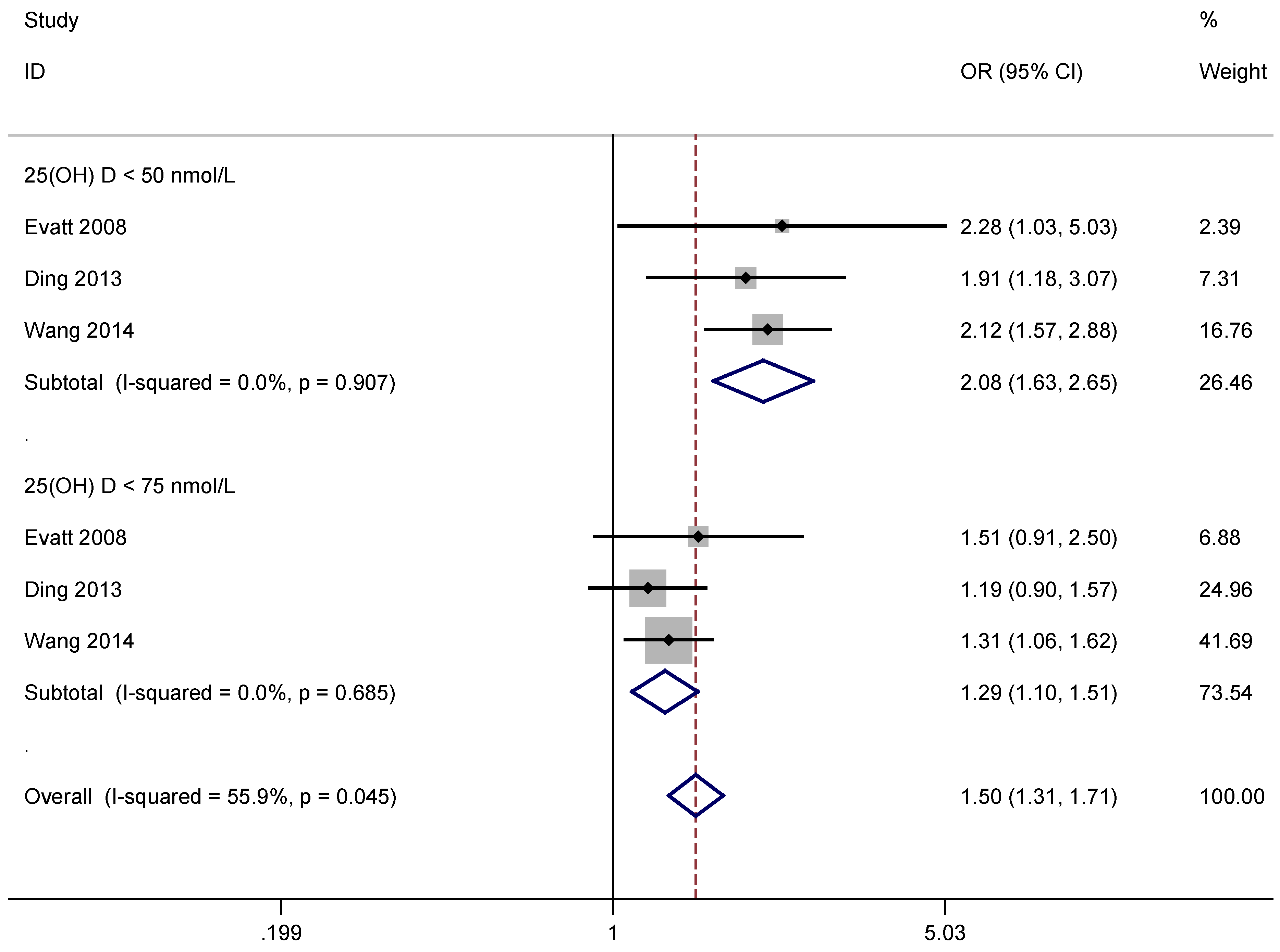
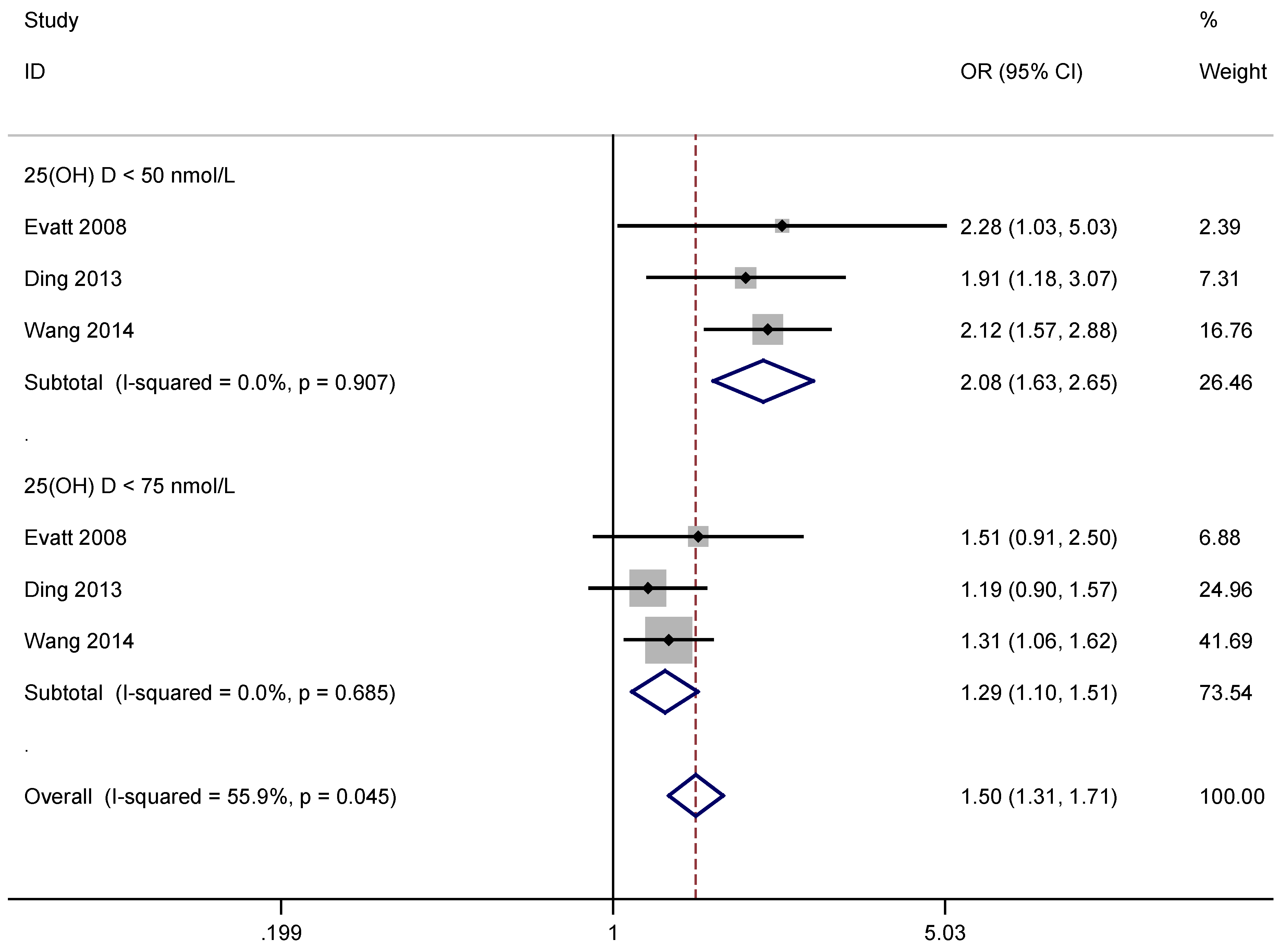
3.2.1. Assessment of Vitamin D Level and Risk of PD
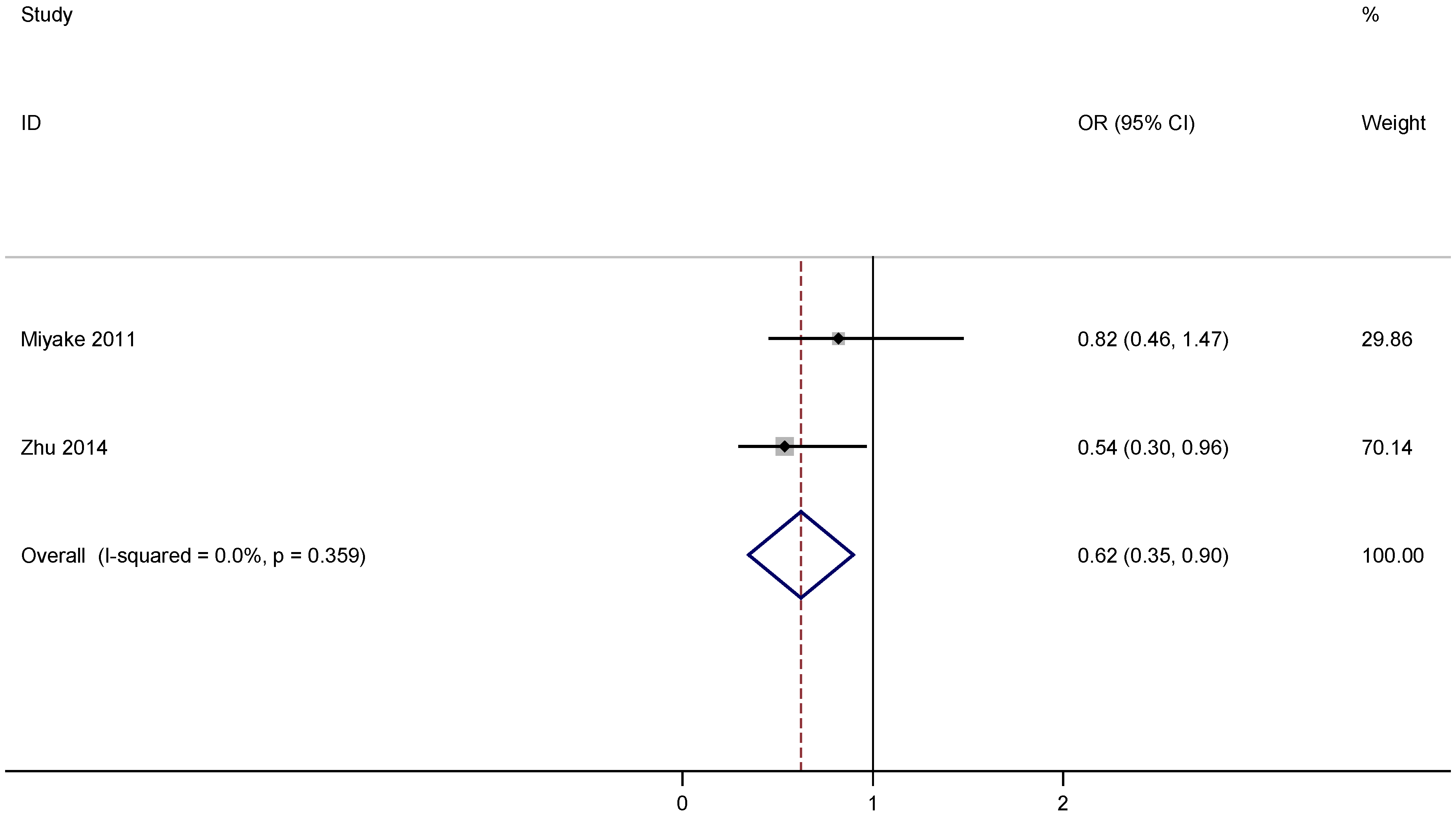
3.2.2. Assessment of Vitamin D Supplementation and Risk of PD
3.2.3. Assessment of Outdoor Work and Risk of PD


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| References | Year | Country | Study Type | Number of Participants | Average Age (years) | OR (95% CI) * | Adjustments | ||
|---|---|---|---|---|---|---|---|---|---|
| PD | Control | PD | Control | ||||||
| Evatt [15] | 2008 | USA | cohort | 100 | 99 | 65.4 | 65.7 | 2.28 (1.03, 5.03) (deficient) 1.51 (0.91, 2.50) (insufficient) | age, sex, race, symptom duration, and sampling season |
| Ding [16] | 2013 | USA | cross-sectional and case-control | 388 | 283 | 65.7 ± 9.6 | 8.0 ± 10.4 | 1.91 (1.18, 3.07) (deficient) 1.19 (0.90, 1.57) (insufficient) | age, sex, race, and vitamin D supplementation |
| Wang [17] | 2015 | USA | case-control | 478 | 431 | 64 ± 12 | 70 ± 8 | 2.12 (1.57, 2.88) (deficient) 1.31 (1.06, 1.62) (insufficient) | age, sex, and sampling season |
| References | Year | Country | Study Type | Participants | Average Age (years) | OR, 95% CI High Versus Low Category | Adjustments | ||
|---|---|---|---|---|---|---|---|---|---|
| PD | Control | PD | Control | ||||||
| Vitamin D supplementation | |||||||||
| Miyake [18] | 2011 | Japan | case-control | 249 | 368 | 68.5 | 66.6 | 0.82 (0.46–1.47) | age, sex, region of residence, pack-years of smoking, years of education, body mass index and dietary factors including cholesterol, dietary glycemic index, vitamin E, β-carotene, vitamin B6, caffeine, iron, and alcohol |
| Zhu [19] | 2014 | China | case-control | 209 | 210 | 64.6 ± 9.4 | 66.0 ± 8.1 | 0.54 (0.30–0.96) | age, sex, smoking, alcohol use, education, and BMI |
| Outdoor work | |||||||||
| Kenborg [20] | 2011 | USA | case-control | 3819 | 19,282 | 71.2 | - | 0.72 (0.63–0.82) | age, chronic obstructive pulmonary disease, comorbidity, place of birth, and social class |
| Kwon [21] | 2013 | USA | case-control | 447 | 578 | 66 | 68 | 0.74 (0.44–1.25) | age, sex, and smoking |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Gröber, U.; Spitz, J.; Reichrath, J.; Kisters, K.; Holick, M.F. Vitamin D: Update 2013: From rickets prophylaxis to general preventive healthcare. Dermatoendocrinology 2013, 5, 331–347. [Google Scholar] [CrossRef] [PubMed]
- Vacek, J.L.; Vanga, S.R.; Good, M.; Lai, S.M.; Lakkireddy, D.; Howard, P.A. Vitamin D deficiency and supplementation and relation to cardiovascular health. Am. J. Cardiol. 2012, 109, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Wacker, M.; Holick, M.F. Sunlight and Vitamin D: A global perspective for health. Dermatoendocrinology 2013, 5, 51–108. [Google Scholar] [CrossRef] [PubMed]
- Bolland, M.J.; Grey, A.; Gamble, G.D.; Reid, I.R. The effect of vitamin D supplementation on skeletal, vascular, or cancer outcomes: A trial sequential meta-analysis. Lancet Diabetes Endocrinol. 2014, 2, 307–320. [Google Scholar] [CrossRef]
- Garcion, E.; Wion-Barbot, N.; Montero-Menei, C.N.; Berger, F.; Wion, D. New clues about vitamin D functions in the nervous system. Trends Endocrinol. Metab. 2002, 13, 100–105. [Google Scholar] [CrossRef]
- Chaudhuri, K.R.; Healy, D.G.; Schapira, A.H. Non-motor symptoms of Parkinson’s disease: Diagnosis and management. Lancet Neurol. 2006, 5, 235–245. [Google Scholar] [CrossRef]
- Braak, H.; Del Tredici, K. Invited Article: Nervous system pathology in sporadic Parkinson disease. Neurology 2008, 70, 1916–1925. [Google Scholar] [CrossRef] [PubMed]
- Dick, F.D.; de, P.G.; Ahmadi, A.; Scott, N.W.; Prescott, G.J.; Bennett, J.; Semple, S.; Dick, S.; Counsell, C.; Mozzoni, P.; et al. Environmental risk factors for Parkinson’s disease and parkinsonism: The Geoparkinson study. Occup. Environ. Med. 2007, 64, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Dardiotis, E.; Xiromerisiou, G.; Hadjichristodoulou, C.; Tsatsakis, A.M.; Wilks, M.F.; Hadjigeorgiou, G.M. The interplay between environmental and genetic factors in Parkinson’s disease susceptibility: The evidence for pesticides. Toxicology 2013, 307, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Kikuyama, M.; Oizumi, K. High prevalence of vitamin D deficiency and reduced bone mass in Parkinson’s disease. Neurology 1997, 49, 1273–1278. [Google Scholar] [CrossRef] [PubMed]
- Van den Bos, F.; Speelman, A.D.; van Nimwegen, M.; van der Schouw, Y.T.; Backx, F.J.; Bloem, B.R.; Munneke, M.; Verhaar, H.J. Bone mineral density and vitamin D status in Parkinson’s disease patients. J. Neurol. 2013, 260, 754–760. [Google Scholar] [PubMed]
- Zhao, Y.; Sun, Y.; Ji, H.F.; Shen, L. Vitamin D levels in Alzheimer’s and Parkinson’s diseases: A meta-analysis. Nutrition 2013, 29, 828–832. [Google Scholar] [CrossRef] [PubMed]
- Lv, Z.; Qi, H.; Wang, L.; Fan, X.; Han, F.; Wang, H.; Bi, S. Vitamin D status and Parkinson’s disease: A systematic review and meta-analysis. Neurol. Sci. 2014, 35, 1723–1730. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Evatt, M.L.; Delong, M.R.; Khazai, N.; Rosen, A.; Triche, S.; Tangpricha, V. Prevalence of vitamin D insufficiency in patients with Parkinson disease and Alzheimer disease. Arch. Neurol. 2008, 65, 1348–1352. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.; Dhima, K.; Lockhart, K.C.; Locascio, J.J.; Hoesing, A.N.; Duong, K.; Trisini-Lipsanopoulos, A.; Hayes, M.T.; Sohur, U.S.; Wills, A.M.; et al. Unrecognized vitamin D3 deficiency is common in Parkinson disease: Harvard Biomarker Study. Neurology 2013, 81, 1531–1537. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Evatt, M.L.; Maldonado, L.G.; Perry, W.R.; Ritchie, J.C.; Beecham, G.W.; Martin, E.R.; Haines, J.L.; Pericak-Vance, M.A.; Vance, J.M.; et al. Vitamin D from different sources is inversely associated with Parkinson disease. Mov. Disord. 2015, 30, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Miyake, Y.; Tanaka, K.; Fukushima, W.; Sasaki, S.; Kiyohara, C.; Tsuboi, Y.; Yamada, T.; Oeda, T.; Miki, T.; Kawamura, N.; et al. Lack of association of dairy food, calcium, and vitamin D intake with the risk of Parkinson’s disease: A case-control study in Japan. Parkinsonism Relat. Disord. 2011, 17, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Zhu, D.; Liu, G.Y.; Lv, Z.; Wen, S.R.; Bi, S.; Wang, W.Z. Inverse associations of outdoor activity and vitamin D intake with the risk of Parkinson’s disease. J. Zhejiang Univ. Sci. B 2014, 15, 923–927. [Google Scholar] [CrossRef] [PubMed]
- Kenborg, L.; Lassen, C.F.; Ritz, B.; Schernhammer, E.S.; Hansen, J.; Gatto, N.M.; Olsen, J.H. Outdoor work and risk for Parkinson’s disease: A population-based case-control study. Occup. Environ. Med. 2011, 68, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Kwon, E.; Gallagher, L.G.; Searles Nielsen, S.; Franklin, G.M.; Littell, C.T.; Longstreth, W.T., Jr.; Swanson, P.D.; Checkoway, H. Parkinson’s disease and history of outdoor occupation. Parkinsonism Relat. Disord. 2013, 19, 1164–1166. [Google Scholar] [CrossRef] [PubMed]
- Knekt, P.; Kilkkinen, A.; Rissanen, H.; Marniemi, J.; Säksjärvi, K.; Heliövaara, M. Serum vitamin D and the risk of Parkinson disease. Arch. Neurol. 2010, 67, 808–811. [Google Scholar] [CrossRef] [PubMed]
- Butler, M.W.; Burt, A.; Edwards, T.L.; Zuchner, S.; Scott, W.K.; Martin, E.R.; Vance, J.M.; Wang, L. Vitamin D receptor gene as a candidate gene for Parkinson disease. Ann. Hum. Genet. 2011, 75, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.H.; Chen, K.H.; Chen, M.L.; Lin, H.I.; Wu, R.M. Vitamin D receptor genetic variants and Parkinson’s disease in a Taiwanese population. Neurobiol. Aging 2014, 35, 1212.e11–1212.e13. [Google Scholar] [CrossRef] [PubMed]
- Török, R.; Török, N.; Szalardy, L.; Plangar, I.; Szolnoki, Z.; Somogyvari, F.; Vecsei, L.; Klivenyi, P. Association of vitamin D receptor gene polymorphisms and Parkinson’s disease in Hungarians. Neurosci. Lett. 2013, 551, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Henchcliffe, C.; Beal, M.F. Mitochondrial biology and oxidative stress in Parkinson disease pathogenesis. Nat. Clin. Pract. Neurol. 2008, 4, 600–609. [Google Scholar] [CrossRef] [PubMed]
- Von Essen, M.R.; Kongsbak, M.; Schjerling, P.; Olgaard, K.; Odum, N.; Geisler, C. Vitamin D controls T cell antigen receptor signaling and activation of human T cells. Nat. Immunol. 2010, 11, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Høyer-Hansen, M.; Nordbrandt, S.P.; Jäättelä, M. Autophagy as a basis for the health-promoting effects of vitamin D. Trends Mol. Med. 2010, 16, 295–302. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, L.; Ji, H.-F. Associations between Vitamin D Status, Supplementation, Outdoor Work and Risk of Parkinson’s Disease: A Meta-Analysis Assessment. Nutrients 2015, 7, 4817-4827. https://doi.org/10.3390/nu7064817
Shen L, Ji H-F. Associations between Vitamin D Status, Supplementation, Outdoor Work and Risk of Parkinson’s Disease: A Meta-Analysis Assessment. Nutrients. 2015; 7(6):4817-4827. https://doi.org/10.3390/nu7064817
Chicago/Turabian StyleShen, Liang, and Hong-Fang Ji. 2015. "Associations between Vitamin D Status, Supplementation, Outdoor Work and Risk of Parkinson’s Disease: A Meta-Analysis Assessment" Nutrients 7, no. 6: 4817-4827. https://doi.org/10.3390/nu7064817
APA StyleShen, L., & Ji, H.-F. (2015). Associations between Vitamin D Status, Supplementation, Outdoor Work and Risk of Parkinson’s Disease: A Meta-Analysis Assessment. Nutrients, 7(6), 4817-4827. https://doi.org/10.3390/nu7064817