The Impact of Movement Behaviors on Bone Health in Elderly with Adequate Nutritional Status: Compositional Data Analysis Depending on the Frailty Status

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample and Design
2.2. Anthropometrics and Bone Health and Body Composition
2.3. Physical Activity and Sedentary Behaviors
2.4. Frailty Status
2.5. Data Analysis
3. Results
3.1. Descriptive
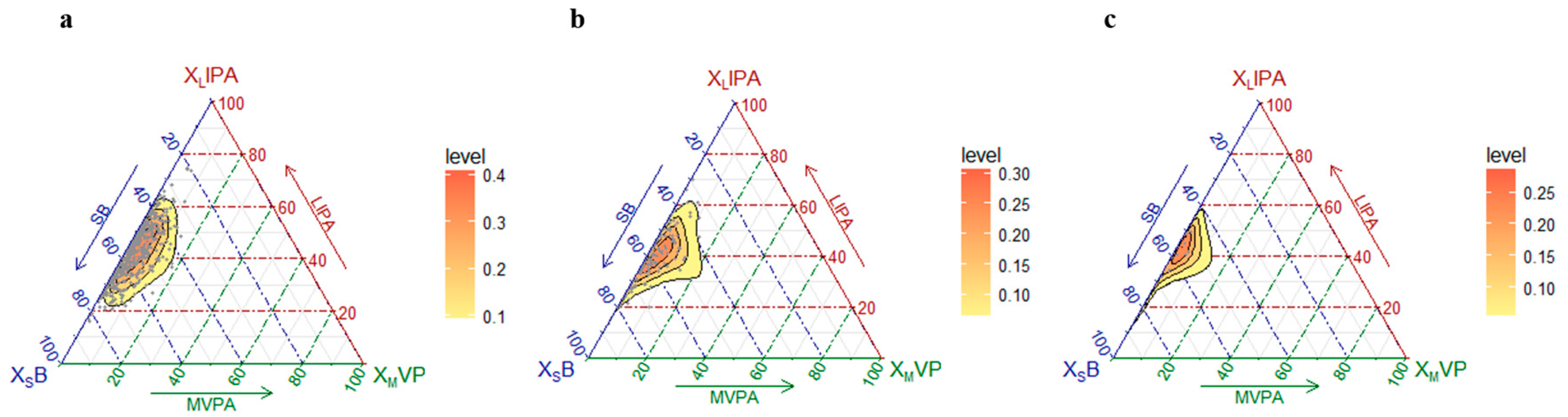
3.2. Movement Patterns According to Frailty Status and Sex: Composition of the Day
3.3. Compositional Data
3.4. Men
3.5. Women
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Yedavally-Yellayi, S.; Ho, A.M.; Patalinghug, E.M. Update on Osteoporosis. Prim. Care Clin. Office Pract. 2019, 46, 175–190. [Google Scholar] [CrossRef] [PubMed]
- Cauley, J.A. Public health impact of osteoporosis. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013, 68, 1243–1251. [Google Scholar] [CrossRef] [PubMed]
- Yoneki, K.; Kitagawa, J.; Hoshi, K.; Harada, M.; Watanabe, T.; Shimoda, T.; Matsuzawa, R.; Yoshida, A.; Matsunaga, Y.; Takeuchi, Y. Association between frailty and bone loss in patients undergoing maintenance hemodialysis. J. Bone Miner. Metab 2018, 37, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.H.; Chang, S.F. Frailty as a Risk Factor for Falls Among Community Dwelling People: Evidence from a Meta-Analysis. J. Nurs. Scholarsh. 2017, 49, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Mañas, A.; del Pozo-Cruz, B.; García-García, F.J.; Guadalupe-Grau, A.; Ara, I. Role of objectively measured sedentary behaviour in physical performance, frailty and mortality among older adults: A short systematic review. Eur. J. Sport Sci. 2017, 17, 940–953. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; McBurnie, M.A. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Rolland, Y.; Van Kan, G.A.; Benetos, A.; Blain, H.; Bonnefoy, M.; Chassagne, P.; Jeandel, C.; Laroche, M.; Nourhashemi, F.; Orcel, P. Frailty, osteoporosis and hip fracture: Causes, consequences and therapeutic perspectives. J. Nutr. Health Aging 2008, 12, a319–a330. [Google Scholar] [CrossRef]
- Chang, Y.-F.; Chang, C.-S.; Wang, M.-W.; Wu, C.-F.; Chen, C.-Y.; Chang, H.-J.; Kuo, P.-H.; Wu, C.-H. Effects of Age and Body Mass Index on Thoracolumbar Spine X-Ray for Diagnosing Osteoporosis in Elderly Women: Tianliao Old People (TOP) Study 07. PLoS ONE 2016, 11, e0161773. [Google Scholar] [CrossRef]
- Cook, M.J.; Oldroyd, A.; Pye, S.R.; Ward, K.A.; Gielen, E.; Ravindrarajah, R.; Adams, J.E.; Lee, D.M.; Bartfai, G.; Boonen, S. Frailty and bone health in European men. Age Ageing 2016, 46, 635–641. [Google Scholar] [CrossRef] [Green Version]
- Kojima, G. Frailty as a predictor of disabilities among community-dwelling older people: A systematic review and meta-analysis. Disabil. Rehabil. 2017, 39, 1897–1908. [Google Scholar] [CrossRef]
- Álvarez-Sánchez, N.; Álvarez-Ríos, A.I.; Guerrero, J.M.; García-García, F.J.; Rodríguez-Mañas, L.; Cruz-Chamorro, I.; Lardone, P.J.; Carrillo-Vico, A. Homocysteine levels are associated with bone resorption in pre-frail and frail Spanish women: The Toledo Study for Healthy Aging. Exp. Gerontol. 2018, 108, 201–208. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M. Sarcopenia: European consensus on definition and diagnosis. Report of the European Working Group on Sarcopenia in Older People A. J. Cruz-Gentoft et al. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.; Jackson, T.; Sapey, E.; Lord, J.M. Frailty and sarcopenia: The potential role of an aged immune system. Ageing Res. Rev. 2017, 36, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Morseth, B.; Emaus, N.; Jørgensen, L. Physical activity and bone: The importance of the various mechanical stimuli for bone mineral density. A review. Nor. Epidemiol. 2011, 20, 173–178. [Google Scholar] [CrossRef]
- Rizzoli, R.; Branco, J.; Brandi, M.-L.; Boonen, S.; Bruyère, O.; Cacoub, P.; Cooper, C.; Diez-Perez, A.; Duder, J.; Fielding, R. Management of osteoporosis of the oldest old. Osteoporos. Int. 2014, 25, 2507–2529. [Google Scholar] [CrossRef] [PubMed]
- Tarantino, U.; Iolascon, G.; Cianferotti, L.; Masi, L.; Marcucci, G.; Giusti, F.; Marini, F.; Parri, S.; Feola, M.; Rao, C. Clinical guidelines for the prevention and treatment of osteoporosis: Summary statements and recommendations from the Italian Society for Orthopaedics and Traumatology. J. Orthop. Traumatol. 2017, 18, 3. [Google Scholar] [CrossRef]
- Klibanski, A.; Adams-Campbell, L.; Bassford, T.; Blair, S.N.; Boden, S.D.; Dickersin, K.; Gifford, D.R.; Glasse, L.; Goldring, S.R.; Hruska, K. Osteoporosis prevention, diagnosis, and therapy. J. Am. Med Assoc. 2001, 285, 785–795. [Google Scholar]
- Beck, B.R.; Daly, R.M.; Singh, M.A.F.; Taaffe, D.R. Exercise and Sports Science Australia (ESSA) position statement on exercise prescription for the prevention and management of osteoporosis. J. Sci. Med. Sport 2017, 20, 438–445. [Google Scholar] [CrossRef]
- Del Pozo-Cruz, B.; Mañas, A.; Martín-García, M.; Marín-Puyalto, J.; García-García, F.J.; Rodriguez-Mañas, L.; Guadalupe-Grau, A.; Ara, I. Frailty is associated with objectively assessed sedentary behaviour patterns in older adults: Evidence from the Toledo Study for Healthy Aging (TSHA). PLoS ONE 2017, 12, e0183911. [Google Scholar] [CrossRef]
- Chastin, S.F.; Palarea-Albaladejo, J.; Dontje, M.L.; Skelton, D.A. Combined effects of time spent in physical activity, sedentary behaviors and sleep on obesity and cardio-metabolic health markers: A novel compositional data analysis approach. PLoS ONE 2015, 10, e0139984. [Google Scholar] [CrossRef]
- Garcia-Garcia, F.J.; Avila, G.G.; Alfaro-Acha, A.; Andres, M.A.; Aparicio, M.E.; Aparicio, S.H.; Zugasti, J.L.; Reus, M.G.-S.; Rodriguez-Artalejo, F.; Rodriguez-Manas, L. The prevalence of frailty syndrome in an older population from Spain. The Toledo Study for Healthy Aging. J. Nutr. Health Aging 2011, 15, 852–856. [Google Scholar] [CrossRef] [PubMed]
- Garry, P.J.; Vellas, B.J. Practical and validated use of the Mini Nutritional Assessment in geriatric evaluation. Nutr. Clin. Care 1999, 2, 146–154. [Google Scholar] [CrossRef]
- Delmonico, M.J.; Harris, T.B.; Lee, J.S.; Visser, M.; Nevitt, M.; Kritchevsky, S.B.; Tylavsky, F.A.; Newman, A.B. Alternative definitions of sarcopenia, lower extremity performance, and functional impairment with aging in older men and women. J. Am. Geriatr. Soc. 2007, 55, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Mañas, A.; del Pozo-Cruz, B.; Guadalupe-Grau, A.; Marín-Puyalto, J.; Alfaro-Acha, A.; Rodríguez-Mañas, L.; García-García, F.J.; Ara, I. Reallocating Accelerometer-Assessed Sedentary Time to Light or Moderate-to Vigorous-Intensity Physical Activity Reduces Frailty Levels in Older Adults: An Isotemporal Substitution Approach in the TSHA Study. J. Am. Med. Direct. Assoc. 2017, 19, 185. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Gómez, I.; Mañas, A.; Losa-Reyna, J.; Rodríguez-Mañas, L.; Chastin, S.F.; Alegre, L.M.; García-García, F.J.; Ara, I. Associations between sedentary time, physical activity and bone health among older people using compositional data analysis. PLoS ONE 2018, 13, e0206013. [Google Scholar] [CrossRef]
- Colley, R.; Connor Gorber, S.; Tremblay, M.S. Quality control and data reduction procedures for accelerometry-derived measures of physical activity. Health Rep. 2010, 21, 63–69. [Google Scholar] [PubMed]
- Aguilar-Farías, N.; Brown, W.J.; Peeters, G.G. ActiGraph GT3X+ cut-points for identifying sedentary behaviour in older adults in free-living environments. J. Sci. Med. Sport 2014, 17, 293–299. [Google Scholar] [CrossRef]
- Santos-Lozano, A.; Santin-Medeiros, F.; Cardon, G.; Torres-Luque, G.; Bailon, R.; Bergmeir, C.; Ruiz, J.R.; Lucia, A.; Garatachea, N. Actigraph GT3X: Validation and determination of physical activity intensity cut points. Int J. Sports Med. 2013, 34, 975–982. [Google Scholar] [CrossRef]
- Sterne, J.A.; Smith, G.D. Sifting the evidence—What’s wrong with significance tests? Phys. Ther. 2001, 81, 1464–1469. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.J.; Giuliani, C.; Morey, M.C.; Pieper, C.F.; Evenson, K.R.; Mercer, V.; Cohen, H.J.; Visser, M.; Brach, J.S.; Kritchevsky, S.B. Physical activity as a preventative factor for frailty: The health, aging, and body composition study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2009, 64, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Bebenek, M.; Kohl, M.; von Stengel, S. Exercise and fractures in postmenopausal women. Final results of the controlled Erlangen Fitness and Osteoporosis Prevention Study (EFOPS). Osteoporos. Int. 2015, 26, 2491–2499. [Google Scholar] [CrossRef] [PubMed]
- Braun, S.I.; Kim, Y.; Jetton, A.E.; Kang, M.; Morgan, D.W. Sedentary Behavior, Physical Activity, and Bone Health in Postmenopausal Women. J. Aging Phys. Act. 2017, 25, 173–181. [Google Scholar] [CrossRef] [PubMed]
- McMillan, L.; Aitken, D.; Ebeling, P.; Jones, G.; Scott, D. The relationship between objectively assessed physical activity and bone health in older adults differs by sex and is mediated by lean mass. Osteoporos. Int. 2018, 29, 1379–1388. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.; Mandrichenko, O.; Helbostadt, J.; Skelton, D.A. Associations between objectively-measured sedentary behaviour and physical activity with bone mineral density in adults and older adults, the NHANES study. Bone 2014, 64, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Langsetmo, L.; Hitchcock, C.; Kingwell, E.; Davison, K.; Berger, C.; Forsmo, S.; Zhou, W.; Kreiger, N.; Prior, J. Physical activity, body mass index and bone mineral density—Associations in a prospective population-based cohort of women and men: The Canadian Multicentre Osteoporosis Study (CaMos). Bone 2012, 50, 401–408. [Google Scholar] [CrossRef] [PubMed]
- McMillan, L.B.; Zengin, A.; Ebeling, P.R.; Scott, D. Prescribing Physical Activity for the Prevention and Treatment of Osteoporosis in Older Adults. Healthcare 2017, 5, 85. [Google Scholar] [CrossRef] [PubMed]
- Beck, T.J.; Kohlmeier, L.A.; Petit, M.A.; Wu, G.; Leboff, M.S.; Cauley, J.A.; Nicholas, S.; Chen, Z. Confounders in the association between exercise and femur bone in postmenopausal women. Med. Sci. Sports Exerc. 2011, 43, 80–89. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Garrido, J.; Ruiz-Ros, V.; Buigues, C.; Navarro-Martinez, R.; Cauli, O. Clinical features of prefrail older individuals and emerging peripheral biomarkers: A systematic review. Arch. Gerontol. Geriatr. 2014, 59, 7–17. [Google Scholar] [CrossRef]
- Gill, T.M.; Gahbauer, E.A.; Allore, H.G.; Han, L. Transitions between frailty states among community-living older persons. Arch. Intern. Med. 2006, 166, 418–423. [Google Scholar] [CrossRef]
- St-Jean-Pelletier, F.; Pion, C.H.; Leduc-Gaudet, J.P.; Sgarioto, N.; Zovilé, I.; Barbat-Artigas, S.; Reynaud, O.; Alkaterji, F.; Lemieux, F.C.; Grenon, A. The impact of ageing, physical activity, and pre-frailty on skeletal muscle phenotype, mitochondrial content, and intramyocellular lipids in men. J. Cachexiasarcopenia Muscle 2017, 8, 213–228. [Google Scholar] [CrossRef] [PubMed]
- Wetzsteon, R.J.; Zemel, B.S.; Shults, J.; Howard, K.M.; Kibe, L.W.; Leonard, M.B. Mechanical loads and cortical bone geometry in healthy children and young adults. Bone 2011, 48, 1103–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gajic-Veljanoski, O.; Papaioannou, A.; Kennedy, C.; Ioannidis, G.; Berger, C.; Wong, A.K.O.; Rockwood, K.; Kirkland, S.; Raina, P.; Thabane, L. Osteoporotic fractures and obesity affect frailty progression: A longitudinal analysis of the Canadian multicentre osteoporosis study. BMC Geriatr. 2018, 18, 4. [Google Scholar] [CrossRef] [PubMed]
- Dawson, A.; Dennison, E. Measuring the musculoskeletal aging phenotype. Maturitas 2016, 93, 13–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serra-Prat, M.; Sist, X.; Saiz, A.; Jurado, L.; Domenich, R.; Roces, A.; Papiol, M. Clinical and functional characterization of pre-frailty among elderly patients consulting primary care centres. J. Nutr. Health Aging 2016, 20, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Jansen, F.M.; Prins, R.G.; Etman, A.; van der Ploeg, H.P.; De Vries, S.I.; van Lenthe, F.J.; Pierik, F.H. Physical activity in non-frail and frail older adults. PLoS ONE 2015, 10, e0123168. [Google Scholar] [CrossRef] [PubMed]
- Carson, V.; Tremblay, M.S.; Chaput, J.-P.; Chastin, S.F. Associations between sleep duration, sedentary time, physical activity, and health indicators among Canadian children and youth using compositional analyses 1. Appl. Physiol. Nutr. Metab. 2016, 41, S294–S302. [Google Scholar] [CrossRef]
- Rodríguez-Gómez, I.; Mañas, A.; Losa-Reyna, J.; Rodríguez-Mañas, L.; Chastin, S.F.; Alegre, L.M.; García-García, F.J.; Ara, I. Compositional Influence of Movement Behaviours on Bone Health during Ageing. Med. Sci. Sports Exerc. 2019. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Whole Sample (n = 740) | Robust (n = 540) | Pre-frailty (n = 180) | Frailty (n = 20) |
|---|---|---|---|---|
| Sex (%) | ||||
| Men | 46.6 | 46.5 | 47.2 | 45.0 |
| Women | 53.4 | 53.5 | 52.8 | 55.0 |
| Age (years) | 76.8 ± 4.9 | 76.0 ± 4.4 | 78.6 ± 5.5 ☨ | 80.1 ± 5.1 * |
| Body mass (kg) | 73.6 ± 12.8 | 73.3 ± 12.5 | 74.8 ± 13.5 | 72.3 ± 13.8 |
| Height (cm) | 155.9 ± 9.0 | 156.3 ± 8.9 | 155.1 ± 9.3 | 154.4 ± 10.0 |
| BMI (kg/m2) | 30.3 ± 4.8 | 30.0 ± 4.7 | 31.1 ± 4.9 ☨ | 30.5 ± 5.8 |
| %Body fat | 36.6 ± 7.7 | 36.3 ± 7.7 | 37.5 ± 7.7 | 36.4 ± 8.5 |
| Sarcopenia (%) | 33.5 | 37.6 | 21.3 | 35.0 |
| Bone health (%) | ||||
| Normal bone health | 32.3 | 34.6 | 25.8 | 30 |
| Osteopenia | 55.1 | 54.9 | 55.6 | 55 |
| Osteoporosis | 12.6 | 10.5 | 18.6 | 15 |
| Highest household educational (%) | ||||
| Less than primary school graduation | 62.3 | 59.3 | 68.9 | 85.0 |
| Primary school graduation | 22.4 | 23.9 | 18.9 | 15.0 |
| Secondary school graduation or more | 14.6 | 16.1 | 11.7 | 0.0 |
| Marital status (%) | ||||
| Single | 5.5 | 5.6 | 5.6 | 5.0 |
| Married | 70.4 | 72.2 | 67.8 | 45.0 |
| Widower | 21.9 | 19.7 | 25.6 | 50.0 |
| Separated/Divorced | 1.6 | 2.0 | 0.6 | 0.0 |
| a. | |||||||
| OUTCOME | MODEL p-VALUE | γ SB | p-VALUE | γ LPA | p-VALUE | γ MVPA | p-VALUE |
| BMC VALUES | |||||||
| Whole body | 0.742 | 12.497 | 0.441 | −11.938 | 0.495 | −0.559 | 0.949 |
| Arms (mean) | 0.200 | −1.961 | 0.112 | 2.391 | 0.073 | −0.429 | 0.517 |
| Legs (mean) | 0.010 | 9.776 | 0.003 | −10.420 | 0.004 | 0.643 | 0.717 |
| Lumbar (mean L1–L4) | 0.775 | −0.107 | 0.582 | 0.148 | 0.482 | −0.041 | 0.698 |
| Femoral neck | 0.732 | −0.048 | 0.461 | 0.055 | 0.435 | −0.007 | 0.846 |
| BMD VALUES | |||||||
| Whole body | 0.220 | 0.010 | 0.114 | −0.012 | 0.083 | 0.002 | 0.589 |
| Arms (mean) | 0.527 | −0.004 | 0.275 | 0.005 | 0.273 | 0.000 | 0.863 |
| Legs (mean) | 0.000 | 0.035 | 0.000 | −0.037 | 0.000 | 0.003 | 0.464 |
| Lumbar (mean L1–L4) | 0.749 | −0.004 | 0.664 | 0.007 | 0.492 | −0.003 | 0.569 |
| Femoral neck | 0.628 | −0.007 | 0.336 | 0.007 | 0.386 | 0.000 | 0.957 |
| b. | |||||||
| OUTCOME | MODEL p-VALUE | γ SB | p-VALUE | γ LPA | p-VALUE | γ MVPA | p-VALUE |
| BMC VALUES | |||||||
| Whole body | 0.041 | −1.032 | 0.981 | −36.195 | 0.452 | 37.228 | 0.014 |
| Arms (mean) | 0.215 | −5.147 | 0.160 | 4.216 | 0.297 | 0.931 | 0.434 |
| Legs (mean) | 0.011 | 2.717 | 0.686 | −9.971 | 0.191 | 7.253 | 0.003 |
| Lumbar (mean L1–L4) | 0.794 | 0.125 | 0.827 | −0.242 | 0.698 | 0.118 | 0.504 |
| Femoral neck | 0.136 | 0.078 | 0.602 | −0.170 | 0.298 | 0.092 | 0.047 |
| BMD VALUES | |||||||
| Whole body | 0.033 | 0.006 | 0.704 | −0.02 | 0.250 | 0.014 | 0.009 |
| Arms (mean) | 0.872 | −0.003 | 0.747 | 0.002 | 0.846 | 0.001 | 0.726 |
| Legs (mean) | 0.054 | 0.006 | 0.659 | −0.019 | 0.248 | 0.013 | 0.016 |
| Lumbar (mean L1–L4) | 0.495 | 0.001 | 0.975 | −0.011 | 0.719 | 0.011 | 0.241 |
| Femoral neck | 0.233 | 0.003 | 0.902 | −0.014 | 0.557 | 0.011 | 0.090 |
| a. | |||||||
| OUTCOME | MODEL p-VALUE | γ SB | p-VALUE | γ LPA | p-VALUE | γ MVPA | p-VALUE |
| BMC VALUES | |||||||
| Whole body | 0.211 | −34.310 | 0.101 | 17.100 | 0.491 | 17.210 | 0.340 |
| Arms (mean) | 0.357 | −2.260 | 0.155 | 1.665 | 0.369 | 0.595 | 0.650 |
| Legs (mean) | 0.054 | −8.067 | 0.047 | 2.235 | 0.638 | 5.832 | 0.087 |
| Lumbar (mean L1–L4) | 0.245 | −0.439 | 0.094 | 0.328 | 0.282 | 0.111 | 0.617 |
| Femoral neck | 0.987 | −0.004 | 0.957 | −0.007 | 0.945 | 0.011 | 0.874 |
| BMD VALUES | |||||||
| Whole body | 0.043 | −0.015 | 0.041 | 0.003 | 0.707 | 0.012 | 0.064 |
| Arms (mean) | 0.361 | −0.006 | 0.188 | 0.003 | 0.571 | 0.003 | 0.425 |
| Legs (mean) | 0.046 | −0.018 | 0.036 | 0.006 | 0.580 | 0.012 | 0.084 |
| Lumbar (mean L1–L4) | 0.326 | −0.019 | 0.136 | 0.017 | 0.255 | 0.002 | 0.845 |
| Femoral neck | 0.210 | −0.016 | 0.078 | 0.012 | 0.241 | 0.004 | 0.638 |
| b. | |||||||
| OUTCOME | MODEL p-VALUE | γ SB | p-VALUE | γ LPA | p-VALUE | γ MVPA | p-VALUE |
| BMC VALUES | |||||||
| Whole body | 0.160 | −124.35 | 0.182 | 91.65 | 0.401 | 32.700 | 0.362 |
| Arms (mean) | 0.467 | −3.269 | 0.574 | 1.672 | 0.795 | 1.597 | 0.353 |
| Legs (mean) | 0.420 | 7.805 | 0.518 | −13.947 | 0.335 | 6.142 | 0.194 |
| Lumbar (mean L1–L4) | 0.689 | −0.599 | 0.528 | 0.476 | 0.654 | 0.123 | 0.679 |
| Femoral neck | 0.348 | −0.061 | 0.801 | −0.041 | 0.880 | 0.103 | 0.191 |
| BMD VALUES | |||||||
| Whole body | 0.246 | −0.027 | 0.275 | 0.019 | 0.522 | 0.008 | 0.378 |
| Arms (mean) | 0.980 | −0.003 | 0.868 | 0.003 | 0.897 | 0.000 | 0.955 |
| Legs (mean) | 0.712 | 0.000 | 0.990 | −0.007 | 0.804 | 0.007 | 0.450 |
| Lumbar (mean L1–L4) | 0.173 | −0.035 | 0.394 | 0.017 | 0.714 | 0.018 | 0.157 |
| Femoral neck | 0.233 | −0.011 | 0.743 | −0.005 | 0.886 | 0.016 | 0.128 |
| a. | |||||||
| OUTCOME | MODEL p-VALUE | γ SB | p-VALUE | γ LPA | p-VALUE | γ MVPA | p-VALUE |
| BMC VALUES | |||||||
| Whole body | 0.033 | 36.761 | 0.020 | −25.831 | 0.158 | −10.93 | 0.235 |
| Arms (mean) | 0.015 | −1.749 | 0.154 | 3.705 | 0.011 | −1.954 | 0.011 |
| Legs (mean) | 0.000 | 19.032 | 0.000 | −17.361 | 0.000 | −1.672 | 0.371 |
| Lumbar (mean L1–L4) | 0.205 | 0.220 | 0.218 | −0.080 | 0.680 | −0.140 | 0.156 |
| Femoral neck | 0.692 | −0.046 | 0.500 | 0.062 | 0.395 | −0.017 | 0.661 |
| BMD VALUES | |||||||
| Whole body | 0.008 | 0.020 | 0.003 | −0.018 | 0.024 | −0.003 | 0.494 |
| Arms (mean) | 0.209 | −0.006 | 0.147 | 0.009 | 0.078 | −0.003 | 0.295 |
| Legs (mean) | 0.000 | 0.066 | 0.000 | −0.063 | 0.000 | −0.002 | 0.648 |
| Lumbar (mean L1–L4) | 0.343 | 0.011 | 0.309 | −0.004 | 0.728 | −0.007 | 0.246 |
| Femoral neck | 0.292 | 0.0025 | 0.787 | 0.005 | 0.583 | −0.007 | 0.117 |
| b. | |||||||
| OUTCOME | MODEL p-VALUE | γ SB | p-VALUE | γ LPA | p-VALUE | γ MVPA | p-VALUE |
| BMC VALUES | |||||||
| Whole body | 0.097 | 38.45 | 0.546 | −79.000 | 0.260 | 40.55 | 0.032 |
| Arms (mean) | 0.192 | −4.518 | 0.230 | 3.387 | 0.403 | 1.131 | 0.254 |
| Legs (mean) | 0.144 | 7.047 | 0.446 | −12.592 | 0.219 | 5.545 | 0.054 |
| Lumbar (mean L1–L4) | 0.714 | 0.291 | 0.655 | −0.188 | 0.788 | −0.17 | 0.546 |
| Femoral neck | 0.546 | 0.030 | 0.873 | −0.080 | 0.688 | 0.050 | 0.273 |
| BMD VALUES | |||||||
| Whole body | 0.132 | 0.027 | 0.286 | −0.041 | 0.140 | 0.014 | 0.050 |
| Arms (mean) | 0.550 | −0.007 | 0.614 | 0.004 | 0.799 | 0.003 | 0.386 |
| Legs (mean) | 0.151 | 0.026 | 0.249 | −0.038 | 0.125 | 0.012 | 0.078 |
| Lumbar (mean L1–L4) | 0.844 | 0.013 | 0.748 | −0.009 | 0.845 | −0.005 | 0.671 |
| Femoral neck | 0.222 | 0.011 | 0.681 | −0.022 | 0.427 | 0.011 | 0.084 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Gómez, I.; Mañas, A.; Losa-Reyna, J.; Rodríguez-Mañas, L.; Chastin, S.F.M.; Alegre, L.M.; García-García, F.J.; Ara, I. The Impact of Movement Behaviors on Bone Health in Elderly with Adequate Nutritional Status: Compositional Data Analysis Depending on the Frailty Status. Nutrients 2019, 11, 582. https://doi.org/10.3390/nu11030582
Rodríguez-Gómez I, Mañas A, Losa-Reyna J, Rodríguez-Mañas L, Chastin SFM, Alegre LM, García-García FJ, Ara I. The Impact of Movement Behaviors on Bone Health in Elderly with Adequate Nutritional Status: Compositional Data Analysis Depending on the Frailty Status. Nutrients. 2019; 11(3):582. https://doi.org/10.3390/nu11030582
Chicago/Turabian StyleRodríguez-Gómez, Irene, Asier Mañas, José Losa-Reyna, Leocadio Rodríguez-Mañas, Sebastien F.M. Chastin, Luis M. Alegre, Francisco J. García-García, and Ignacio Ara. 2019. "The Impact of Movement Behaviors on Bone Health in Elderly with Adequate Nutritional Status: Compositional Data Analysis Depending on the Frailty Status" Nutrients 11, no. 3: 582. https://doi.org/10.3390/nu11030582