1. Introduction
Given the recent severe food insecurity in the Horn of Africa [
1,
2] and the tens of thousands of refugees streaming into camps in Djibouti, Ethiopia and Kenya–with high mortality and acute malnutrition rates not seen for over a decade—a study of earlier (1997–2009) malnutrition and child mortality levels and trends in the region is timely and informative.
UNHCR’s Global Report 2005 [
3] (
i.e., with data from around the mid-point of the period studied here) for the Horn of Africa estimates that at that time there were 750,000 refugees and 1,250,000 other persons of concern plus 840,000 internally displaced people (IDPs) and 150,000 refugees in Sudan; all persons involuntarily migrated from their homes and livelihood. Thus approximately 3 million people were displaced, as refugees or IDPs. The causes are complex, but particularly include drought and conflict. Some of these refugees and IDPs (hereafter referred to as displaced persons) were housed in camps—many for years—run by United Nations (UN) agencies with non-governmental organization (NGO) partners. They received varying levels of humanitarian assistance, mainly medical, food aid, shelter, protection and core relief items. Others merged with the local populations, sometimes also having access to humanitarian assistance. Under these conditions, especially in children, acute malnutrition and elevated mortality rates were of particular concern.
We examined the results of 1,175 small-scale surveys carried out during 1997–2009 that assessed the extent and severity of acute malnutrition and child mortality. Analyses are secondary, based primarily on the results available from the surveys themselves. Surveys typically sampled approximately 900 households often using a 30 cluster × 30 household design, and followed the methods given in the ‘SMART Handbook’ [
4]. Survey design and implementation were not under our control, results being taken from the published reports as compiled by UN agencies (Standing Committee on Nutrition (SCN) and High Commissioner for Refugees (UNHCR)) and the Centre for Research on the Epidemiology of Disasters (CRED). The available survey results were compiled into a database to address questions of operational relevance for the Horn of Africa: (1) how elevated were malnutrition and mortality among displaced populations compared with host populations and what were their trends through time; (2) whether the relation between malnutrition and child mortality changed through time, and (3) how useful malnutrition prevalence was, or could be, in identifying populations with elevated mortality as priority for assistance. Growth patterns of children in the Horn of Africa vary greatly depending on whether the population’s livelihood is agricultural (
i.e., crop growing) or pastoral (
i.e., depending on cattle) [
5]. For instance, comparing Ugandan (mainly agricultural) and Somali (pastoral) pre-school children under their normal conditions using national surveys, the global acute malnutrition (GAM) prevalences were approximately 5% and nearly 20%, respectively. Moreover, comparative height growth occurred in the other direction (
i.e., Somali children grow faster in length, so that for example by 1 year Ugandan child stunting rates are about 40%, and Somali 25%). These effects balance each other in the sense that underweight prevalences are similar (
i.e., 30% and 25%, respectively) [
6]. However, small-scale surveys do not usually determine sampled children’s ages, so the measure of malnutrition depends primarily on weight-for-height (
i.e., wasting) [Global Acute Malnutrition (GAM) is the usual indicator, combining wasting prevalences (<–2SDs weight-for-age); since oedema is usually 1% or less, GAM and wasting are nearly identical, and for the present purposes (since oedema prevalences were not recorded) treated as the same)]. Thus, both the relation of acute malnutrition (when measured as GAM) to mortality, and hence the interpretation of GAM prevalences in considering mortality risk, need to take into account livelihoods, specifically agricultural or pastoralist. An objective was to examine the implications of taking livelihood into account in this context. The survey methods and results, while following standard procedures, did not always include U5MR (33% of surveys in the database did not estimate U5MR). One aim therefore was to indicate likely U5MR levels from GAM estimates, for when U5MR is not measured, and to contribute to the interpretation when both are.
Interpretation of survey results in terms of urgency of need for assistance depends on comparisons with cut-points, which presently do not vary among populations. For example, for child GAMs, the World Health Organization (WHO) recommends that a GAM prevalence of 10–15% is ‘serious’, and above 15% ‘critical’, for all populations [
7]. The UN Standing Committee on Nutrition (SCN) [
8] suggests that over 10% wasting prevalence is a serious situation. Under-5 mortality (U5MR) of >2/10,000/day is taken as an alert level indicating an emergency and urgent need for action [
8,
9,
10], and 1/10,000/day is a warning level. Similar cut-points for U5MR and GAM are used for Somali data by FAO [
11]. However, the relation between malnutrition (GAM) and mortality has not been used before to assess the implications of different levels of these indicators; rather they have been used in tandem (e.g., as in [
11]) together with other indicators.
Previous studies on populations less affected by displacement demonstrated that the relation between mortality and GAM varied by livelihood, suggesting variable GAM cut-points for different populations ranging from 8% to 20% GAM for agriculturalists
versus pastoralists, respectively [
6].
This study aims to improve the understanding of the practical interpretation of malnutrition levels in relation to mortality risk, from analysis of routine data usually available in emergencies. While further information—such as length of time displaced or of receipt of humanitarian assistance—would be useful, these were not available, as is often the case in actual decision-making. We aim to present a pragmatic analysis based on the data available, having established the most extensive compilation of survey results of this type yet accumulated, as far as is known.
2. Methods
Data were assembled by extracting survey results (aggregated prevalences and mortality estimates) from the UNSCN NICS (Nutrition in Crisis Situations) database [
12], plus additional survey results from the United Nations High Commissioner for Refugees’ (UNHCR) health information system (HIS) and the Centre for Research on the Epidemiology of Disasters (CRED) [
13]. Data from Ethiopia, Kenya, Sudan, and Uganda were selected; initially data from Somalia were included, however the data were of more uncertain quality and preliminary results showed more consistency from the other four countries, thus the Somali results are not reported here. The distribution of sources of survey results was 85% from NICS, 1% from UNHCR’s HIS, and 14% from CRED. Duplicates were eliminated, giving valid cases of 1,175 for GAM and 782 for U5MR. Sample sizes were recorded available for 44% of the surveys, and of these 75% were between 700 and 1000. All U5MR cases also had GAM recorded. GAM and U5MR results were obtained by surveys carried out by NGOs or UN agencies, almost always following a sampling procedure similar to the 30 cluster by 30 household design [
14]. The original data are not included in the databases, are not readily available, and could not be accessed for this study.
GAM is defined as percentage of the children sampled in each survey of less than minus 2 standard deviations of reference standards, plus prevalence of oedema (usually a fraction of wasting prevalence). When prevalences were reported based on NCHS standards, these were transformed to the equivalent using WHO standards using the WHO algorithm [
14] (neglecting oedema). U5MR was estimated generally using a 90-day recall period, and is given as deaths/10,000/day. Extreme values were excluded to avoid their undue influence on the results as follows. Values greater than 50% GAM prevalence were excluded (8 cases: >+4SDs). A cut-point for U5MR of greater than 7 (>3SDs; 23 cases) was used. Otherwise all data from 1997 to 2009 were included.
The displacement status of the populations surveyed is included in the NICS and other databases from where the data were taken, and was copied unchanged. In the data used, 14% were from populations defined as refugees, 9% IDPs, 59% were defined as resident (i.e., local surrounding population), and 18% mixed displaced and resident. The refugee and IDP data were combined into a category called displaced to increase sample size. The distribution of data was: Ethiopia 513 (44%), Kenya 125 (11%), Sudan 436 (37%), and Uganda 101 (9%).
Livelihood (pastoralist and agriculturalist) was not recorded in the survey results, but was assessed from where the population surveyed was located, from the livelihood (and ecology) of the area, recorded at the district level or equivalent. In Ethiopia pastoralists was defined as in Afar and Somali regions, and agriculturalists in others; in Uganda pastoralists were defined as in Karamoja. In Kenya all surveys were in pastoral areas of Northeast or Rift Valley provinces. In Sudan, surveys were from predominantly pastoral areas, and were assigned to the pastoral category.
Data was analyzed using the Statistical Package for Social Sciences (SPSS) version 16 and Microsoft Excel. Results in
Table 1 and
Table 2 were calculated using SPSS ‘compare means’, ANOVA, and non-parametric tests (Mann-Whitney and Kruskall-Wallis) as discussed below. GAM and U5MR were categorized to calculate sensitivity and specificity, by cross tabulation, as shown in
Table 3 and
Table 4; the test statistic used is the Youden Index [
15,
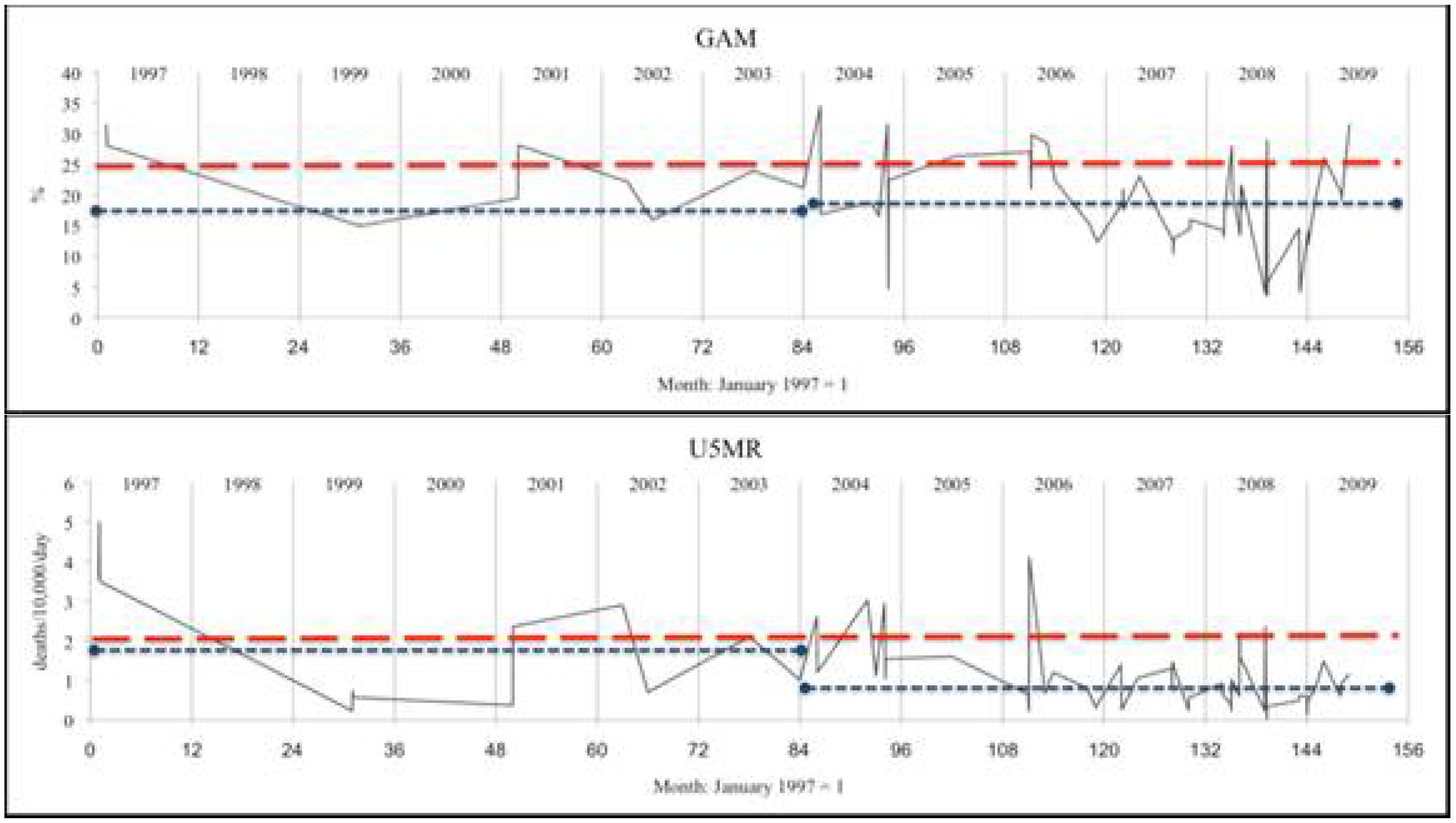
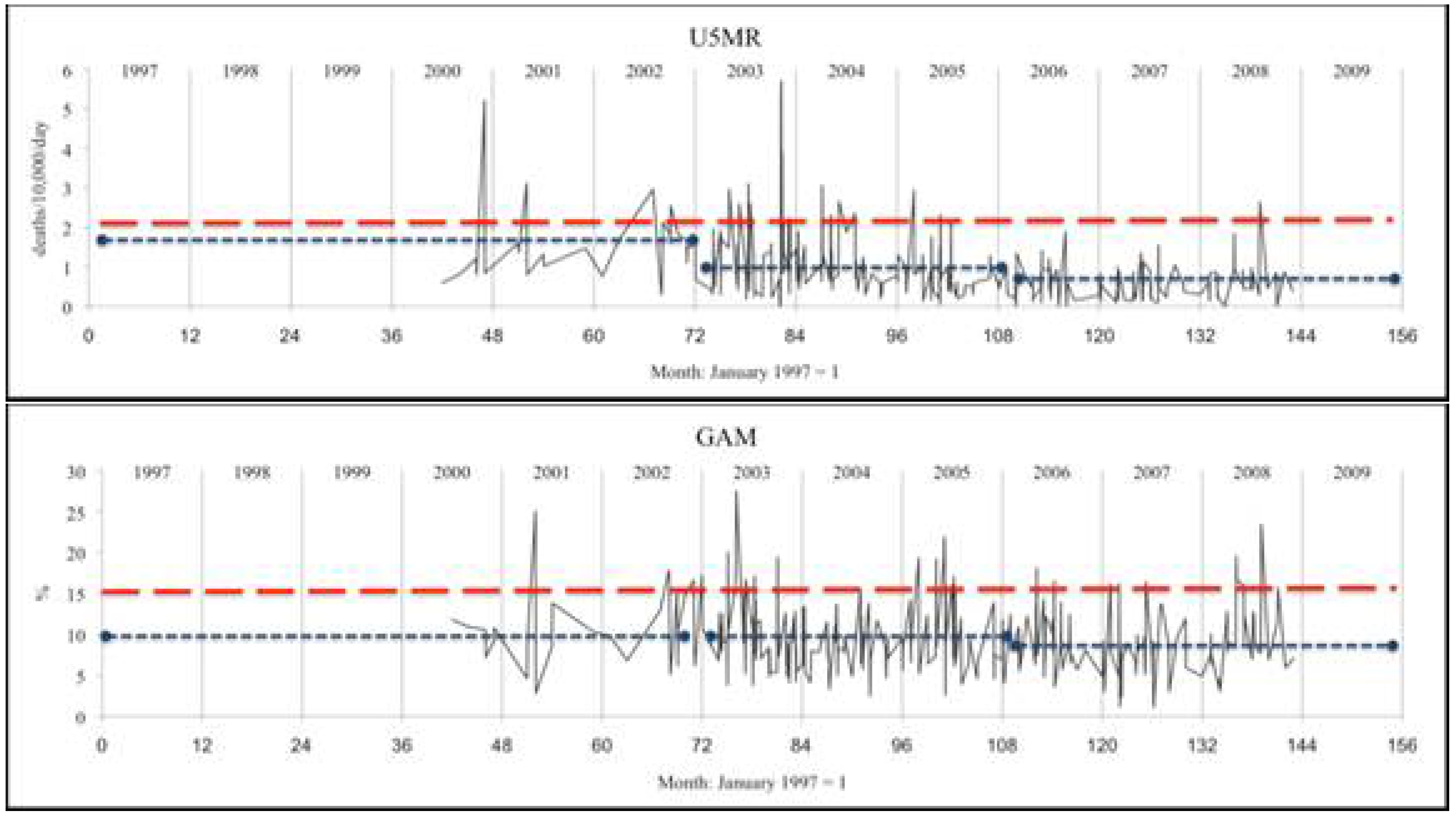
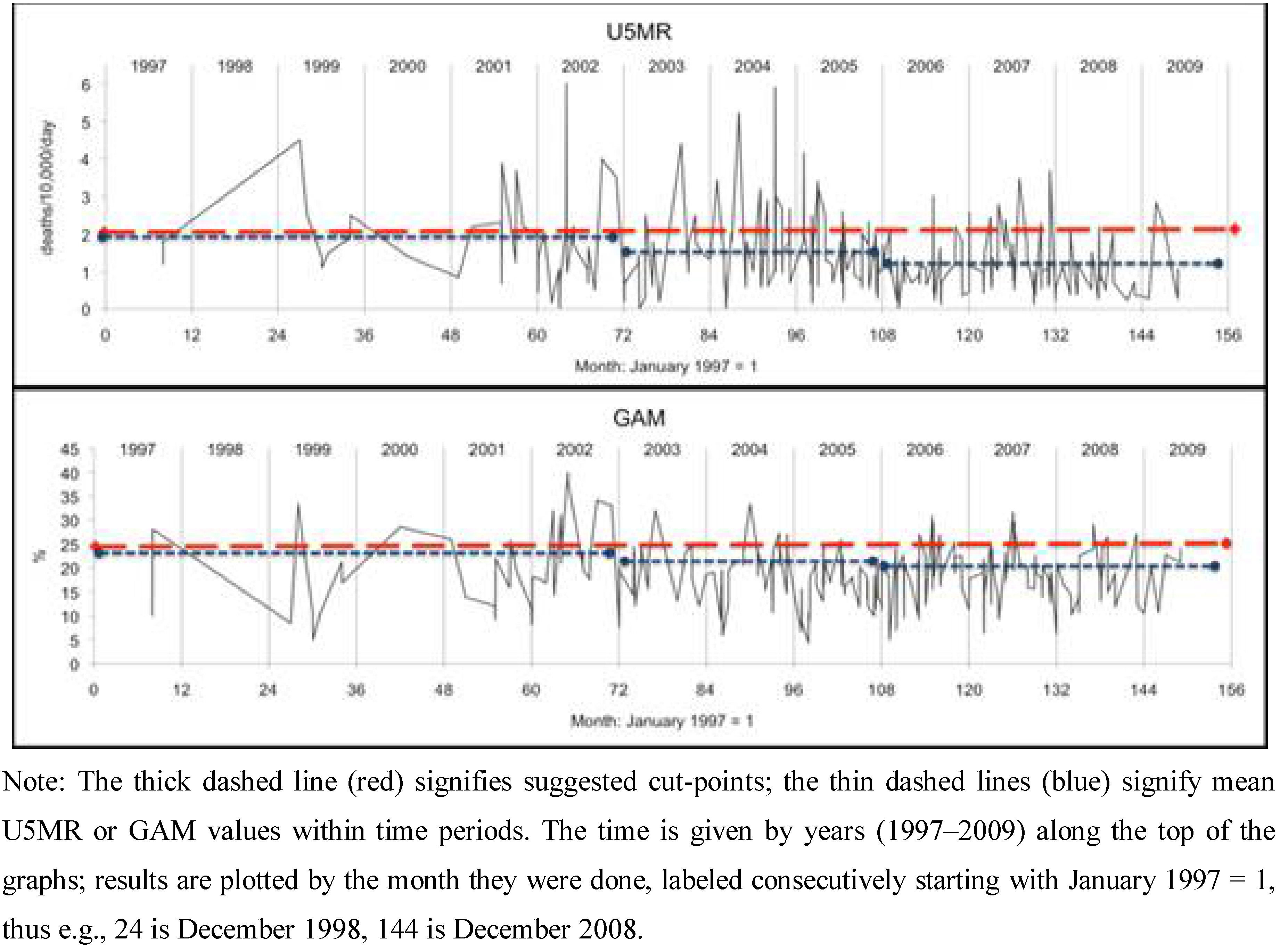
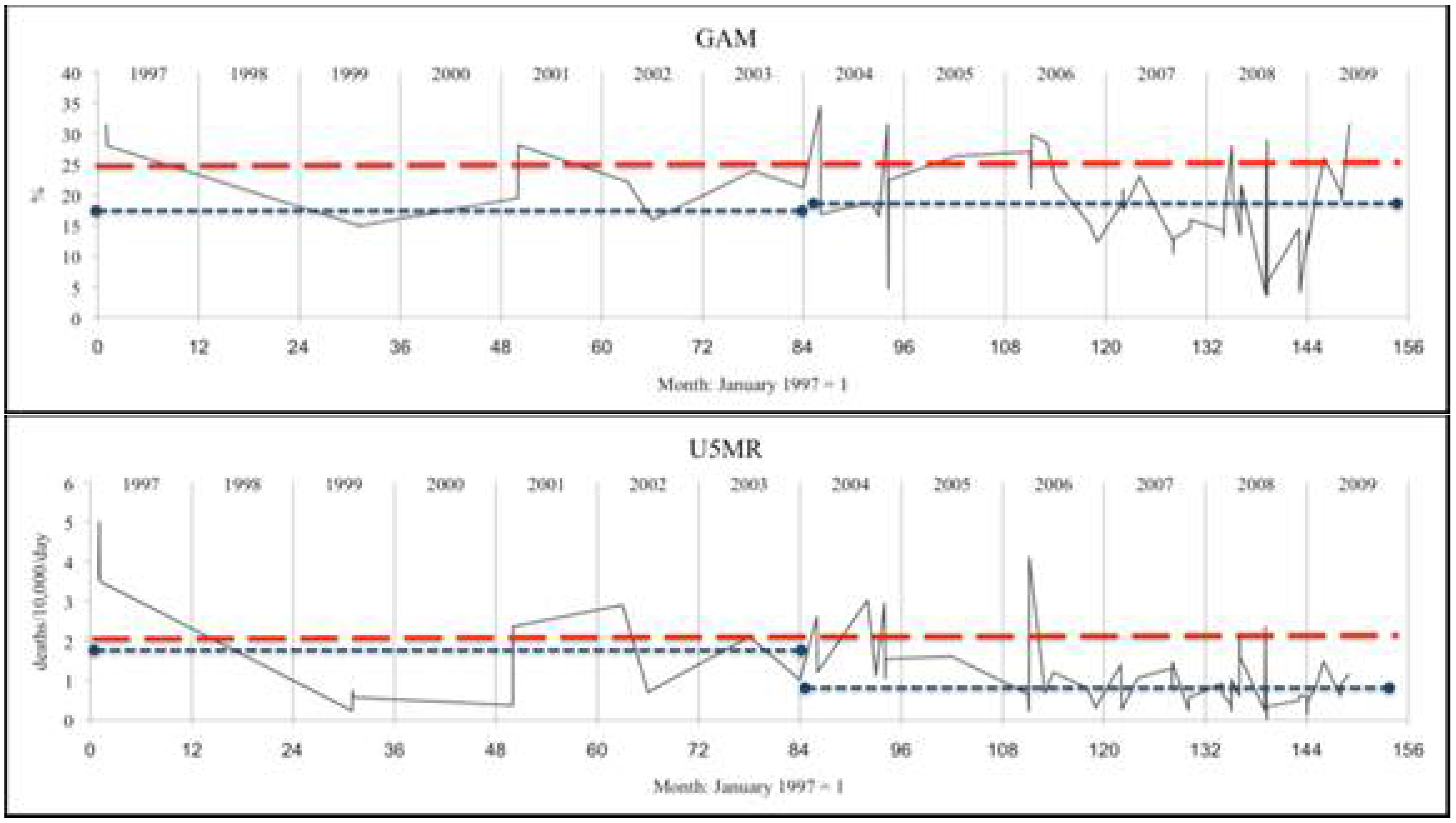
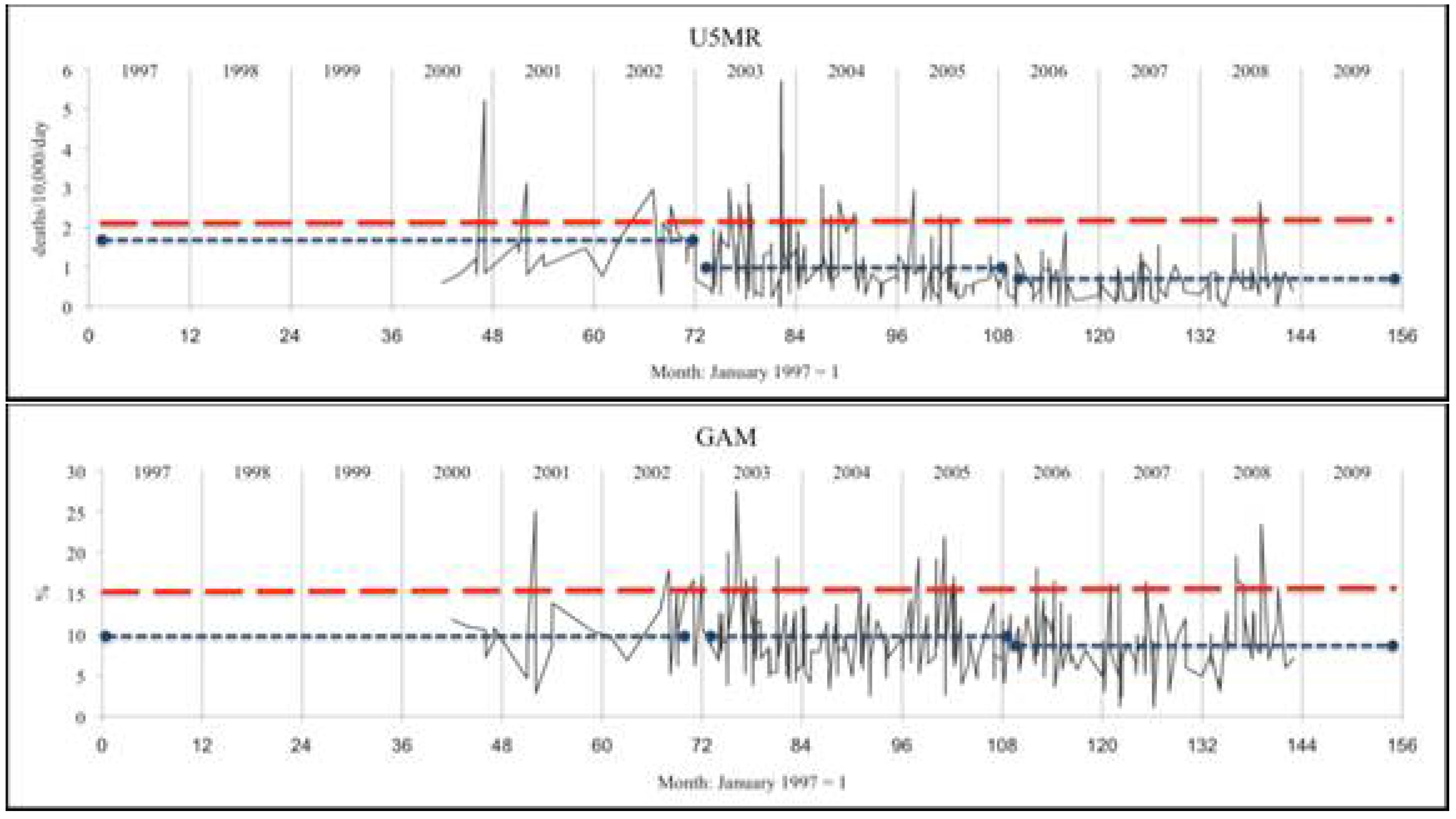
16]. The graphs of survey results plotted against time shown in
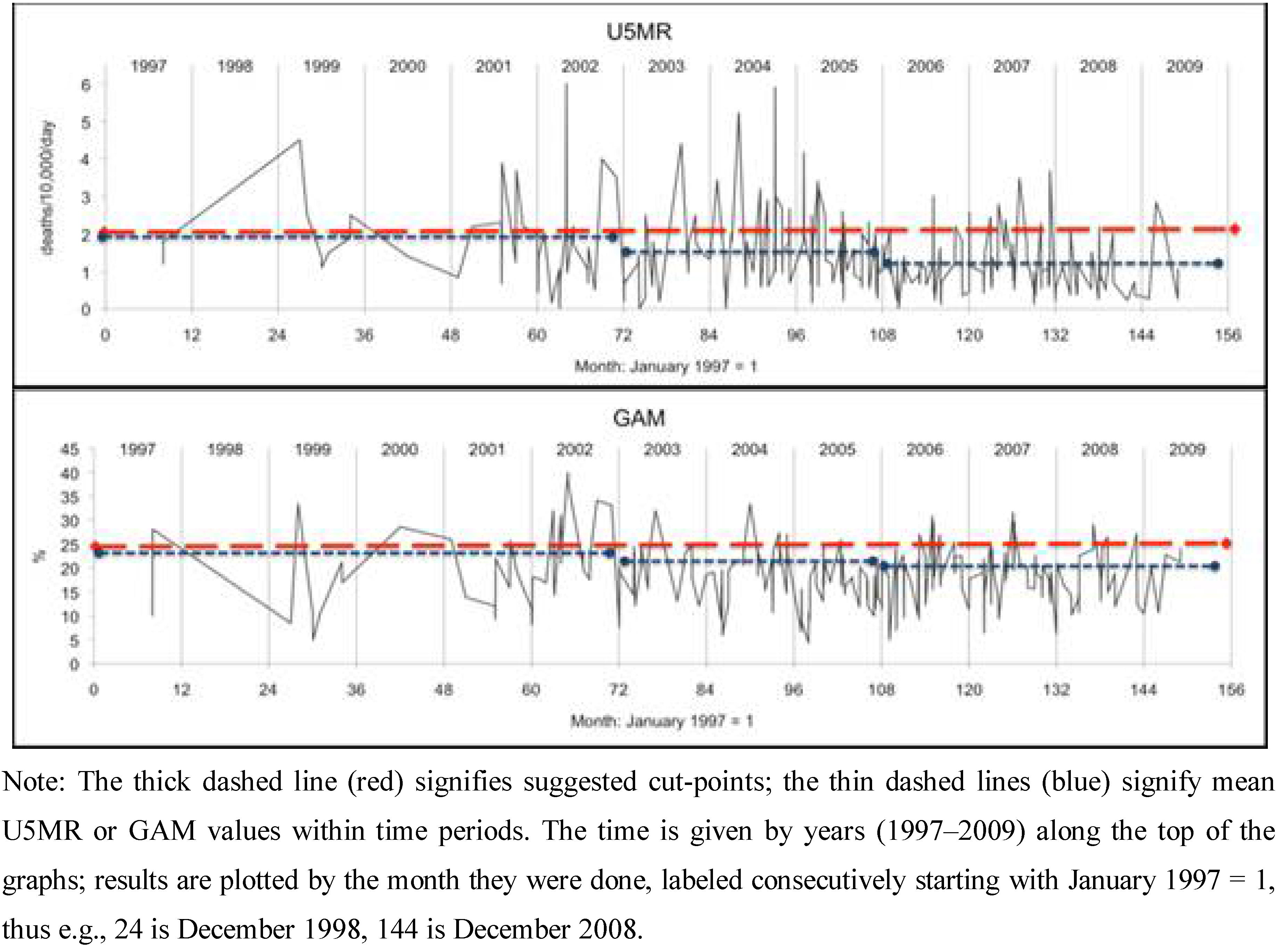
Figure 1 were generated in Excel. Survey dates were given by month and year and were coded as months with January 1997 = 1. Where two or more surveys were in the same month for the same country, they were separated by 0.05 months to allow Excel to plot the series shown in
Figure 1. Analyses were unweighted (by sample size), as a majority of sample sizes were not recorded, and those reported were in a narrow range.
Table 1.
Under-5 mortality rates (deaths/10,000/day) and GAM prevalence by livelihood and refugee status in Ethiopia, Kenya, Sudan and Uganda between 1997 and 2009 (n = number of survey results).
Table 1.
Under-5 mortality rates (deaths/10,000/day) and GAM prevalence by livelihood and refugee status in Ethiopia, Kenya, Sudan and Uganda between 1997 and 2009 (n = number of survey results).
| | Displaced persons (n) c,i | Local (Resident) (n) d,j | Mixed (n) e,k |
|---|
| A: Under-5 Mortality | | | |
| Pastoralists a | 1.43 (89) | 1.53 (186) | 1.48 (138) |
| Agriculturalists b | 1.41 (39) | 0.93 (315) | |
| Total f | 1.42 (128) | 1.15 (501) | |
| B: GAM (%) | | | |
| Pastoralists g | 16.4 (173) | 19.3 (302) | 18.0 (188) |
| Agriculturalists h | 7.2 (104) | 9.0 (389) | |
| Total l | 13.0 (277) | 13.5 (691) | |
Table 2.
Under-5 mortality (deaths/10,000/day) and GAM (%) by periods of years refugees/IDP, resident and mixed populations combined between 1997 and 2009 (n = number of survey results; p values estimated by Kruskall-Wallis non-parametric tests).
Table 2.
Under-5 mortality (deaths/10,000/day) and GAM (%) by periods of years refugees/IDP, resident and mixed populations combined between 1997 and 2009 (n = number of survey results; p values estimated by Kruskall-Wallis non-parametric tests).
| | Under-5 Mortality (n) | Global Acute Malnutrition (with oedema included) (n) |
|---|
| A: Sudan (pastoralists) | | |
| 1997–2002 | 1.83 (57) | 18.9 (117) |
| 2003–2006 | 1.40 (158) | 17.7 (222) |
| 2007–2009 | 1.09 (77) | 17.4 (97) |
| Total | 1.46 (292) | 18.0 (436) |
| p | 0.000 | 0.60 |
| B: Kenya (pastoralists) | | |
| 1997–2004 | 1.90 (21) | 17.9 (51) |
| 2005–2009 | 0.87 (47) | 18.6 (74) |
| Total | 1.19 (68) | 18.3 (125) |
| p | 0.000 | 0.58 |
| C: Ethiopia (agriculturalists only) | |
| 1997–2002 | 1.59 (32) | 9.2 (110) |
| 2003–2006 | 0.94 (221) | 9.3 (225) |
| 2007–2009 | 0.56 (76) | 8.8 (77) |
| Total | 0.92 (329) | 9.2 (412) |
| p | 0.000 | 0.12 |
| D: Ethiopia (pastoralists only) | |
| 1997–2004 | 2.25 (30) | 20.9 (65) |
| 2005–2009 | 2.10 (33) | 16.0 (36) |
| Total | 2.18 (63) | 19.1 (101) |
| p | 0.39 | 0.10 |
Table 3.
Under-5 mortality (deaths/10,000/day) and GAM (%) by period for refugees/IDP, resident and mixed populations in pastoralists in Sudan and Kenya between 1997 and 2009 (n = number of survey results; p values estimated by Kruskall-Wallis non-parametric tests).
Table 3.
Under-5 mortality (deaths/10,000/day) and GAM (%) by period for refugees/IDP, resident and mixed populations in pastoralists in Sudan and Kenya between 1997 and 2009 (n = number of survey results; p values estimated by Kruskall-Wallis non-parametric tests).
| U5MR, deaths/10,000/day | GAM % |
|---|
| Time period | Displaced persons | Local (Resident) | Mixed | Displaced persons | Local (Resident) | Mixed |
|---|
| 1997–2002 | 1.77 (15) | 1.95 (18) | 1.84 (34) | 15.6 (52) | 20.9 (52) | 19.5 (50) |
| 2003–2006 | 1.58 (49) | 1.28 (68) | 1.41 (61) | 18.1 (65) | 19.7 (111) | 16.4 (86) |
| 2007–2009 | 1.09 (26) | 0.88 (50) | 1.10 (38) | 15.5 (43) | 18.2 (59) | 16.8 (42) |
| Total | 1.47 (90) | 1.22 (136) | 1.43 (133) | 16.6 (160) | 19.6 (222) | 17.4 (178) |
| p | 0.08 | 0.00 | 0.01 | 0.02 | 0.15 | 0.17 |
Table 4.
Example of correspondence between U5MR and GAM for surveys between 1997 and 2009.
| A: Kenya (pastoralists) at cut-off point of 20% GAM a |
|---|
| U5MR | |
| GAM | ≥2.0 | <2.0 | Total |
| ≥20% | 11 | 18 | 29 |
| <20% | 2 | 37 | 39 |
| Total | 13 | 55 | 68 |
| B: Ethiopia (agriculturalists only) at cut-off point of 10% GAM b |
|---|
| U5MR | |
| GAM | ≥2.0 | <2.0 | Total |
| ≥10% | 16 | 99 | 115 |
| <10% | 12 | 202 | 214 |
| Total | 28 | 301 | 329 |
Figure 1. Patterns of survey results: malnutrition (GAM) and child mortality (U5MR) plotted by month of survey.
C: Ethiopia (agriculturalists only)
C: Ethiopia (agriculturalists only)


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}