Birth Defects in Gaza: Prevalence, Types, Familiarity and Correlation with Environmental Factors


Abstract
:1. Introduction
2. Results and Discussion
2.1. Registration of Births

{kind=link}
{kind=link}
{kind=link}
| (A) For all deliveries | (B) For parents of BD children, P, PBD, and late M |
| Name of parents Hospital ID | Anamnesis of mother and father |
| Family residence | Number of brothers and sisters of mother and father and their health status |
| Child sex | Number of children of brothers and sister of mother and father and their health status |
| Children date of birth | Type of dwelling |
| Weeks at delivery | Water access |
| Modality of delivery | Bombing on residence, in presence or when absent |
| Child weight | Bombing in adjacent housing |
| Child health conditions | Attacks to residence by white phosphorus, in presence or when absent |
| Clinical observations | Wounds, burns, injuries reported, which injuries |
| Child diagnosis | Care of other family members who received injury and which kind of injury |
| Congenital major structural birth defect from a list of major ones * | Clean up bombed, attacked residence |
| Consent of parents to use professionally the information | Use of recovery materials from debris to rebuild housing |
| Occupation of parents | Personally worked or familiar at home worked in recycling materials form rubble |
| List of other children of the couple and note on their health status: if alive, dead (and cause of death), previous miscarriages (numbers, time, the week they occurred and if the fetus had BD) | Children of the family play in bombed/attacked grounds |
| Direct exposure to WP and WP attacks on their residence in their absence | Health problems during attacks 2006 and 2008/09, description |
| Information if cases of BD occurred among the neighbors |
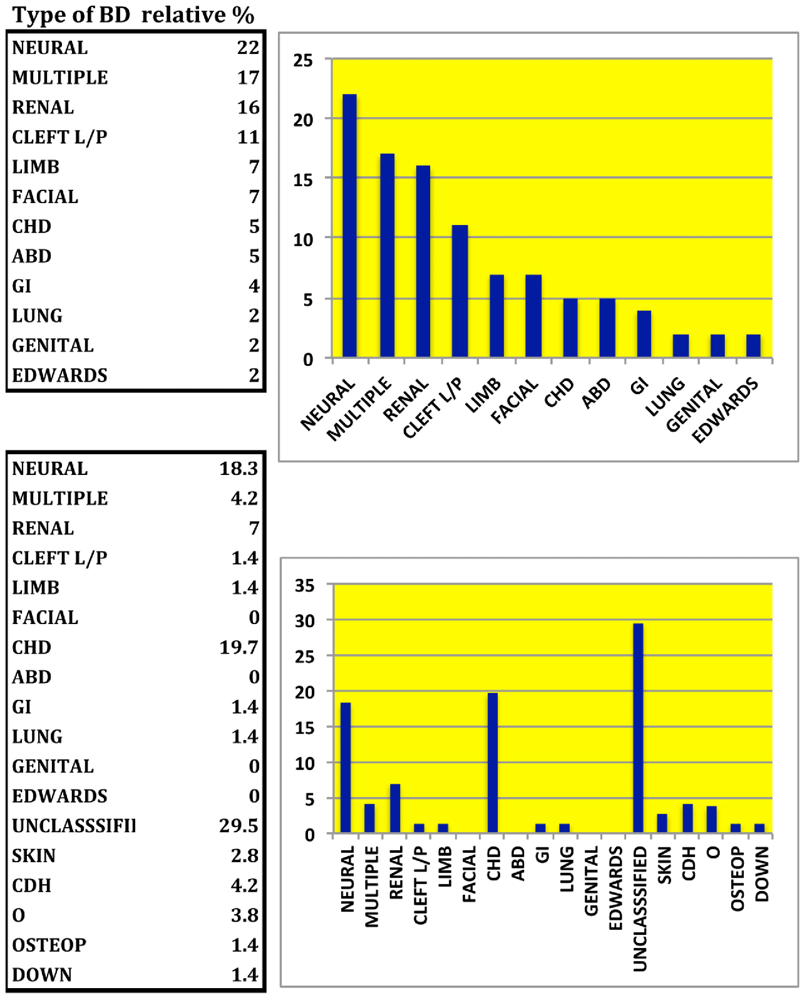
2.2. Classification of BD Types and Family History
| New born | Normal | Birth defect | Miscarriage | Premature | Still Born | Previous BD |
|---|---|---|---|---|---|---|
| Total numbers | 3,811 | 55 | 94 | 77 * | 30 | 82 |
| prevalence/1,000 | 974.6 | 14.0 | 23.3 | 19.6 | 7.4 | 20.9 a |
| Sex ratio M/F | 1 b | 0.94 | 1.1 | 0.67 | 0.88 | 0.95 |
| % Parents first cousins | 27 b | 29 | 36,1 | 13,3 | 30 | 39 |
| P vs. Normal | 0.847 | 0.06 | 0.009 | 0.871 | 0.022 |
| Q0 Ancephaly + multiple malformation | |
| Q20 CHD | Q74. Q74.2 congenital malformations of lower limbs |
| Q02 Microcephal + IUGR | Q39.0 aresia of oesophagus without fistula |
| Q75.9 Congenital malformation of skull and face bones + distended abdomen | Q39.0 aresia of oesophagus without fistula, premature |
| Q41.2 Small bowel volvulus + Menconium cyst | Q0.00 Anencephaly |
| Q87.0 CL, abnormal ear & mouth shape, deformity in toes | Q05 Spina bifida |
| Q89.7 and vaginal anomalies, abdominal distension, hydrops fetalis | Q30.0 Choanal atresia |
| Q98.7 multiple | Q03 hydrocephalus |
| Q79.5 Congenital malformation abdomen + lung hyperplasia | Q75.9 Facial bones anomaly |
| Q74.9 Unspecified congenital malformation of limbs | Q37 Ccenter palate with ccenter lip + multiple |
| Q60.6 Potter syndrome and renal agenesis, premature | Q25 Transposition of the great arteries |
| Q03 Hydrocephalus | Q62 Hydronephrosis |
| Q01.2 Occipital encephalocele | Q75.9 Facial bones anomaly |
| Q60.6 Potter’s syndrome + hypoplastic lungs | Q37 Ccenter palate with ccenter lip |
| Q75.9 Congenital malformation of skull and face bones, +ascite+IUFD | Q37 Ccenter palate with ccenter lip, premature |
| Q61.3 Polycystic kidney, unspecified | Q98.7 multiple, IUFD |
| Q0.00 Anencephaly-IUFD | Q03.9 Congenital hydrocephalus, unspecified + brain atrophy, premature |
| Q61.3 Polycystic kidney, unspecified | Q25 Transposition of the great arteries, TGA |
| Q01 Encephalocele | Q98.7 multiple |
| Q61.3 Polycystic kidney, unspecifiedHydrops fetalis not Rh | Q61.3 Polycystic kidney, unspecified + Intestinal obstruction |
| Q91.3 Edward syndrome | Q98.7 multiple, Premature |
| Q37 Ccenter palate with ccenter lip | Q98.7 multiple, Premature |
| Q87.8 Cystic Hygroma | Q61.3 Polycystic kidney, unspecified + mass in abdomen + asphyxia, dead |
| Q37 Ccenter palate with ccenter lip | Q74.2 congenital malformations of lower limbs |
| Q98.7 multiple+SB | Q74.2 congenital malformations of lower limbs + Abdominal wall |
| Q79.0 diaphragmatic hernia+Abdominal wall defect | Q37 Ccenter palate with ccenter lip + multiple |
| Q05 Spina bifida | Q05 Spina bifida |
| Q61.9 Congenital single renal cyst |
| Previous late miscarriages (%) | Previoud BD (%) | |
|---|---|---|
| Normal | na | 1.9 |
| Birth Defect | 18.0 | 20.0 |
| Miscarriage | 42.3 | 3.2 |
| Premature birth | 10.6 | 4.2 |
| Stillborn | 9.0 | 3.3 |
| Normal in family with previous BD | 10.9 | 0.2 a |

| BD in newborn | Parents relation | Previous BD/year | N sister children BD | N brother children BD | N sisters children BD | N brothers children BD |
|---|---|---|---|---|---|---|
| Q20 | na | 1child-Q20 | 0 | 0 | 0 | 0 |
| Q02 | 1 | 1child Q20, 1y | 0 | 0 | 0 | 0 |
| Q41.2 | 3 | 1 child Q02; 1child Q04.3 | 0 | 0 | 0 | 0 |
| Q03 | 3 | 1 child Q61.3 | na | na | na | na |
| Q00.0 | 1 | 1 child Q20, CHD, IUGF; 1 child Q04.3 | 0 | 0 | 0 | |
| Q03 | 3 | 3 children Q03/18,11,10 y | 0 | 0 | 0 | 0 |
| Q75.9 | 1 | 2 children Q04.9/3,1y | 0 | 0 | 0 | |
| Q75.9 | 2 | 1 child Q03 | 0 | 0 | 0 | 0 |
| Q03.9 | 3 | # Q03/18 to 10y | 0 | 0 | 0 | 0 |
| Q05 | Na | N | 1child Q04.3 | 0 | 0 | 0 |
| Q39.0 | 3 | N | 0 | 0 | 0 | 1child Q03, 2 children dumbness |
| Q61.3 | 3 | N | 0 | 0 | 0 | |
| Q87.0 | 1 | N | 0 | 0 | 0 | Q37 |
| Q75.9 | 1 | N | 0 | 0 | 1, Q01.9 | 0 |
| Q37 | 1 | Y, 2 children multiple /7,8 y | 1 child Q04.3 | 0 | 0 | 1 child Q04.3 |
| Q39.0 | 2 | N | 4 children Q00.0 | 0 | 0 | 1 child Q04.3 |
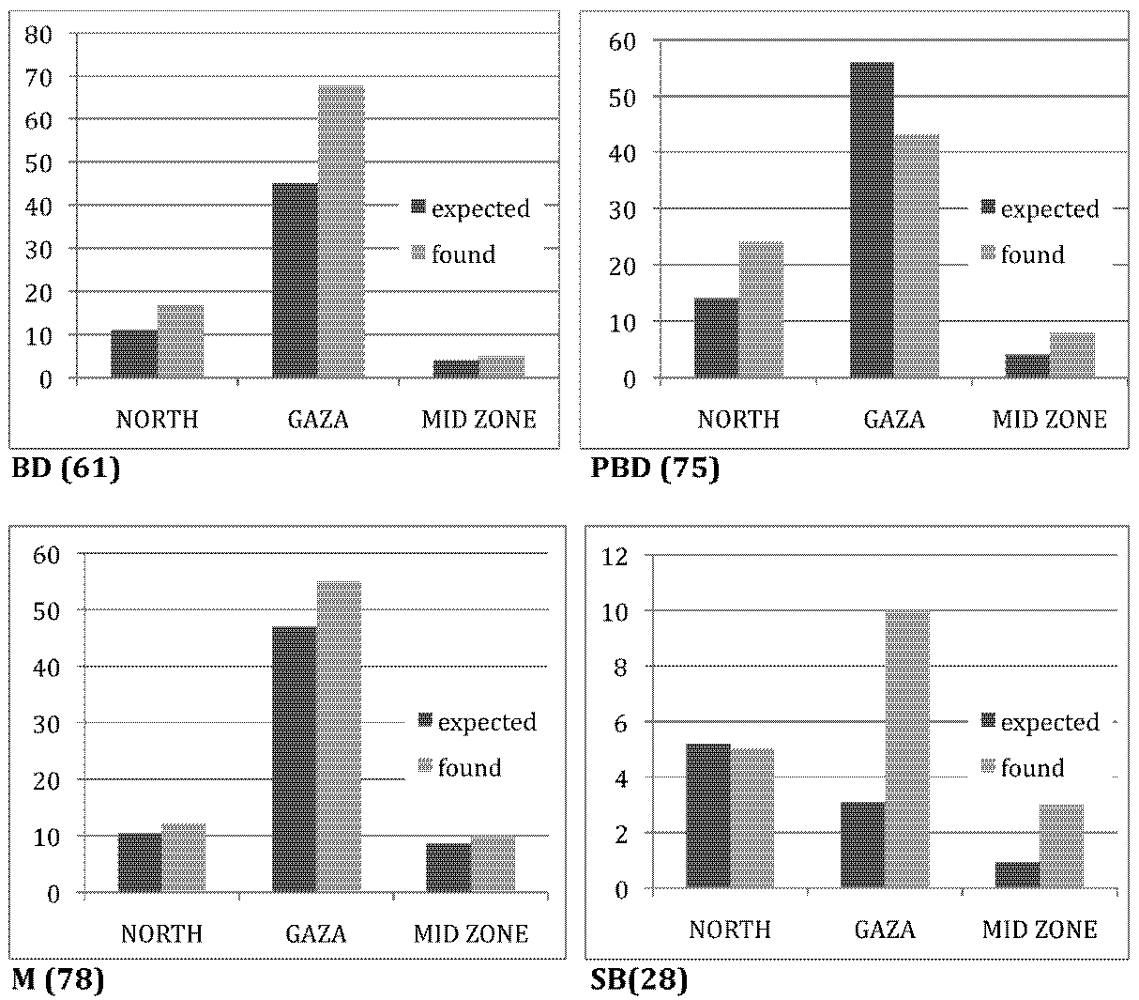
2.3. Residence and BD

2.4. Environmental Risks and Correlation to BD Occurrence
| Exposure | None | only WP ** | only Bombed | WP and Bombed | |||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Number | Prevalence (95% CI) | Number | Prevalence (95% CI) | Number | Prevalence (95% CI) | Number | Prevalence (95% CI) | |
| Normal | 2,933 | 2,884 | 98.3 (97.9–98.8) | 49 | 1.7 (1.2–2.1) | N/A | N/A | ||
| BD | 44 | 19 | 43.1 (28.5–57.8) | 12 | 27.2 (14.1–40.4) | 9 | 20.4 (8.5–32.4) | 8 | 18.2 (6.8–29.6) |
| Overall | 2977 | 2,903 | 97.5 (97.0–98.1) | 61 | 2.0 (1.5–2.6) | ||||

3. Experimental Section
4. Conclusions
Acknowledgments
Conflict of Interest
References
- Ministry of Health, Palestinian National Authority, Health Annual Report, Gaza Strip 2009; Ministry of Health, Palestinian National Authority: Gaza, Palestinian, 2011.
- Records of Maternity Hospital Al Shifa; Hospital Al Shifa: Gaza, Palestine, 2010.
- Haeusler, M.; Barisic, I.; Loane, M.; Garne, E.; Dolk, H. The EUROCAT network-organization and processes. Birth Defects Res. Part A 2011, 91, S2–S15. [Google Scholar]
- Swanson, J.M.; Entringer, S.; Buss, C.; Wadhaw, P.D. Developmental origins of health and disease: Environmental exposures. Semin. Reprod. Med. 2009, 27, 391–402. [Google Scholar]
- Surani, M.A. Reprogramming of genome function through epigenetic inheritance. Nature 2001, 414, 122–128. [Google Scholar]
- Alaani, S.; Savabieasfahani, M.; Tafash, M.; Manduca, P. Four polygamous families with congenital birth defects from Fallujah, Iraq. Int. J. Environ. Res. Public Health 2011, 8, 89–96. [Google Scholar]
- Manduca, P. High Prevalence Data and Increase in Time of Birth Defects in Fallujah, Iraq: Historical Reproductive Life and Hair Metal Load in Newborns and Children with Birth Defects and Their Families. Available online: http://www.newweapons.org (accessed on 17 March 2011).
- Darbre, P.D. Metalloestrogens: An emerging class of inorganic xenoestrogens with potential to add to the oestrogenic burden of the human breast. J. Appl. Toxicol. 2006, 26, 191–197. [Google Scholar]
- Cui, X.; Choi, S.M.; Yoo, S.D.; Lee, B.M. Toxicological characteristics of endocrine-disrupting chemicals: Developmental toxicity, carcinogenicity, and mutagenicity. J. Toxicol. Environ. Health B Crit. Rev. 2004, 7, 1–24. [Google Scholar]
- Romitti, P.A. Utility of family history reports of majorbirth defects as a public health strategy. Pediatrics 2007, 120 Suppl 2, S71–S77. [Google Scholar]
- Au, K.S.; Ashley-Koch, A.; Northrup, H. Epidemiologic and genetic aspects of spina bifida and other neural tube defects. Dev. Disabil. Res. Rev 2010, 16, 6–15. [Google Scholar]
- Wilson, P.D. Polycystic kidney disease. N. Engl. J. Med. 2004, 350, 151–164. [Google Scholar]
- Barbari, A.; Stephan, A.; Masri, M.; Karam, A.; Aoun, S.; El Nahas, J.; Bou Khalil, J. Consanguinity-associated kidney diseases in Lebanon: An epidemiological study. J. Mol. Immunol. 2003, 39, 1109–1114. [Google Scholar]
- Baillard, F.; Anderson, R.H. Tetralogy of fallot. Orphanet J. Rare Dis. 2009, 4. [Google Scholar] [CrossRef]
- Juriloff, D.M.; Harris, M.J. Mouse genetic models of cleft lip with or without cleft palate. Birth Defects Res. A 2008, 82, 63–77. [Google Scholar]
- Kuss, P.; Villavicencio-Lorini, P.; Witte, F.; Klose, J.; Albrecht, A.N.; Seemann, P.; Hecht, J.; Munlos, S. Mutant Hoxd13 induces extra digits in a mouse model of synpolydactyly directly and by decreasing retinoic acid synthesis. J. Clin. Invest. 2009, 119, 146–156. [Google Scholar]
- Skaik, S.; Abu-Shaban, N.; Barbieri, M.; Barbieri, M.; Giani, U.; Manduca, P. Metals detected by ICP/MS in wound tissue of war injuries without fragments in Gaza. BMC Int. Health Hum. Rights 2010, 10, 17–24. [Google Scholar]
- Jpärup, L. Hazards of heavy metal contamination. Br. Med. Bull. 2003, 68, 167–182. [Google Scholar]
- Beyersmann, D.; Hartwig, A. Carcinogenic metal compounds: Recent insight into molecular and cellular mechanisms. Arch. Toxicol. 2008, 82, 493–512. [Google Scholar]
- Choi, S.M.; Yoo, S.D.; Lee, B.M. Toxicological characteristics of endocrine-disrupting chemicals: Developmental toxicity, carcinogenicity, and mutagenicity. J. Toxicol. Environ. Health B Crit. Rev. 2004, 7, 1–24. [Google Scholar]
- Salnikow, K.; Zhitkovich, A. Genetic and epigenetic mechanisms in metal carcinogenesis and cocarcinogenesis: Nickel, arsenic, and chromium. Chem. Res. Toxicol. 2008, 21, 28–44. [Google Scholar]
- Haijova, P. Epigenetic reprogramming-taking a lesson from the embryo. Curr. Opin. Cell Biol. 2010, 22, 342–345. [Google Scholar]
- Perera, A.; Herbestman, J. Prenatal environmental exposure, epigenetics and disease. Reprod. Toxicol. 2001, 31, 363–373. [Google Scholar]
- El Wadia, H. personal communication. ICU of Al Shifa: Gaza, Palestine, 2012. [Google Scholar]
- ICD10. Available online: http://www.cdc.gov/ncbddd/birthdefects/index.html (accessed on 13 October 2011).
- EUROCAT. Available online: http://www.eurocat-network.eu/ (accessed on 13 October 2011).
- March of Dimes, Global Report on Birth Defects; March of Dimes Birth Defects Foundation: New York, NY, USA, 2006.
- ICHBDSR. Annual Report 2009 with Data for 2007; ICHBDSR: Roma, Italy, 2009. Available online: http://www.icbdsr.org/ (accessed on 13 October 2011).
- Abed, Y.; Al Barqouni, N.; Manduca, P.; Minutolo, R.; Mokhallati, M.; Naim, A. Prevanlence of Children with Major Structural Birth Defect (BD) in Pediatric Hospitals of GAZA Strip. Beirut, Lebanon, 5–6 March 2012. Presented at the Lancet-Palestinian Health Alliance Meeting.
Supplementary Files
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Naim, A.; Al Dalies, H.; El Balawi, M.; Salem, E.; Al Meziny, K.; Al Shawwa, R.; Minutolo, R.; Manduca, P. Birth Defects in Gaza: Prevalence, Types, Familiarity and Correlation with Environmental Factors. Int. J. Environ. Res. Public Health 2012, 9, 1732-1747. https://doi.org/10.3390/ijerph9051732
Naim A, Al Dalies H, El Balawi M, Salem E, Al Meziny K, Al Shawwa R, Minutolo R, Manduca P. Birth Defects in Gaza: Prevalence, Types, Familiarity and Correlation with Environmental Factors. International Journal of Environmental Research and Public Health. 2012; 9(5):1732-1747. https://doi.org/10.3390/ijerph9051732
Chicago/Turabian StyleNaim, Awny, Hedaya Al Dalies, Mohammed El Balawi, Eman Salem, Kholud Al Meziny, Raneem Al Shawwa, Roberto Minutolo, and Paola Manduca. 2012. "Birth Defects in Gaza: Prevalence, Types, Familiarity and Correlation with Environmental Factors" International Journal of Environmental Research and Public Health 9, no. 5: 1732-1747. https://doi.org/10.3390/ijerph9051732
APA StyleNaim, A., Al Dalies, H., El Balawi, M., Salem, E., Al Meziny, K., Al Shawwa, R., Minutolo, R., & Manduca, P. (2012). Birth Defects in Gaza: Prevalence, Types, Familiarity and Correlation with Environmental Factors. International Journal of Environmental Research and Public Health, 9(5), 1732-1747. https://doi.org/10.3390/ijerph9051732