Co-Ingestion of Rice Bran Soymilk or Plain Soymilk with White Bread: Effects on the Glycemic and Insulinemic Response

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Protocol
2.3. Glycemic Index Methodology
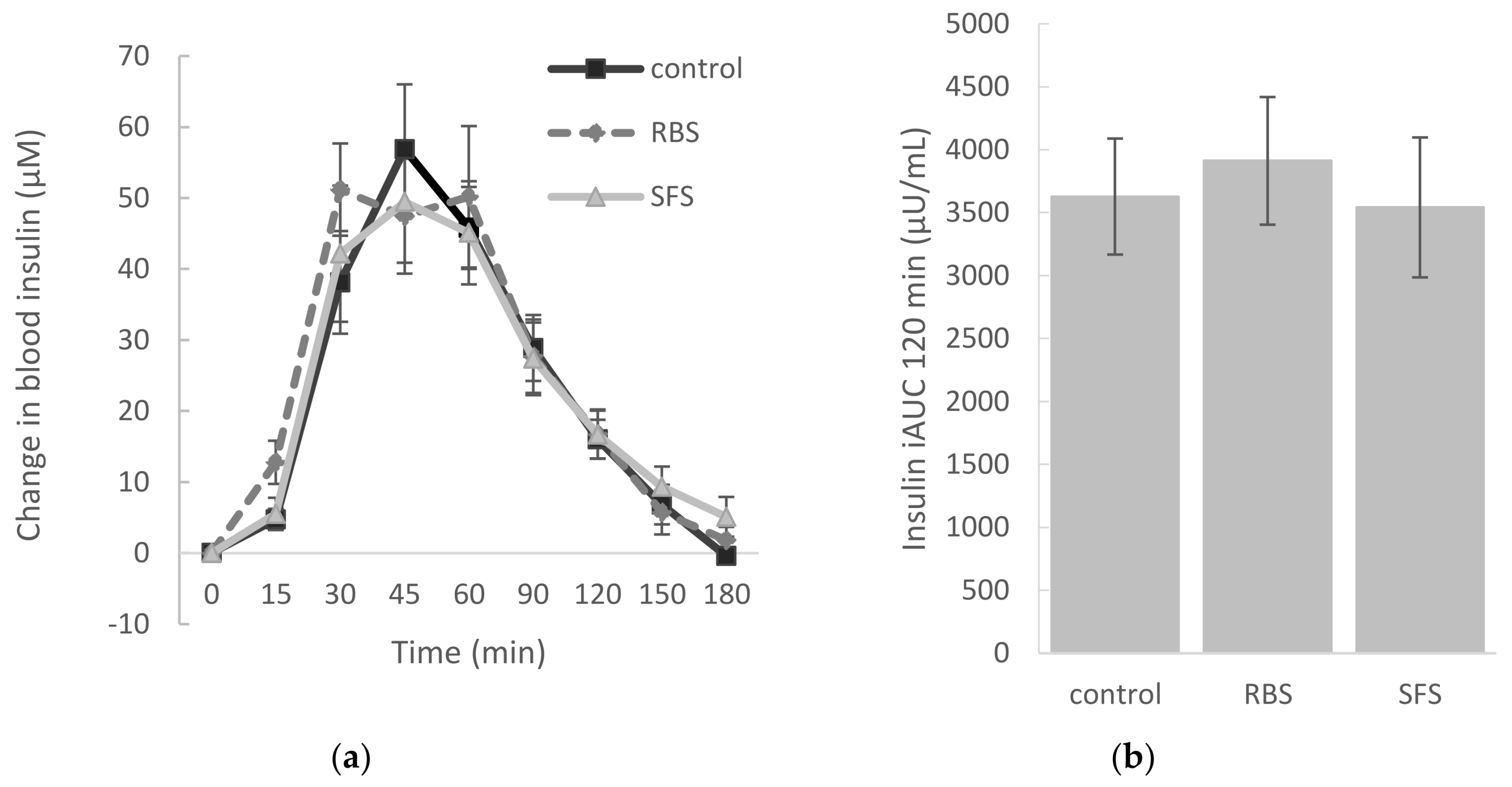
2.4. Insulinemic Index Methodology
2.5. Treatment Meals
- white bread (control) as a reference
- rice bran soymilk (RBS) (Sunstar group, Osaka, Japan) co-ingested with white bread
- sugar-free soymilk (SFS) (F&N, Singapore, Singapore) co-ingested with white bread
2.6. Statistical Analyses
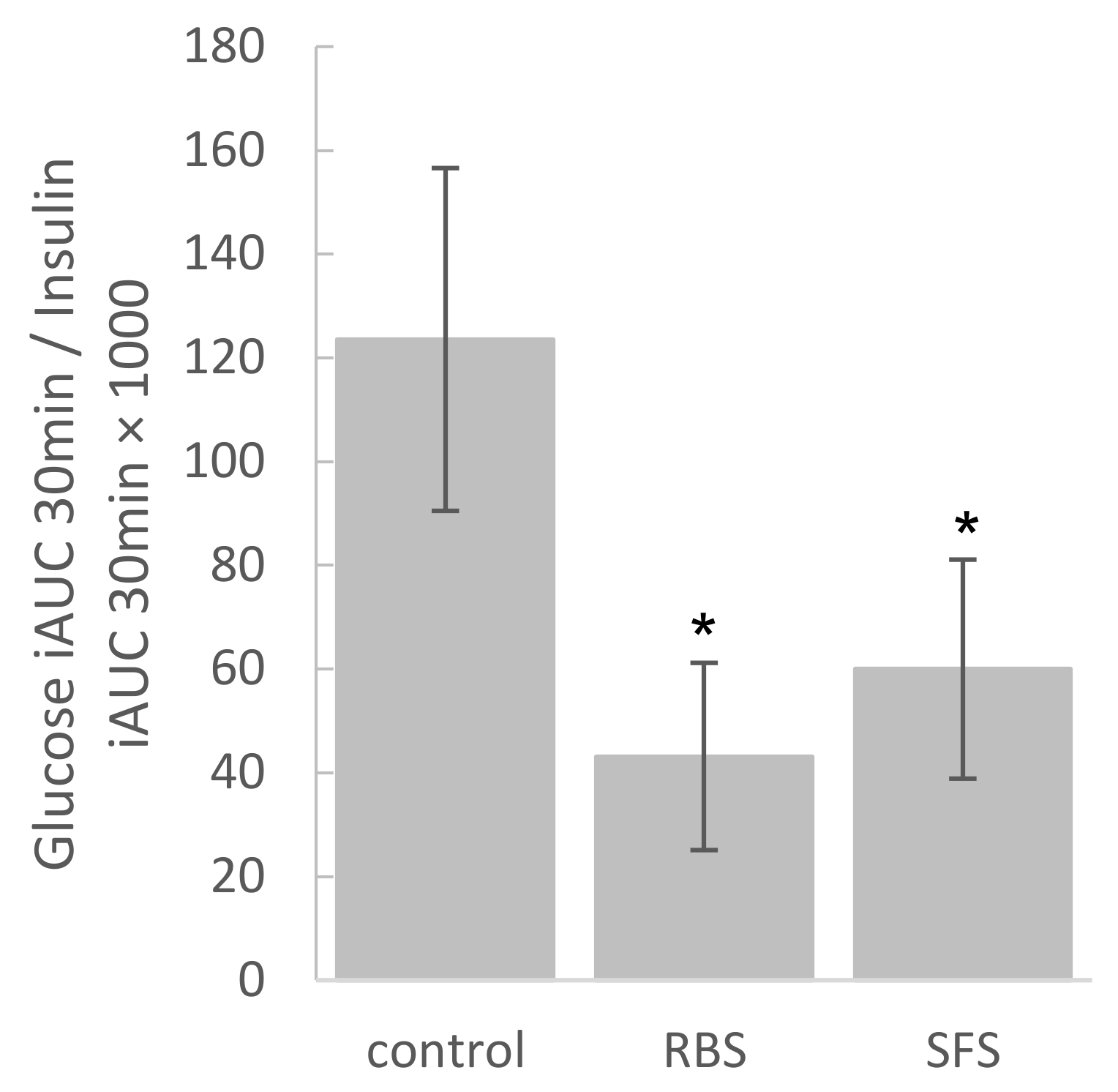
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Macro- and Micro-nutrient | RBS | SFS |
|---|---|---|
| Energy (kcal) | 96.0 | 72.2 |
| Protein (g) | 3.4 | 7.8 |
| Fat (g) | 3.4 | 3.5 |
| Total carbohydrate (g) | 16.1 | 4.8 |
| Available carbohydrate (g) | 9.7 | 2.3 |
| Dietary fiber (g) | 6.4 | 2.5 |
| Sodium (mg) | 8–25 | 5.9 |
| Iron (mg) | 1.3 | - |
| Potassium (mg) | 265 | - |
| Magnesium (mg) | 116 | - |
| Calcium (mg) | 12.5 | 390 |
| Vitamin B1 (mg) | 0.20 | - |
| Vitamin E (mg) | 1.0 | - |
| Vitamin K (mg) | 0–8 | - |
| Niacin (mg) | 5 | - |
| Vitamin B6 (mg) | 0.4 | - |
| γ-Aminobutyric acid (GABA) (mg) | 3 | - |
| Oryzanol (mg) | 23.8 | - |
| Sucrose (g) | 1.0 | - |
References
- Kelley, D.E. Sugars and starch in the nutritional management of diabetes mellitus. Am. J. Clin. Nutr. 2003, 78, 858S–864S. [Google Scholar] [CrossRef] [PubMed]
- Riccardi, G.; Rivellese, A.A.; Giacco, R. Role of glycemic index and glycemic load in the healthy state, in prediabetes, and in diabetes. Am. J. Clin. Nutr. 2008, 87, 269S–274S. [Google Scholar] [CrossRef] [PubMed]
- Brand-Miller, J.C.; Holt, S.H.A.; Pawlak, D.B.; McMillan, J. Glycemic index and obesity. Am. J. Clin. Nutr. 2002, 76, 281S–285S. [Google Scholar] [CrossRef] [PubMed]
- Brand-Miller, J.; Hayne, S.; Petocz, P.; Colagiuri, S. Low-glycemic index diets in the management of diabetes a meta-analysis of randomized controlled trials. Diabetes Care 2003, 26, 2261–2267. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, D.S. Dietary glycemic index and obesity. J. Nutr. 2000, 130, 280S–283S. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, D.J.A.; Kendall, C.W.C.; Augustin, L.S.A.; Franceschi, S.; Hamidi, M.; Marchie, A.; Jenkins, A.L.; Axelsen, M. Glycemic index: Overview of implications in health and disease. Am. J. Clin. Nutr. 2002, 76, 266S–273S. [Google Scholar] [CrossRef] [PubMed]
- Warren, J.M.; Henry, C.J.K.; Simonite, V. Low glycemic index breakfasts and reduced food intake in preadolescent children. Pediatrics 2003, 112, e414–e419. [Google Scholar] [CrossRef] [PubMed]
- Lennerz, B.S.; Alsop, D.C.; Holsen, L.M.; Stern, E.; Rojas, R.; Ebbeling, C.B.; Goldstein, J.M.; Ludwig, D.S. Effects of dietary glycemic index on brain regions related to reward and craving in men. Am. J. Clin. Nutr. 2013, 98, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Brennan, C.S. Dietary fibre, glycaemic response, and diabetes. Mol. Nutr. Food Res. 2005, 49, 560–570. [Google Scholar] [CrossRef] [PubMed]
- Quek, R.; Bi, X.; Henry, C.J. Impact of protein-rich meals on glycaemic response of rice. Br. J. Nutr. 2016, 115, 1194–1201. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.Y.; Siow, P.C.; Peh, E.; Henry, C.J. Influence of rice, pea and oat proteins in attenuating glycemic response of sugar-sweetened beverages. Eur. J. Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Soong, Y.Y.; Lim, J.; Sun, L.; Henry, C.J. Effect of co-ingestion of amino acids with rice on glycaemic and insulinaemic response. Br. J. Nutr. 2015, 114, 1845–1851. [Google Scholar] [CrossRef] [PubMed]
- Hu, E.A.; Pan, A.; Malik, V.; Sun, Q. White rice consumption and risk of type 2 diabetes: Meta-analysis and systematic review. BMJ 2012, 344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, K.-H.; Lee, J.-H.; Kim, J.-W.; Cho, J.H.; Choi, Y.-H.; Ko, S.-H.; Zimmet, P.; Son, H.-Y. Epidemic obesity and type 2 diabetes in Asia. Lancet 2006, 368, 1681–1688. [Google Scholar] [CrossRef]
- Xu, Y.; Wang, L.; He, J.; Bi, Y.; Li, M.; Wang, T.; Wang, L.; Jiang, Y.; Dai, M.; Lu, J.; et al. Prevalence and control of diabetes in Chinese adults. JAMA 2013, 310, 948–959. [Google Scholar] [CrossRef] [PubMed]
- Bakhit, R.M.; Klein, B.P.; Essex-Sorlie, D.; Ham, J.O.; Erdman, J.W., Jr.; Potter, S.M. Intake of 25 g of soybean protein with or without soybean fiber alters plasma lipids in men with elevated cholesterol concentrations. J. Nutr. 1994, 124, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpour-Niazi, S.; Mirmiran, P.; Hedayati, M.; Azizi, F. Substitution of red meat with legumes in the therapeutic lifestyle change diet based on dietary advice improves cardiometabolic risk factors in overweight type 2 diabetes patients: A cross-over randomized clinical trial. Eur. J. Clin. Nutr. 2015, 69, 592–597. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, D.A.; Kendall, C.C.; Augustin, L.A.; Mitchell, S.; Sahye-Pudaruth, S.; Blanco Mejia, S.; Chiavaroli, L.; Mirrahimi, A.; Ireland, C.; Bashyam, B.; et al. Effect of legumes as part of a low glycemic index diet on glycemic control and cardiovascular risk factors in type 2 diabetes mellitus: A randomized controlled trial. Arch. Intern. Med. 2012, 172, 1653–1660. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Sun, L.L.; He, L.P.; Ling, W.H.; Liu, Z.M.; Chen, Y.M. Soy food consumption, cardiometabolic alterations and carotid intima-media thickness in Chinese adults. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 1097–1104. [Google Scholar] [CrossRef] [PubMed]
- Sagara, M.; Kanda, T.; Njelekera, M.; Teramoto, T.; Armitage, L.; Birt, N.; Birt, C.; Yamori, Y. Effects of dietary intake of soy protein and isoflavones on cardiovascular disease risk factors in high risk, middle-aged men in Scotland. J. Am. Coll. Nutr. 2004, 23, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Mueller, N.; Odegaard, A.; Gross, M.; Koh, W.-P.; Yu, M.; Yuan, J.-M.; Pereira, M. Soy intake and risk of type 2 diabetes mellitus in Chinese Singaporeans. Eur. J. Nutr. 2012, 51, 1033–1040. [Google Scholar] [CrossRef] [PubMed]
- Nanri, A.; Mizoue, T.; Takahashi, Y.; Kirii, K.; Inoue, M.; Noda, M.; Tsugane, S. Soy product and isoflavone intakes are associated with a lower risk of type 2 diabetes in overweight Japanese women. J. Nutr. 2010, 140, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Villegas, R.; Gao, Y.-T.; Yang, G.; Li, H.-L.; Elasy, T.A.; Zheng, W.; Shu, X.O. Legume and soy food intake and the incidence of type 2 diabetes in the shanghai women’s health study. Am. J. Clin. Nutr. 2008, 87, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Tan, K.W.; Han, C.M.; Leow, M.K.; Henry, C.J. Impact of preloading either dairy or soy milk on postprandial glycemia, insulinemia and gastric emptying in healthy adults. Eur. J. Nutr. 2015, 56, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Sohail, M.; Rakha, A.; Butt, M.S.; Iqbal, M.J.; Rashid, S. Rice bran nutraceutics: A comprehensive review. Crit. Rev. Food Sci. Nutr. 2017, 57, 3771–3780. [Google Scholar] [CrossRef] [PubMed]
- Sharif, M.K.; Butt, M.S.; Anjum, F.M.; Khan, S.H. Rice bran: A novel functional ingredient. Crit. Rev. Food Sci. Nutr. 2014, 54, 807–816. [Google Scholar] [CrossRef] [PubMed]
- FAO. Carbohydrates in Human Nutrition: Report of a Joint FAO/WHO Expert Consultation. Available online: http://www.who.int/nutrition/publications/nutrientrequirements/9251041148/en/ (accessed on 3 April 2018).
- Wolever, T.M.S. The Glycaemic Index: A Physiological Classification of Dietary Carbohydrate; Cabi: Wallingford, UK, 2006. [Google Scholar]
- Bender, R.; Lange, S. Adjusting for multiple Testing—When and how? J. Clin. Epidemiol. 2001, 54, 343–349. [Google Scholar] [CrossRef]
- Hayter, A.J. The maximum familywise error rate of fisher’s least significant difference test. J. Am. Statist. Assoc. 1986, 81, 1000–1004. [Google Scholar] [CrossRef]
- Karhunen, L.J.; Juvonen, K.R.; Huotari, A.; Purhonen, A.K.; Herzig, K.H. Effect of protein, fat, carbohydrate and fibre on gastrointestinal peptide release in humans. Regul. Pept. 2008, 149, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Iverson, J.F.; Gannon, M.C.; Nuttall, F.Q. Ingestion of leucine + phenylalanine with glucose produces an additive effect on serum insulin but less than additive effect on plasma glucose. J. Amino Acids 2013. [Google Scholar] [CrossRef] [PubMed]
- Kalogeropoulou, D.; LaFave, L.; Schweim, K.; Gannon, M.C.; Nuttall, F.Q. Leucine, when ingested with glucose, synergistically stimulates insulin secretion and lowers blood glucose. Metabolism 2008, 57, 1747–1752. [Google Scholar] [CrossRef] [PubMed]
- Bernard, J.R.; Liao, Y.-H.; Doerner, P.G.; Ding, Z.; Hsieh, M.; Wang, W.; Nelson, J.L.; Ivy, J.L. An amino acid mixture is essential to optimize insulin-stimulated glucose uptake and GLUT4 translocation in perfused rodent hindlimb muscle. J. Appl. Physiol. 2012, 113, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Liu, R.; Xiong, Y.; Li, X.; Wang, X.; Ma, Y.; Guo, H.; Hao, L.; Yao, P.; Liu, L.; et al. Leucine facilitates the insulin-stimulated glucose uptake and insulin signaling in skeletal muscle cells: Involving mTORC1 and mTORC2. Amino Acids 2014, 46, 1971–1979. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Lee, I.M. Sedentary behaviour and life expectancy in the USA: A cause-deleted life table analysis. BMJ Open 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quddusi, S.; Vahl, T.P.; Hanson, K.; Prigeon, R.L.; D’Alessio, D.A. Differential effects of acute and extended infusions of glucagon-like peptide-1 on first- and second-phase insulin secretion in diabetic and nondiabetic humans. Diabetes Care 2003, 26, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Wei Jie Tan, K.; Jeyakumar Henry, C. Co-ingestion of essence of chicken to moderate glycaemic response of bread. Int. J. Food Sci. Nutr. 2015, 66, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Bruce, D.G.; Chisholm, D.J.; Storlien, L.H.; Kraegen, E.W. Physiological importance of deficiency in early prandial insulin secretion in non-insulin-dependent diabetes. Diabetes 1988, 37, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, A.; Arai, H.; Fukaya, M.; Sato, M.; Hisami, Y.-O.; Takeda, E.; Doi, T. Early-phase insulin secretion is disturbed in obese subjects with glucose intolerance. Metabolism 2007, 56, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Tura, A.; Kautzky-Willer, A.; Pacini, G. Insulinogenic indices from insulin and C-peptide: Comparison of beta-cell function from OGTT and IVGTT. Diabetes Res. Clin. Pract. 2006, 72, 298–301. [Google Scholar] [CrossRef] [PubMed]
- Del Prato, S. Loss of early insulin secretion leads to postprandial hyperglycaemia. Diabetologia 2003, 46, M2–M8. [Google Scholar] [CrossRef] [PubMed]
- Kozuka, C.; Yabiku, K.; Sunagawa, S.; Ueda, R.; Taira, S.; Ohshiro, H.; Ikema, T.; Yamakawa, K.; Higa, M.; Tanaka, H.; et al. Brown rice and its component, gamma-oryzanol, attenuate the preference for high-fat diet by decreasing hypothalamic endoplasmic reticulum stress in mice. Diabetes 2012, 61, 3084–3093. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.A.; Sami, S.A.; Khan, F.A. Effects of stabilized rice bran, its soluble and fiber fractions on blood glucose levels and serum lipid parameters in humans with diabetes mellitus types I and II. J. Nutr. Biochem. 2002, 13, 175–187. [Google Scholar] [CrossRef]
- Jung, C.H.; Lee, D.H.; Ahn, J.; Lee, H.; Choi, W.H.; Jang, Y.J.; Ha, T.Y. Gamma-oryzanol enhances adipocyte differentiation and glucose uptake. Nutrients 2015, 7, 4851–4861. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, R.; Colangelo, L.A.; Yeh, H.C.; Anderson, C.A.; Daviglus, M.L.; Liu, K.; Brancati, F.L. Potassium intake and risk of incident type 2 diabetes mellitus: The coronary artery risk development in young adults (cardia) study. Diabetologia 2012, 55, 1295–1303. [Google Scholar] [CrossRef] [PubMed]
- Karamali, M.; Bahramimoghadam, S.; Sharifzadeh, F.; Asemi, Z. Magnesium-zinc-calcium-vitamin D co-supplementation improves glycemic control and markers of cardio-metabolic risk in gestational diabetes: A randomized, double-blind, placebo-controlled trial. Appl. Physiol. Nutr. Metab. 2018. [Google Scholar] [CrossRef] [PubMed]
- Morais, J.B.S.; Severo, J.S.; de Alencar, G.R.R.; de Oliveira, A.R.S.; Cruz, K.J.C.; Marreiro, D.D.N.; Freitas, B.; de Carvalho, C.M.R.; Martins, M.; Frota, K.M.G. Effect of magnesium supplementation on insulin resistance in humans: A systematic review. Nutrition 2017, 38, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Ahn, C.; Kang, J.H.; Jeung, E.B. Calcium homeostasis in diabetes mellitus. J. Vet. Sci. 2017, 18, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Norouzi, S.; Adulcikas, J.; Sohal, S.S.; Myers, S. Zinc transporters and insulin resistance: Therapeutic implications for type 2 diabetes and metabolic disease. J. Biomed. Sci. 2017. [Google Scholar] [CrossRef] [PubMed]
- Schisterman, E.F.; Mumford, S.L.; Sjaarda, L.A. Failure to consider the menstrual cycle phase may cause misinterpretation of clinical and research findings of cardiometabolic biomarkers in premenopausal women. Epidemiol. Rev. 2014, 36, 71–82. [Google Scholar] [CrossRef] [PubMed]



| Meal Characteristic | Control | RBS | SFS |
|---|---|---|---|
| Volume of liquid (mL) | 195 | 195 | 195 |
| Amount of bread (g) | 95.8 | 89.5 | 91.4 |
| Calorie (kcal) | 251.9 | 331.3 | 312.5 |
| Protein (g) | 9.5 | 12.3 | 16.9 |
| Total CHO (g) | 52.4 | 65.0 | 54.8 |
| Dietary fiber (g) | 2.4 | 8.6 | 4.8 |
| Available CHO (g) | 50.0 | 56.4 | 50.0 |
| Fat (g) | 1.8 | 5.1 | 5.3 |
| Characteristic (n = 15) | Mean ± SEM | Range (min–max) |
|---|---|---|
| Age (years) | 28.6 ± 1.6 | 22.4–41.6 |
| Height (cm) | 174.1 ± 2.1 | 158.0–189.0 |
| Weight (kg) | 68.3 ± 2.3 | 52.8–82.8 |
| BMI (kg/m2) | 22.5 ± 0.6 | 19.4–26.5 |
| Systolic blood pressure (mmHg) | 120.1 ± 2.3 | 106–139 |
| Diastolic blood pressure (mmHg) | 71.6 ± 2.5 | 59–90 |
| Waist circumference (cm) | 79.4 ± 1.8 | 72–93 |
| Hip circumference (cm) | 96.5 ± 1.6 | 85–105 |
| Fasting blood glucose (mmol/L) | 4.7 ± 0.1 | 4.0–5.4 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Camps, S.G.; Lim, J.; Ishikado, A.; Inaba, Y.; Suwa, M.; Matsumoto, M.; Henry, C.J. Co-Ingestion of Rice Bran Soymilk or Plain Soymilk with White Bread: Effects on the Glycemic and Insulinemic Response. Nutrients 2018, 10, 449. https://doi.org/10.3390/nu10040449
Camps SG, Lim J, Ishikado A, Inaba Y, Suwa M, Matsumoto M, Henry CJ. Co-Ingestion of Rice Bran Soymilk or Plain Soymilk with White Bread: Effects on the Glycemic and Insulinemic Response. Nutrients. 2018; 10(4):449. https://doi.org/10.3390/nu10040449
Chicago/Turabian StyleCamps, Stefan Gerardus, Joseph Lim, Atsushi Ishikado, Yumi Inaba, Makoto Suwa, Motonobu Matsumoto, and Christiani Jeyakumar Henry. 2018. "Co-Ingestion of Rice Bran Soymilk or Plain Soymilk with White Bread: Effects on the Glycemic and Insulinemic Response" Nutrients 10, no. 4: 449. https://doi.org/10.3390/nu10040449