1. Introduction
Evidence is emerging that secondhand smoke (SHS) exposure during pregnancy increases the risk of low birth weight among the infants of non-smoking women. This may be of particular importance in Jordan due to the high prevalence of SHS exposure experienced by non smoking women. Although SHS is a known cause of premature death and disease among women and children [
1], most studies examining the relationship between SHS exposure in women and children have been conducted in developed countries where exposure is relatively low and with patients for whom maternal smoking during pregnancy is relatively high [
2–
5]. In contrast, effects of SHS exposure (including product type, magnitude, and time of exposure) among women and children in developing countries has not been well studied even though smoking prevalence is much higher in those countries because tobacco control initiatives are minimal [
6]. The lack of data about the impact of SHS exposure on women’s and children’s health outcomes in developing countries with a high smoking prevalence among the general population and low maternal smoking prevalence during pregnancy makes it difficult for researchers, lawmakers, health professionals, and families to make informed decisions about tobacco prevention. Globally, about one-sixth of all newborns are low birth weight (LBW) (LBW, <2,500 grams), which is the single most important underlying risk factor for neonatal deaths [
7,
8]. In undeveloped countries, including Jordon, only about half of the newborns are weighed at birth, and gestational age is known for a smaller proportion of those newborns. Moreover, LBW babies who survive the critical neonatal period may suffer long term impaired physical and mental growth. Therefore, an early identification and prompt referral of LBW newborns is vital in preventing neonatal deaths and long term physical and mental impairment.
1.2. Hypotheses
In this prospective survey study, the influence of SHS exposure on neonatal birth weight and the risk of having a LBW neonate as a result of Jordanian non-smoking women pregnant women being exposed to SHS were investigated. The research hypotheses were:
Among non-smoking Jordanian women giving birth at a major medical center in northern Jordan:
Increasing the reported average number of SHS exposure hours per week from home, work, and outside in the first, second, and third trimesters lead to decreasing the neonatal birth weight significantly after controlling for covariates.
Women who reported higher average number of SHS exposure hours per week from home, work, and outside in the first, second, and third trimesters were at significantly greater risk for having a LBW neonate than women who reported lower average number of SHS exposure hours after controlling for covariates.
1.3. Health and Smoking Behavior in Jordan
Jordan is a developing, low-to-middle income country that is advancing and adapting to a twenty-first century economy. It is geographically situated between Saudi Arabia, Iraq, Israel, and Syria and thus is directly embedded in the culture, societal trends, and concerns of the Middle East as a whole. Administratively, Jordan has three regions with 12 governorates. The gross domestic product is $8.9 billion, which yields a mean of $1,744 per capita [
9–
11].
Jordanians view smoking as a social habit; having coffee and cigarettes with friends and family members is deeply rooted in the culture. From 2002 to 2006, 50% of adult men and 11% of adult women smoked [
12–
14]. A recent series of surveys in Jordan estimated smoking rates of 24.9% among youth with a 76.3% self-report of SHS exposure [
15], 22.4% among male physicians [
16], and 28.6% among college students [
17,
18], which rose to 35% in 2008 [
19]. Furthermore, there are no restrictive antismoking regulations in the workplace. Generally, women do not encourage their husbands or visitors to smoke outside their homes or in a different room.
Jordan and many other Middle Eastern countries lack systematic knowledge and surveillance data about the harm and economic effects of smoking and second-hand smoke exposure. Unfortunately, many aspects and social attitudes of using tobacco are shaped by their acceptance in Jordanian Arab culture [
20]. Therefore, this study concerning the magnitude of exposure and the harmful effects of SHS on neonate and newborn weight may provide impetus for Jordanian society and policy makers to develop guidelines to reduce SHS exposure.
1.4. Theoretical Framework
Few reports chronicling the possible influence of SHS exposure among non-smoking Jordanian pregnant women on birth weight in this population were found. Further, LBW neonates have a greater risk for mortality and morbidity in the first week of life [
21]. Therefore, it is imperative to further examine the dangers associated with this potential environmental risk. This is especially important in countries, such as Jordan, where there is a high prevalence of smoking in the male population [
22–
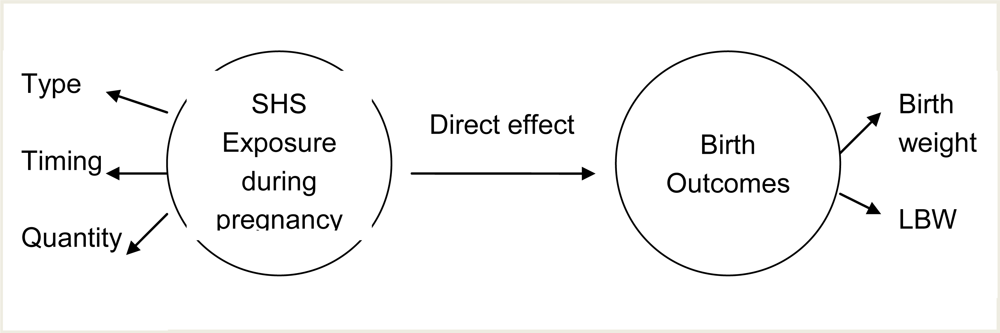
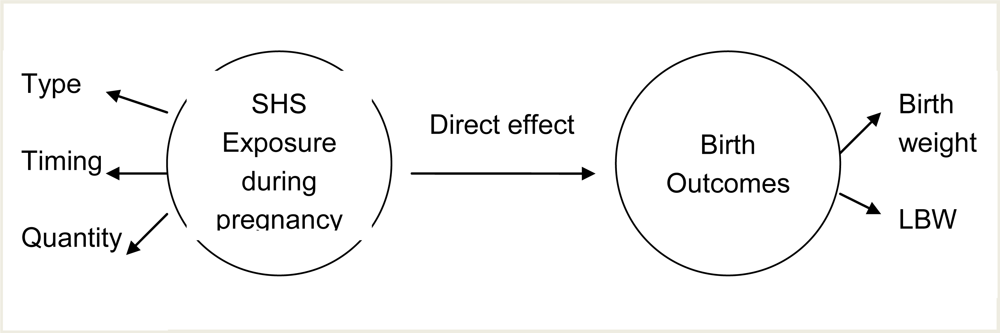
24]. Moreover, most researchers have focused on birth weight and SHS exposure during pregnancy in general. Further knowledge is needed about the type of SHS exposure (at home, work, or outside home/work), the quantity of SHS exposure (average number of exposure hours per week), and the timing of SHS exposure (first, second, and third trimesters). Two major variables are involved in the relationship between SHS exposure during pregnancy and birth outcome. (See
Figure 1.) These variables are: SHS exposure during pregnancy, and birth outcome.
Secondhand smoke exposure. Pregnant women are usually exposed to SHS in different places for different durations and at different times during pregnancy. For the purpose of this study, the assessment of SHS exposure included three major components: the type of SHS exposure (at home, work, or outside), the quantity of SHS exposure (average number of exposure hours per week), and the timing of the SHS exposure (first, second, and third trimesters).
Direct effect of SHS exposure. The toxins in SHS directly cause harmful effects in the fetus [
25–
28]. Nicotine is known to be vasoactive and is thought to reduce fetal circulation via the placenta [
29–
34]. Cotinine, a major metabolite of nicotine, has been measured in follicular fluid and amniotic fluid. Carbon monoxide is known to deplete fetal oxygen supplies [
23,
35–
37].
Birth outcome. For the purpose of this study, birth outcomes included low birth weight and actual birth weight. Birth weight was defined as the number of grams that represented the neonate’s weight at birth. Low birth weight was defined as a birth weight of less than 2,500 grams
1.5. Potential Covariates of Newborn Weight
The rate of newborn, infant, and early childhood growth is a sensitive indicator on the impact of SHS exposure. Multiple maternal and neonatal factors are also associated with birth weight. Two separate secondary data analyses of survey data for 35 developing countries showed that maternal education and household wealth have a strong positive association with height for age and early life diseases, with substantial shared variance between these two variables in explaining child height for age [
38,
39]. Clearly, factors such as parental stature and gestational age have significant influences on birth weight. The incidence of LBW in neonates is significantly higher for first pregnancies, high maternal weight gain during pregnancy, maternal age less than ≤18 or ≥35 years, maternal alcohol or drug use, and for female neonates [
38,
40–
44].
3. Results
3.1. Maternal and Neonate’s Characteristics
The mean age of the study participants was 28 years (SD = 5.52), the mean height was 160.2 centimeters (SD = 6.25), the mean years of education was 11.4 years (SD = 2.79), and the mean total family income was 2,888 $US per month (SD = 105.22). 42.3% of the study participants reported having an education level of less than high school; 33.3% completed high school education, and 24.3% completed post high school education. With regard to the father’s education level, 45% reported having an education level of less than high school; 32.3% completed high school education, and 22.6% completed post high school education. Only 10% of the study participants reported having jobs outside home (
n = 31). Many of the demographics fit the national profile as the mean height for women is 160 Centimeters, and 55% of women have more than high school education. However the reported total family income was lower than the national average ($ 4,820) [
10].
3.2. Maternal Obstetric History and Current Delivery
The mean weight before pregnancy of the study participants was 63 kilograms (SD = 10.53); the mean weight gain during pregnancy was 11.1 kilograms (SD = 3.48); the mean number of pregnancies was 3.5 pregnancies (SD = 2.24); and the mean number of living children prior to the subject neonate was three (SD = 1.83. 79% of the participants reported initiation of prenatal care in the first trimester; 20% reported initiation in the second trimester; and 1% reported initiation in the third trimester (see
Table 1).
The mean birth weight of the participants’ neonates was 3,245.95 grams (SD = 444.06), and the mean gestational age was 39.3 weeks (SD = 1.19). Furthermore, 50.3% of the participants had baby boys (n = 151); 76% had vaginal deliveries (n = 228); 24% had caesarean sections (n = 72); and 9.3% had LBW neonates (n = 28).
3.3. Environmental Tobacco Smoke Exposure
The type of SHS exposures in this study were classified as exposure from all places, exposure from two places, exposure from one place, or no exposure. Two percent of the participants reported SHS exposure from all places; 55% reported SHS exposure from home and outside; 30.3% reported SHS exposure from outside; 7.7% reported SHS exposure from home; and 2.7% reported no SHS exposure (
Table 2).
The mean SHS exposure hours from the home environment were the highest across all the three trimesters. They were 13.1, 13.2, and 13.1 hours per week in the first, second, and third trimesters respectively. The mean SHS exposure hours from work were 5.0, 4.8, and 4.5 hours per week in the first, second, and third trimesters respectively. The mean SHS exposure hours from outside were 4.8, 4.85, and 4.85 hours per week in the first, second, and third trimesters respectively (
Table 3).
With regard to SHS exposure at home, 65.3% reported SHS exposure at home. Among subjects who reported SHS exposure at home, 52.7% reported SHS exposure from their husbands only, 10% from their husbands and other smokers at home, and 2.7% from smokers other than their husbands. (The 2.7% had husbands were nonsmokers.) Furthermore, the average reported number of cigarettes that were smoked by the exposed mother’s husband in the home was 16.3 cigarettes per day (SD = 15.89).
3.4. Comparison between the Groups of Participants Who Had Normal Birth Weight Neonates and who had LBW Neonates
Before running the multiple regression and logistic regression, an equivalent analysis was conducted between the group of participants who had normal birth weight neonates (
n = 272) and the group of participants who had LBW neonates (
n = 28) in terms of potential covariates. Descriptive statistics, t-tests for continuous variables, and chi-square tests for categorical variables were performed to compare the two groups. There were 272 participants who had normal birth weight neonates (90.7%) and 28 participants who had LBW neonates (9.3%). This is similar to the LBW rate in Jordan as a whole (10.6%) [
47]. The mean birth weight for the first group was 3338.8 grams (SD = 351.5), and the mean birth weight for the second group was 2343.6 (SD = 110.9).
Table 4 shows the participants’ weight before pregnancy
t (298) = 3.2, p < 0.001, weight gain during pregnancy
t (298) = 2.1, p = 0.036, and gestational age of the neonate
t (298) = 2.8, p < 0.005 were significant covariates (p < 0.05) (
Table 4). These covariates were included in the final logistic regression model because they were significantly different between the two groups.
There was no significant difference between the two groups in terms of neonates’ gender χ2 (1, n= 300) = 0.69, p = 0.41 (two-tailed), mother having a job outside home χ2 (1, n = 300) = 1.89, p = 0.17 (two-tailed), or initiation of prenatal care in the first trimester χ2 (1, n = 300) = 1.87, p = 0.17 (two-tailed). There were no participants who used drugs or alcohol during pregnancy.
3.5. The Influence of SHS on Neonatal Birth Weight
A stepwise multiple regression analysis was conducted to test the first hypothesis, where the dependent variable, which is the neonatal birth weight, could be explained by the independent variable, which is the reported average number of SHS exposure hours per week, in the first, second, and third trimesters. Multicollinearity was examined between the independent variables before the stepwise multiple regression analysis, to test for collinearity. Specifically the highest correlation coefficient between any independent predictor variables was only 0.49. The variance inflation for the independent variables was calculated with a result of 0.91, which indicated a high level of tolerance thus low collinearity.
The potential covariates that were entered in the model included the neonate’s gender, gestational age, number of mother’s previous pregnancies, weight gain during pregnancy, initiation of prenatal care, maternal age, maternal height, maternal weight before pregnancy, mother’s years of education, mother’s occupation during pregnancy, and total family income. From previous literature [
8,
27,
38] these variables were known to have a significant relationship with neonatal birth weight and may increase the risk of having LBW neonate.
Based on the multiple regression analysis, as the reported average number of SHS exposure hours per week from home, work, and outside in the second trimester increased, the neonatal birth weight significantly decreased while holding constant the gestational age of the neonate, mother’s weight before pregnancy and mother’s weight gain during pregnancy. These covariates were the ones that were retained in the model after running the stepwise multiple regression analysis. Overall, the model was significant (R
2 = 0.38;
F (6,293) = 30.13; p < 0.05) (
Table 5).
The total neonatal birth weight variance that was explained by the significant independent variables and significant covariates was 38%. The reported average number of SHS exposure hours per week from home, work, and outside in the second trimester explained 22% of the neonatal birth weight variance. The gestational age of the neonate, mother’s weight before pregnancy, and mother’s weight gain during pregnancy explained the remaining 16% of the neonatal birth weight variance.
3.6. The Risk of Having Low Birth Weight Neonate as a Result of SHS Exposure
A logistic regression was performed to test the second hypothesis. The estimated coefficients were the actual measures of the changes in the log odds ratio (ratio of the probabilities) of having LBW as the average number of SHS exposure increased one hour per week in each trimester while holding all covariates constant.
Based on logistic regression analysis, women who reported a higher average number of SHS exposure hours per week from occupational exposure in the second trimester were at significantly greater risk for having a LBW neonate than women who reported a lower average number of hours of SHS exposure from occupational exposure after controlling for mother’s weight before pregnancy, mother’s height, mother’s weight gain during pregnancy, total family income, and gestational age of the neonate. The adjusted odds ratio was OR = 1.331 (95% CI 1.052–1.684) for one unit increase of SHS exposure from work in the second trimester (p < 0.05). Women who reported a higher average number of SHS exposure hours per week from home and outside in the third trimester were at significantly greater risk for having a LBW neonate than women who reported a lower average number of hours of SHS exposure after controlling for the same covariates. The adjusted odds ratios were OR = 1.075 (95% C1 1.029–1.124) for one unit increase of SHS exposure from home in the third trimester and OR = 1.154 (95% CI 1.055–1.262) for one unit increase of SHS exposure from outside in the third trimester (p < 0.05) (
Table 6).
With regard to significant covariates, subjects who reported a higher average weight before pregnancy were at significantly lower risk of having a LBW neonate than subjects who reported a lower average weight before pregnancy (B = −0.068, p < 0.05). The adjusted odds ratio was OR = 0.934 (95% CI 0.881–0.992) for one unit increase of mother’s weight before pregnancy. Subjects who reported a higher average weight gain during pregnancy were at significantly lower risk of having a LBW neonate than those who reported a lower average weight gain during pregnancy (B = −0.156, p < 0.05). The adjusted odds ratio was OR = 0.856 (95% CI 0.739–0.991) for one unit increase of weight gain.
In summary, as the reported average number of SHS exposure hours per week from all places (home, work, and outside) in the second trimester increased, the neonatal birth weight significantly decreased while holding all covariates constant (R2 = 0.38; F (6,293) = 30.13; p < 0.05). The SHS exposure variables accounted for 22% of the birth weight variance. Also, subjects who reported higher average number of SHS exposure hours per week from occupational exposure in the second trimester and from home and outside in the third trimester were at significantly greater risk for having a LBW neonate than women who reported lower average number of SHS exposure hours (p < 0.05). The adjusted odds ratio were OR = 1.331 (95% CI 1.052–1.684) for work exposure, OR = 1.075 (95% C1 1.029–1.124) for home exposure, and OR = 1.154 (95% CI 1.055–1.262) for outside exposure.
4. Discussion
Based on the results of this study, there was an adverse effect of SHS exposure on birth outcomes. This influence started from the second trimester and lasted through the third trimester. The results of this study are consistent with the results of previous studies, in which the researchers found that maternal exposure to SHS was associated with increased levels of carbon monoxide, nicotine, and cotinine in the serum or urine of the mother and the neonates and amniotic fluid [
35,
48].
The study results are also consistent with the results of previous studies, in which the researchers found that SHS exposure significantly reduced neonate’s birth weight [
27,
34,
37,
49]. The second trimester fetal growth is most rapid [
7], and therefore that could explain the increased influence of SHS exposure starting from the second trimester. However, in maternal smoking and birth outcomes studies, smoking after the fourth month appears to be particularly crucial in lowering birth weight [
37]. Interestingly, this study supports a recent systematic review and meta analysis [
37] in which 58 studies were included to determine the effects of SHS exposure on birth outcomes. They proved estimates of 33g or more of birth weight reduction and increase the risk of birth weight below 2500 g by 22%, which represents a higher effect than older studies. In our study we found that the impact of SHS exposure is higher than previous estimates by the US Surgeon General’s report on the health consequences of SHS exposure [
1]. Our findings are strengthened by the fact that maternal smoking as a confounding factor does not exist at all due to the fact that most Jordanian pregnant women do not smoke.
The findings of this study add new support to the growing evidence showing adverse effects of SHS exposure on birth outcome. The quantity of SHS exposure was an important predictor of birth weight. As the quantity of SHS exposure increased, the birth weight of the neonate significantly decreased. All types of SHS exposure (home, work, and outside) significantly reduced birth weight. The last two trimesters were the times in which SHS exposure significantly reduced birth weight. The findings related to timing of exposure were of particular importance since it was not investigated in the previously reviewed studies.
The study results are consistent with the conclusions of the World Health Organization. The International Consultation on Environmental Tobacco Smoke and Child Health concluded that maternal smoking during pregnancy is a major cause of reduced birth weight, decreased lung function, and sudden infant death syndrome (SIDS). Exposure to SHS among nonsmoking pregnant women can also cause a decrease in birth weight [
50]. However, most of the evidence for these conclusions were drawn from studies conducted in the Western and developed countries. In this study, the relationship between SHS exposure and birth outcome was examined in Jordan, which is one of the developing countries that has a high prevalence of smoking among males (50%).
Smoking is on the rise in developing countries. Environmental conditions such as overcrowding may make the health effects of SHS more pronounced [
28]. However, only two studies investigated the adverse health effects of SHS exposure in developing countries. The results of this study are consistent with the results of these two studies that were conducted in China [
51] and India [
28]. The authors of both studies found a significant relationship between SHS exposure and adverse birth outcomes.
In summary, based on the results of this study, SHS exposure during pregnancy exerts significant adverse effects on birth outcome. These results are consistent with the studies that were conducted in the developed countries, in the developing countries, and with the recommendations and conclusions of the WHO. The findings of this study add new support to the growing evidence showing adverse effects of SHS exposure on birth outcome. The quantity, type, and timing of exposure were all significant predictors of birth weight.
4.1. Significant Covariates
In this study, mother’s weight before pregnancy, mother’s weight gain, and gestational age of the neonate were significant predictors of neonate’s birth weight and accounted for 16% of its variance. Furthermore, mother’s weight before pregnancy and weight gain during pregnancy significantly decreased the risk of having a LBW neonate. These results are consistent with the results of previous studies. Higher weight gain during pregnancy and higher maternal pre-pregnancy weight were found to significantly decrease the risk of having a LBW neonate [
52]. Maternal weight before pregnancy, representing the maternal long-term nutritional status, was an important independent determinant of birth weight and accounted for 13% of its variance. The weight gain during pregnancy, representing the short-term nutritional status, explained 5.6% of the variance [
29]. Moreover, gestational age significantly decreased the neonatal birth weight [
40].
In summary, mother’s weight before pregnancy, mother’s weight gain, and gestational age of the neonate were significant predictors of neonate’s birth weight. Controlling for these covariates is important while examining the influence of SHS exposure on birth weight.
4.2 Practice Implications
Birth weight is inversely correlated with both neonatal and postnatal mortality. The increased risk is not limited to LBW infants. Infants with birth weights of 3,000–3,499 grams have infant mortality rates that are higher than those of infants weighing 3,500–3,999 grams at birth [
53]. However, reductions in birth weight that lead to LBW are much more hazardous. Approximately two-thirds of all infant deaths in the United States occurred to infants born with LBW. Low birth weight infants are also at an increased risk of neurological problems, including cerebral palsy, seizure disorders, severe mental retardation, lower respiratory tract conditions, and general morbidity [
21]. Thus, it is conceivable that the reduction in birth weight, either less than 3,500 grams or less than 2,500 grams, caused by SHS exposure may increase the risk for morbidity and mortality during the first year of life. Based on this, it is important to review the implications of these study results for public health practice.
4.3. Public Health Implications
The goal of reducing LBW incidence by at least one third between 2000 and 2010 is one of the major goals in ‘A World Fit for Children’ [
54]. Physical environment plays an important role in determining the birth weight and the future health of the infant. More than 20 million infants worldwide, representing approximately 16% of all births, are born with LBW, 95.6% of these are born in developing countries. The level of LBW in developing countries (16.5%) is more than double the level in developed countries (7%) [
54].
Since nearly 1.1 billion people who smoked cigarettes consumed a total of five billion cigarettes in 1995, it is reasonable to assume that SHS exposure is a prevalent and an important public health problem. This is particularly true for developing countries, where men smoke substantially more than women (49%
versus 9%) [
55]. Swift action to highlight the need for strong public policies to protect infants and children from exposure to tobacco smoke is essential [
50]. This can be achieved by two complementary strategies: eliminating infants’ contact with tobacco smoke in utero and in childhood and reducing overall consumption of tobacco products. Effectively implementing these strategies requires combining educational programs and legislative interventions aimed particularly at eliminating tobacco use in settings frequented by infants and children [
50].
The workplace is also important to consider because women of childbearing age are present in the workplace in greater numbers than ever before. For example, women’s participation in the formal labor force in Jordan grew from 15% in 1980 to 24% in 1999 [
56]. Moreover, the workplace is one source of SHS exposure for pregnant women that can and should be minimized to reduce the risk of adverse pregnancy outcomes for working women [
57]. The safety of workplaces needs strong public health policies to protect working women. The antismoking regulations should be applied in the workplace, and they can be achieved by consultation with international organizations such as the World Health Organization, especially among developing countries like Jordan.
In summary, SHS exposure is a prevalent and an important public health problem, especially in developing countries. Exposure to SHS plays an important role in determining the birth weight. Combining educational programs and legislative interventions aimed particularly at eliminating tobacco use is the best public health strategy to reduce SHS influence on birth weight. Moreover, application of antismoking regulations in the workplace is a key component of the required public health policies.
4.4. Limitations
Although the study sample has the limitation of only being able to be generalized to those women who give birth in the public hospital of Irbid, Jordan, it has the strength of being systematically selected from this population. In Jordan, 95% of the deliveries occur in hospitals. Although 65% of these deliveries occur in public hospitals, public hospitals do not represent the whole population, since 35 % of deliveries occur in private hospitals. Also the self-reported measures of exposure are likely to be imprecise and subject to recall bias.


{kind=link}