Development, Methodology and Potential of the New Universal Visual Scoring System (UniViSS) for Caries Detection and Diagnosis


Abstract
:1. Introduction
2. Material and Methods
2.1. Selection of the Diagnostic Criteria
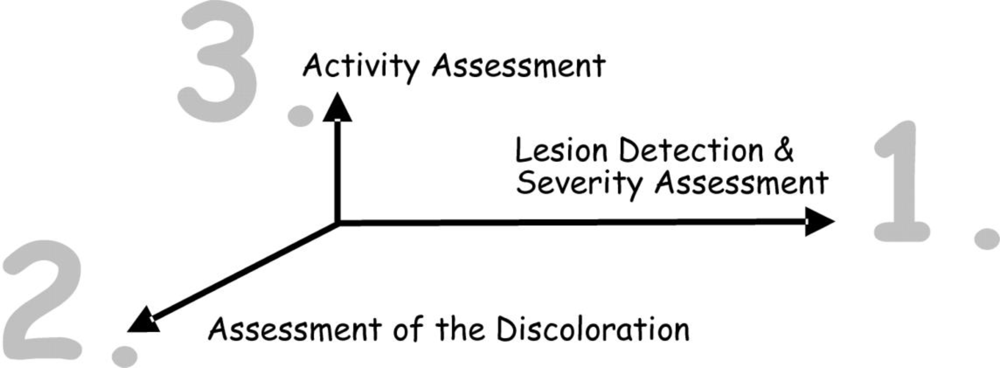
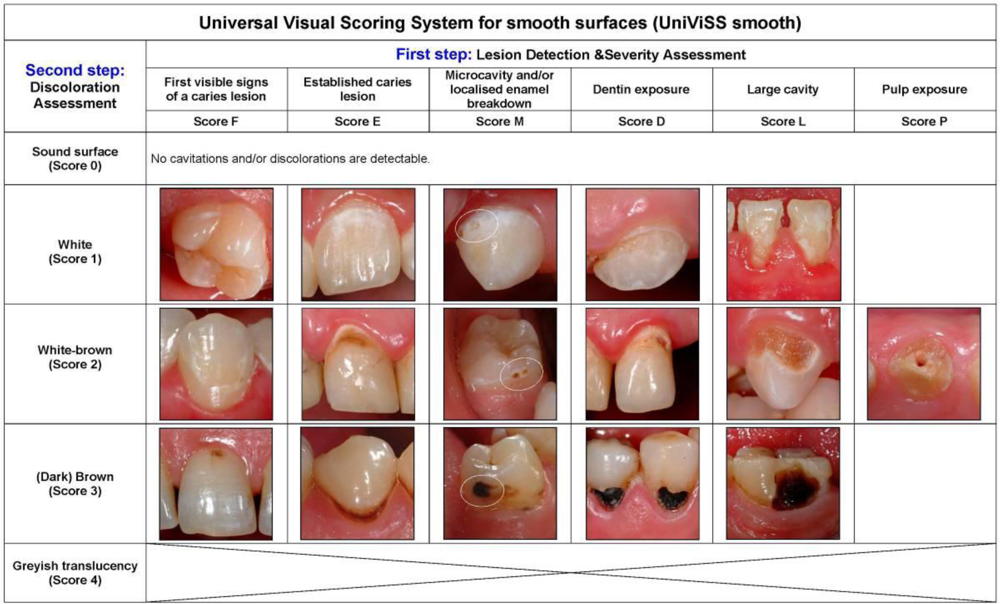
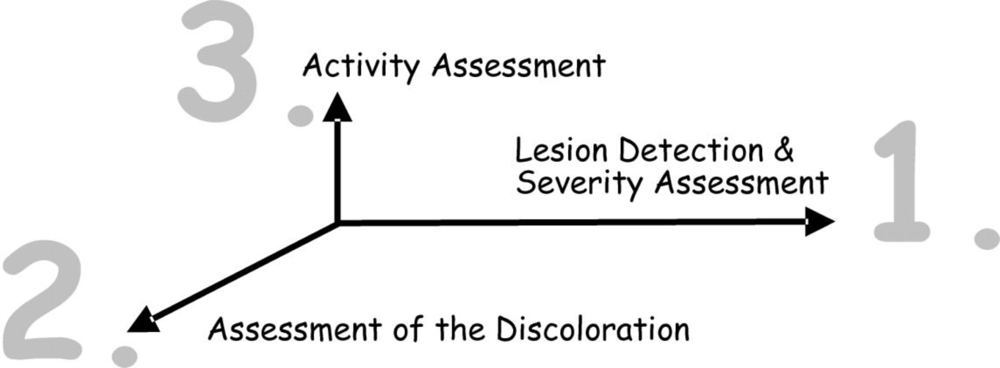
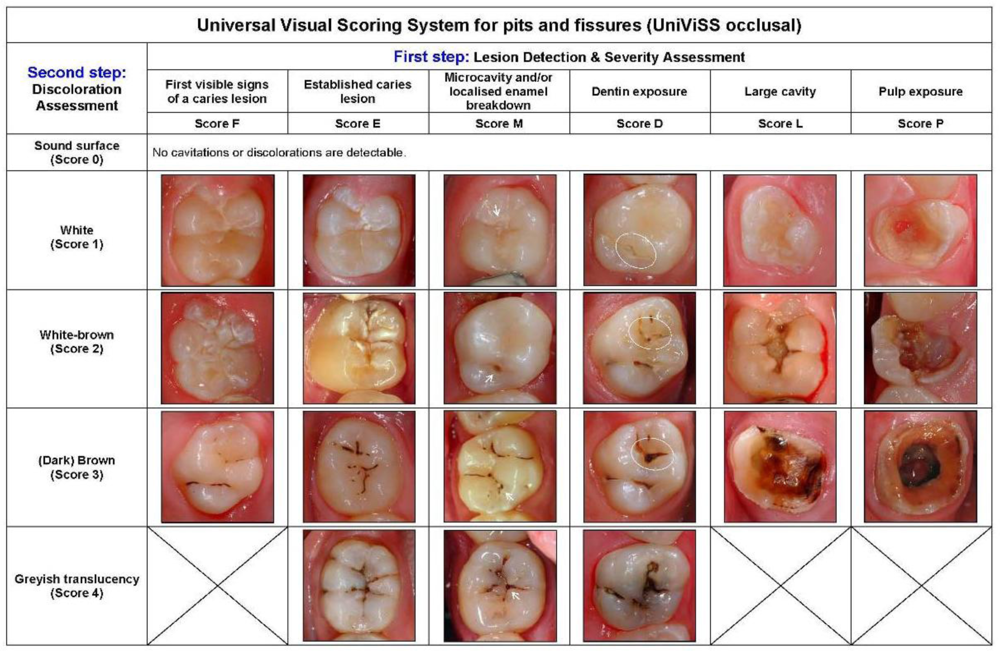
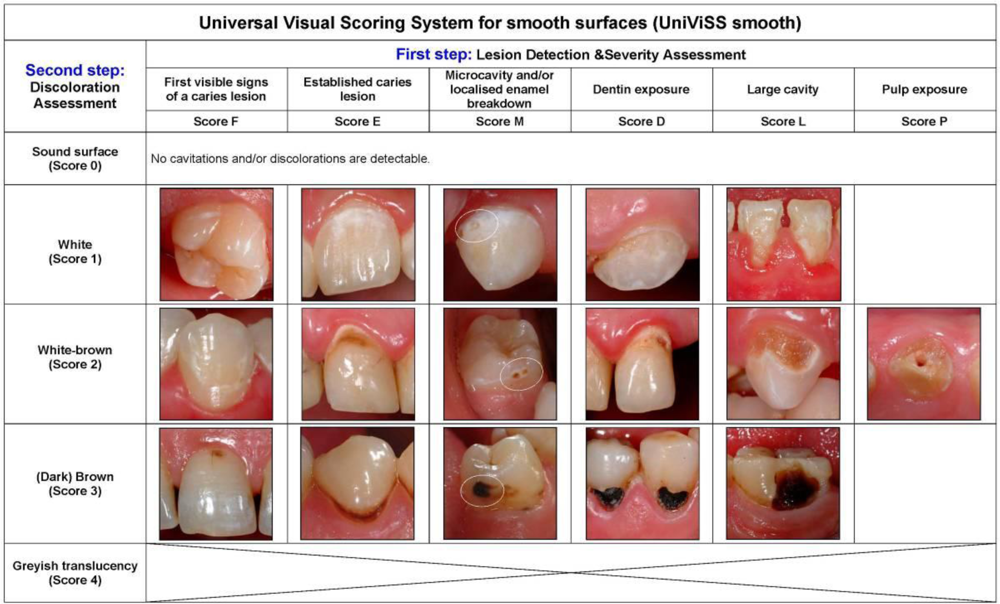
2.2. Systematization of the Diagnostic Criteria
2.3. Pre-Clinical Tests on Practicability
- - Examination of 40 subjects at two different points in time as part of a general screening. The examinations were done by separate examiners (I.G., S.B., H.S.).
- - Evaluation of the criteria under field conditions for 12-year olds as part of the standard school examination in a provincial town of the Philippines (R.H.-W.).
- - Application and assessment in a dental office (T.O.).
- - On-going review of the criteria set as part of patient care in university hospitals and the training of under- and postgraduate students and dentists (J.K., R.H.-W.).
2.4. Validation and Reproducibility Testing of UniViSS on Occlusal Surfaces
3. Results
4. Conclusions
References
- Oral Health Surveys. Basic Methods, 4th ed; WHO: Geneva, Switzerland, 1997.
- Kühnisch, J; Berger, S; Goddon, I; Senkel, H; Pitts, NB; Heinrich-Weltzien, R. Occlusal caries detection according to WHO basic methods, ICDAS II and laser fluorescence measurements: results from an epidemiological study. Community Dent. Oral Epidemiol 2008, 36, 475–484. [Google Scholar]
- Ekstrand, KR; Ricketts, DNJ; Kidd, EAM. Reproducibility and accuracy of three methods for assessment of demineralization depth of the occlusal surface: an in vitro examination. Caries Res 1997, 31, 224–231. [Google Scholar]
- Nyvad, B; Machiulskiene, V; Baelum, V. Reliability of a new caries diagnostic system differentiating between active and inactive caries lesions. Caries Res 1999, 33, 252–260. [Google Scholar]
- .
- .
- Fejerskov, O; Kidd, EAM. Dental Caries The Disease and Its Clinical Management; Blackwell Munksgaard: Oxford, UK, 2003. [Google Scholar]
- Ekstrand, KR; Ricketts, DNJ; Kidd, EAM; Qvist, V; Schou, S. Detection, diagnosis, monitoring and logical treatment of occlusal caries in relation to lesion activity and severity: an in vivo examination with histological validation. Caries Res 1998, 32, 247–254. [Google Scholar]
- Heinrich-Weltzien, R; Weerheijm, K; Kühnisch, J; Oehme, T; Stösser, L. Clinical evaluation of visual, radiographic, and laser fluorescence methods for detection of occlusal caries. ASDC J. Dent. Child 2002, 69, 127–132. [Google Scholar]
- Heinrich-Weltzien, R; Kühnisch, J; Ifland, S; Tranæus, S; Angmar-Månsson, B; Stösser, L. Detection of initial caries lesions on smooth surfaces by quantitative light-induced fluorescence (QLF) and visual examination—an in vivo comparison. Eur. J. Oral Sci 2005, 113, 494–498. [Google Scholar]
- Heinrich-Weltzien, R; Kühnisch, J; Oehme, T; Ziehe, A; Stosser, L; Garcia-Godoy, F. Comparison of different DIAGNOdent cut-off limits for in vivo detection of occlusal caries. Oper. Dent 2003, 28, 672–680. [Google Scholar]
- Kühnisch, J; Bücher, K; Henschel, V; Hickel, R. Reliability of DIAGNOdent 2095 and DIAGNOdent Pen measurements—Results from an in vitro study on occlusal sites. Eur. J. Oral. Sci 2007, 115, 206–211. [Google Scholar]
- Kühnisch, J; Heinrich-Weltzien, R; Tabatabaie, M; Stösser, L; Huysmans, MCDNJM. An in vitro comparison between two methods of electrical resistance measurements for occlusal caries detection. Caries Res 2006, 40, 104–111. [Google Scholar]
- Kühnisch, J; Ziehe, A; Brandstädt, A; Heinrich-Weltzien, R. An in vitro study of the reliability of DIAGNOdent® measurements. J. Oral Rehabil 2004, 31, 895–899. [Google Scholar]
- Pitts, NB. Modern concepts of caries measurements. J. Dent. Res 2004, 83, C43–C47. [Google Scholar]
- Ismail, AI. Visual and visuo-tactile detection of dental caries. J. Dent. Res 2004, 83, C56–C66. [Google Scholar]
- Ekstrand, KR; Martignon, S; Ricketts, DJN; Qvist, V. Detection and activity assessment of primary coronal caries lesions: a morphological study. Oper. Dent 2007, 32, 225–235. [Google Scholar]
- König, KG. Findings in serially sectioned teeth showing early fissure lesions. Adv. Fluorine Res 1966, 4, 73–79. [Google Scholar]
- Wenzel, A; Fejerskov, O. Validity of diagnosis of questionable caries lesions in occlusal surfaces of extracted third molars. Caries Res 1992, 26, 188–194. [Google Scholar]
- Marthaler, TM. A standardized system of recording dental conditions. Helv. Odontol. Acta 1966, 10, 1–18. [Google Scholar]
- Kühnisch, J; Senkel, H; Heinrich-Weltzien, R. Vergleichende Untersuchung zur Zahngesundheit von deutschen und ausländischen 8- bis 10-Jährigen des westfälischen Ennepe-Ruhr-Kreises. Gesundheitswesen 2003, 65, 96–101. [Google Scholar]
- Kühnisch, J; Bücher, K; Henschel, V; Hickel, R. Reliability of DIAGNOdent 2095 and DIAGNOdent Pen measurements—Results from an in vitro study on occlusal sites. Eur. J. Oral Sci 2002, 115, 206–211. [Google Scholar]
- Kühnisch, J; Heinrich-Weltzien, R; Senkel, H; Clasen, AB; Stösser, L. Dental health and caries topography in 8-yr-old German and immigrant children. Eur. J. Paediatr. Dent 2001, 2, 191–196. [Google Scholar]
- Jablonski-Momeni, A; Stachniss, V; Ricketts, DNJ; Heinzel-Gutenbrunner, M; Pieper, K. Reproducibility and accuracy of the ICDAS-II for detection of occlusal caries in vitro. Caries Res 2008, 42, 79–87. [Google Scholar]
- Pitts, NB. Are we ready to move from operative to non-operative/preventive treatment of dental caries in clinical practice? Caries Res 2004, 38, 294–304. [Google Scholar]
- Ricketts, DNJ; Kidd, EAM; Beighton, D. Operative and microbiological validation of visual, radiographic and electronic diagnosis of occlusal caries in non-cavitated teeth judged to be in need of operative care. Br. Dent. J 1995, 179, 214–220. [Google Scholar]
- Handelman, SL; Leverett, DH; Espeland, MA; Curzon, JA. Clinical radiographic evaluation of sealed carious and sound tooth surfaces. J. Am. Dent. Assoc 1986, 113, 751–754. [Google Scholar]
- Jensen, OE; Handelman, SL. Effect of an autopolymerizing sealant on viability of microflora in occlusal dental caries. Scand. J. Dent. Res 1980, 88, 382–388. [Google Scholar]
- Mertz-Fairhurst, EJ; Schuster, GS; Fairhurst, CW. Arresting caries by sealants: result of a clinical study. J. Am. Dent. Assoc 1986, 112, 194–197. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Study type | Tools | Illumination | Tooth cleaning |
|---|---|---|---|
| Field | Cotton rolls | Head lamp | Patient brushed him/herself |
| Clinical | Magnifying glass/loop | Examination lamp | Professional tooth cleaning with a bristle brush etc. |
| Laboratory | Dental unit with air syringe | Operating light of the dental unit | Professional tooth cleaning with air polishing |
| Occlusal pits and fissures | Smooth surfaces | ||
|---|---|---|---|
| Inactive | Active | Inactive | Active |
| Persistence of the lesions over years/decades | Detection within some years after tooth eruption | Persistence of the lesions over years/decades | Detection within some years after tooth eruption |
| No plaque coverage | Plaque coverage | No plaque coverage | Plaque coverage |
| Glossy, shiny appearance of the enamel surface after air-drying | Matt/frosty/rough appearance of the enamel surface after air-drying | Glossy, shiny appearance of the enamel surface after air-drying | Matt/frosty/rough appearance of the enamel surface after air-drying |
| No pathological enlargements | Microcavities | Lesions located in distance to the gingiva | White spots near the gingiva margin |
| Brown discoloration in enamel | White(-brown) discoloration in enamel | Brown discoloration in enamel | White(-brown) discoloration in enamel |
| Hard, dry, discolored dentine | Soft, wet, (un)discolored dentine | Hard, dry, discolored dentine | Soft, wet, (un)discolored dentine |
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Kühnisch, J.; Goddon, I.; Berger, S.; Senkel, H.; Bücher, K.; Oehme, T.; Hickel, R.; Heinrich-Weltzien, R. Development, Methodology and Potential of the New Universal Visual Scoring System (UniViSS) for Caries Detection and Diagnosis. Int. J. Environ. Res. Public Health 2009, 6, 2500-2509. https://doi.org/10.3390/ijerph6092500
Kühnisch J, Goddon I, Berger S, Senkel H, Bücher K, Oehme T, Hickel R, Heinrich-Weltzien R. Development, Methodology and Potential of the New Universal Visual Scoring System (UniViSS) for Caries Detection and Diagnosis. International Journal of Environmental Research and Public Health. 2009; 6(9):2500-2509. https://doi.org/10.3390/ijerph6092500
Chicago/Turabian StyleKühnisch, Jan, Inka Goddon, Susanne Berger, Helga Senkel, Katharina Bücher, Thomas Oehme, Reinhard Hickel, and Roswitha Heinrich-Weltzien. 2009. "Development, Methodology and Potential of the New Universal Visual Scoring System (UniViSS) for Caries Detection and Diagnosis" International Journal of Environmental Research and Public Health 6, no. 9: 2500-2509. https://doi.org/10.3390/ijerph6092500