Restaurant and Bar Owners’ Exposure to Secondhand Smoke and Attitudes Regarding Smoking Bans in Five Chinese Cities

Abstract
:
1. Introduction
2. Methods
3. Results
3.1. Smoking Policy and Exposure to Secondhand Smoke
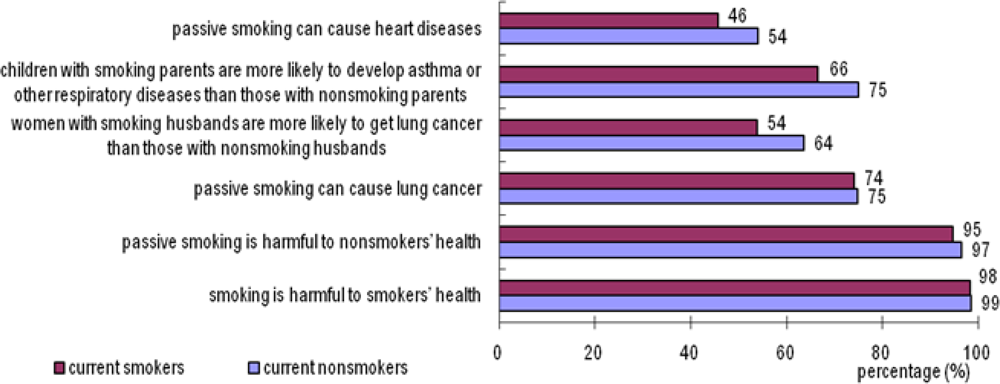
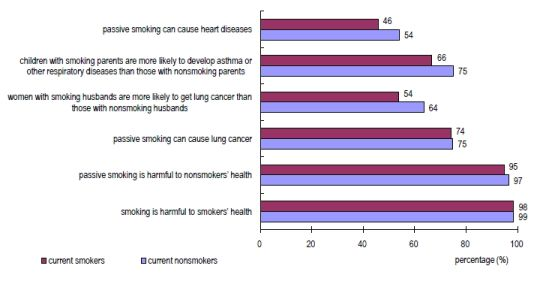
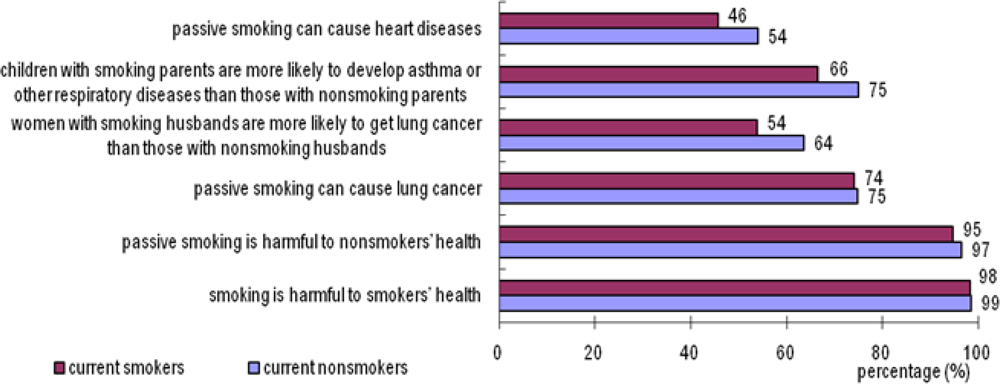
3.2. Knowledge of Tobacco-Related Health Effects
3.3. Attitudes Towards Smoking Bans in Hospitality Venues
4. Discussion
5. Study Limitations and Strengths
6. Conclusions
Acknowledgments
References
- Cal/EPA. Proposed Identification of Environmental Tobacco Smoke as a Toxic Air Contaminant; California Environmental Protection Agency Air Resources Board and Office of Environmental Health Hazard Assessment: Sacramento, CA, USA, 2005. [Google Scholar]
- IARC. Monographs on the Evaluation of Carcinogenic Risks to Humans. Tobacco Smoke and Involuntary Smoking, Volume 83; IARC: Lyon, France, 2004. [Google Scholar]
- US Department of Health and Human Services (USDHHS). The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2006. [Google Scholar]
- Lightwood, JM; Glantz, SA. Declines in acute myocardial infarction after smoke-free laws and individual risk attributable to secondhand smoke. Circulation 2009, 120, 1373–1397. [Google Scholar]
- Meyers, DG; Neuberger, JS; He, J. Cardiovascular effect of bans on smoking in public places. J. Amer. Coll. Cardiol 2009, 54, 1249–1255. [Google Scholar]
- Ong, MK; Glantz, SA. Cardiovascular health and economic effects of smoke-free workplaces. Amer. J. Med 2004, 117, 32–38. [Google Scholar]
- Sargent, RP; Shepard, RM; Glantz, SA. Reduced incidence of admissions for myocardial infarction associated with public smoking ban: Before and after study. Brit. Med. J 2004, 328, 977–980. [Google Scholar]
- American Nonsmokers’ Rights Foundation (ANRF). Summary of 100% Smokefree State Laws and Population Protected by 100% U.S. Smokefree Laws; American Nonsmokers’ Rights Foundation: Berkeley, CA, USA, 2010. Available on line: http://www.nosmoke.org/pdf/SummaryUSPopList.pdf (accessed on 1 April 2011).
- WHO. World Health Organization Report on the Global Tobacco Epidemic, 2009: Implementing Smoke-Free Environments; WHO: Geneva, Switzerland, 2009. Available online: http://www.who.int/tobacco/mpower/2009/en/ (accessed on March 2010).
- CDC. Smoking and Tobacco Use: GATS: Fact Sheet: China: 2010; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2010. Available online: http://www.cdc.gov/tobacco/global/gats/countries/wpr/fact_sheets/china/2010/index.htm (accessed on 2 May 2011).
- Li, Y; Jiang, Y; Yang, Y; Nan, Y; Feng, G; Zhou, G; Li, M; Zhang, C. Current situation of law and regulation for banning smoking in public places in China. J. Environ. Health 2007, 24, 221–223. [Google Scholar]
- Ministry of Health. China Tobacco Control Report: 2007; Ministry of Health: Beijing, China, 2007. [Google Scholar]
- Beijing Government. Regulations on Smoking in Public Places in Beijing, Rule 204; Beijing Government: Beijing, China, 2008; Volume 204. [Google Scholar]
- Yang, G; Ma, J; Liu, N; Zhou, L. Smoking and passive smoking in China, 2002. Chin. J. Epidemiol 2005, 2, 77–83. [Google Scholar]
- IARC. Handbooks of Cancer Prevention, Tobacco Control, Vol. 13: Evaluating the Effectiveness of Smoke-Free Policies; IARC: Lyon, France, 2009. [Google Scholar]
- National Bureau of Statistics of China. China Statistic Year Book 2007; National Bureau of Statistics of China: Beijing, China, 2007. Available online: http://www.stats.gov.cn/tjsj/ndsj/2007/indexee.htm (accessed on 11 October 2010).
- Liu, R; Yang, Y; Travers, M; Fong, GT; O’Connor, RJ; Hyland, A; Li, L; Nan, Y; Feng, G; Li, Q; et al. A cross-sectional study on levels of second-hand smoke in restaurants and bars in five cities in China. Tob. Control 2010, 19, i24–i29. [Google Scholar]
- Yang, Y; Jiang, Y; Wu, X; Feng, G. Analysis of policies on banning smoking in public places and their implementation in China. Chin. J. Health Edu 2008, 24, 657–660. [Google Scholar]
- National Bureau of Statistics of China. China Labour Statistical Yearbook 2006; National Bureau of Statistics of China: Beijing, China, 2006. Available online: http://www.stats.gov.cn/tjsj/ndsj/laodong/2006/2006laodong.htm (accessed on 2 May 2011).
- Liu, R; Yang, Y; Liu, X; Chang, A; Gong, J; Zhao, B; Liu, T; Jiang, Y; Hyland, A; Li, Q. Knowledge and attitudes towards secondhand smoke among hospitality patronage in five cities in China. Chin. J. Epidemiol 2008, 29, 421–425. [Google Scholar]
- Fong, GT; Hammond, D; Jiang, YA; Li, QA; Quah, ACK; Driezen, P; Yan, M. Perceptions of tobacco health warnings in China compared with picture and text-only health warnings from other countries: An experimental study. Tob. Control 2010, 19, i69–i77. [Google Scholar]
- ASHRAE. ASHRAE Position Document on Environmental Tobacco Smoke; American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc: Atlanta, GA, USA, 2008. [Google Scholar]
- Hyland, A; Vena, C; Cummings, MK. A review of the economic effect of smoke-free restaurant and bar policies on the hospitality economy. Epidemiology 2000, 11, S145. [Google Scholar]
- Ma, SJ; Hoang, MA; Samet, JM; Wang, JF; Mei, CZ; Xu, XF; Stillman, FA. Myths and attitudes that sustain smoking in China. J. Health Commun 2008, 13, 654–666. [Google Scholar]

{kind=link}
{kind=link}
| Total n (%) | Beijing n (%) | Wuhan n (%) | Xi’an n (%) | Kunming n (%) | Guiyang n (%) | χ2 test p value | |
|---|---|---|---|---|---|---|---|
| Total | 814 (100.0) | 161 (100.0) | 172 (100.0) | 161 (100.0) | 160 (100.0) | 160 (100.0) | |
| Type of Establishment | |||||||
| Chinese dining | 506 (62.2) | 95 (59.0) | 112 (65.1) | 100 (62.1) | 100 (62.5) | 99 (61.9) | 0.996 |
| Chinese fast food | 58 (7.1) | 17 (10.6) | 10 (5.8) | 10 (6.2) | 10 (6.3) | 11 (6.9) | |
| Western dining | 52 (6.4) | 11 (6.8) | 10 (5.8) | 10 (6.2) | 10 (6.3) | 11 (6.9) | |
| Western fast food | 49 (6.0) | 11 (6.8) | 10 (5.8) | 10 (6.2) | 9 (5.6) | 9 (5.6) | |
| Bar | 149 (18.3) | 27 (16.8) | 30 (17.4) | 31 (19.3) | 31 (19.4) | 30 (18.8) | |
| Gender | |||||||
| Male | 413 (50.7) | 93 (57.8) | 71 (41.3) | 84 (52.2) | 82 (51.3) | 83 (51.9) | 0.049 |
| Female | 399 (49.0) | 67 (41.6) | 100 (58.1) | 77 (47.8) | 78 (48.8) | 77 (48.1) | |
| Missing | 2 (0.2) | 1 (0.6) | 1 (0.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Age | |||||||
| ≤35 | 571 (70.0) | 111 (68.9) | 116 (67.4) | 109 (67.7) | 117 (73.1) | 118 (73.8) | 0.692 |
| >35 | 239 (29.5) | 50 (31.1) | 54 (31.4) | 50 (31.1) | 43 (26.9) | 42 (26.3) | |
| Missing | 4 (0.5) | 0 (0.0) | 2 (1.2) | 2 (1.2) | 0 (0.0) | 0 (0.0) | |
| Education | |||||||
| ≤High school | 444 (54.5) | 85 (52.8) | 100 (58.1) | 91 (56.5) | 98 (61.3) | 70 (43.8) | 0.016 |
| >High School | 368 (45.2) | 76 (47.2) | 70 (40.7) | 70 (43.5) | 62 (38.8) | 90 (56.3) | |
| Missing | 2 (0.2) | 0 (0.0) | 2 (1.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Current Smoking | |||||||
| No | 525 (64.5) | 106 (65.8) | 121 (70.3) | 99 (61.5) | 100 (62.5) | 99 (61.9) | 0.338 |
| Yes | 287 (35.3) | 54 (33.5) | 50 (29.1) | 62 (38.5) | 60 (37.5) | 61 (38.1) | |
| Missing | 2 (0.2) | 1 (0.6) | 1 (0.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Days Exposed | Restaurants Smoking policy at work | Bars Smoking policy at work | ||||||
|---|---|---|---|---|---|---|---|---|
| Prohibit % (n) | Restrict % (n) | Allow % (n) | Total % (n) | Prohibit % (n) | Restrict % (n) | Allow% (n) | Total % (n) | |
| None | 51.1 (24) | 14.4 (16) | 6.1 (13) | 14.3 (53) | 0.0 (0) | 17.6 (3) | 7.7 (2) | 10.2 (5) |
| 1–2 | 21.3 (10) | 15.3 (17) | 9.0 (19) | 12.4 (46) | 33.3 (2) | 17.6 (3) | 11.5 (3) | 16.3 (8) |
| 3–4 | 10.6 (5) | 18.0 (20) | 9.9 (21) | 12.4 (46) | 0.0 (0) | 17.6 (3) | 3.8 (1) | 8.2 (4) |
| 5–7 | 17.0 (8) | 52.3 (58) | 75.0 (159) | 60.8 (225) | 66.7 (4) | 47.1 (8) | 76.9 (20) | 65.3 (32) |
| Total | 100.0 (47) | 100.0 (111) | 100.0 (212) | 100.0 (370) | 100.0 (6) | 100.0 (17) | 100.0 (26) | 100.0 (49) |
| Smokers (%) | Non-smokers (%) | All subjects (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Prohibit | Restrict | Total | Prohibit | Restrict | Total | Prohibit | Restrict | Total | |
| School | 84.3 | 15.0 | 99.3 | 87.6 | 11.8 | 99.4 | 86.4 | 13.0 | 99.4 |
| Public vehicle | 87.4 | 10.1 | 97.5 | 87.4 | 11.2 | 98.6 | 87.4 | 10.8 | 98.2 |
| Hospital | 69.6 | 30.4 | 100 | 74.7 | 24.8 | 99.4 | 73.3 | 26.3 | 99.6 |
| Office | 49.3 | 45.1 | 94.4 | 62.7 | 32.8 | 95.5 | 58.1 | 36.9 | 95.0 |
| Restaurant | 10.8 | 64.7 | 75.5 | 20.2 | 63.2 | 83.4 | 16.8 | 63.8 | 80.6 |
| Bar | 6.3 | 46.9 | 53.2 | 14.1 | 52.7 | 66.8 | 11.4 | 50.3 | 61.7 |
| total | What kind of smoking policy do you think restaurants/bars should have? a n (%) | Willing to do so b n (%) | ||||||
|---|---|---|---|---|---|---|---|---|
| restaurants | bars | |||||||
| prohibit | restrict | allow | prohibit | restrict | allow | |||
| Total | 814 | 137 (16.8) | 519 (63.7) | 106 (13.0) | 92 (11.3) | 411 (50.6) | 195 (24.0) | 433 (53.3) |
| City | ||||||||
| Beijing | 161 | 36 (22.4) | 106 (65.8) | 11 (6.8) | 26 (16.3) | 88 (55.0) | 21 (13.1) | 108 (67.9) |
| Wuhan | 172 | 26 (15.2) | 89 (52.0) | 45 (26.3) | 20 (11.7) | 67 (39.2) | 67 (39.2) | 83 (48.3) |
| Xi’an | 161 | 36 (22.4) | 100 (62.1) | 11 (6.8) | 18 (11.2) | 78 (48.4) | 32 (19.9) | 76 (47.2) |
| Kunming | 160 | 18 (11.3) | 107 (66.9) | 26 (16.3) | 11 (6.9) | 81 (50.6) | 51 (31.9) | 76 (47.5) |
| Guiyang | 160 | 21 (13.1) | 117 (73.1) | 13 (8.1) | 17 (10.6) | 97 (60.6) | 24 (15.0) | 90 (56.3) |
| Type of Establishment | ||||||||
| Chinese dining | 506 | 87 (17.2) | 312 (61.7) | 71 (14) | 63 (12.5) | 252 (49.9) | 110 (21.8) | 270 (53.6) |
| Chinese fast food | 58 | 15 (25.9) | 37 (63.8) | 4 (6.9) | 10 (17.2) | 31 (53.4) | 12 (20.7) | 32 (55.2) |
| Western dining | 52 | 3 (5.9) | 42 (82.4) | 4 (7.8) | 3 (5.9) | 29 (56.9) | 12 (23.5) | 36 (69.2) |
| Western fast food | 49 | 17 (34.7) | 28 (57.1) | 3 (6.1) | 8 (16.3) | 26 (53.1) | 11 (22.4) | 38 (77.6) |
| Bar | 149 | 15 (10.1) | 100 (67.1) | 24 (16.1) | 8 (5.4) | 73 (49.0) | 50 (33.6) | 57 (38.3) |
| Gender | ||||||||
| Male | 413 | 64 (15.5) | 259 (62.9) | 58 (14.1) | 45 (10.9) | 204 (49.5) | 111 (26.9) | 210 (51.0) |
| Female | 399 | 73 (18.3) | 259 (64.9) | 47 (11.8) | 47 (11.8) | 206 (51.8) | 83 (20.9) | 223 (56.0) |
| Age | ||||||||
| ≤35 | 571 | 84 (14.7) | 385 (67.4) | 66 (11.6) | 59 (10.3) | 306 (53.6) | 127 (22.2) | 266 (46.7) |
| >35 | 238 | 51 (21.4) | 132 (55.5) | 40 (16.8) | 32 (13.5) | 104 (43.9) | 67 (28.3) | 111 (46.4) |
| Education | ||||||||
| ≤High school | 444 | 80 (58.4) | 274 (52.9) | 30 (16.2) | 22 (11.9) | 79 (42.7) | 58 (31.4) | 96 (51.9) |
| >High school | 367 | 57 (41.6) | 244 (47.1) | 37 (14.3) | 37 (14.3) | 134 (51.9) | 55 (21.3) | 139 (53.7) |
| Current smoking | ||||||||
| Yes | 287 | 106 (20.2) | 332 (63.2) | 62 (11.8) | 74 (14.1) | 276 (52.7) | 99 (18.9) | 125 (43.6) |
| No | 525 | 31 (10.8) | 185 (64.7) | 44 (15.4) | 18 (6.3) | 134 (46.9) | 95 (33.2) | 308 (58.9) |
| Knowledge scores | ||||||||
| 0–3 | 221 | 29 (13.1) | 132 (59.7) | 38 (17.2) | 15 (6.8) | 98 (44.3) | 60 (27.1) | 101 (45.7) |
| 4–6 | 592 | 108 (18.2) | 387 (65.4) | 68 (11.5) | 77 (13.0) | 313 (53.0) | 135 (22.8) | 332 (56.1) |
| Banning smoking would not reduce revenues | ||||||||
| Disagree/DNK c | 447 | 42 (9.4) | 295 (66.0) | 72 (16.1) | 34 (7.6) | 219 (49.0) | 121 (27.1) | 194 (43.4) |
| Agree | 365 | 95 (26.0) | 223 (61.1) | 34 (9.3) | 58 (15.9) | 191 (52.5) | 74 (20.3) | 238 (65.6) |
| Support prohibiting or restricting smoking in restaurants OR (95% CI) a | Support prohibiting or restricting smoking in bars OR (95% CI) a | Willing to prohibit or restrict smoking in their own venues OR (95% CI) a | |
|---|---|---|---|
| City | |||
| Beijing | (reference) | (reference) | (reference) |
| Wuhan | 0.3 (0.1, 0.5) *** | 0.4 (0.3, 0.6) *** | 0.4 (0.3, 0.7) *** |
| Xi’an | 0.8 (0.4, 1.5) | 0.6 (0.4, 0.99) ** | 0.4 (0.3, 0.7) *** |
| Kunming | 0.6 (0.3, 1.0) | 0.6 (0.4, 0.9) ** | 0.5 (0.3, 0.7) *** |
| Guiyang | 1.0 (0.5, 2.0) | 1.1 (0.7, 1.8) | 0.7 (0.4, 1.1) |
| Type of Establishment | |||
| Chinese dining | (reference) | — | (reference) |
| Chinese fast food | 2.3 (0.9, 5.6) | — | 0.9 (0.5, 1.7) |
| Western dining | 1.7 (0.7, 4.2) | — | 1.9 (1.01, 3.7) * |
| Western fast food | 2.5 (0.8, 7.5) | — | 2.6 (1.3, 5.3) ** |
| Bar | 1.0 (0.6, 1.6) | — | 0.6 (0.4, 0.9) ** |
| Age | |||
| ≤35 | (reference) | (reference) | — |
| >35 | 0.7 (0.5, 1.1) | 0.8 (0.6, 1.1) | — |
| Current smoking | |||
| No | (reference) | (reference) | (reference) |
| Yes | 0.6 (0.4, 0.9) ** | 0.6 (0.4, 0.8) *** | 0.6 (0.4, 0.8) *** |
| Knowledge scores | |||
| 0–3 | (reference) | (reference) | (reference) |
| 4–6 | 1.9 (1.3, 2.9) *** | 1.9 (1.3, 2.6) *** | 1.4 (1.01, 2.0) * |
| Banning smoking would not reduce revenues | |||
| Disagree/DNK b | (reference) | (reference) | (reference) |
| Agree | 2.2 (1.5, 3.2) *** | 1.6 (1.2, 2.2) *** | 2.3 (1.7, 3.1) *** |
© 2011 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Liu, R.; Hammond, S.K.; Hyland, A.; Travers, M.J.; Yang, Y.; Nan, Y.; Feng, G.; Li, Q.; Jiang, Y. Restaurant and Bar Owners’ Exposure to Secondhand Smoke and Attitudes Regarding Smoking Bans in Five Chinese Cities. Int. J. Environ. Res. Public Health 2011, 8, 1520-1533. https://doi.org/10.3390/ijerph8051520
Liu R, Hammond SK, Hyland A, Travers MJ, Yang Y, Nan Y, Feng G, Li Q, Jiang Y. Restaurant and Bar Owners’ Exposure to Secondhand Smoke and Attitudes Regarding Smoking Bans in Five Chinese Cities. International Journal of Environmental Research and Public Health. 2011; 8(5):1520-1533. https://doi.org/10.3390/ijerph8051520
Chicago/Turabian StyleLiu, Ruiling, S. Katharine Hammond, Andrew Hyland, Mark J. Travers, Yan Yang, Yi Nan, Guoze Feng, Qiang Li, and Yuan Jiang. 2011. "Restaurant and Bar Owners’ Exposure to Secondhand Smoke and Attitudes Regarding Smoking Bans in Five Chinese Cities" International Journal of Environmental Research and Public Health 8, no. 5: 1520-1533. https://doi.org/10.3390/ijerph8051520