Anorexia Nervosa and Body Fat Distribution: A Systematic Review




Abstract
:1. Introduction
2. Experimental Section
2.1. Inclusion and Exclusion Criteria
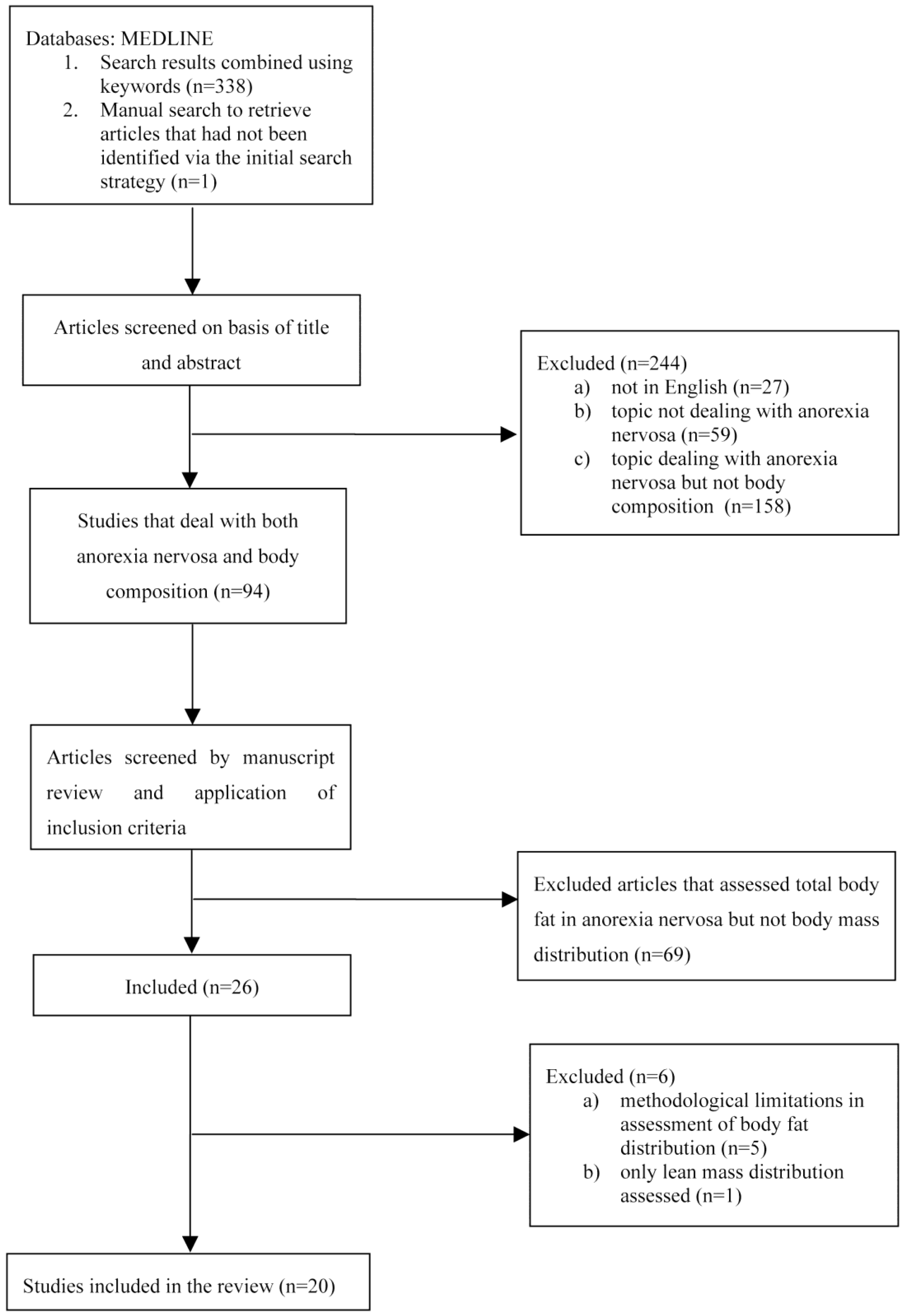
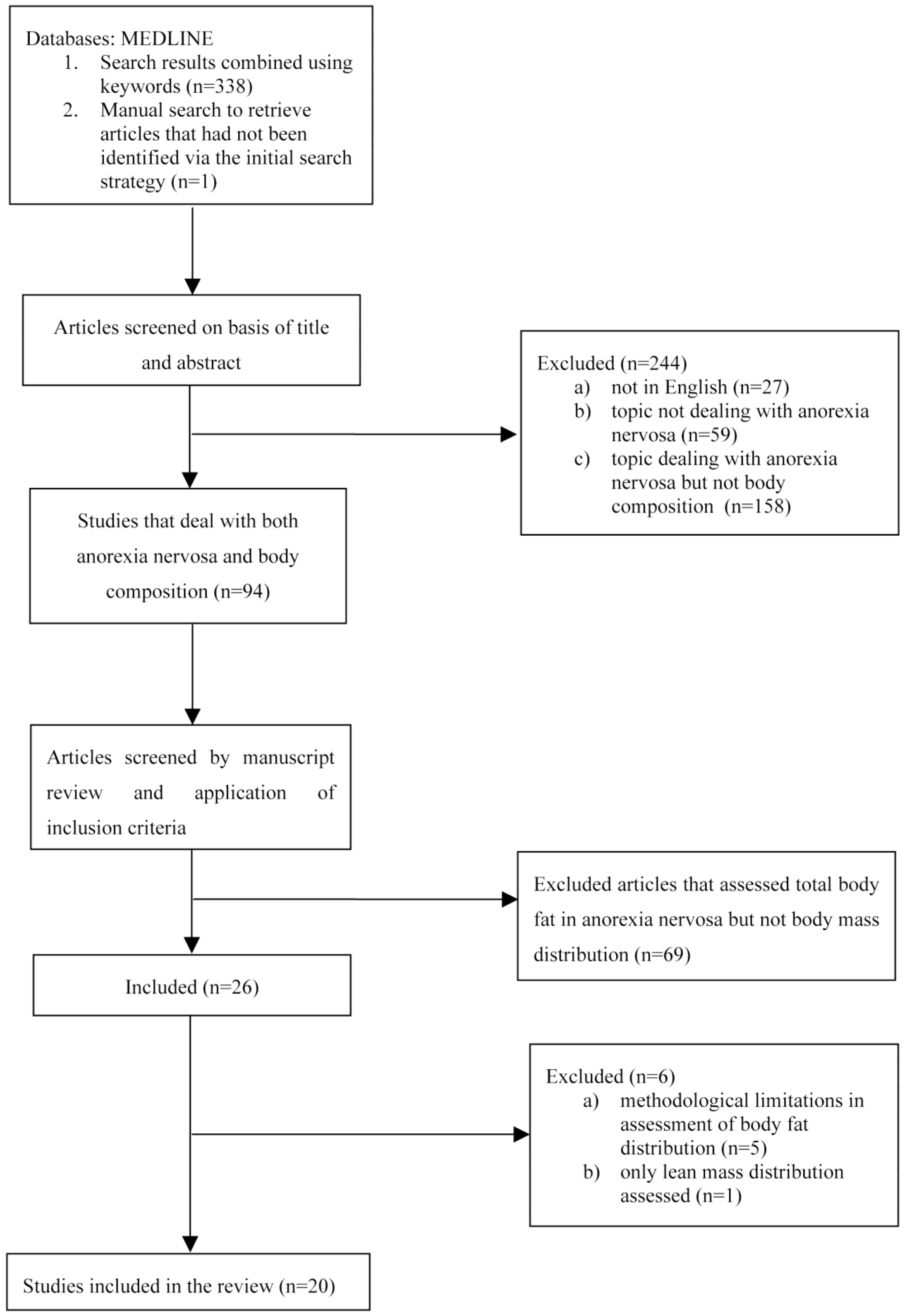
2.2. Information Source and Search Strategy
2.3. Study Selection
2.4. Data Collection Process and Data Items
2.5. Data Synthesis

{kind=link}
| First Author | Year | Method | Study | Sample | Intervention | BF Distribution before Weight Gain | BF Distribution after Partial/Complete Weight Restoration |
|---|---|---|---|---|---|---|---|
| Adolescents | |||||||
| Kerruish et al. [22] | 2002 | DXA | Cross-sectional | 23 adolescent AN females vs. 25 age-matched controls | - | Lower trunk fat, leg fat and trunk/leg fat ratio than in control subjects (less central fat) | - |
| Misra et al. [23] | 2003 | DXA | Longitudinal, over 1 year | 21 adolescent AN females (only 13 had a BMI increase) vs. 21 age-matched controls | Complete weight restoration (BMI >10th percentile) | Lower percentage trunk fat than controls, whereas percentage extremity fat was not significantly different between the groups | Trunk fat and trunk/extremity fat ratio did not exceed that of controls, indicating that the changes in adolescent females with AN most likely represented a normalization of BF distribution. |
| Misra et al. [24] | 2005 | DXA | Longitudinal, over 1 year | 23 adolescent AN females (only 11 obtained a BMI increase) vs. 20 age-matched controls | Complete weight restoration | Percentage trunk fat was significantly lower than in controls, whereas percentage extremity fat did not differ, suggesting preferential loss of trunk fat with weight loss | - |
| De Alvaro et al. [25] | 2007 | DXA | Longitudinal, over 24 months | 42 adolescent AN-R females (only 15 achieved weight and menses recovery) vs. 23 controls | Slow complete weight restoration | Lower trunk/extremity fat ratio in prolonged malnutrition patients due to a greater loss of trunk fat. | Slow and complete weight restoration was associated with an adequately distributed fat mass acquisition, with no changes in regional fat percentages |
| Misra et al. [26] | 2008 | DXA | Cross-sectional | 15 adolescent AN boys vs. 15 controls | - | Adolescent boys with AN had higher percentage trunk fat and trunk/extremity ratio than controls associated with lower testosterone concentrations | - |
| Franzoni et al. [27] | 2014 | DXA | Longitudinal, 1 year of treatment | 46 adolescent AN-R females; no controls | Short-term partial weight restoration | Not mentioned | More evident deposition of fat in trunk region, in the absence of healthy control group |
| Forbes [28] | 1990 | AM | Cross-sectional | 2 males and 30 females with AN (adolescents) aged 10–22 years vs. normative data | - | Regional adiposity was measured using waist and hip circumferences—these measures decreased, with no change in waist-to-hip ratio | - |
| Adults | |||||||
| Kirchengast et al. [29] | 1999 | DXA | Cross-sectional | 15 adult AN females vs. 15 age-matched controls | - | Underweight infertile AN patients showed hypergynoid distribution despite low oestrogen levels | - |
| Iketani et al. [30] | 1999 | DXA | Longitudinal, inpatient and outpatient treatments | 21 adult AN females vs. 10 age-matched controls | Short-term partial weight restoration | BF reduction in all regions (trunk, pelvis, upper and lower extremities) but no mention of its relative distribution. | Trunk and pelvis BF increased remarkably and reached the levels of controls, but the upper and lower extremity BF remained below the control level. |
| Pagliato et al. [31] | 2000 | DXA | Longitudinal, inpatient treatment | 17 adult AN patients; no controls | Short-term partial weight restoration | Not mentioned | In the inpatient group, the increase of BF in trunk region was higher with respect to other patterns |
| Grinspoon et al. [32] | 2001 | DXA | Longitudinal, outpatient treatment | 27 adult AN females vs. 20 age-matched controls | Spontaneous partial weight restoration | Percentage trunk fat not statistically different between patients and controls, percentage extremity fat significantly lower than in controls, but trunk/extremity fat ratio no different to that in healthy controls | Increase in trunk adiposity. Estrogen administration did not appear to prevent such distribution |
| Kirchengast et al. [33] | 2003 | DXA | Cross-sectional | 15 adult AN females vs. 19 age-matched controls | - | AN patients showed a gynoid fat pattern no different from healthy controls | - |
| Dellava et al. [34] | 2010 | DXA | Cross-sectional | 16 adult AN females vs. 18 age- and BMI-matched controls | Long-term weight maintenance | - | Women recovered from AN for two years or more had similar body fat distribution to controls |
| Prioletta et al. [35] | 2011 | DXA | Longitudinal, 12-week multidisciplinary re-education program | 19 AN females aged 17–32 years vs. 20 age-matched controls | Short-term partial weight restoration | No difference in percentage trunk fat with respect to controls | Minimum and short-term partial weight restoration led to a preferential redistribution of BF in trunk region with respect to controls, and such distribution was correlated with insulin-resistance status |
| El Ghoch et al. [36] | 2014 | DXA | Longitudinal, (20-week inpatient treatment) | 50 adult AN females vs. 100 healthy, lean age- and BMI-matched controls | Short-term complete weight restoration | Arm, leg, trunk, android and gynoid fat mass percentages were lower than in controls, but no significant difference was found between the two groups in term of the android/gynoid ratio. | Preferential distribution of body fat in central regions (trunk, android), but such distribution did not appear to influence eating disorder psychopathology or psychological distress factors. |
| Mayo-Smith et al. [37] | 1989 | CT | Cross-sectional | 15 AN females aged 15–33 years vs. 39 controls aged 18–35 years | - | Subcutaneous and visceral adipose tissue evaluated by CT. AN patients tend to lose more subcutaneous fat than intra-abdominal fat compared to controls | - |
| Zamboni et al. [38] | 1997 | CT | Longitudinal, 12-week inpatient treatment | 21 adult AN females; no controls | Short-term partial weight restoration | Patients lost more subcutaneous adipose tissue than visceral adipose tissue | The increase in fat in subcutaneous abdominal tissue was significantly greater than visceral abdominal tissue. |
| Mayer et al. [39] | 2009 | MRI | Long-term longitudinal, 1-year follow-up after inpatient treatment | 21 adult AN females vs. 10 age- and BMI-matched controls | Long-term weight maintenance | With acute weight restoration, AN patients had significantly greater visceral and intramuscular adipose tissue than control women | The abnormal fat distribution appeared to normalize within a 1-year period of weight maintenance |
| Orphanidou et al. [40] | 1997 | Skin-fold Thickness and DXA | Longitudinal, 20-week inpatient or 48-week outpatient | 26 adult AN females vs. 21 controls | Short-term partial weight restoration | Not mentioned | BF distribution showed greater deposition in the central regions than in the extremities |
| Mayer et al. [14] | 2005 | AM DXA MRI | Longitudinal, inpatient treatment (4–17 weeks) | 29 adult AN females vs. 15 age- and BMI-matched controls | Short-term complete weight restoration | At baseline, trunk/total fat was not statistically different from controls | Using different methods to assess body fat distribution suggested disproportionate central adipose tissue deposition |
3. Results
3.1. Body Fat Distribution in Adolescents with Anorexia Nervosa
3.2. Body Fat Distribution in Adults with Anorexia Nervosa
3.3. Body Fat Distribution after Partial and Complete Weight Restoration in Adolescents with Anorexia Nervosa
3.4. Body Fat Distribution after Short-term Partial and Complete Weight Restoration in Adults with Anorexia Nervosa
3.5. Body Fat Distribution after Long-term Maintenance of Complete Weight Restoration in Anorexia Nervosa
3.6. Change in Body Fat Distribution, Metabolic Indices and Psychopathology
4. Discussion
4.1. Summary of Evidence and Limitation
4.1.1. Strong Evidence
4.1.2. Evidence Still Requiring Confirmation
4.1.3. Weak Evidence
4.1.4. Paucity or Lack of Evidence
4.2. Implications for Future Research
5. Conclusions
Supplementary Files
Supplementary File 1Author Contributions
Conflicts of Interest
References
- Agras, W.S. The consequences and costs of the eating disorders. Psychiatr. Clin. N. Am. 2001, 24, 371–379. [Google Scholar] [CrossRef]
- Dalle Grave, R. Eating disorders: Progress and challenges. Eur. J. Intern. Med. 2011, 22, 153–160. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Clinical Excellence. Eating disorders. Core Interventions in the Treatment and Management of Anorexia Nervosa, Bulimia Nervosa and Related Eating Disorders; Clinical Guideline 9: National Collaborating Centre for Mental Health; British Psychological Society and RCPsych Publications: London, UK, 2004. [Google Scholar]
- El Ghoch, M.; Alberti, M.; Milanese, C.; Battistini, N.C.; Pellegrini, M.; Capelli, C.; Calugi, S.; Dalle Grave, R. Comparison between dual-energy X-ray absorptiometry and skinfolds thickness in assessing body fat in anorexia nervosa before and after weight restoration. Clin. Nutr. 2012, 31, 911–916. [Google Scholar] [CrossRef] [PubMed]
- Krahn, D.D.; Rock, C.; Dechert, R.E.; Nairn, K.K.; Hasse, S.A. Changes in resting energy expenditure and body composition in anorexia nervosa patients during refeeding. J. Am. Diet. Assoc. 1993, 93, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Probst, M.; Goris, M.; Vandereycken, W.; Van Coppenolle, H. Body composition in female anorexia nervosa patients. Br. J. Nutr. 1996, 76, 639–647. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; (DSM-5™); American Psychiatric Publishing: Arlington, MA, USA, 2013. [Google Scholar]
- Marzola, E.; Nasser, J.A.; Hashim, S.A.; Shih, P.A.; Kaye, W.H. Nutritional rehabilitation in anorexia nervosa: Review of the literature and implications for treatment. BMC Psychiatry 2013, 13, 290. [Google Scholar] [CrossRef] [PubMed]
- Frisch, R.E. Fatness and fertility. Sci. Am. 1988, 258, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Dalle Grave, R.; Pasqualoni, E.; Marchesini, G. Symptoms of starvation in eating disorder patients. In Handbook of Behavior, Food and Nutrition; Springer Science Business Media: New York, NY, USA, 2011; pp. 2259–2269. [Google Scholar]
- Mayer, L.E.; Roberto, C.A.; Glasofer, D.R.; Etu, S.F.; Gallagher, D.; Wang, J.; Heymsfield, S.B.; Pierson, R.N., Jr.; Attia, E.; Devlin, M.J.; et al. Does percent body fat predict outcome in anorexia nervosa? Am. J. Psychiatry 2007, 164, 970–972. [Google Scholar]
- Bodell, L.P.; Mayer, L.E. Percent body fat is a risk factor for relapse in anorexia nervosa: A replication study. Int. J. Eat. Disord. 2011, 44, 118–123. [Google Scholar] [PubMed]
- Fairburn, C.G. Cognitive Behavior Therapy and Eating Disorders; Guilford Press: New York, NY, USA, 2008. [Google Scholar]
- Mayer, L.; Walsh, B.T.; Pierson, R.N., Jr.; Heymsfield, S.B.; Gallagher, D.; Wang, J.; Parides, M.K.; Leibel, R.L.; Warren, M.P.; Killory, E.; et al. Body fat redistribution after weight gain in women with anorexia nervosa. Am. J. Clin. Nutr. 2005, 81, 1286–1291. [Google Scholar]
- Folsom, A.R.; Kushi, L.H.; Anderson, K.E.; Mink, P.J.; Olson, J.E.; Hong, C.P.; Sellers, T.A.; Lazovich, D.; Prineas, R.J. Associations of general and abdominal obesity with multiple health outcomes in older women: The Iowa Women’s Health Study. Arch. Intern. Med. 2000, 160, 2117–2128. [Google Scholar] [CrossRef] [PubMed]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACP J. Club. 1995, 123, A12–A13. [Google Scholar] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [PubMed]
- (NICE) National Institute for Health and Clinical Excellence. Clinical Guidelines, Appendix 4. Quality of Case Series Form. Available online: http://www.nice.org.uk/nicemedia/pdf/Appendix_04_qualityofcase_series_form_preop.pdf (accessed on 30 March 2010).
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ji, J.; Liu, Y.J.; Deng, X.; He, Q.Q. Passive smoking and risk of type 2 diabetes: A meta-analysis of prospective cohort studies. PLoS One 2013, 8, e69915. [Google Scholar] [CrossRef] [PubMed]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Britten, N.; Arai, L.; Roen, K.; Rodgers, M. Developing guidance on the conduct of narrative synthesis in systematic reviews. J. Epidemiol. Community Health 2005, 59 (Suppl. 1), A7. [Google Scholar]
- Kerruish, K.P.; O’Connor, J.; Humphries, I.R.; Kohn, M.R.; Clarke, S.D.; Briody, J.N.; Thomson, E.J.; Wright, K.A.; Gaskin, K.J.; Baur, L.A. Body composition in adolescents with anorexia nervosa. Am. J. Clin. Nutr. 2002, 75, 31–37. [Google Scholar] [PubMed]
- Misra, M.; Soyka, L.A.; Miller, K.K.; Grinspoon, S.; Levitsky, L.L.; Klibanski, A. Regional body composition in adolescents with anorexia nervosa and changes with weight recovery. Am. J. Clin. Nutr. 2003, 77, 1361–1367. [Google Scholar] [PubMed]
- Misra, M.; Miller, K.K.; Almazan, C.; Worley, M.; Herzog, D.B.; Klibanski, A. Hormonal determinants of regional body composition in adolescent girls with anorexia nervosa and controls. J. Clin. Endocrinol. Metab. 2005, 90, 2580–2587. [Google Scholar] [CrossRef] [PubMed]
- De Alvaro, M.T.; Munoz-Calvo, M.T.; Barrios, V.; Martinez, G.; Martos-Moreno, G.A.; Hawkins, F.; Argente, J. Regional fat distribution in adolescents with anorexia nervosa: Effect of duration of malnutrition and weight recovery. Eur. J. Endocrinol. 2007, 157, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Misra, M.; Katzman, D.K.; Cord, J.; Manning, S.J.; Mickley, D.; Herzog, D.B.; Miller, K.K.; Klibanski, A. Percentage extremity fat, but not percentage trunk fat, is lower in adolescent boys with anorexia nervosa than in healthy adolescents. Am. J. Clin. Nutr. 2008, 88, 1478–1484. [Google Scholar] [CrossRef] [PubMed]
- Franzoni, E.; Ciccarese, F.; Di Pietro, E.; Facchini, G.; Moscano, F.; Iero, L.; Monaldi, A.; Battista, G.; Bazzocchi, A. Follow-up of bone mineral density and body composition in adolescents with restrictive anorexia nervosa: Role of dual-energy X-ray absorptiometry. Eur. J. Clin. Nutr. 2014, 68, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Forbes, G.B. The abdomen: Hip ratio normative data and observations on selected patients. Int. J. Obes. 1990, 14, 149–157. [Google Scholar] [PubMed]
- Kirchengast, S.; Huber, J. Body composition characteristics, sex hormone levels and circadian gonadotropin fluctuations in infertile young women. Coll. Antropol. 1999, 23, 407–423. [Google Scholar] [PubMed]
- Iketani, T.; Kiriike, N.; Nagata, T.; Yamagami, S. Altered body fat distribution after recovery of weight in patients with anorexia nervosa. Int. J. Eat. Disord. 1999, 26, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Pagliato, E.; Corradi, E.; Gentile, M.G.; Testolin, G. Changes in body composition and resting energy expenditure in anorectic patients after a weight gain of fifteen percent. Ann. N. Y. Acad. Sci. 2000, 904, 617–620. [Google Scholar] [CrossRef] [PubMed]
- Grinspoon, S.; Thomas, L.; Miller, K.; Pitts, S.; Herzog, D.; Klibanski, A. Changes in regional fat redistribution and the effects of estrogen during spontaneous weight gain in women with anorexia nervosa. Am. J. Clin. Nutr. 2001, 73, 865–869. [Google Scholar] [PubMed]
- Kirchengast, S.; Huber, J. Body composition characteristics and fat distribution patterns in young infertile women. Fertil. Steril. 2004, 81, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Dellava, J.E.; Hamer, R.M.; Kanodia, A.; Reyes-Rodriguez, M.L.; Bulik, C.M. Diet and physical activity in women recovered from anorexia nervosa: A pilot study. Int. J. Eat. Disord. 2011, 44, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Prioletta, A.; Muscogiuri, G.; Sorice, G.P.; Lassandro, A.P.; Mezza, T.; Policola, C.; Salomone, E.; Cipolla, C.; Della Casa, S.; Pontecorvi, A.; et al. In anorexia nervosa, even a small increase in abdominal fat is responsible for the appearance of insulin resistance. Clin. Endocrinol. (Oxf.) 2011, 75, 202–206. [Google Scholar] [CrossRef]
- El Ghoch, M.; Milanese, C.; Calugi, S.; Pellegrini, M.; Battistini, N.C.; Dalle Grave, R. Body composition, eating disorder psychopathology, and psychological distress in anorexia nervosa: A longitudinal study. Am. J. Clin. Nutr. 2014, 99, 771–778. [Google Scholar]
- Mayo-Smith, W.; Hayes, C.W.; Biller, B.M.; Klibanski, A.; Rosenthal, H.; Rosenthal, D.I. Body fat distribution measured with CT: Correlations in healthy subjects, patients with anorexia nervosa, and patients with Cushing syndrome. Radiology 1989, 170, 515–518. [Google Scholar] [CrossRef] [PubMed]
- Zamboni, M.; Armellini, F.; Turcato, E.; Todisco, P.; Gallagher, D.; Dalle Grave, R.; Heymsfield, S.; Bosello, O. Body fat distribution before and after weight gain in anorexia nervosa. Int. J. Obes. Relat. Metab. Disord. 1997, 21, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Mayer, L.E.; Klein, D.A.; Black, E.; Attia, E.; Shen, W.; Mao, X.; Shungu, D.C.; Punyanita, M.; Gallagher, D.; Wang, J.; et al. Adipose tissue distribution after weight restoration and weight maintenance in women with anorexia nervosa. Am. J. Clin. Nutr. 2009, 90, 1132–1137. [Google Scholar] [CrossRef] [PubMed]
- Orphanidou, C.I.; McCargar, L.J.; Birmingham, C.L.; Belzberg, A.S. Changes in body composition and fat distribution after short-term weight gain in patients with anorexia nervosa. Am. J. Clin. Nutr. 1997, 65, 1034–1041. [Google Scholar] [PubMed]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Bautista, L.; Franzosi, M.G.; Commerford, P.; Lang, C.C.; Rumboldt, Z.; Onen, C.L.; Lisheng, L.; Tanomsup, S; et al. Obesity and the risk of myocardial infarction in 27,000 participants from 52 countries: A case-control study. Lancet 2005, 366, 1640–1649. [Google Scholar]
- Carr, M.C.; Brunzell, J.D. Abdominal obesity and dyslipidemia in the metabolic syndrome: Importance of type 2 diabetes and familial combined hyperlipidemia in coronary artery disease risk. J. Clin. Endocrinol. Metab. 2004, 89, 2601–2607. [Google Scholar] [CrossRef] [PubMed]
- Diamanti-Kandarakis, E.; Bergiele, A. The influence of obesity on hyperandrogenism and infertility in the female. Obes. Rev. 2001, 2, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Manolopoulos, K.N.; Karpe, F.; Frayn, K.N. Gluteofemoral body fat as a determinant of metabolic health. Int. J. Obes. (Lond.) 2010, 34, 949–959. [Google Scholar] [CrossRef]
- Okura, T.; Nakata, Y.; Yamabuki, K.; Tanaka, K. Regional body composition changes exhibit opposing effects on coronary heart disease risk factors. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Chaston, T.B.; Dixon, J.B. Factors associated with percent change in visceral versus subcutaneous abdominal fat during weight loss: Findings from a systematic review. Int. J. Obes. (Lond.) 2008, 32, 619–628. [Google Scholar] [CrossRef]
- Zamboni, M.; Armellini, F.; Harris, T.; Turcato, E.; Micciolo, R.; Bergamo-Andreis, I.A.; Bosello, O. Effects of age on body fat distribution and cardiovascular risk factors in women. Am. J. Clin. Nutr. 1997, 66, 111–115. [Google Scholar] [PubMed]
- Fosbøl, M.Ø.; Zerahn, B. Contemporary methods of body composition measurement. Clin. Physiol. Funct. Imaging 2014. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
El Ghoch, M.; Calugi, S.; Lamburghini, S.; Dalle Grave, R. Anorexia Nervosa and Body Fat Distribution: A Systematic Review. Nutrients 2014, 6, 3895-3912. https://doi.org/10.3390/nu6093895
El Ghoch M, Calugi S, Lamburghini S, Dalle Grave R. Anorexia Nervosa and Body Fat Distribution: A Systematic Review. Nutrients. 2014; 6(9):3895-3912. https://doi.org/10.3390/nu6093895
Chicago/Turabian StyleEl Ghoch, Marwan, Simona Calugi, Silvia Lamburghini, and Riccardo Dalle Grave. 2014. "Anorexia Nervosa and Body Fat Distribution: A Systematic Review" Nutrients 6, no. 9: 3895-3912. https://doi.org/10.3390/nu6093895
APA StyleEl Ghoch, M., Calugi, S., Lamburghini, S., & Dalle Grave, R. (2014). Anorexia Nervosa and Body Fat Distribution: A Systematic Review. Nutrients, 6(9), 3895-3912. https://doi.org/10.3390/nu6093895