Calcium Intake and Body Composition in African-American Children and Adolescents at Risk for Overweight and Obesity

Abstract
:1. Introduction
2. Experimental Section
2.1. Participants
2.2. Measurements
2.2.1. Three-Day Food Diary
2.2.2. Blood Pressure
2.2.3. Lipid Measurements
2.2.4. Glucose Measurements
2.2.5. Body Composition from Dual Energy X-ray Absorptiometry (DXA)
2.2.6. Anthropometric Measurements
2.3. Statistical Analyses
3. Results and Discussion
3.1. Results

{kind=link}
{kind=link}
| Female | Male | |||
|---|---|---|---|---|
| 11–13.9 (n = 32) | 14–18 (n = 80) | 11–13.9 (n = 28) | 14–18 (n = 46) | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| Weight (kg) | 85 ± 23 | 102 ± 22 | 87 ± 22 | 110 ± 21 |
| Height (cm) | 158 ± 6 | 162 ± 8 | 163 ± 11 | 170 ± 7 |
| BMI (kg/m2) | 34 ± 9 | 38 ± 8 | 33 ± 7 | 38 ± 7 |
| BMI Z score | 2.2 ± 0.5 | 2.2 ± 0.4 | 2.3 ± 0.4 | 2.5 ± 0.5 |
| Relative BMI (%) | 184 ± 51 | 189 ± 37 | 179 ± 37 | 185 ± 33 |
| Whole Body Bone Mineral Content (kg) | 2.1 ± 0.3 | 2.5 ± 0.3 | 2.1 ± 0.4 | 2.7 ± 0.4 |
| Whole Body Bone Mineral Density (g/cm2) | 1.02 ± 0.09 | 1.16 ± 0.08 | 1.00 ± 0.10 | 1.14 ± 0.11 |
| Fat Mass (kg) | 38 ± 16 | 47 ± 14 | 35 ± 15 | 44 ± 15 |
| Fat Free Mass (kg) | 48 ± 8 | 55 ± 9 | 51 ± 10 | 66 ± 9 |
| Total Mass (Fat + Fat Free Mass) (kg) | 86 ± 23 | 102 ± 22 | 87 ± 22 | 110 ± 21 |
| Body Fat (%) | 43 ± 7 | 45 ± 6 | 40 ± 9 | 39 ± 7 |
| Systolic Hypertension (%) | ||||
| Normotensive | 50.0 | 45.0 | 48.3 | 37.8 |
| Prehypertension | 18.8 | 22.5 | 20.7 | 26.7 |
| Hypertension | 31.3 | 32.5 | 27.6 | 35.6 |
| Diastolic Hypertension (%) | ||||
| Normotensive | 96.9 | 85.0 | 89.7 | 95.6 |
| Prehypertension | 3.1 | 10.0 | 3.4 | 4.4 |
| Hypertension | 0 | 5.0 | 6.9 | 0 |
| Impaired Glucose Metabolism | 31.3 | 20.3 | 22.2 | 33.3 |
| Dyslipidemia | 51.6 | 43.0 | 52.2 | 64.4 |
| Female | Male | Female | Male | |
|---|---|---|---|---|
| 11–13 y (n = 32) | 11–13 y (n = 28) | 14–19 y (n = 80) | 14–19 y (n = 46) | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| Energy (kcal) | 1775.6 ± 631.5 | 1902.6 ± 529.7 | 1688.7 ± 700.1 | 1926.4 ± 416.1 |
| Protein (g) | 68.1 ± 24.2 | 72.7 ± 21.8 | 63.4 ± 24.9 | 74.7 ± 22.3 |
| Carbohydrate (g) | 216.6 ± 78.9 | 230.0 ± 72.9 | 200.6 ± 99.3 | 234.5 ± 55.5 |
| Fat (g) | 71.9 ± 29.0 | 78.0 ± 23.8 | 71.2 ± 33.0 | 78.7 ± 19.9 |
| Fiber, total dietary (g) | 9.1 ± 3.5 | 9.8 ± 5.2 | 9.3 ± 5.0 | 10.0 ± 4.3 |
| Riboflavin (mg) | 1.0 ± 0.6 | 1.1 ± 0.5 | 0.9 ± 0.5 | 1.1 ± 0.6 |
| Folate (mcg) | 161.2 ± 112.2 | 174.4 ± 100.7 | 158.2 ± 107.0 | 181.5 ± 156.3 |
| Vitamin B-12 (mcg) | 5.1 ± 6.6 | 2.9 ± 2.9 | 2.9 ± 5.3 | 2.9 ± 3.8 |
| Vit-A (mcg_RAE) | 284.6 ± 417.5 | 181.4 ± 126.2 | 176.9 ± 153.8 | 223.2 ± 193.9 |
| Vitamin D (IU) | 65.3 ± 74.2 | 63.2 ± 49.4 | 41.5 ± 57.5 | 56.1 ± 71.4 |
| Tocopherol, alpha (mg) | 1.1 ± 0.9 | 1.5 ± 1.2 | 1.7 ± 2.0 | 1.5 ± 2.0 |
| Vitamin K (mcg) | 17.3 ± 33.6 | 20.3 ± 38.2 | 26.8 ± 45.4 | 15.3 ± 24.5 |
| Vitamin C (mg) | 46.8 ± 37.2 | 63.7 ± 50.4 | 52.9 ± 45.4 | 69.1 ± 51.6 |
| Calcium (mg) | 509.0 ± 254.8 | 671.8 ± 280.7 | 489.3 ± 252.3 | 613.9 ± 236.0 |
| Magnesium (mg) | 87.0 ± 50.4 | 112.9 ± 54.5 | 100.1 ± 69.9 | 94.8 ± 58.6 |
| Phosphorus (mg) | 572.0 ± 374.6 | 738.1 ± 389.4 | 552.1 ± 361.0 | 547.3 ± 365.9 |
| Potassium (mg) | 982.3 ± 446.3 | 1364.0 ± 643.0 | 1218.7 ± 833.1 | 1186.6 ± 615.7 |
| Iron (mg) | 11.0 ± 4.4 | 10.5 ± 3.1 | 10.4 ± 6.5 | 12.1 ± 4.6 |
| Zinc (mg) | 4.6 ± 3.3 | 5.4 ± 2.7 | 5.2 ± 4.0 | 5.0 ± 3.8 |
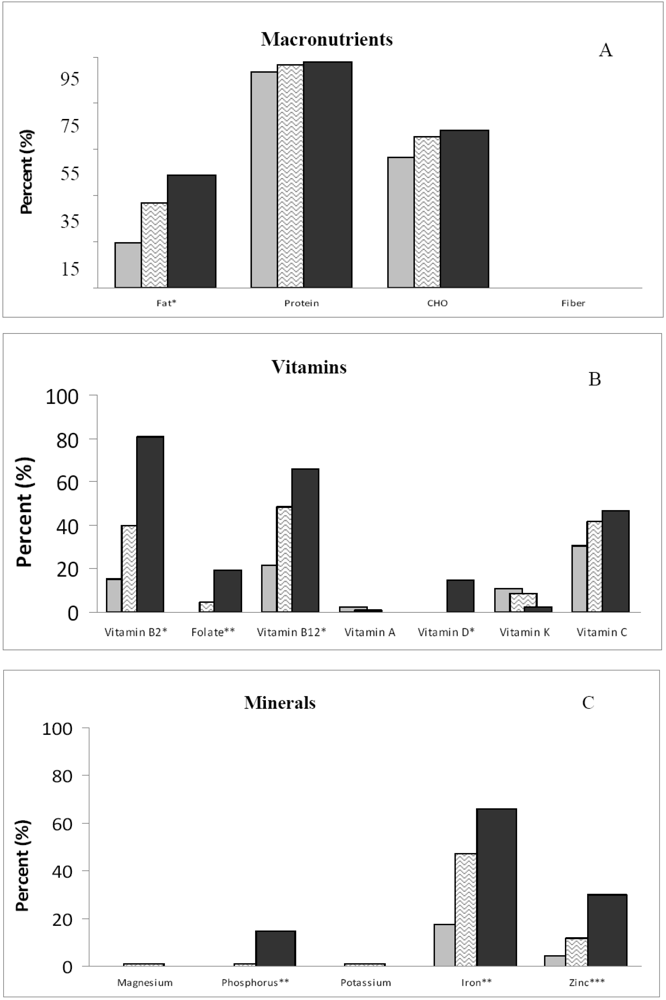
 ; middle (365–700 mg/d),
; middle (365–700 mg/d),  ; and high (>701 mg/d),
; and high (>701 mg/d),  ]. Significance for analysis of variance across groups adjusted for energy and gender: *p < 0.01; **p < 0.001; ***p < 0.0001.
; middle (365–700 mg/d), ; and high (>701 mg/d), ]. Significance for analysis of variance across groups adjusted for energy and gender: *p < 0.01; **p < 0.001; ***p < 0.0001.
]. Significance for analysis of variance across groups adjusted for energy and gender: *p < 0.01; **p < 0.001; ***p < 0.0001.
; middle (365–700 mg/d), ; and high (>701 mg/d), ]. Significance for analysis of variance across groups adjusted for energy and gender: *p < 0.01; **p < 0.001; ***p < 0.0001.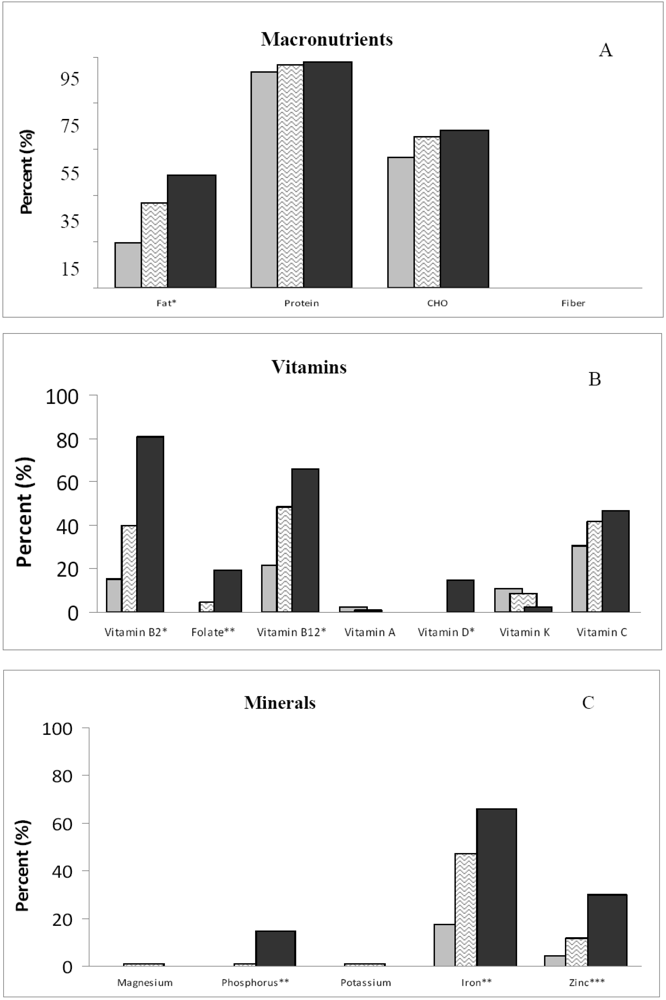
| Calcium-Intake Group | |||
|---|---|---|---|
| <365 mg/day (n = 46) | 365–700 mg/day (n = 93) | ≥701 mg/day (n = 48) | |
| Protein (g) | 64.0 ± 2.4 | 69.8 ± 1.6 | 70.3 ± 2.4 |
| Fat (g) | 76.7 ± 1.8 | 74.2 ± 1.2 | 72.1 ± 1.8 |
| Carbohydrates (g) | 215.6 ± 5.1 | 215.4 ± 3.4 | 221.2 ± 4.9 |
| Lactose (g) 3 | 0.6 ± 0.7 | 1.8 ± 0.5 | 4.6 ± 0.7 |
| Fiber, total dietary (g) 1 | 7.9 ± 0.6 | 9.9 ± 0.4 | 10.3 ± 0.6 |
| Riboflavin (mg) 2 | 0.6 ± 0.1 | 0.9 ± 0.0 | 1.5 ± 0.1 |
| Folate (µg) 2 | 102.1 ± 17.1 | 164.5 ± 11.4 | 239.3 ± 16.5 |
| Vitamin B12 (µg) | 2.1 ± 0.8 | 3.4 ± 0.5 | 4.2 ± 0.7 |
| Vit-A (mcg_RAE) 3 | 132.3 ± 34.2 | 186.9 ± 22.9 | 324.4 ± 33.0 |
| Vitamin D (IU) 2 | 7.9 ± 8.3 | 45.5 ± 5.5 | 108.3 ± 8.0 |
| Vitamin K (mcg) | 25.1 ± 6.0 | 20.2 ± 4.0 | 20.8 ± 5.7 |
| Vitamin E (mg) | 1.6 ± 0.3 | 1.5 ± 0.2 | 1.5 ± 0.3 |
| Vitamin C (mg) | 55.0 ± 7.1 | 59.7 ± 4.7 | 56.8 ± 6.8 |
| Magnesium (mg) 2 | 66.0 ± 8.8 | 99.7 ± 5.9 | 130.3 ± 8.5 |
| Phosphorus (mg) 2 | 378.7 ± 48.1 | 541.2 ± 32.2 | 867.9 ± 46.4 |
| Potassium (mg) 2 | 872.8 ± 98.7 | 1171.7 ± 66.0 | 1565.9 ± 95.2 |
| Iron (mg) 2 | 8.9 ± 0.8 | 11.2 ± 0.5 | 12.9 ± 0.7 |
| Zinc (mg) 2 | 3.3 ± 0.5 | 4.9 ± 0.3 | 7.2 ± 0.5 |
3.2. Discussion
4. Conclusions
Acknowledgments
References
- Centers for Disease Control and Prevention. Health, United States, 2003 with chartbook trends in the health of Americans. Available online: http://www.cdc.gov/nchs/data/hus/hus03.pdf (accessed on 11 June 2010).
- Ogden, C.L.; Flegal, K.M.; Carroll, M.D.; Johnson, C. Prevalence and trends in overweight among US children and adolescence, 1999–2000. JAMA 2002, 288, 1728–1732. [Google Scholar]
- Ogden, C.L.; Carroll, M.D.; Flegal, K.M. High body mass index for age among US children and adolescents, 2003–2006. JAMA 2008, 299, 2401–2405. [Google Scholar]
- Hill, J.O.; Trowbridge, F.L. Childhood obesity: Future direction and research priorities. Pediatrics 1998, 101, 570–574. [Google Scholar]
- Hedley, A.A.; Ogden, C.L.; Johnson, C.L.; Carroll, M.D.; Curtin, L.R.; Flegal, K.M. Prevalence of overweight and obesity in US children, adolescents, and adults, 1999–2000. JAMA 2004, 291, 2847–2850. [Google Scholar] [PubMed]
- Dwyer, J.T.; Stone, E.J.; Yang, M.; Webber, L.S.; Must, A.; Feldman, H.A.; Nader, P.R.; Perry, C.L.; Parcel, G.S. Prevalence of marked overweight and obesity in a multiethnic pediatric population: Findings from the Child and Adolescent Trial for Cardiovascular Health (CATCH) study. J. Am. Diet. Assoc. 2000, 100, 1149–1156. [Google Scholar]
- Troiano, R.P.; Flegal, K.M. Overweight children and adolescents: Description, epidemiology, and demographics. Pediatrics 1998, 101, 497–504. [Google Scholar] [PubMed]
- Styne, D.M. Childhood and adolescent obesity. Prevalence and significance. Pediatr. Clin. North Am. 2001, 48, 823–854. [Google Scholar] [CrossRef] [PubMed]
- Fulgoni, V., III; Nicholls, J.; Reed, A.; Buckley, R.; Kafer, K.; Huth, P.; DiRienzo, D.; Miller, G.D. Dairy consumption and related nutrient intake in African-American adults and children in the United States: Continuing survey of food intakes by individuals 1994–1996, 1998, and the National Health And Nutrition Examination Survey 1999–2000. J. Am. Diet. Assoc. 2007, 107, 256–264. [Google Scholar] [PubMed]
- Skinner, J.D.; Bounds, W.; Carruth, B.R.; Ziegler, P. Longitudinal calcium intake is negatively related to children’s body fat indexes. J. Am. Diet. Assoc. 2003, 103, 1626–1631. [Google Scholar]
- Novotny, R.; Daida, Y.G.; Acharya, S.; Grove, J.S.; Vogt, T.M. Dairy intake is associated with lower body fat and soda intake with greater weight in adolescent girls. J. Nutr. 2004, 134, 1905–1909. [Google Scholar]
- Davies, K.M.; Heaney, R.P.; Recker, R.R.; Lappe, J.M.; Barger-Lux, M.J.; Rafferty, K.; Hinders, S. Calcium intake and body weight. J. Clin. Endocrinol. Metab. 2000, 85, 4635–4638. [Google Scholar]
- Barr, S.I. Increased dairy product or calcium intake: Is body weight or composition affected in humans? J. Nutr. 2003, 133, 245S–248S. [Google Scholar]
- Velasquez-Mieyer, P.; Neira, C.P.; Nieto, R.; Cowan, P.A. Obesity and cardiometabolic syndrome in children. Ther. Adv. Cardiovasc. Dis. 2007, 1, 61–81. [Google Scholar]
- Ness, A.R.; Smith, G.D.; Hart, C. Milk, coronary heart disease and mortality. J. Epidemiol. Community Health 2001, 55, 379–382. [Google Scholar]
- Pittas, A.G.; Lau, J.; Hu, F.B.; Dawson-Hughes, B. The role of vitamin D and calcium in type 2 diabetes. A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2007, 92, 2017–2029. [Google Scholar] [CrossRef] [PubMed]
- Lindquist, C.H.; Gower, B.A.; Goran, M.I. Role of dietary factors in ethnic differences in early risk of cardiovascular disease and type 2 diabetes. Am. J. Clin. Nutr. 2000, 71, 725–732. [Google Scholar]
- Standing Committee on the Scientific Evaluation of Dietary Reference Intakes; Food and Nutrition Board; Institute of Medicine, Dietary Reference Intakes for Calcium, Phosphorous, Magnesium, Vitamin D and Fluoride; National Academies Press: Washington, DC, USA., 1997; p. 430.
- Panel on Dietary Antioxidants and Related Compounds; Subcommittees on Upper Reference Levels of Nutrients and Interpretation and Uses of Dietary Reference Intakes; Standing Committee on the Scientific Evaluation of Dietary Reference Intakes; Food and Nutrition Board; Institute of Medicine, Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; National Academies Press: Washington, DC, USA, 2000; p. 139.
- Panel on Micronutrients; Subcommittees on Upper Reference Levels of Nutrients and of Interpretation and Use of Dietary Reference Intakes; Standing Committee on the Scientific Evaluation of Dietary Reference Intakes; Food and Nutrition Board; Institute of Medicine, Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium and Zinc; National Academies Press: Washington, DC, USA, 2001; p. 113.
- Panel on Macronutrients; Subcommittees on Upper Reference Levels of Nutrients and of Interpretation and Uses of Dietary Reference Intakes; Standing Committee on the Scientific Evaluation of Dietary Reference Intakes; Food and Nutrition Board; Institute of Medicine, Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; National Academies Press: Washington, DC, USA, 2002; p. 936.
- Panel on Micronutrient; Subcommittees on Upper Reference Levels of Nutrients and of Interpretation and Uses of Dietary Reference Intakes; Standing Committee on the Scientific Evaluation of Dietary Reference Intakes; Food and Nutrition Board; Institute of Medicine, Dietary Reference Intakes for Water, Potassium, Sodium, Chloride and Sulfate; National Academies Press: Washington, DC, USA, 2005; pp. 71–145.
- National High Blood Pressure Education Program Working Group on Hypertension Control in Children and Adolescents. Update on the 1987 task force report on high blood pressure in children and adolescents: A working group report from the National High Blood Pressure Education Program. Pediatrics 1996, 98, 649–658. [PubMed]
- Falkner, B.; Daniels, S.R. Summary of the fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Hypertension 2004, 44, 387–388. [Google Scholar] [CrossRef] [PubMed]
- Kadish, A.H.; Little, R.H.; Sternberg, J.C. A new and rapid method for the determination of glucose by measurement of rate of oxygen consumption. Clin. Chem. 1968, 14, 116–119. [Google Scholar]
- Nicklas, T.A. Calcium intake trends and health consequences from childhood through adulthood. J. Am. Coll. Nutr. 2003, 22, 340–356. [Google Scholar]
- Berkey, C.S.; Rockett, H.R.; Willett, W.C.; Colditz, G.A. Milk, dairy fat, dietary calcium, and weight gain: A longitudinal study of adolescents. Arch. Pediatr. Adolesc. Med. 2005, 159, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Westerterp, K.R.; Goris, A.H. Validity of the assessment of dietary intake: Problems of misreporting. Curr. Opin. Clin. Nutr. Metab. Care 2002, 5, 489–493. [Google Scholar]
- Livingstone, M.B.; Robson, P.J.; Wallace, J.M. Issues in dietary intake assessment of children and adolescents. Br. J. Nutr. 2004, 92 (Suppl. 2), S213–S222. [Google Scholar] [PubMed]
- Kranz, S.; Lin, P.J.; Wagstaff, D.A. Children’s dairy intake in the United States: too little, too fat? J. Pediatr. 2007, 151, 642–646.e2. [Google Scholar] [CrossRef] [PubMed]
- Byers, K.G.; Savaiano, D.A. The myth of increased lactose intolerance in African-Americans. J. Am. Coll. Nutr. 2005, 24, 569S–573S. [Google Scholar]
- Marshall, T.A.; Eichenberger Gilmore, J.M.; Broffitt, B.; Stumbo, P.J.; Levy, S.M. Diet quality in young children is influenced by beverage consumption. J. Am. Coll. Nutr. 2005, 24, 65–75. [Google Scholar]
- Rafferty, K.; Davies, K.M.; Heaney, R.P. Potassium intake and the calcium economy. J. Am. Coll. Nutr. 2005, 24, 99–106. [Google Scholar]
- Murphy, M.M.; Douglass, J.S.; Johnson, R.K.; Spence, L.A. Drinking flavored or plain milk is positively associated with nutrient intake and is not associated with adverse effects on weight status in US children and adolescents. J. Am. Diet. Assoc. 2008, 108, 631–639. [Google Scholar]
- Ballew, C.; Kuester, S.; Gillespie, C. Beverage choices affect adequacy of children's nutrient intakes. Arch. Pediatr. Adolesc. Med. 2000, 154, 1148–1152. [Google Scholar]
- Hiza, H.A.B.; Bente, L.; Fungwe, T. Nutrient Content of the U.S. Food Supply, 2005; Home Economics Research Report No. 58; Center for Nutrition Policy and Promotion, U.S. Department of Agriculture: Washington, DC, USA, 2008. [Google Scholar]
- McGill, C.R.; Fulgoni, V.L., III; DiRienzo, D.; Huth, P.J.; Kurilich, A.C.; Miller, G.D. Contribution of dairy products to dietary potassium intake in the United States population. J. Am. Coll. Nutr. 2008, 27, 44–50. [Google Scholar] [PubMed]
- Karanja, N.; Morris, C.D.; Rufolo, P.; Snyder, G.; Illingworth, D.R.; McCarron, D.A. Impact of increasing calcium in the diet on nutrient consumption, plasma lipids, and lipoproteins in humans. Am. J. Clin. Nutr. 1994, 59, 900–907. [Google Scholar] [PubMed]
- Barlow, S.E. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics 2007, 120 (Suppl. 4), S164–S192. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.; Auinger, P.; Li, C.; Ford, E.S. Metabolic syndrome rates in United States adolescents, from the National Health and Nutrition Examination Survey, 1999–2002. J. Pediatr. 2008, 152, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Bacha, F.; Gungor, N.; Arslanian, S. Comparison of different definitions of pediatric metabolic syndrome: Relation to abdominal adiposity, insulin resistance, adiponectin, and inflammatory biomarkers. J. Pediatr. 2008, 152, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Ostchega, Y.; Carroll, M.; Prineas, R.J.; McDowell, M.A.; Louis, T.; Tilert, T. Trends of elevated blood pressure among children and adolescents: Data from the National Health and Nutrition Examination Survey 1988–2006. Am. J. Hypertens. 2009, 22, 59–67. [Google Scholar]
- Pereira, M.A.; Jacobs, D.R., Jr.; van Horn, L.; Slattery, M.L.; Kartashov, A.I.; Ludwig, D.S. Dairy consumption, obesity, and the insulin resistance syndrome in young adults: The CARDIA Stuty. JAMA 2002, 287, 2081–2089. [Google Scholar] [PubMed]
- Guo, S.S.; Roche, A.F.; Chumlea, W.C.; Gardner, J.D.; Siervogel, R.M. The predictive value of childhood body mass index values for overweight at age 35 y. Am. J. Clin. Nutr. 1994, 59, 810–819. [Google Scholar] [PubMed]
- Major, G.C.; Alarie, F.; Dore, J.; Phouttama, S.; Tremblay, A. Supplementation with calcium + vitamin D enhances the beneficial effect of weight loss on plasma lipid and lipoprotein concentrations. Am. J. Clin. Nutr. 2007, 85, 54–59. [Google Scholar]
- Houston, M.C.; Harper, K.J. Potassium, magnesium, and calcium: Their role in both the cause and treatment of hypertension. J. Clin. Hypertens. (Greenwich) 2008, 10, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Bell, N.; Greene, A.; Epstein, S.; Oexmann, M.; Shaw, S.; Shary, J. Evidence for alteration of the vitamin D-endrocrine system in blacks. J. Clin. Invest. 1985, 76, 470–473. [Google Scholar]
- Bell, N.H.; Yergery, A.L.; Vieiri, N.E.; Oexmann, M.J.; Shary, J.R. Demonstration of a difference in urinary calcium, not calcium absorption, in black and white adolescents. J. Bone Miner. Res. 1993, 8, 1111–1115. [Google Scholar] [PubMed]
- Bell, N.H.; Shary, J.; Stevens, J.; Garza, M.; Gordon, L.; Edwards, J. Demonstration that bone mass is greater in black than in white children. J. Bone Miner. Res. 1991, 6, 719–723. [Google Scholar]
- Pihoker, C.; Scott, C.R.; Lensing, S.Y.; Cradock, M.M.; Smith, J. Non-insulin dependent diabetes mellitus in African-American youths of Arkansas. Clin. Pediatr. (Phila) 1998, 37, 97–102. [Google Scholar] [PubMed]
- Pinhas-Hamiel, O.; Dolan, L.M.; Zeitler, P.S. Diabetic ketoacidosis among obese African-American adolescents with NIDDM. Diabetes Care 1997, 20, 484–486. [Google Scholar]
- Scott, C.R.; Smith, J.M.; Cradock, M.M.; Pihoker, C. Characteristics of youth-onset noninsulin-dependent diabetes mellitus and insulin-dependent diabetes mellitus at diagnosis. Pediatrics 1997, 100, 84–91. [Google Scholar]
© 2010 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Tylavsky, F.A.; Cowan, P.A.; Terrell, S.; Hutson, M.; Velasquez-Mieyer, P. Calcium Intake and Body Composition in African-American Children and Adolescents at Risk for Overweight and Obesity. Nutrients 2010, 2, 950-964. https://doi.org/10.3390/nu2090950
Tylavsky FA, Cowan PA, Terrell S, Hutson M, Velasquez-Mieyer P. Calcium Intake and Body Composition in African-American Children and Adolescents at Risk for Overweight and Obesity. Nutrients. 2010; 2(9):950-964. https://doi.org/10.3390/nu2090950
Chicago/Turabian StyleTylavsky, Frances A., Patricia A. Cowan, Sarah Terrell, Merschon Hutson, and Pedro Velasquez-Mieyer. 2010. "Calcium Intake and Body Composition in African-American Children and Adolescents at Risk for Overweight and Obesity" Nutrients 2, no. 9: 950-964. https://doi.org/10.3390/nu2090950