Comparison between Calcitriol and Calcitriol Plus Low-Dose Cinacalcet for the Treatment of Moderate to Severe Secondary Hyperparathyroidism in Chronic Dialysis Patients


 and
and
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Population
2.2. Demographic and Laboratory Data
2.3. Statistical Analysis
2.4. Ethical Issues
3. Results
3.1. Baseline Characteristics between Different Treatment Groups (Table 1)

{kind=link}
{kind=link}
| All (N = 81) | d-Cinacalcet (N = 40) | VitD (N = 41) | p value | |
|---|---|---|---|---|
| Age (years) | 55.5 ± 12.6 | 54.1 ± 11.3 | 57.0 ± 13.8 | 0.304 |
| Gender (%) | 0.750 | |||
| Male | 33 (41) | 17 (43) | 16 (39) | |
| Female | 48 (59) | 23 (57) | 25 (61) | |
| Dialysis duration (months) | 99.4 ± 51.5 | 89.4 ± 52.3 | 109.2 ± 49.5 | 0.085 |
| Primary cause of renal failure (%) | 0.293 | |||
| Chronic glomerulonephritis | 49 (60) | 27 (68) | 22 (54) | |
| Diabetes mellitus | 9 (11) | 3 (7) | 6 (15) | |
| Polycystic kidney disease | 2 (3) | 2 (5) | 0 (0) | |
| Hypertension | 12 (15) | 4 (10) | 8 (19) | |
| Obstructive nephropathy | 9 (11) | 4 (10) | 5 (12) | |
| Comorbidity (%) | ||||
| Diabetes mellitus | 12 (15) | 4 (10) | 8 (20) | 0.228 |
| Hypertension | 47 (58) | 22 (55) | 25 (61) | 0.586 |
| Severity of UHPT * (%) | 0.396 | |||
| Moderate (iPTH: 500–800 pg/mL) | 19 (23) | 11 (27.5) | 8 (19.5) | |
| Severe (iPTH > 800 pg/mL) | 62 (77) | 29 (72.5) | 33 (80.5) | |
| Calcium (mg/dL) | 9.8 ± 0.6 | 9.9 ± 0.6 | 9.7 ± 0.6 | 0.065 |
| Phosphorus (mg/dL) | 5.8 ± 1.1 | 5.9 ± 1.3 | 5.7 ± 0.8 | 0.373 |
| Ca × P (mg2/dL2) | 56.7 ± 12.2 | 58.7 ± 15.0 | 54.8 ± 8.4 | 0.157 |
| intact PTH (pg/mL) | 1140.4 ± 450.7 | 1166.0 ± 469.3 | 1115.5 ± 436.2 | 0.618 |
| Albumin (mg/dL) | 3.9 ± 0.3 | 3.9 ± 0.2 | 3.9 ± 0.4 | 0.319 |
| Alkaline phosphate (U/L) | 139.2 ± 90.4 | 145.4 ± 87.6 | 133.2 ± 93.8 | 0.548 |
| Hemoglobin (mg/dL) | 10.4 ± 1.3 | 10.4 ± 1.4 | 10.4 ± 1.1 | 0.966 |
| nPNA (g/kg/day) ┼ | 1.15 ± 0.42 | 1.16 ± 0.38 | 1.14 ± 0.49 | 0.586 |
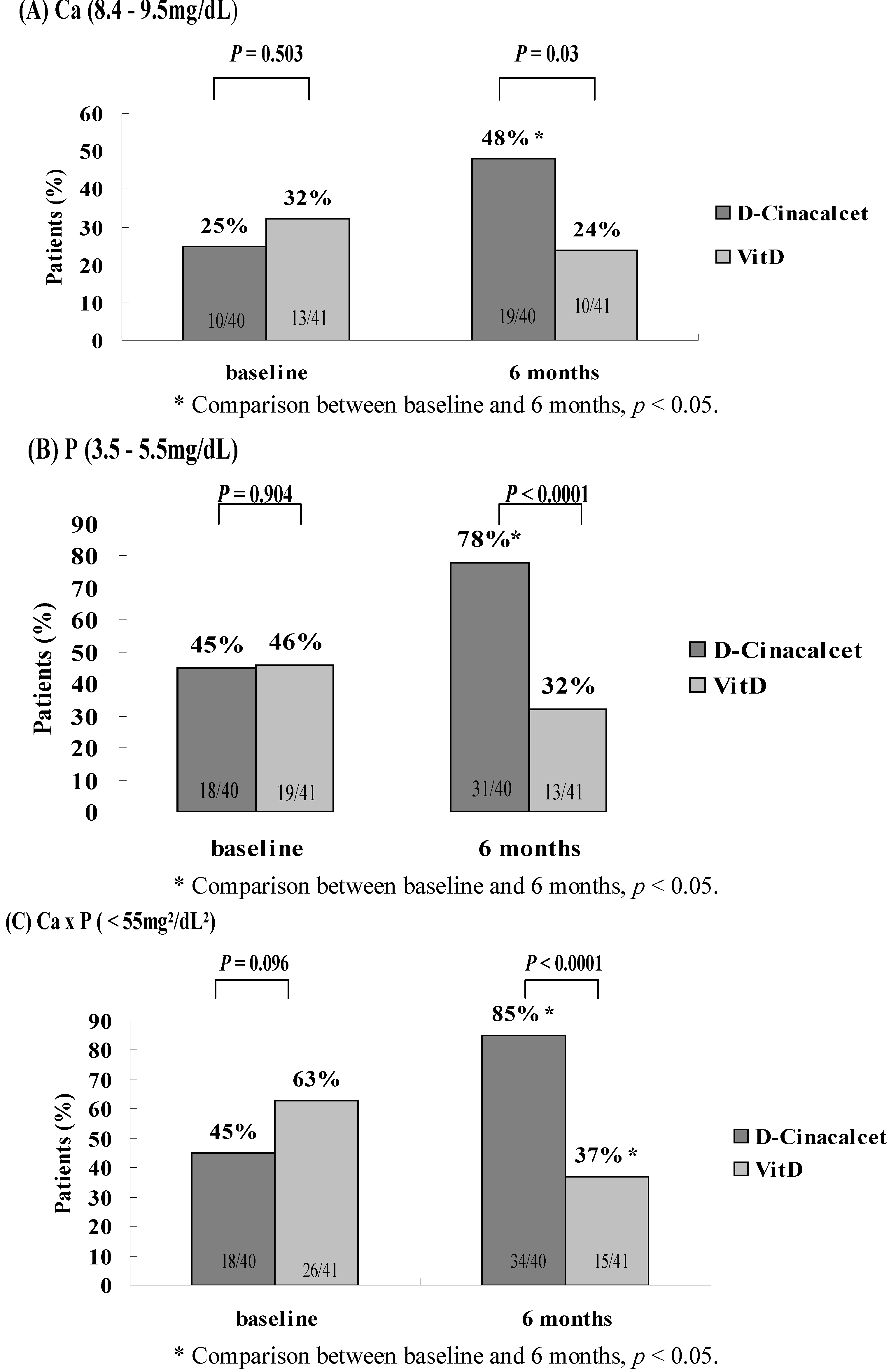
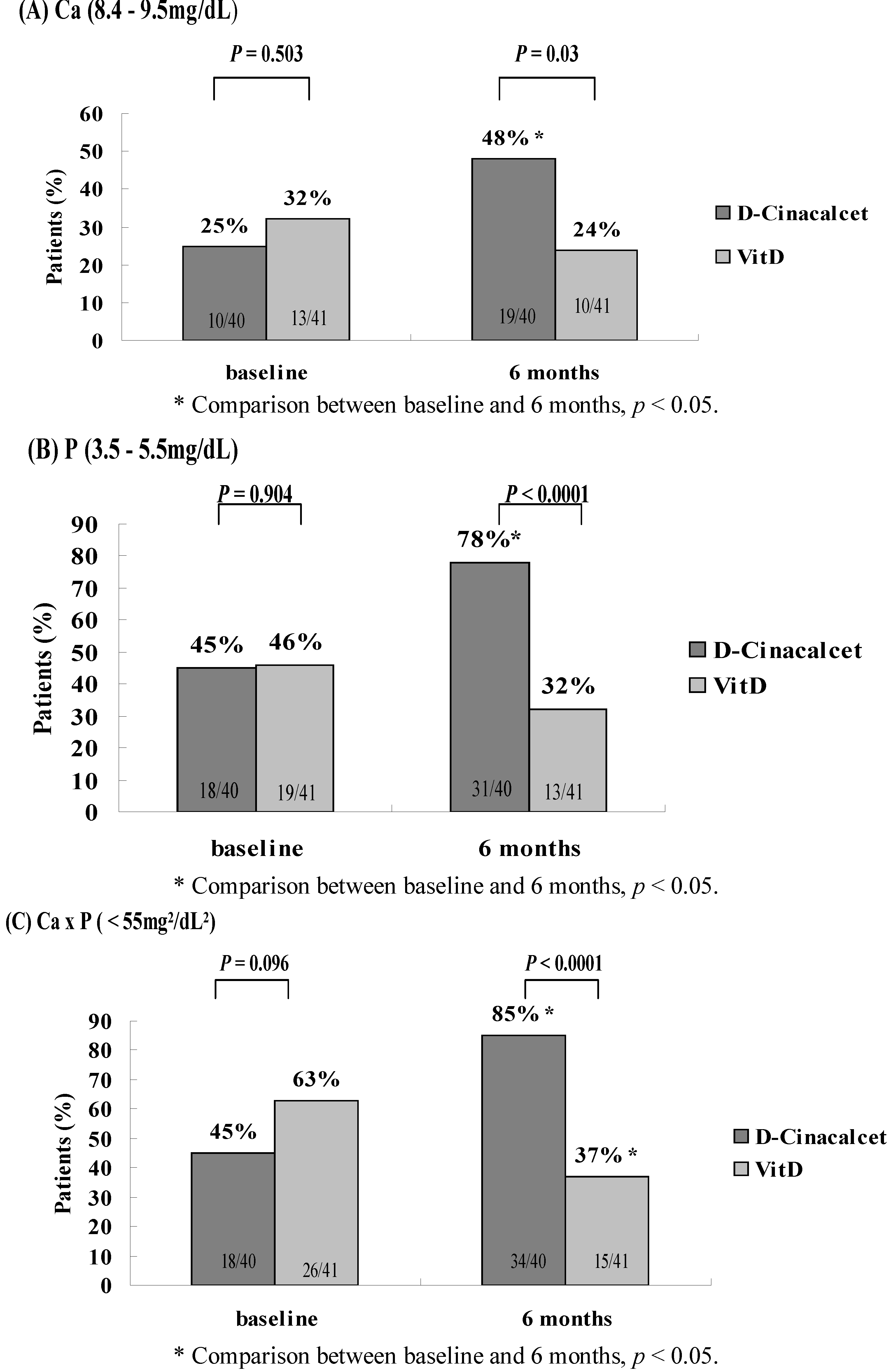
3.2. Comparison of Longitudinal Evolution of CKD-Mineral Bone Disease Parameters Stratified by Diverse Treatment Modalities (Table 2)
| d-Cinacalcet (N = 40) | VitD (N = 41) | p value | |
|---|---|---|---|
| Calcium (mg/dL) | |||
| Baseline | 9.9 ± 0.6 | 9.7 ± 0.6 | 0.065 |
| 3 months | 9.4 ± 0.7 a | 9.8 ± 0.6 | 0.004 |
| Reduction rate (%) | 5.6 ± 6.9 | −1.2 ± 6.0 | <0.0001 |
| 6 months | 9.6 ± 0.8 b | 10.0 ± 0.6 b | 0.018 |
| Reduction rate (%) | 3.5 ± 7.1 | −2.9 ± 5.1 | <0.0001 |
| Phosphorus (mg/dL) | |||
| Baseline | 5.9 ± 1.3 | 5.7 ± 0.8 | 0.373 |
| 3 months | 5.4 ± 1.2 a | 6.0 ± 1.0 | 0.032 |
| Reduction rate (%) | 5.8 ± 16.6 | −6.4 ± 18.4 | 0.003 |
| 6 months | 4.9 ± 0.9 bc | 5.7 ± 0.9 | <0.0001 |
| Reduction rate (%) | 14.3 ± 17.3 | −2.9 ± 20.5 | <0.0001 |
| Ca×P (mg2/dL2) | |||
| Baseline | 58.7 ± 15.0 | 54.8 ± 8.4 | 0.157 |
| 3 months | 51.0 ± 11.3 a | 58.4 ± 10.2 a | 0.003 |
| Reduction rate (%) | 10.5 ± 19.8 | −7.7 ± 20.2 | <0.0001 |
| 6 months | 46.9 ± 8.9 bc | 56.9 ± 9.0 | <0.0001 |
| Reduction rate (%) | 17.0 ± 20.0 | −5.7 ± 20.8 | <0.0001 |
| intact PTH (pg/mL) | |||
| Baseline | 1166.0 ± 469.3 | 1115.5 ± 436.2 | 0.618 |
| 3 months | 838.0 ± 418.4 a | 1152.7 ± 728.4 | 0.024 |
| Reduction rate (%) | 27.3 ± 21.1 | 3.7 ± 46.4 | 0.005 |
| 6 months | 679.8 ± 421.6 bc | 1021.9 ± 655.1 | 0.007 |
| Reduction rate (%) | 40.1 ± 26.5 | 7.7 ± 40.8 | <0.0001 |
| Albumin (mg/dL) | |||
| Baseline | 3.9 ± 0.2 | 3.9 ± 0.4 | 0.319 |
| 3 months | 3.8 ± 0.4 | 3.9 ± 0.2 | 0.104 |
| 6 months | 3.7 ± 0.4 | 3.7 ± 0.3 | 0.503 |
| Alkaline phosphate (U/L) | |||
| Baseline | 145.4 ± 87.6 | 133.2 ± 93.8 | 0.548 |
| 3 months | 139.7 ± 76.3 | 130.0 ± 92.0 | 0.609 |
| 6 months | 132.9 ± 90.6 | 130.2 ± 102.9 | 0.900 |
| Hemoglobin (mg/dL) | |||
| Baseline | 10.4 ± 1.4 | 10.4 ± 1.1 | 0.966 |
| 3 months | 10.8 ± 1.3 | 10.3 ± 1.1 | 0.109 |
| 6 months | 10.6 ± 1.2 | 10.4 ± 1.2 | 0.337 |
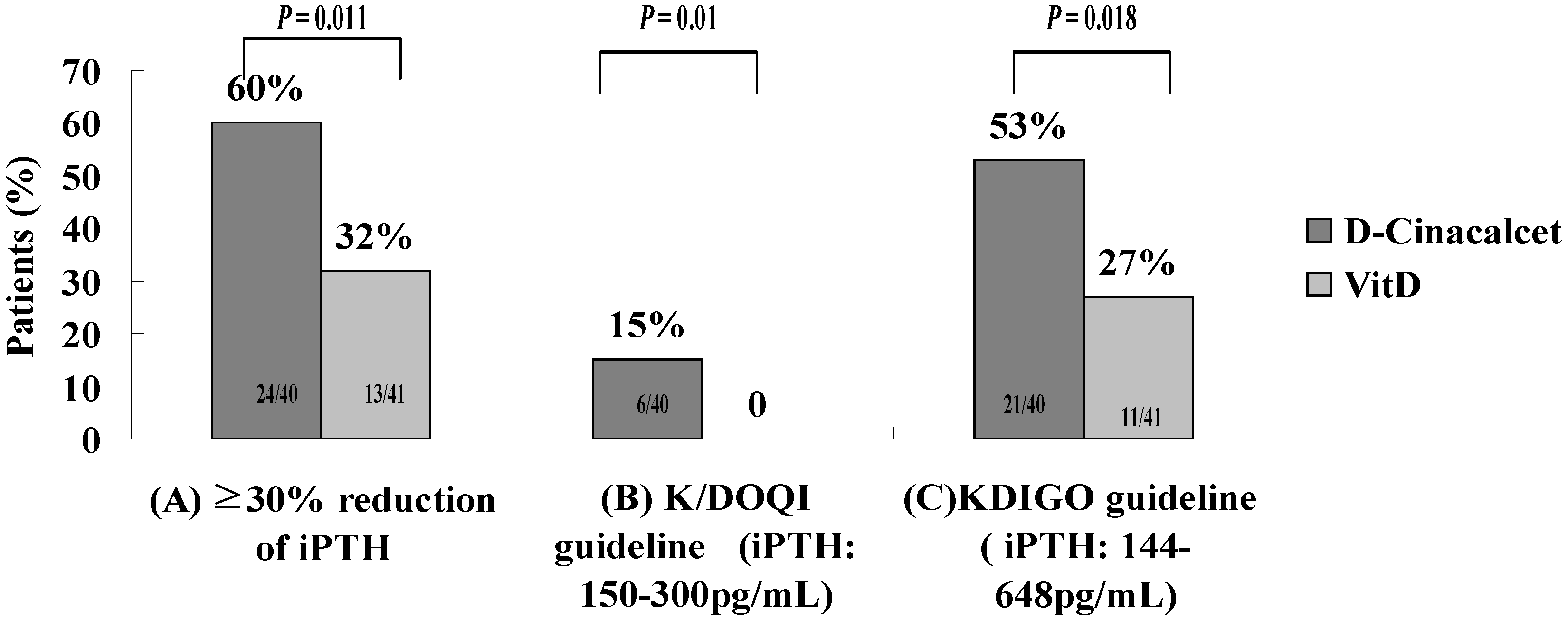
3.3. Goal Attainment of K/DOQI and KDIGO

3.4. The Use and Dosage of Phosphate Binder and Calcitriol
| Baseline | 6 months | |||||
|---|---|---|---|---|---|---|
| d-Cinacalcet (N = 40) | VitD (N = 41) | p value | d-Cinacalcet (N = 40) | VitD (N = 41) | p value | |
| Use of calcitriol (%) | 26 (65) | 41 (100) | <0.0001 | 30 (75) | 25 (61) * | 0.176 |
| Intravenous calcitriol (%) | 14 (35) | 34 (83) | <0.0001 | 17 (43) | 24 (59) * | 0.221 |
| Dose (μg/week) | 5.43 ± 0.94 | 4.94 ± 1.35 | 0.184 | 4.47 ± 1.33 | 4.28 ± 1.50 * | 0.226 |
| Oral Calcitriol (%) | 12 (30) | 7 (17) | 0.170 | 13 (33) | 1 (2)* | <0.0001 |
| Dose (μg/week) | 2.17 ± 0.58 | 2.05 ± 0.21 | 0.124 | 2.27 ± 0.88 | 2.31 ± 0.35 | 0.773 |
| Use of phosphate binders (%) | 33 (83) | 40 (98) | 0.023 | 28 (70) | 37 (90) | 0.022 |
| Aluminum hydroxide (%) | 24 (60) | 36 (88) | 0.004 | 12 (30) * | 31 (76) | <0.0001 |
| Dose (mg/day) | 1333 ± 481 | 1167 ± 378 | 0.161 | 1166 ± 389 * | 1129 ± 341 | 0.772 |
| Calcium carbonate (%) | 11 (28) | 15 (37) | 0.381 | 19 (48) * | 18 (44) | 0.745 |
| Dose (mg/day) | 1948 ± 727 | 1800 ± 621 | 0.592 | 1816 ± 628 | 1705.0 ± 443 | 0.542 |
| Calcium acetate (%) | 4 (10) | 6 (15) | 0.526 | 7 (18) | 5 (12) | 0.502 |
| Dose (mg/day) | 2143 ± 861 | 2293 ± 885 | 0.806 | 1920 ± 334 | 2742 ± 939 | 0.070 |
4. Discussion
4.1. Combination Therapy of Low-Dose Cinacalcet and Calcitriol: A Solution for Moderate to Severe UHPT
4.2. Combination Therapy of Low-Dose Cinacalcet and Calcitriol to Reduce Hypocalcemia Episodes and Use of Aluminum Hydroxide
4.3. Limitations of the Study
5. Conclusions
Conflict of Interest
References
- Levin, A.; Bakris, G.L.; Molitch, M.; Smulders, M.; Tian, J.; Williams, L.A.; Andress, D.L. Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: Results of the study to evaluate early kidney disease. Kidney Int. 2007, 71, 31–38. [Google Scholar] [CrossRef]
- Pitts, T.O.; Piraino, B.H.; Mitro, R.; Chen, T.C.; Segre, G.V.; Greenberg, A.; Puschett, J.B. Hyperparathyroidism and 1,25-dihydroxyvitamin D deficiency in mild, moderate, and severe renal failure. J. Clin. Endocrinol. Metab. 1988, 67, 876–881. [Google Scholar] [CrossRef]
- Li, Y.C.; Amling, M.; Pirro, A.E.; Priemel, M.; Meuse, J.; Baron, R.; Delling, G.; Demay, M.B. Normalization of mineral ion homeostasis by dietary means prevents hyperparathyroidism, rickets, and osteomalacia, but not alopecia in vitamin D receptor-ablated mice. Endocrinology 1998, 139, 4391–4396. [Google Scholar] [CrossRef]
- Panda, D.K.; Miao, D.; Bolivar, I.; Li, J.; Huo, R.; Hendy, G.N.; Goltzman, D. Inactivation of the 25-hydroxyvitamin D 1alpha-hydroxylase and vitamin D receptor demonstrates independent and interdependent effects of calcium and vitamin D on skeletal and mineral homeostasis. J. Biol. Chem. 2004, 279, 16754–16766. [Google Scholar]
- Krajisnik, T.; Björklund, P.; Marsell, R.; Ljunggren, O.; Akerström, G.; Jonsson, K.B.; Westin, G.; Larsson, T.E. Fibroblast growth factor-23 regulates parathyroid hormone and 1alpha-hydroxylase expression in cultured bovine parathyroid cells. J. Endocrinol. 2007, 195, 125–131. [Google Scholar] [CrossRef]
- Lee, C.T.; Tsai, Y.C.; Ng, H.Y.; Su, Y.; Lee, W.C.; Lee, L.C.; Chiou, T.T.; Liao, S.C.; Hsu, K.T. Association between C-reactive proteinandbiomarkers of bone and mineralmetabolism in chronic hemodialysis patients: A cross-sectional study. J. Ren. Nutr. 2009, 19, 220–227. [Google Scholar] [CrossRef]
- Block, G.A.; Klassen, P.S.; Lazarus, J.M.; Ofsthun, N.; Lowrie, E.G.; Chertow, G.M. Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. J. Am. Soc. Nephrol. 2004, 15, 2208–2218. [Google Scholar] [CrossRef]
- Palmer, S.C.; Hayen, A.; Macaskill, P.; Pellegrini, F.; Craig, J.C.; Elder, G.J.; Strippoli, G.F. Serum levels of phosphorous, parathyroid hormone, and calcium and risks of death and cardiovascular disease in individiuals with chronic kidney disease: A systematic review and meta-analysis. JAMA 2011, 305, 1119–1127. [Google Scholar]
- Kalantar-Zadeh, K.; Kuwae, N.; Regidor, D.L.; Kovesdy, C.P.; Kilpatrick, R.D.; Shinaberger, C.S.; McAllister, C.J.; Budoff, M.J.; Salusky, I.B.; Kopple, J.D. Survival predictability of time varying indicators of bone disease in maintenance hemodialysis patients. Kidney Int. 2006, 70, 771–780. [Google Scholar] [CrossRef]
- Teng, M.; Wolf, M.; Ofsthun, M.N.; Lazarus, J.M.; Hernán, M.A.; Camargo, C.A., Jr.; Thadhani, R. Activated injectable vitamin D and hemodialysis survival: A historical cohort study. J. Am. Soc. Nephrol. 2005, 16, 1115–1125. [Google Scholar] [CrossRef]
- Teng, M.; Wolf, M.; Lowrie, E.; Ofsthun, N.; Lazarus, J.M.; Thadhani, R. Survival of patients undergoing hemodialysis with paricalcitol or calcitriol therapy. N. Engl. J. Med. 2003, 349, 446–456. [Google Scholar] [CrossRef]
- Shoji, T.; Shinohara, K.; Kimoto, E.; Emoto, M.; Tahara, H.; Koyama, H.; Inaba, M.; Fukumoto, S.; Ishimura, E.; Miki, T.; et al. Lower risk for cardiovascular mortality in oral 1alpha-hydroxy vitamin D3 users in a haemodialysis population. Nephrol. Dial. Transplant. 2004, 19, 179–184. [Google Scholar] [CrossRef]
- Palmer, S.C.; McGregor, D.O.; Macaskill, P.; Craig, J.C.; Elder, G.J.; Strippoli, G.F. Meta-Analysis: Vitamin D compounds in chronic kidney disease. Ann. Intern. Med. 2007, 147, 840–853. [Google Scholar]
- Goodman, W.G.; Frazao, J.M.; Goodkin, D.A.; Turner, S.A.; Liu, W.; Coburn, J.W. A calcimimetic agent lowers plasma parathyroid hormone levels in patients with secondary hyperparathyroidism. Kidney Int. 2000, 58, 436–445. [Google Scholar] [CrossRef]
- Block, G.A.; Martin, K.J.; de Francisco, A.L.; Turner, S.A.; Avram, M.M.; Suranyi, M.G.; Hercz, G.; Cunningham, J.; Abu-Alfa, A.K.; Messa, P.; et al. Cinacalcet for secondary hyperparathyroidism in patients receiving hemodialysis. N. Engl. J. Med. 2004, 350, 1516–1525. [Google Scholar] [CrossRef]
- Block, G.A.; Zaun, D.; Smits, G.; Persky, M.; Brillhart, S.; Nieman, K.; Liu, J.; St Peter, W.L. Cinacalcet hydrochloride treatment significantly improved all-cause and cardiovascular survival in a large cohort of hemodialysis patients. Kidney Int. 2010, 78, 578–589. [Google Scholar] [CrossRef]
- Fishbane, S.; Shapiro, W.B.; Corry, D.B.; Vicks, S.L.; Roppolo, M.; Rappaport, K.; Ling, X.; Goodman, W.G.; Turner, S.; Charytan, C. Cinacalcet HCL and concurrent low-dose vitamin D improves treatment of secondary hyperparathyroidism in dialysis patients compared with vitamin D alone: The ACHIEVE study results. Clin. Am. Soc. Nephrol. 2008, 3, 1718–1725. [Google Scholar] [CrossRef]
- Block, G.A.; Zeig, S.; Sugihara, J.; Chertow, G.M.; Chi, E.M.; Turner, S.A.; Bushinsky, D.A; TARGET Investigators. Combined therapy with cinacalcet and low doses of vitamin D sterols in patients with moderate to severe secondary hyperparathyroidism. Nephrol. Dial. Transplant. 2008, 23, 2311–2318. [Google Scholar]
- Ketteler, M.; Martin, K.J.; Cozzolino, M.; Goldsmith, D.; Sharma, A.; Khan, S.; Dumas, E.; Amdahl, M.; Marx, S.; Audhya, P. Paricalcitol versus cinacalcet plus low-dose vitamin D therapy for the treatment of secondary hyperparathyroidism in patients receiving haemodialysis: Results of the IMPACT SHPT study. Nephrol. Dial. Transplant. 2012, 27, 3270–3278. [Google Scholar] [CrossRef]
- National Kidney Foundation. K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am. J. Kidney Dis. 2003, 42, S1–S201.
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group. KDIGO clinical practice guidelines for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease-mineral and bone disorder (CKD-MBD). Kidney Int. 2009, 76, S1–S130.
- Frazão, J.M.; Messa, P.; Mellotte, G.J.; Geiger, H.; Hagen, E.C.; Quarles, L.D.; Kerr, P.G.; Baños, A.; Dehmel, B.; Urena, P. Cinacalcet reduces plasma intact parathyroid hormone, serum phosphorus and calcium levels in patients with secondary hyperparathyroidism irrespective its severity. Clin. Nephrol. 2011, 76, 233–243. [Google Scholar]
- Martin, K.J.; González, E.A.; Gellens, M.; Hamm, L.L.; Abboud, H.; Lindberg, J. 19-Nor-1-alpha-25-dihydroxyvitamin D2 (paricalcitol) safely and effectively reduces the levels of intact parathyroid hormone in patients on hemodialysis. J. Am. Soc. Nephrol. 1998, 9, 1427–1432. [Google Scholar]
- Ross, E.A.; Tian, J.; Abboud, H.; Hippensteel, R.; Melnick, J.Z.; Pradhan, R.S.; Williams, L.A.; Hamm, L.L.; Sprague, S.M. Oral paricalcitol for the treatment of secondary hyperparathyroidism on hemodialysis or peritoneal dialysis. Am. J. Nephrol. 2008, 28, 97–106. [Google Scholar] [CrossRef]
- Antonsen, J.E.; Sherrard, D.J.; Andress, D.L. A calcimimetic agent acutely suppresses parathyroid hormone levels in patients with chronic renal failure. Rapid communication. Kidney Int. 1998, 53, 223–227. [Google Scholar]
- Goodman, W.G.; Hladik, G.A.; Turner, S.A.; Blaisdell, P.W.; Goodkin, D.A.; Liu, W.; Barri, Y.M.; Cohen, R.M.; Coburn, J.W. The Calcimimetic agent AMG 073 lowers plasma parathyroid hormone levels in hemodialysis patients with secondary hyperparathyroidism. J. Am. Soc. Nephrol. 2002, 13, 1017–1024. [Google Scholar]
- Fukagawa, M.; Yumita, S.; Akizawa, T.; Uchida, E.; Tsukamoto, Y.; Iwasaki, M.; Koshikawa, S.; KRN1493 study group. Cinacalcet (KRN1493) effectively decreases the serum intact PTH level with favourable control of the serum phosphorous and calcium levels in Japanese dialysis patients. Nephrol. Dial. Transplant. 2008, 23, 328–335. [Google Scholar]
- Rothe, H.M.; Shapiro, W.B.; Sun, W.Y.; Chou, S.Y. Calcium-Sensing receptor gene polymorphism Arg990Gly and its possible effect on response to cinacalcet HCl. Pharmacogenet. Genomics 2005, 15, 29–34. [Google Scholar] [CrossRef]
- Li, D.; Shao, L.; Zhou, H.; Jiang, W.; Zhang, W.; Xu, Y. The efficacy of cinacalcet combined with conventional therapy on bone and mineral metabolism in dialysis patients with secondary hyperparathyroidism: A meta-analysis. Endocrine 2013, 43, 68–77. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Lee, Y.-T.; Ng, H.-Y.; Kuo, C.-C.; Chen, T.-C.; Wu, C.-S.; Chiu, T.T.-Y.; Lee, W.-C.; Lee, C.-T. Comparison between Calcitriol and Calcitriol Plus Low-Dose Cinacalcet for the Treatment of Moderate to Severe Secondary Hyperparathyroidism in Chronic Dialysis Patients. Nutrients 2013, 5, 1336-1348. https://doi.org/10.3390/nu5041336
Lee Y-T, Ng H-Y, Kuo C-C, Chen T-C, Wu C-S, Chiu TT-Y, Lee W-C, Lee C-T. Comparison between Calcitriol and Calcitriol Plus Low-Dose Cinacalcet for the Treatment of Moderate to Severe Secondary Hyperparathyroidism in Chronic Dialysis Patients. Nutrients. 2013; 5(4):1336-1348. https://doi.org/10.3390/nu5041336
Chicago/Turabian StyleLee, Yueh-Ting, Hwee-Yeong Ng, Chien-Chun Kuo, Te-Chuan Chen, Chien-Shing Wu, Terry Ting-Yu Chiu, Wen-Chin Lee, and Chien-Te Lee. 2013. "Comparison between Calcitriol and Calcitriol Plus Low-Dose Cinacalcet for the Treatment of Moderate to Severe Secondary Hyperparathyroidism in Chronic Dialysis Patients" Nutrients 5, no. 4: 1336-1348. https://doi.org/10.3390/nu5041336