Meat Consumption as a Risk Factor for Type 2 Diabetes

Abstract
:1. Introduction
- (1)
- Physical inactivity
- (2)
- First-degree relative with diabetes
- (3)
- High-risk race/ethnicity (e.g., African American, Latino, Native American, Asian American, Pacific Islander)
- (4)
- Women who delivered a baby weighing >9 lb or were diagnosed with gestational diabetes
- (5)
- Hypertension (blood pressure ≥ 140/90 mmHg or on therapy for hypertension)
- (6)
- High density lipoprotein cholesterol level < 35 mg/dL (0.90 mmol/L) and/or a triglyceride level > 250 mg/dL (2.82 mmol/L)
- (7)
- Women with polycystic ovarian syndrome
- (8)
- A1C ≥ 5.7%, impaired glucose tolerance, or impaired fasting glucose on previous testing
- (9)
- Other clinical conditions associated with insulin resistance (e.g., severe obesity, acanthosis nigricans)
- (10)
- History of cardiovascular disease
2. Findings
2.1. Risk Associated with Meat Consumption as a Categorical Variable

{kind=link}
| Meat as a Categorical Variable | ||||
|---|---|---|---|---|
| Study | Observation Period | Population | Findings | Adjustments |
| Adventist Mortality Study Snowdon et al. (1985) [7] | 1960 | 24,673 white Seventh-day Adventists | Prevalence ratio and 95% CI for diabetes diagnosis: Men = 1.8 (1.3, 2.5); Women = 1.4 (1.2, 1.8) | Age and body weight |
| Adventist Mortality Study Snowdon et al. (1985) [7] | 21-year follow-up | 24,673 white Seventh-day Adventists | Relative risk for diabetes on death certificate: Men = 2.2 (1.5, 3.4); Women = 1.4 (1.0, 1.9) | Age |
| Adventist Health Study-1 Fraser (1999) [8] | 1976 | 34,192 Seventh-day Adventists in California | Odds ratio and 95% CI for diabetes diagnosis: Men = 1.97 (1.56, 2.47, p = 0.0001); Women = 1.93 (1.65, 2.25, p = 0.0001) | Age |
| Adventist Mortality Study and Adventist Health Study-1 Tonstad et al. (2013) [11] | 17-year follow-up | 8401 Seventh-day Adventists | Odds ratio with 95% CI for diabetes diagnosis: 1.29 (1.08, 1.55) | Age and gender |
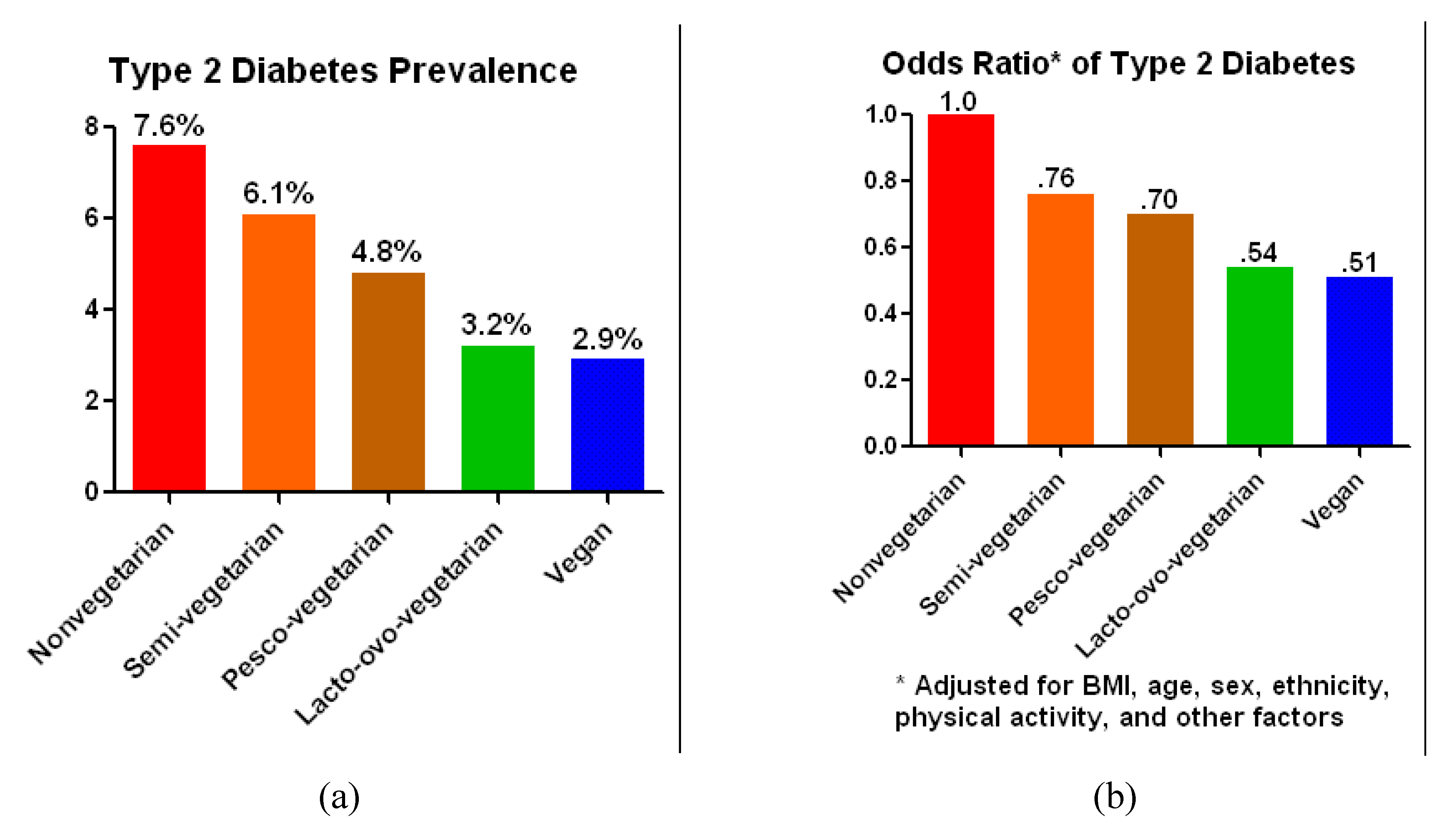
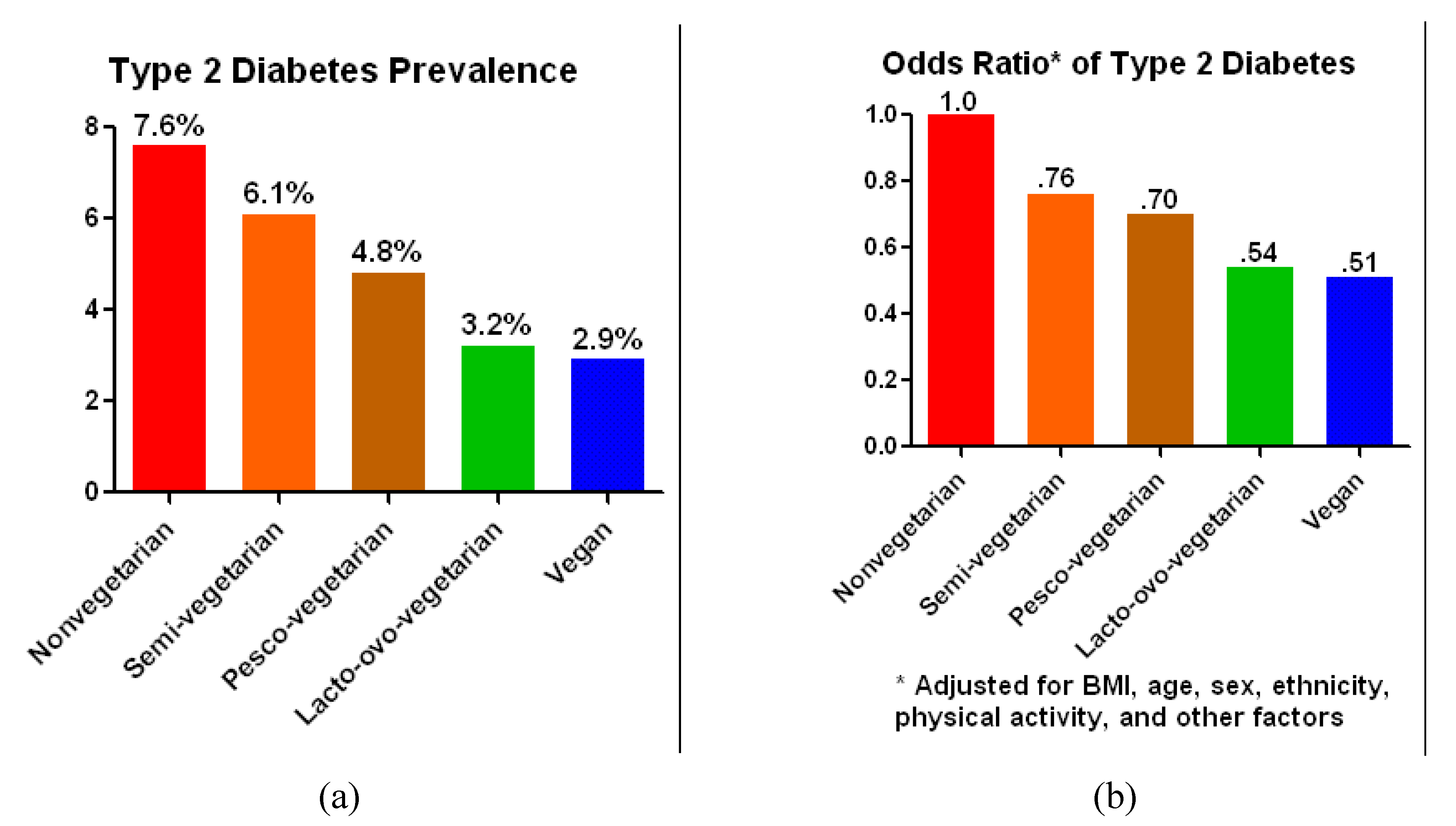
| Adventist Health Study-2 Tonstad et al. (2009) [10] | 2002–2006 | 60,903 Seventh-day Adventists in North America | Odds ratio and 95% CI for diabetes diagnosis: 0.54 (0.49, 0.60) | Age, sex, ethnicity, education, income, physical activity, television watching, sleep habits, alcohol use, and body mass index |
| Adventist Health Study-2 Tonstad et al. (2013) [11] | 2-year follow-up | 41,387 Seventh-day Adventists | Odds ratio with 95% CI for diabetes diagnosis: 0.618 (0.0503, 0.760) | Age, body mass index, gender, ethnicity, income, and education |
| Meta-analysis Pan et al. (2011) [12] | 4.6 to 28 years follow-up | 442,101 | Relative ratios and 95% CI for diabetes diagnosis + D1: 100 g unprocessed red meat/day = 1.19 (1.04, 1.37); 50 g processed red meat/day = 1.51 (1.25, 1.83) | Multivariate analyses adjusted for age, ethnicity, smoking, energy intake, alcohol intake, history of HTN and hypercholesterolemia, family history of diabetes, body weight, and physical activity. A diet score was created looking at trans fats, glycemic load, cereal fiber, and the ratio of polyunsaturated to saturated fat. |
2.1.1. Risk Associated with Gradations of Meat Consumption
2.1.2. Mechanisms of Action
2.1.2.1. Effect on Body Weight
2.1.2.2. Effect on Visceral Fat
2.1.2.3. Effect on Intracellular Lipid
2.1.2.4. Effect on Iron Balance
2.1.2.5. Nitrates in Processed Meats
2.1.2.6. Inflammation
2.1.3. The Use of Risk Factors in Clinical Practice and Health Policies
3. Conclusions
Conflicts of Interest
References
- American Diabetes Association. Standards of medical care in diabetes—2012. Diabetes Care 2012, 36, S11–S66. [Google Scholar] [CrossRef]
- Harris, M.I.; Hadden, W.C.; Knowler, W.C.; Bennett, P.H. Prevalence of diabetes and impaired glucose tolerance and plasma glucose levels in U.S. population aged 20–74 years. Diabetes 1987, 36, 523–524. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Diabetes Fact Sheet: National Estimates and General Information on Diabetes and Prediabetes in the United States, 2011. Available online: http://www.cdc.gov/diabetes/pubs/factsheet11.htm (accessed on 20 August 2013).
- Field, A.E.; Coakley, E.H.; Must, A.; Spadano, J.L.; Laird, N.; Dietz, W.H.; Rimm, E.; Colditz, G.A. Impact of overweight on the risk of developing common chronic diseases during a 10-year period. Arch. Intern. Med. 2001, 161, 1581–1586. [Google Scholar] [CrossRef]
- The Diabetes Prevention Program Research Group. Relationship of body size and shape to the development of diabetes in the diabetes prevention program. Obesity 2006, 14, 2107–2117. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans; Government Printing Office: Washington, DC, USA, 2010, 7th ed. Available online: http://www.cnpp.usda.gov/DGAs2010-PolicyDocument.htm (accessed on 20 August 2013).
- Snowdon, D.A.; Phillips, R.L. Does a vegetarian diet reduce the occurrence of diabetes? Am. J. Public Health 1985, 75, 507–512. [Google Scholar] [CrossRef]
- Fraser, G.E. Associations between diet and cancer, ischemic heart disease, and all-cause mortality in non-hispanic white California Seventh-day Adventists. Am. J. Clin. Nutr. 1999, 70, S532–S538. [Google Scholar]
- Vang, A.; Singh, P.N.; Lee, J.W.; Haddad, E.H.; Brinegar, C.H. Meats, processed meats, obesity, weight gain and occurrence of diabetes among adults: Findings from Adventist Health Studies. Ann. Nutr. Metab. 2008, 52, 96–104. [Google Scholar] [CrossRef]
- Tonstad, S.; Butler, T.; Yan, R.; Fraser, G.E. Type of vegetarian diet, body weight and prevalence of type 2 diabetes. Diabetes Care 2009, 32, 791–796. [Google Scholar] [CrossRef]
- Tonstad, S.; Stewart, K.; Oda, K.; Batceh, M.; Herring, R.P.; Fraser, G.E. Vegetarian diets and incidence of diabetes in the Adventist Health Study-2. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 292–299. [Google Scholar] [CrossRef]
- Pan, A.; Sun, Q.; Bernstein, A.M.; Schulze, M.B.; Manson, J.E.; Willett, W.C.; Hu, F.B. Red meat consumption and risk of type 2 diabetes: 3 Cohorts of US adults and an ppdated meta-analysis. Am. J. Clin. Nutr. 2011, 94, 1088–1096. [Google Scholar] [CrossRef]
- Aune, D.; Ursin, G.; Veierod, M.B. Meat consumption and the risk of type 2 diabetes: A systematic review and meta-analysis of cohort studies. Diabetologia 2009, 52, 2277–2287. [Google Scholar] [CrossRef]
- Micha, R.; Wallace, S.K.; Mozaffarian, D. Red and processed meat consumption and risk of incident coronary heart disease, stroke, and diabetes mellitus: A systematic review and meta-analysis. Circulation 2010, 121, 2271–2283. [Google Scholar] [CrossRef]
- Fung, T.T.; Schulze, M.; Manson, J.E.; Willett, W.C.; Hu, F.B. Dietary patterns, meat intake, and the risk of type 2 diabetes in women. Arch. Intern. Med. 2004, 164, 2235–2240. [Google Scholar] [CrossRef]
- Schulze, M.B.; Manson, J.E.; Willett, W.C.; Hu, F.B. Processed meat intake and incidence of type 2 diabetes in younger and middle-aged women. Diabetologia 2003, 46, 1465–1473. [Google Scholar] [CrossRef]
- Kaushik, M.; Mozaffarian, D.; Spiegelman, D.; Manson, J.E.; Willett, W.C.; Hu, F.B. Long-chain omega-3 fatty acids, fish intake, and the risk of type 2 diabetes mellitus. Am. J. Clin. Nutr. 2009, 90, 613–620. [Google Scholar] [CrossRef]
- Nöthings, U.; Boeing, H.; Maskarinec, G.; Sluik, D.; Teucher, B.; Kaaks, R.; Tjonneland, A.; Halkjaer, J.; Dethlefsen, C.; Overvad, K.; et al. Food intake of individuals with and without diabetes across different countries and ethnic groups. Eur. J. Clin. Nutr. 2011, 65, 635–641. [Google Scholar] [CrossRef]
- Berkow, S.; Barnard, N.D. Vegetarian diets and weight status. Nutr. Rev. 2006, 64, 175–188. [Google Scholar] [CrossRef]
- Barnard, N.D.; Scialli, A.R.; Turner-McGrievy, G.; Lanou, A.J.; Glass, J. The effects of a low-fat, plant-based dietary intervention on body weight, metabolism, and insulin sensitivity. Am. J. Med. 2005, 118, 991–997. [Google Scholar] [CrossRef]
- Kendall, A.; Levitsky, D.A.; Strupp, B.J.; Lissner, J. Weight loss on a low-fat diet: Consequence of the imprecision of the control of food intake in humans. Am. J. Clin. Nutr. 1991, 53, 1124–1129. [Google Scholar]
- Howarth, N.C.; Saltzman, E.; Roberts, S.B. Dietary fiber and weight regulation. Nutr. Rev. 2001, 59, 129–139. [Google Scholar] [CrossRef]
- Bell, E.A.; Rolls, BJ. Energy density of foods affects energy intake across multiple levels of fat content in lean and obese women. Am. J. Clin. Nutr. 2001, 73, 1010–1018. [Google Scholar]
- Bujnowski, D.; Xun, P.; Daviglus, M.L.; van Horn, L.; He, K.; Stamler, J. Longitudinal association between animal and vegetable protein intake and obesity among men in the United States: The Chicago Western Electric Study. J. Am. Diet. Assoc. 2011, 111, 1150–1155. [Google Scholar] [CrossRef]
- Bravata, D.M.; Sanders, L.; Huang, J.; Krumholz, H.M.; Olkin, I.; Gardner, C.D.; Bravata, D.M. Efficacy and safety of low-carbohydrate diets: A systematic review. JAMA 2003, 289, 1837–1850. [Google Scholar] [CrossRef]
- Kahleova, H.; Matoulek, M.; Malinska, H.; Oliyarnik, O.; Kazdova, L.; Neskudla, T.; Skoch, A.; Hajek, M.; Hill, M.; Kahle, M. Vegetarian diet improves insulin resistance and oxidative stress markers more than conventional diet in subjects with type 2 diabetes. Diabet. Med. 2011, 28, 549–559. [Google Scholar] [CrossRef]
- Hamdy, O.; Porramatikul, S.; Al-Ozairi, E. Metabolic obesity: The paradox between visceral and subcutaneous fat. Curr. Diabetes Rev. 2006, 2, 367–373. [Google Scholar] [CrossRef]
- Petersen, K.F.; Dufour, S.; Befroy, D.; Garcia, R.; Shulman, G.I. Impaired mitochondrial activity in the insulin-resistant offspring of patients with type 2 diabetes. N. Engl. J. Med. 2004, 350, 664–671. [Google Scholar] [CrossRef]
- Krssak, M.; Petersen, K.F.; Dresner, A.; DiPietro, L.; Vogel, S.M.; Rothman, D.L.; Roden, M.; Shulman, G.I. Intramyocellular lipid concentrations are correlated with insulin sensitivity in humans: A 1H NMR Spectroscopy Study. Diabetologia 1999, 42, 113–116. [Google Scholar] [CrossRef]
- Perseghin, G.; Scifo, P.; de Cobelli, F.; Pagliato, E.; Battezzati, A.; Arcelloni, C.; Vanzulli, A.; Testolin, G.; Pozza, G.; Del Maschio, A. Intramyocellular triglyceride content is a determinant of in vivo insulin resistance in humans: A 1H-13C nuclear magnetic resonance spectroscopy assessment in offspring of type 2 diabetic parents. Diabetes 1999, 48, 1600–1606. [Google Scholar] [CrossRef]
- Sparks, L.M.; Xie, H.; Koza, R.A.; Mynatt, R.; Hulver, M.W.; Bray, G.A.; Smith, S.R. A High-fat diet coordinately downregulates genes required for mitochondrial oxidative phosphorylation in skeletal muscle. Diabetes 2005, 54, 1926–1933. [Google Scholar] [CrossRef]
- Goff, L.M.; Bell, J.D.; So, P.W.; Bornhorst, A.; Frost, G.S. Veganism and its relationship with insulin resistance and intramyocellular lipid. Eur. J. Clin. Nutr. 2005, 59, 291–298. [Google Scholar] [CrossRef]
- Rajpathak, S.N.; Crandall, J.P.; Wylie-Rosett, J.; Kabat, G.C.; Rohan, T.E.; Hu, F.B. The role of iron in type 2 diabetes in humans. Biochim. Biophys. Acta 2009, 1790, 671–681. [Google Scholar]
- Hua, N.W.; Stoohs, R.A.; Facchini, F.S. Low iron status and enhanced insulin sensitivity in lacto-ovo-vegetarians. Br. J. Nutr. 2001, 86, 515–519. [Google Scholar] [CrossRef]
- Liu, Q.; Sun, L.; Tan, Y.; Wang, G.; Lin, X.; Cai, L. Role of iron deficiency and overload in the pathogenesis of diabetes and diabetic complications. Curr. Med. Chem. 2009, 16, 113–129. [Google Scholar] [CrossRef]
- Pereira, E.C.; Ferderbar, S.; Bertolami, M.C.; Flaudi, A.A.; Monte, O.; Xavier, H.T.; Pereira, T.V.; Abdalla, D.S. Biomarkers of oxidative stress and endothelial dysfunction in glucose Intolerance and diabetes mellitus. Clin. Biochem. 2008, 41, 1454–1460. [Google Scholar] [CrossRef]
- Barbaresko, J.; Koch, M.; Schulze, M.B.; Nöthlings, U. Dietary pattern analysis and biomarkers of low-grade inflammation: A systematic literature review. Nutr. Rev. 2013, 71, 511–527. [Google Scholar] [CrossRef]
- Lev, S.H.; Sun, Q.; Willett, W.C.; Eliassen, A.H.; Wu, K.; Pan, A.; Grodstein, F.; Hu, F.B. Associations between red meat intake and biomarkers of inflammation and glucose metabolism in women. Am. J. Clin. Nutr. 2010, 99, 352–360. [Google Scholar]
- Narayan, K.M.; Boyle, J.P.; Thompson, T.J.; Sorensen, S.W.; Williamson, D.F. Lifetime risk for diabetes mellitus in the United States. JAMA 2003, 290, 1884–1890. [Google Scholar] [CrossRef]
- Ferdowsian, H.R.; Barnard, N.D. The effects of plant-based diets on plasma lipids. Am. J. Cardiol. 2009, 104, 947–956. [Google Scholar] [CrossRef]
- Berkow, S.; Barnard, N.D. Blood pressure regulation and vegetarian diets. Nutr. Rev. 2005, 63, 1–8. [Google Scholar] [CrossRef]
- Ornish, D.; Brown, S.E.; Scherwitz, L.W.; Billings, J.H.; Armstrong, W.T.; Ports, T.A.; McLanahan, S.M.; Kirkeeide, R.L.; Brand, R.J.; Gould, K.L. Can lifestyle changes reverse coronary heart disease? Lancet 1990, 336, 129–133. [Google Scholar] [CrossRef]
- Ornish, D.; Scherwitz, L.W.; Billings, J.H.; Brown, S.E.; Gould, K.L.; Merritt, T.A.; Sparler, S.; Armstrong, W.T.; Ports, T.A.; Kirkeedie, R.L. Intensive lifestyle changes for reversal of coronary heart disease. JAMA 1998, 280, 2001–2007. [Google Scholar] [CrossRef]
- Barnard, N.D.; Cohen, J.; Jenkins, D.J.; Turner-McGrievy, G.; Gloede, L.; Jaster, B.; Seidl, K.; Green, A.A.; Talpers, S. A low-fat, vegan diet improves glycemic control and cardiovascular risk factors in a randomized clinical trial in individuals with type 2 diabetes. Diabetes Care 2006, 29, 1777–1783. [Google Scholar] [CrossRef]
- Vogt, T.M.; Appel, L.J.; Obarzanek, E.; Moore, T.J.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Cutler, J.A.; Windhauser, M.M. Dietary approaches to stop hypertension: Rationale, design, and methods. J. Am. Diet. Assoc. 1999, 99, S12–S18. [Google Scholar] [CrossRef]
- Turner-McGrievy, G.M.; Barnard, N.D.; Scialli, A.R. A two-year randomized weight loss trial comparing a vegan diet to a more moderate low-fat diet. Obesity 2007, 15, 2276–2281. [Google Scholar] [CrossRef]
- Meat, Poultry, and Fish Per Capita Availability Adjusted for Loss. Available online: http://www.ers.usda.gov/Data/FoodConsumption/FoodGuideIndex.htm#meat (accessed on 20 August 2013).
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Barnard, N.; Levin, S.; Trapp, C. Meat Consumption as a Risk Factor for Type 2 Diabetes. Nutrients 2014, 6, 897-910. https://doi.org/10.3390/nu6020897
Barnard N, Levin S, Trapp C. Meat Consumption as a Risk Factor for Type 2 Diabetes. Nutrients. 2014; 6(2):897-910. https://doi.org/10.3390/nu6020897
Chicago/Turabian StyleBarnard, Neal, Susan Levin, and Caroline Trapp. 2014. "Meat Consumption as a Risk Factor for Type 2 Diabetes" Nutrients 6, no. 2: 897-910. https://doi.org/10.3390/nu6020897