Long-Term Effects of Self-Control on Alcohol Use and Sexual Behavior among Urban Minority Young Women

Abstract
:1. Introduction
1.1. Co-Morbidity of High Risk Drinking and Sexual Behavior
1.2. The Development and Expression of Self-Control
1.3. A Focus on Urban Minority Women
1.4. Study Goals
2. Methods
2.1. Sample
2.2. Procedure
2.3. Measures
2.4. Data Analysis Plan
3. Results
3.1. Attrition Analyses
3.2. Prevalence of Young Adult High-Risk Behaviors
3.3. LCA Results

{kind=link}
{kind=link}
| Number of classes | Log-likelihood (L2) | BIC-L2 | AIC-L2 | Npar/DF | G2 | L2/df | p-value a | %ERb |
|---|---|---|---|---|---|---|---|---|
| 1-class | 2548.2 | 5148.7 | 5112.4 | 8/238 | 880.3 | 10.71 | 0.0000 | 0.000 |
| 2-class | 2216.3 | 4543.7 | 4466.6 | 17/238 | 472.1 | 9.31 | 0.0000 | 0.087 |
| 3-class | 2060.1 | 4290.3 | 4172.3 | 26/229 | 159.8 | 8.99 | 0.9829 | 0.081 |
| 4-class | 2038.6 | 4306.0 | 4147.1 | 35/220 | 116.7 | 9.26 | 1.0 | 0.800 |
| 5-class | 2022.1 | 4332.0 | 4132.2 | 44/211 | 83.8 | 9.58 | 1.0 | 0.794 |
| 6-class | 2014.8 | 4376.1 | 4135.5 | 53/202 | 69.1 | 9.97 | 1.0 | 0.790 |
| 7-class | 2009.2 | 4423.9 | 4142.4 | 62/193 | 57.9 | 10.41 | 1.0 | 0.790 |
| 8-class | 2005.1 | 4474.4 | 4152.1 | 71/184 | 49.6 | 10.89 | 1.0 | 0.787 |
| 9-class | 2001.3 | 4525.8 | 4162.7 | 80/175 | 42.2 | 11.44 | 1.0 | 0.785 |
| 10-class | 1997.4 | 4576.9 | 4172.8 | 89/166 | 34.4 | 12.03 | 1.0 | 0.784 |
| Model 1: Unconstrained | Model 2: Constrained | |||||
|---|---|---|---|---|---|---|
| Class 1 | Class 2 | Class 3 | Class 1 | Class 2 | Class 3 | |
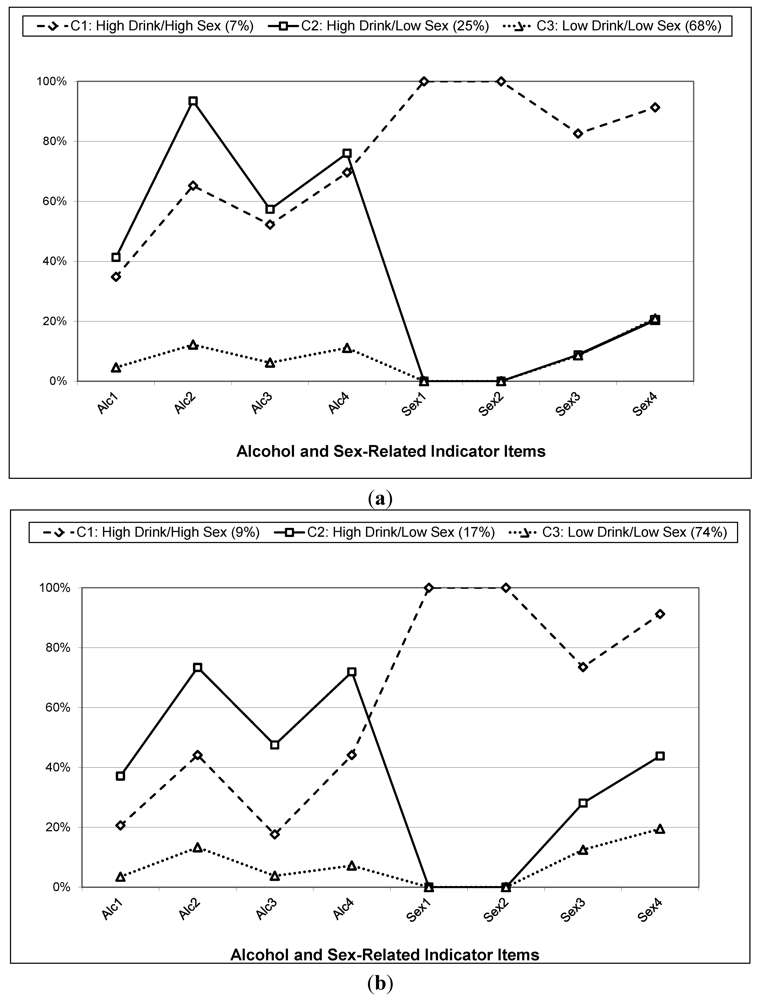
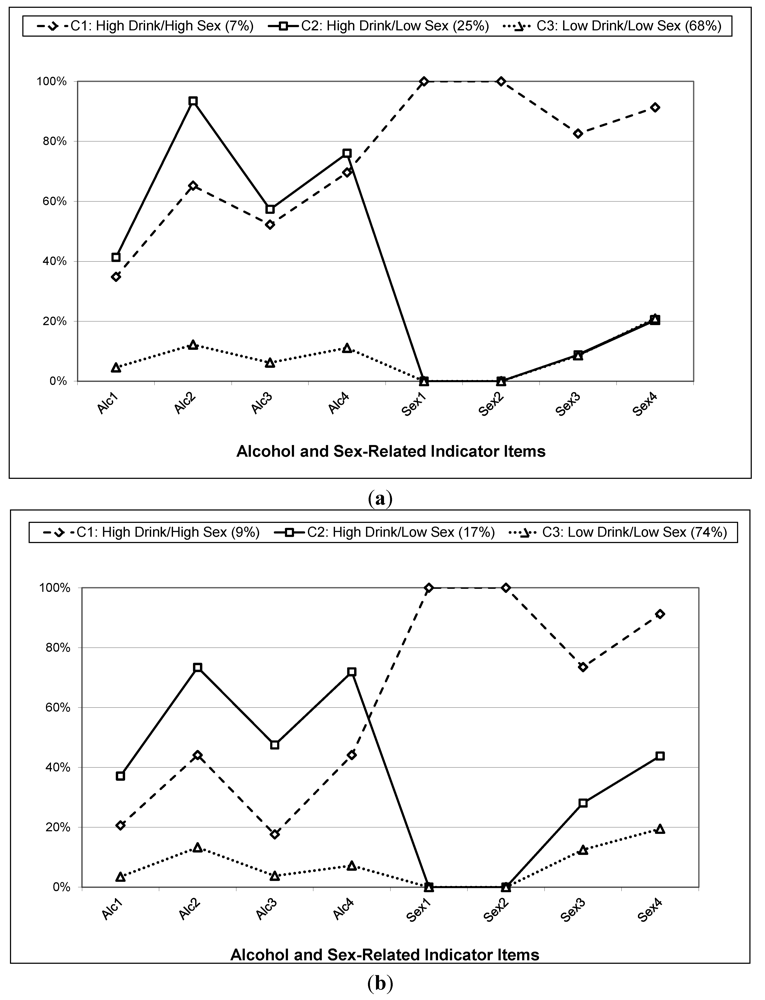
| Black Participants | ||||||
| Proportion | 0.033 | 0.113 | 0.304 | 0.033 | 0.118 | 0.299 |
| Count (N = 312) | 23 | 78 | 211 | 23 | 82 | 207 |
| 7% | 25% | 68% | 7% | 26% | 66% | |
| Item Probabilities (for higher risk responding) | ||||||
| Drinking Frequency (Alc1) | 0.348 | 0.413 | 0.046 | 0.263 | 0.409 | 0.046 |
| Drunkenness Frequency (Alc2) | 0.652 | 0.935 | 0.122 | 0.526 | 0.899 | 0.134 |
| Drinking Quantity (per occasion) (Alc3) | 0.522 | 0.573 | 0.062 | 0.316 | 0.571 | 0.051 |
| Binge Days in Past 3 Months (Alc4) | 0.696 | 0.760 | 0.111 | 0.544 | 0.766 | 0.102 |
| # Sexual Partners (Sex1) | 1.000 | 0.000 | 0.000 | 1.000 | 0.000 | 0.000 |
| Recent Sexual Partners (Sex2) | 1.000 | 0.000 | 0.000 | 1.000 | 0.000 | 0.000 |
| New Sexual Partners (Sex3) | 0.826 | 0.088 | 0.086 | 0.772 | 0.141 | 0.120 |
| Sex Events w/ Non-Main Partner (Sex4) | 0.913 | 0.204 | 0.209 | 0.912 | 0.271 | 0.215 |
| Class 1 | Class 2 | Class 3 | Class 1 | Class 2 | Class 3 | |
| Other Participants | ||||||
| Proportion | 0.049 | 0.092 | 0.407 | 0.049 | 0.075 | 0.425 |
| Count (N = 380) | 34 | 64 | 282 | 34 | 52 | 294 |
| 9% | 17% | 74% | 9% | 14% | 77% | |
| Item Probabilities (for higher risk responding) | ||||||
| Drinking Frequency (Alc1) | 0.206 | 0.371 | 0.035 | 0.263 | 0.409 | 0.046 |
| Drunkenness Frequency (Alc2) | 0.441 | 0.734 | 0.133 | 0.526 | 0.899 | 0.134 |
| Drinking Quantity (per occasion) (Alc3) | 0.176 | 0.475 | 0.038 | 0.316 | 0.571 | 0.051 |
| Binge Days in Past 3 Months (Alc4) | 0.441 | 0.719 | 0.072 | 0.544 | 0.766 | 0.102 |
| # Sexual Partners (Sex1) | 1.000 | 0.000 | 0.000 | 1.000 | 0.000 | 0.000 |
| Recent Sexual Partners (Sex2) | 1.000 | 0.000 | 0.000 | 1.000 | 0.000 | 0.000 |
| New Sexual Partners (Sex3) | 0.735 | 0.281 | 0.125 | 0.772 | 0.141 | 0.120 |
| Sex Events w/ Non-Main Partner (Sex4) | 0.912 | 0.438 | 0.195 | 0.912 | 0.271 | 0.215 |
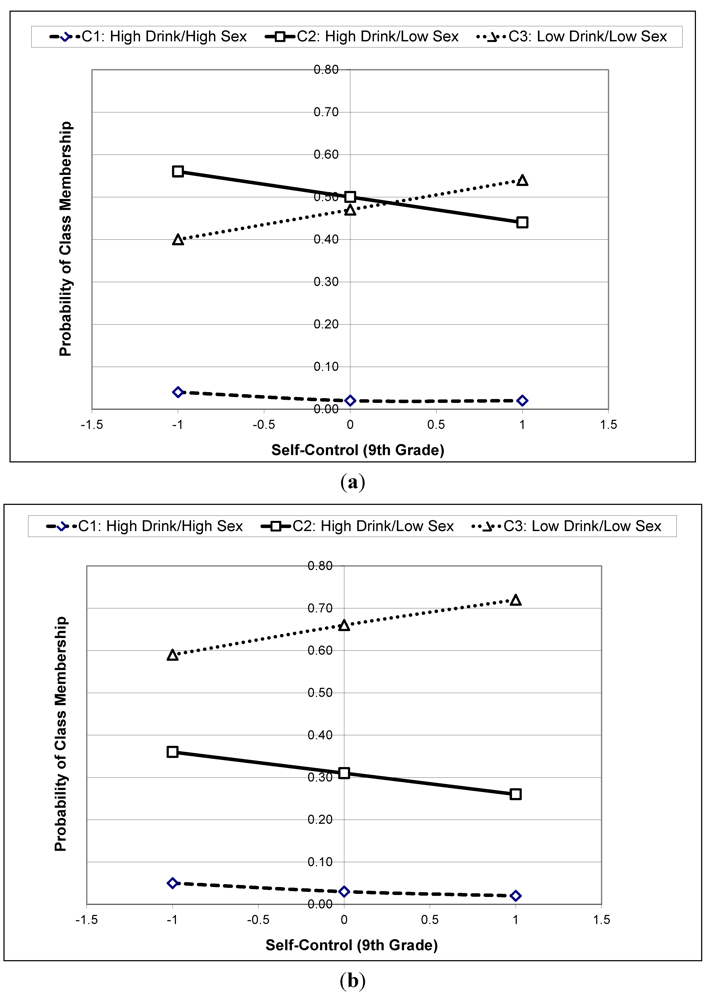
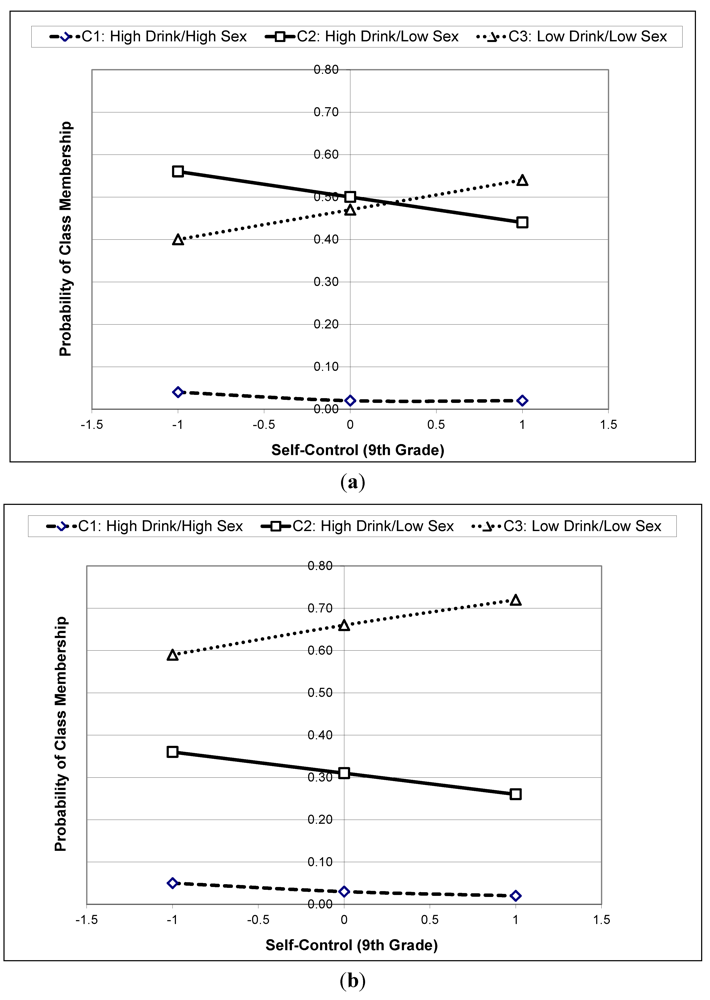
3.4. Results of the MNR Model
| Beta | p-value | Odds | ||||
|---|---|---|---|---|---|---|
| Relative to Class 3 | ||||||
| Class 1 | Class 2 | Class 1 | Class 2 | Class 1 | Class 2 | |
| Black (Reference = Other) | 0.171 | 0.824 | 0.540 | 0.002 | 1.186 | 2.280 |
| Psychosocial Markers (9th Grade) | ||||||
| Risk-Taking | −0.058 | 0.180 | 0.712 | 0.154 | 0.944 | 1.197 |
| Social Confidence | 0.247 | 0.108 | 0.091 | 0.407 | 1.280 | 1.114 |
| Self-Esteem | 0.390 | −0.197 | 0.108 | 0.210 | 1.477 | 0.821 |
| Self-Control | −0.571 | −0.275 | 0.002 | 0.101 | 0.565 | 0.760 |
| Covariates (9th Grade) | ||||||
| Grades In School | 0.215 | −0.034 | 0.128 | 0.818 | 1.240 | 0.967 |
| Free School Lunch | 0.102 | −0.426 | 0.721 | 0.094 | 1.107 | 0.653 |
| Nuclear Family | −0.611 | 0.081 | 0.038 | 0.731 | 0.543 | 1.084 |
4. Discussion
4.1. Implications for Self-Control and Addictive Behaviors
4.2. Strengths and Limitations
4.3. Directions for Future Research
Acknowledgements
References
- Substance Abuse and Mental Health Services Administration (SAMHSA), Results from the 2010 National Survey on Drug Use and Health: Summary of National Findings; US Department of Health and Human Services: Washington, DC, USA, 2011; NSDUH Series H-41; HHS Publication No. (SMA) 11-4658.
- Hingson, R.; Heeren, T.; Winter, M.; Wechsler, H. Magnitude of alcohol-related mortality and morbidity among U.S. college students ages 18–24: Changes from 1998 to 2001. Annu. Rev. Publ. 2005, 26, 259–279. [Google Scholar] [CrossRef]
- Perkins, H.W. Surveying the damage: A review of research on consequences of alcohol misuse in college populations. J. Stud. Alcohol 2002, S14, 91–100. [Google Scholar]
- O’Neill, S.E.; Parra, G.R.; Sher, K.J. Clinical relevance of heavy drinking during the college years: Cross-sectional and prospective perspectives. Psychol. Addict. Behav. 2001, 15, 350–359. [Google Scholar]
- Yi, H.; Williams, G.D.; Smothers, B.A. Trends in Alcohol-Related Fatal Traffic Crashes: United States, 1977–2002; Surveillance Report No. 69; National Institute on Alcohol Abuse and Alcoholism: Bethesda, MD, USA, 2004. [Google Scholar]
- Weinstock, H.; Berman, S.; Cates, W. Sexually transmitted diseases among American youth: Incidence and prevalence estimates, 2000. Perspect. Sex. Repro. H 2000, 36, 6–10. [Google Scholar]
- Futterman, D.C. HIV in adolescents and young adults: Half of all new infections in the United States. Top. HIV Med. 2005, 13, 101–105. [Google Scholar]
- Naimi, T.S.; Lipscomb, L.E.; Brewer, R.D.; Gilbert, B.C. Binge drinking in the preconception period and the risk of unintended pregnancy: Implications for women and their children. Pediatrics 2003, 111, 1136–1141. [Google Scholar]
- Cook, R.L.; Clark, D.B. Is there an association between alcohol consumption and sexually transmitted diseases? A systematic review. Sex Transm Dis. 2005, 32, 156–164. [Google Scholar]
- Cooper, M.L. Alcohol use and risky sexual behavior among college students and youth: Evaluating the evidence. J. Stud. Alcohol 2002, S14, 101–117. [Google Scholar]
- Leigh, B.C.; Stall, R. Substance use and risky sexual behavior for exposure to HIV: Issues in methodology. Am. Psychol. 1993, 48, 1035–1045. [Google Scholar]
- Hingson, R.W.; Strunin, L.; Berlin, B.M.; Heeren, T. Beliefs about AIDS, use of alcohol and drugs, and unprotected sex among Massachusetts adolescents. Am. J. Public Health 1990, 80, 295–299. [Google Scholar] [PubMed]
- Leigh, B.C. The relationship of sex-related alcohol expectancies to alcohol consumption and sexual behavior. Br. J. Addict. 1990, 85, 919–928. [Google Scholar]
- Brown, J.L.; Vanable, P.A. Alcohol use, partner type, and risky sexual behavior among college students: Findings from an event-level study. Addict. Behav. 2007, 12, 2940–2952. [Google Scholar]
- Cooper, M.L.; Peirce, R.S.; Huselid, R.F. Substance use and sexual risk taking among Black and White adolescents. Health Psychol. 1994, 13, 251–262. [Google Scholar]
- Dermen, K.H.; Cooper, M.L. Sex-related alcohol expectancies among adolescents. Psychol. Addict. Behav. 1994, 8, 161–168. [Google Scholar]
- Martens, M.P.; Page, J.C.; Mowry, E.S.; Damann, K.M.; Taylor, K.K.; Cimini, M.D. Differences between actual and perceived student norms: An examination of alcohol use, drug use, and sexual behavior. J. Am. Coll. Health 2006, 54, 295–300. [Google Scholar] [PubMed]
- Patrick, M.E.; Maggs, J.L. Profiles of motivations for alcohol use and sexual behavior among first-year university students. J. Adolesc. 2010, 33, 755–765. [Google Scholar]
- Steele, C.M.; Josephs, R.A. Alcohol myopia: Its prized and dangerous effects. Am. Psychol. 1990, 45, 921–933. [Google Scholar]
- Quinn, P.D.; Fromme, K. Self-regulation as a protective factor against risky drinking and sexual behavior. Psychol. Addict. Behav. 2010, 24, 376–385. [Google Scholar]
- Wills, T.A.; Ainette, M.G. Temperament, self-control, and adolescent substance use: a two-factor model of etiological processes. In Handbook of Drug Use Etiology: Theory, Methods, and Empirical Findings; Scheier, L.M., Ed.; American Psychological Association: Washington, DC, USA, 2010; pp. 127–146. [Google Scholar]
- Baumeister, R.F.; Vohs, K.D.; Tice, D.M. The strength model of self-control. Curr. Dir. Psychol. Sci. 2007, 16, 396–403. [Google Scholar]
- Gross, J. Emotion regulation: Past, present, future. Cogn. Emot. 1999, 13, 551–573. [Google Scholar] [CrossRef]
- Posner, M.I.; Rothbart, M.K. Developing mechanisms of self-regulation. Dev. Psychopathol. 2000, 12, 427–441. [Google Scholar]
- Sussman, S.; McCuller, W.J.; Dent, C.W. The associations of social self-control, personality disorders, and demographics with drug use among high-risk youth. Addict. Behav. 2003, 28, 1159–1166. [Google Scholar] [PubMed]
- Tangney, J.P.; Baumeister, R.F.; Boone, A.L. High self-control predicts good adjustment, less pathology, better grades, and interpersonal success. J. Persons. 2004, 72, 271–324. [Google Scholar]
- Otten, R.; Barker, E.D.; Maughan, B.; Arseneault, L.; Engels, R.C. Self-control and its relation to joint developmental trajectories of cannabis use and depressive mood symptoms. Drug Alcohol Depend. 2010, 112, 201–208. [Google Scholar]
- Baumeister, R.F.; Heatherton, T.F.; Tice, D.M. Losing Control: How and Why People Fail at Self-Regulation; Academic Press: San Diego, CA, USA, 1994. [Google Scholar]
- Calkins, S.D. Origins and outcomes of individual differences in emotional regulation. In Emotion Regulation: Behavioral and Biological Considerations, Monographs of the Society for Research in Child Development; Fox, N.A., Ed.; University of Chicago Press: Chicago, IL, USA, 1994; Volume 59, 2–3, Series 240. [Google Scholar]
- Fox, N.A.; Calkins, S.D.; Bell, M.A. Neural plasticity and development in the first two years of life: Evidence from cognitive and socioemotional domains of research. Dev. Psychopathol. 1994, 6, 677–696. [Google Scholar]
- Vazsonyi, A.T.; Huang, L. Where self-control comes from: On the development of self-control and its relationship to deviance over time. Dev. Psychol. 2010, 46, 245–257. [Google Scholar]
- Wills, T.A.; Ainette, M.G.; Stoolmiller, M.; Gibbons, F.X.; Shinar, O. Good self-control as a buffering agent for adolescent substance use: An investigation in early adolescence with time-varying covariates. Psychol. Addict. Behav. 2008, 22, 459–471. [Google Scholar]
- Engels, R.C.; Vermulst, A.A.; Dubas, J.S.; Bot, S.M.; Gerris, J. Long-term effects of family functioning and child characteristics on problem drinking in young adulthood. Eur. Addict. Res. 2005, 11, 32–37. [Google Scholar]
- Mestre, V.; Samper, P.; Nacher, M.J.; Tur, A.; Cortes, M.T. Psychological processes and family variables as prosocial behavior predictors in a sample of Spanish adolescents. Psychol. Rep. 2006, 98, 30–36. [Google Scholar]
- Beaver, K.M.; Ratchford, M.; Ferguson, C.J. Evidence of genetic and environmental effects on the development of low self-control. Crim. Justice Behav. 2009, 36, 1158–1172. [Google Scholar]
- Brannigan, A.; Gemmell, W.; Pevalin, D.J.; Wade, T.J. Self-control and social control in childhood misconduct and aggression: The role of family structure, hyperactivity, and hostile parenting. Can. J. Criminol. 2002, 44, 119–142. [Google Scholar]
- Wills, T.A.; Cleary, S.D.; Filer, M.; Shinar, O.; Mariani, J.; Spera, K. Temperament related to early-onset substance use: Test of a developmental model. Prev. Sci. 2001, 2, 145–163. [Google Scholar]
- Longshore, D.; Chang, E.; Messina, N. Self-control and social bonds: A combined control perspective on juvenile offending. J. Quant. Criminol. 2005, 21, 419–437. [Google Scholar]
- Wills, T.A.; Vaccaro, D.; McNamara, G. Life events, family support, and competence in adolescent substance use. Am. J. Commun. Psychol. 1992, 20, 349–374. [Google Scholar] [CrossRef]
- Windle, M. The difficult temperament in adolescence: Associations with substance use, family support, and problem behaviors. J. Clin. Psychol. 1991, 47, 310–315. [Google Scholar] [PubMed]
- O’Malley, P.; Johnston, L.D. Epidemiology of alcohol and other drug use among American college students. J. Stud. Alcohol 2002, 14, 23–39. [Google Scholar]
- Slutske, W.S.; Hunt-Carter, E.E; Nabors-Oberg, R.E.; Sher, K.J.; Bucholz, K.K.; Madden, P.A; Anokhin, A.; Heath, A.C. Do college students drink more than their non-college-attending peers? Evidence from a population-based longitudinal female twin study. J. Abnorm. Psychol. 2004, 113, 530–540. [Google Scholar] [PubMed]
- Fromme, K.; Corbin, W.R.; Kruse, M.I. Behavioral risks during the transition from high school to college. Dev. Psychol. 2008, 44, 1497–1504. [Google Scholar]
- Kost, K.; Henshaw, S.; Carlin, L. US Teenage Pregnancies,Births and Abortions: National and State Trends and Trends by Race and Ethnicity; Guttmacher Institute: New York, NY, USA, 2010. Available online: http://www.guttmacher.org/pubs/USTPtrends.pdf (accessed on 10 September 2011).
- Miller, W.C.; Ford, C.A.; Morris, M.; Handcock, M.S.; Schmitz, J.L.; Hobbs, M.M.; Cohen, M.S.; Harris, K.M.; Udry, J.R. Prevalence of chlamydial and gonococcal infections among young adults in the United States. J. Am. Med. Assoc. 2004, 291, 2229–2236. [Google Scholar]
- Diagnoses of HIV infection and AIDS in the United States and Dependent Areas, 2009; HIV Surveillance Report; Centers for Diseases and Control and Prevention: Atlanta, GA, USA, 2011; 21. Available online: http://www.cdc.gov/hiv/surveillance/resources/reports/2009report/index.htm (accessed on 10 September 2011).
- Sobell, L.C.; Sobell, M.B. Timeline follow-back: A technique for assessing self-reported alcohol consumption. In Measuring Alcohol Consumption; Litten, R., Allen, J., Eds.; The Humana Press Inc.: Rockville, MD, USA, 1992; pp. 207–224. [Google Scholar]
- Weinhardt, L.S.; Carey, M.P.; Maisto, S.A.; Carey, K.B.; Cohen, M.M.; Wickramasinghe, S.M. Reliability of the timeline followback sexual behavior interview. Ann. Behav. Med. 1998, 20, 25–30. [Google Scholar]
- Sobell, L.C.; Brown, J.; Leo, G.I.; Sobell, M.B. The reliability of the Alcohol Timeline Followback when administered by telephone and by computer. Drug Alcohol Depend. 1996, 42, 49–54. [Google Scholar]
- Eysenck, S.B.J.; Eysenck, H.J. The place of impulsiveness in a dimensional system of personality description. Br. J. Social. Clin. Psychol. 1977, 16, 57–68. [Google Scholar]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Kendall, P.C.; Wilcox, L.E. Self-control in children: Development of a rating scale. J. Consult. Clin. Psychol. 1979, 47, 1020–1029. [Google Scholar]
- Storr, C.L.; Zhou, H.; Liang, K.-Y.; Anthony, J.C. Empirically derived latent classes of tobacco dependence syndromes observed in recent-onset tobacco smokers: Epidemiological evidence from a national probability sample survey. Nicotine Tob. Res. 2004, 6, 533–545. [Google Scholar]
- Hasking, P.A.; Scheier, L.M.; Abdallah, A.B. The three latent classes of adolescent delinquency and the risk factors for membership in each class. Aggress. Behav. 2010, 37, 19–35. [Google Scholar]
- Fergusson, D.M.; Horwood, L.J.; Lynskey, M.T. The comorbidities of adolescent problem behaviors: A latent class model. J. Abnorm. Child Psych. 1994, 22, 339–354. [Google Scholar]
- Collins, L.M.; Graham, J.W.; Long, J.D.; Hansen, W.B. Crossvalidation of latent class models of early substance use onset. Multivar. Behav. Res. 1994, 29, 165–183. [Google Scholar]
- Coffman, D.L.; Patrick, M.E.; Palen, L.A.; Rhoades, B.L.; Ventura, A.K. Why do high school seniors drink? Implications for a targeted approach to intervention. Prev. Sci. 2007, 8, 241–248. [Google Scholar]
- Flaherty, B.P. Assessing reliability of categorical substance use measures with latent class analysis. Drug Alcohol Depend. 2002, 68, S7–S20. [Google Scholar]
- Clogg, C.C.; Goodman, L.A. Latent structure analysis of a set of multidimensional contingency tables. J. Am. Stat. Assoc. 1984, 79, 762–771. [Google Scholar]
- Hagenaars, J.A.; McCutcheon, A.L. Applied Latent Class Analysis; Cambridge University Press: Cambridge, UK, 2002. [Google Scholar]
- Schwarz, G. Estimating the dimension of a model. Ann. Stat. 1978, 6, 461–464. [Google Scholar]
- Akaike, H. Factor analysis and the AIC. Psychometrika 1987, 52, 317–332. [Google Scholar] [CrossRef]
- Singer, J.D.; Willett, J.B. Applied Longitudinal Data Analysis: Modeling Change and Even Occurrence; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Agresti, A. Categorical Data Analysis; John Wiley & Sons: New York, NY, USA, 1990. [Google Scholar]
- Haberman, S.J. Analysis of Quantitative Data. Vol. 2. New Developments; Academic Press: New York, NY, USA, 1979. [Google Scholar]
- Kotz, S.; Johnson, N.L. Encyclopedia of Statistical Sciences; John Wiley & Sons: New York, NY, USA, 2006. [Google Scholar]
- Garrett, E.S.; Zeger, S.L. Latent class model diagnosis. Biometrics 2000, 56, 1055–1067. [Google Scholar]
- Arnett, J.J. Emerging adulthood: A theory of development from the late teens through the twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar]
- Raffaelli, M.; Crockett, L.J. Sexual risk taking in adolescence: The role of self-regulation and attraction to risk. Dev. Psychol. 2003, 39, 1036–1046. [Google Scholar]
- Wills, T.A.; Stoolmiller, M. The role of self-control in early escalation of substance use: A time-varying analysis. J. Consult. Clin. Psychol. 2002, 70, 986–997. [Google Scholar]
- Sussman, S.; Leventhal, A.; Bluthenthal, R.N.; Freimuth, M.; Forster, M.; Ames, S.L. A framework for the specificity of addictions. Int. J. Environ. Res. Public Health 2011, 8, 3399–3415. [Google Scholar]
- Wills, T.A.; Dishion, T.J. Temperament and adolescent substance use: A transactional analysis of emerging self-control. J. Clin. Child Adolesc. 2004, 33, 69–81. [Google Scholar]
- Hofmann, W.; Friese, M.; Strack, F. Impulse and self-control from a dual systems perspective. Perspect Psychol. Sci. 2009, 4, 162–176. [Google Scholar]
- Friese, M.; Hofmann, W.; Wiers, R.W. On taming horses and strengthening riders: Recent developments in research on interventions to improve self-control in health behaviors. Self Identity 2011, 10, 336–351. [Google Scholar]
- Baumeister, R.F.; Gailliot, M.; DeWall, C.N.; Oaten, M. Self-regulation and personality: How interventions increase regulatory success, and how depletion moderates the effects of traits on behavior. J. Personal. 2006, 74, 1773–1801. [Google Scholar]
- Lubke, G.H.; Muthén, B.O. Investigating population heterogeneity with factor mixture models. Psychol. Methods 2005, 10, 21–39. [Google Scholar]
- Nagin, D.S.; Tremblay, R.E. Developmental trajectory groups: Fact or a useful statistical fiction? Criminology 2005, 43, 873–904. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Griffin, K.W.; Scheier, L.M.; Acevedo, B.; Grenard, J.L.; Botvin, G.J. Long-Term Effects of Self-Control on Alcohol Use and Sexual Behavior among Urban Minority Young Women. Int. J. Environ. Res. Public Health 2012, 9, 1-23. https://doi.org/10.3390/ijerph9010001
Griffin KW, Scheier LM, Acevedo B, Grenard JL, Botvin GJ. Long-Term Effects of Self-Control on Alcohol Use and Sexual Behavior among Urban Minority Young Women. International Journal of Environmental Research and Public Health. 2012; 9(1):1-23. https://doi.org/10.3390/ijerph9010001
Chicago/Turabian StyleGriffin, Kenneth W., Lawrence M. Scheier, Bianca Acevedo, Jerry L. Grenard, and Gilbert J. Botvin. 2012. "Long-Term Effects of Self-Control on Alcohol Use and Sexual Behavior among Urban Minority Young Women" International Journal of Environmental Research and Public Health 9, no. 1: 1-23. https://doi.org/10.3390/ijerph9010001