This section details the setup logistics (videoconferencing infrastructure, specialty consult submission, educational media, satisfaction surveys, website and marketing), staffing (clinical, administrative and technical), operations (before, during and after each session) and progressive expansion of SCAN-ECHO (additional specialties and attendees).
3.1. Setup
Videoconferencing infrastructure: Prior to launching SCAN-ECHO, the videoconferencing network had already been deployed at the Greater Los Angeles VA Medical Center and the affiliated CBOCs. Initially, this system was being used for selected provider to remote patient care encounters (e.g., infectious disease care and telemental health sessions). As the SCAN-ECHO implementation advanced, additional videoconferencing consoles were deployed throughout this region.
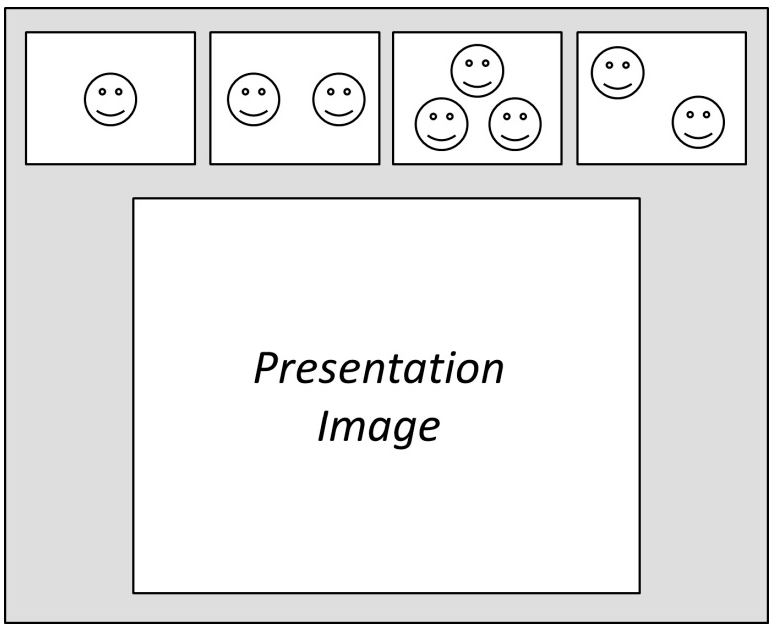
This system can be used in one-on-one or (for SCAN-ECHO) multipoint mode, wherein all videoconference participants are present on a designated portion of the screen; hence, all attendees can see and hear each other (
Figure 1).
Figure 1.
Screen layout for multipoint videoconference.
Figure 1.
Screen layout for multipoint videoconference.
The presenter can choose to broadcast an image of him/herself via the camera in the presentation image area (
Figure 1) or, at the touch of a button, the presenter can switch to broadcasting the full-screen image of a computer connected to the telehealth unit. Our presenters regularly prepared PowerPoint presentations for the didactics and each clinical case. These sessions involve strategically alternating between camera and computer screen (PowerPoint) view.
The basis of our (initial) system configuration involved the use of a dedicated high-speed digital audiovisual communication network, proprietary hardware (dedicated digital communication lines, terminals and a multipoint control unit (MCU) that serves as the videoconference system interface) and corresponding technical support staff (see the paragraph on technical staffing). Alternatively, a secured web-based videoconferencing system may be considered as a more economical alternative, requiring only that participants have access to a standard computer equipped with a high-speed Internet connection (≥3 mbps) and a webcam with a built-in microphone (around $30–$60), obviating the need for the acquisition, deployment, maintenance and staffing costs associated with a proprietary videoconferencing network.
Regardless of the communication technology utilized, all participants are expected to adhere to appropriate confidentiality protocols when referring to specific patients (e.g., Smith’s 2nd patient, Patient #101, etc.). Additionally, if images or health records are included in case presentations, all identifying information should be removed or graphically obscured per Health Insurance Portability and Accountability Act (HIPAA) protocols.
Specialty consult submission: The SCAN-ECHO process begins with the primary care provider obtaining informed consent from the patient to engage in this consultation; the patient has the right to know that his/her case will be discussed with other healthcare providers and that his/her medical records will likely be reviewed and discussed. Part of this informed consent process involves explaining to the patient that care may be better managed by the patient’s local provider, based on the recommendations rendered by the SCAN-ECHO consult. Alternatively, the patient has the right to refuse the SCAN-ECHO consult with no consequence and to have an (in-person) appointment with the specialist at the (distant) VA Medical Center. Finally, the patient is told that even if he/she consents to the SCAN-ECHO consultation, this does not preclude future in-person visits to the specialist at the VA Medical Center should such appointments be clinically warranted. Patients typically embrace the convenience of the SCAN-ECHO option and willingly give consent to the process.
Next, the primary care provider submits a SCAN-ECHO specialty consult request via the Computerized Patient Record System (CPRS), which is routed to the lead physician on the specialty team. For documentation thoroughness and simplicity, the first question on the referral screen asks “Does the patient consent to this SCAN-ECHO consult (Y/N)?” When considering the design of the referral screen, our clinicians reported that consult screens that demand entering multiple data fields tend to reduce the likelihood of such consults being completed and submitted. As such, we deliberately designed the SCAN-ECHO consult request screen to be brief, but specific, requiring only two entries: (1) the patient ID; and (2) the clinical question. We programmed the referral screen to automatically fill-in the referring provider’s name, date and time of the referral. Upon receipt of this referral, the designated specialty physician could read the clinical question that was submitted and access the patient’s full medical records to gather comprehensive details regarding the patient’s case and formulate a cogent care plan. Additionally, the specialist can ask further questions of the referring provider during the SCAN-ECHO session, in order to better focus the clinical recommendation(s).
Educational media: We initially began with one SCAN-ECHO specialty service: pain management. Prior to the launch, we reasoned that since this service involves professional consultations without the patient present, the sessions would be most productive if the referring provider were armed with highly detailed information regarding the nature of the patient’s condition in anticipation of the specialist’s diagnostic questions. To address this need, the project manager coordinated with the clinicians on the team to produce a series of pain diagnostic tutorial videos, providing instructions for carrying out comprehensive examinations of the five most common pain regions: hip, knee, shoulder, back and neck. These training videos were produced in a professional studio and distributed to participating providers on a disc; we also posted these tutorial videos on-line to facilitate further access.
Satisfaction surveys: We developed and implemented two on-line satisfaction surveys, which were sent at the conclusion of each session: A link to the Attendee Satisfaction Survey is emailed to all attendees to solicit their opinions about the overall session; a second email with a link to the Consult Satisfaction Survey is sent (only) to providers who processed a case in the session, to assess the utility of the specialty clinical consultation. For convenience, the surveys primarily consist of quick response type questions (e.g., checkboxes, Likert scales), along with some questions involving textual responses. This survey can be completed in 1 to 3 min (see the
Results Section).
Website: The project manager assembled a website for the SCAN-ECHO Pain Management service, providing a description of the specialty clinic, instructions for submitting consultation requests, videoconference session schedule, names and photographs of each specialty team members with corresponding links to their email and an up-to-date resource library containing a variety of downloadable properties (e.g., clinical guidelines, policies, diagnostic protocols, treatment algorithms, didactic PowerPoint in-services associated with each session and case summaries with treatment recommendations).
Marketing: The project manager assembled a social marketing/provider activation plan, which involved identifying and recruiting local site champions at each CBOC and scheduling an in-person site visit to introduce clinicians to the SCAN-ECHO service. These presentations were made during the regularly-scheduled administrative staff meeting time(s) at each site, so as not to disrupt regular clinical operations. The project manager explained the SCAN-ECHO service using a traditional PowerPoint presentation, which included an overview of SCAN-ECHO, advantages to patients (prompter care from their regular local providers, reduce/eliminate inconvenience, time and expense associated with travel to the VA Medical Center) and advantages to providers (continuing education, reduce peer isolation and personalized contact with specialists). These provider activation sessions concluded with step-by-step guidance for submitting a SCAN-ECHO consultation request and instructions for connecting to the sessions via the Telehealth console.
3.2. Staffing
Staffing, clinical: The SCAN-ECHO Pain Management team consists of one physician, two nurse practitioners and one psychologist, who provide clinical care in the Pain Management Clinic at the Greater Los Angeles VA Medical Center. Their SCAN-ECHO responsibilities involve about 10 h per month: approximately four hours to review, research and assemble treatment recommendations to address referred cases; three hours to prepare the didactic presentation; one hour a month to engage in the actual SCAN-ECHO sessions; and two one-hour staff meetings to process administrative issues.
Staffing, administrative: The project manager coordinates the operational duties, including scheduling SCAN-ECHO videoconference sessions, coordinating with telehealth technical staff, sending meeting notices (1 week and 1 day before each consultation clinic), managing email traffic from attendees and potential attendees, assembling, deploying and analyzing satisfaction surveys, coordinating with clinicians to develop educational materials and tuning service delivery per attendee feedback. The project manager also hosts each SCAN-ECHO session (see the paragraph on operations, SCAN-ECHO session). Additionally, the program manager is responsible for program expansion; this is a two-pronged approach that involves: (1) recruiting additional remote subscribers via telephone and email outreach along with in-person recruitment presentations; and (2) recruiting specialists to provide additional SCAN-ECHO consultation services (e.g., gerontology, gynecology, nephrology, neurology and urology).
Staffing, technical: The telehealth technical staff consists of two technicians to operate the multipoint control unit (MCU), which serves as the hub/interface of the videoconferencing network, two telehealth technicians stationed at the Medical Center, one telehealth technician stationed at each CBOC to facilitate quality connectivity and a technical support team to maintain existing hardware and to deploy additional teleconferencing terminals. Note, utilizing a proprietary network requires multiple technicians as specified above; use of a web-based videoconferencing system would likely substantially reduce the need for as many technicians.
3.3. Operations
Once established, running the SCAN-ECHO service on a regular basis can best be conceptualized in a serial fashion. This section provides an overview of SCAN-ECHO standard operations before, during and after each session.
3.3.1. Before
Scheduling: We discovered that there were three natural break points that remote clinicians could be available: 08:00–09:00 (pre-clinic administrative time), 12:00–13:00 (lunch time) and 16:00–17:00 (end of the day). Experience promptly revealed that the 16:00–17:00 hour was least optimal due to natural end-of-the-day exhaustion; additionally, often clinicians would still be tending to patients (well) past 16:00. We discovered that convening sessions on a fixed schedule (e.g., 3rd Thursday of the month from 12:00–13:00) facilitated the strongest attendance.
Reservations: The project manager is responsible for scheduling the videoconference system (MCU), (video) conference room and sending email notifications to all SCAN-ECHO participants detailing the date, time, connection code and referring providers whose cases will be addressed in each session. These emails are sent out one week before each session along with a one-day-before reminder message.
Specialty team meetings: The specialty team initially convened for one hour per week to formulate and adapt SCAN-ECHO operations and strategies. Subject matter included ideas for improving and refining services, processing findings gathered from the participant surveys, considering new ideas, recommendations and questions that emerged during sessions, identifying relevant didactic subject matter and brainstorming as needed. Additionally, the project manager, a mental health clinician, actively solicited and attended to the emerging impressions and feelings of all involved. As our processes became more refined, we shifted to meeting every other week.
Website: The project manager regularly updates the website; this typically involves uploading the PowerPoint didactic presentations and case summaries generated by the specialty team.
3.3.2. During
SCAN-ECHO session: Each SCAN-ECHO session runs one hour consisting of about three minutes for introductions, roll-call and administrative news, 10–15 min for the didactic, and the remaining time is used to address approximately three clinical referrals. The program manager arrives early to set up the room (align seating, adjust lighting, load PowerPoint didactic and case presentation) and to test/debug the videoconference technology. During the actual SCAN-ECHO sessions, the program manager fulfills multiple production roles, serving as host, facilitating introductions, moderating Q & A traffic, timekeeping for each segment and as the cameraman. SCAN-ECHO sessions are also optimal for on-camera demonstrations (e.g., physical exam protocol, identifying injection point(s), etc.). SCAN-ECHO sessions may convene more frequently, depending on the volume of referrals and the availability of the specialty team and attendees.
3.3.3. After
At the conclusion of each session, our team remains in the conference room and engages in a debriefing, openly discussing the cases, the tenor of the session, what worked, what needs to work better and possible changes and ideas for future sessions. Additionally, the program manager informally tends to the feelings and impressions of each team member and provides appropriate processing and support. This debriefing typically runs about 15 min.
Next, members of the specialty team enter the treatment recommendations that emerged during the session in each patient’s (electronic) medical records, thereby closing-out each consult request.
The program manager emails the attendee’s links to the on-line satisfaction survey(s) pertaining to the session (see
Results).




{kind=link}
{kind=link}
