Prognostic Factors of Early Stage Epithelial Ovarian Carcinoma

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Data Collection
2.3. Statistical Analysis
2.4. Details of Ethics Approval
3. Results
3.1. Patent Characteristics
3.2. Analyses of Prognostic Factors for 5-year DFS in Early Stage EOC Women
3.3. Analyses of Prognostic Factors for 5-year OS in Early Stage EOC Women
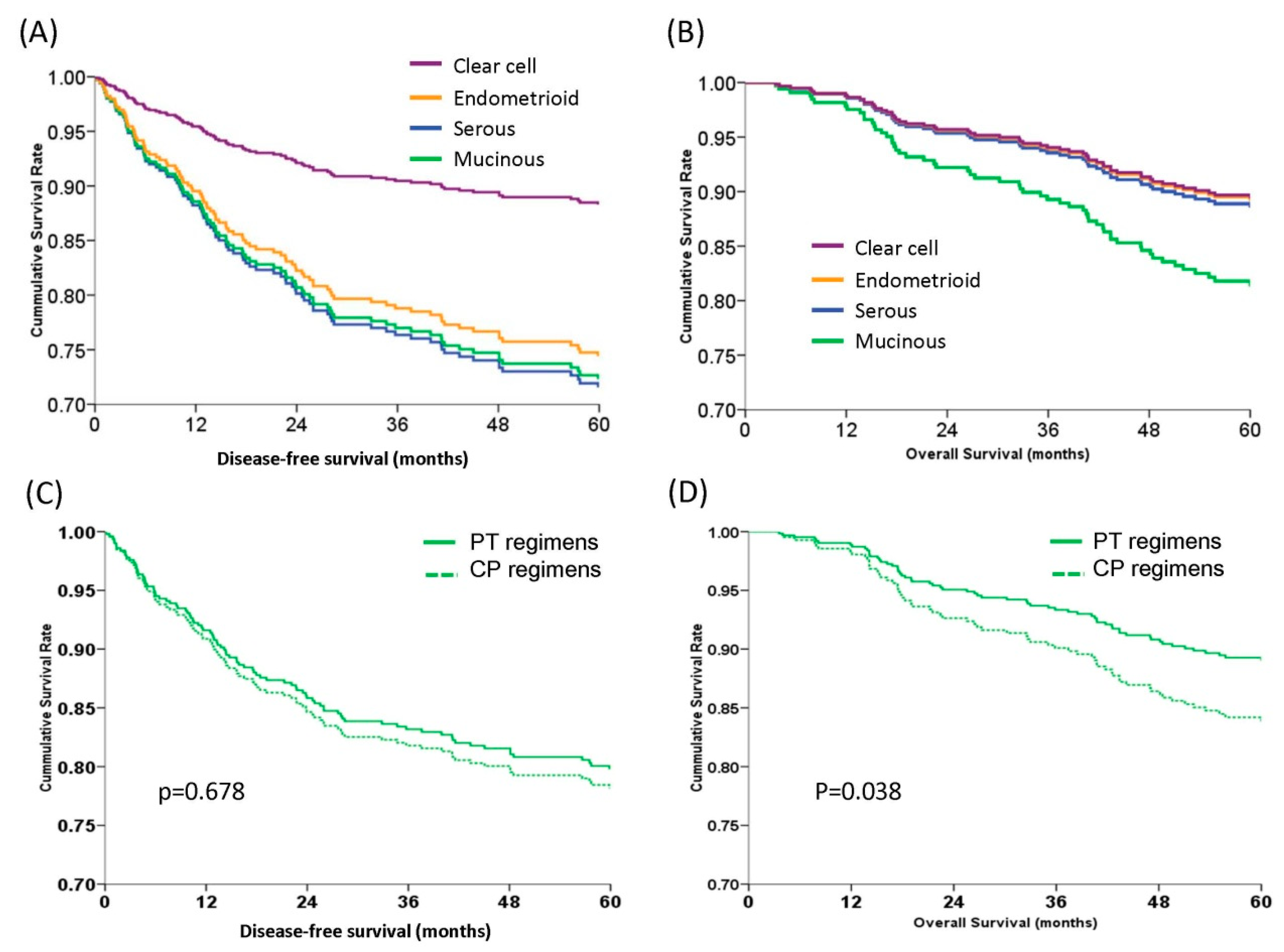
3.4. Patients with the Clear Cell Histologic Type Demonstrated the Best 5-year DFS but Similar 5-year OS Compared with the Other Histologic Types
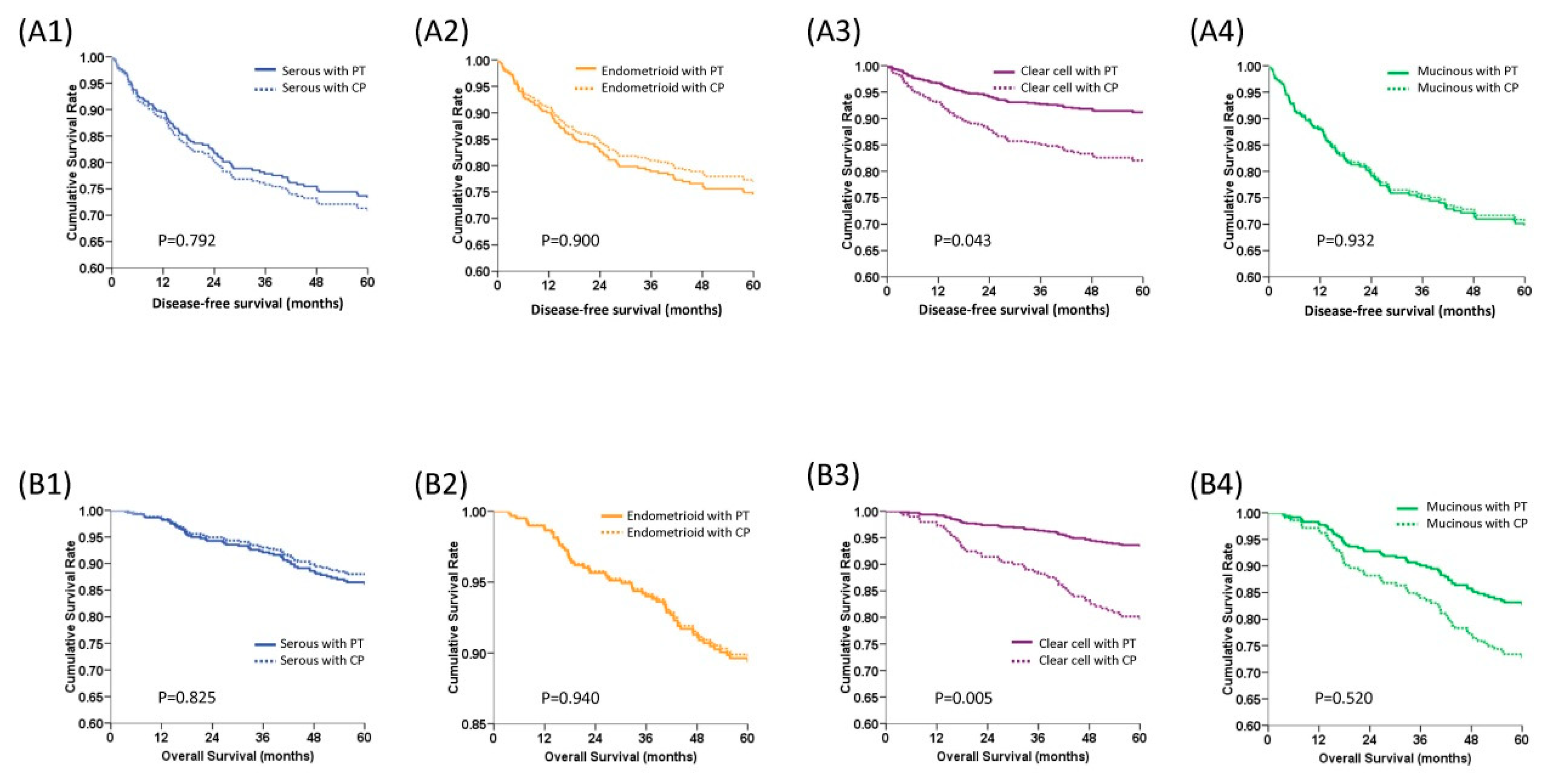
3.5. PT (Platinum and Paclitaxel) Regimens Had Better DFS and OS in Patients with Clear Cell Histology than CP (Platinum and Cyclophosphamide) Regimens
3.6. The PT and CP Regimens Showed Similar DFS and OS in Early Stage Ovarian Cancer Patients
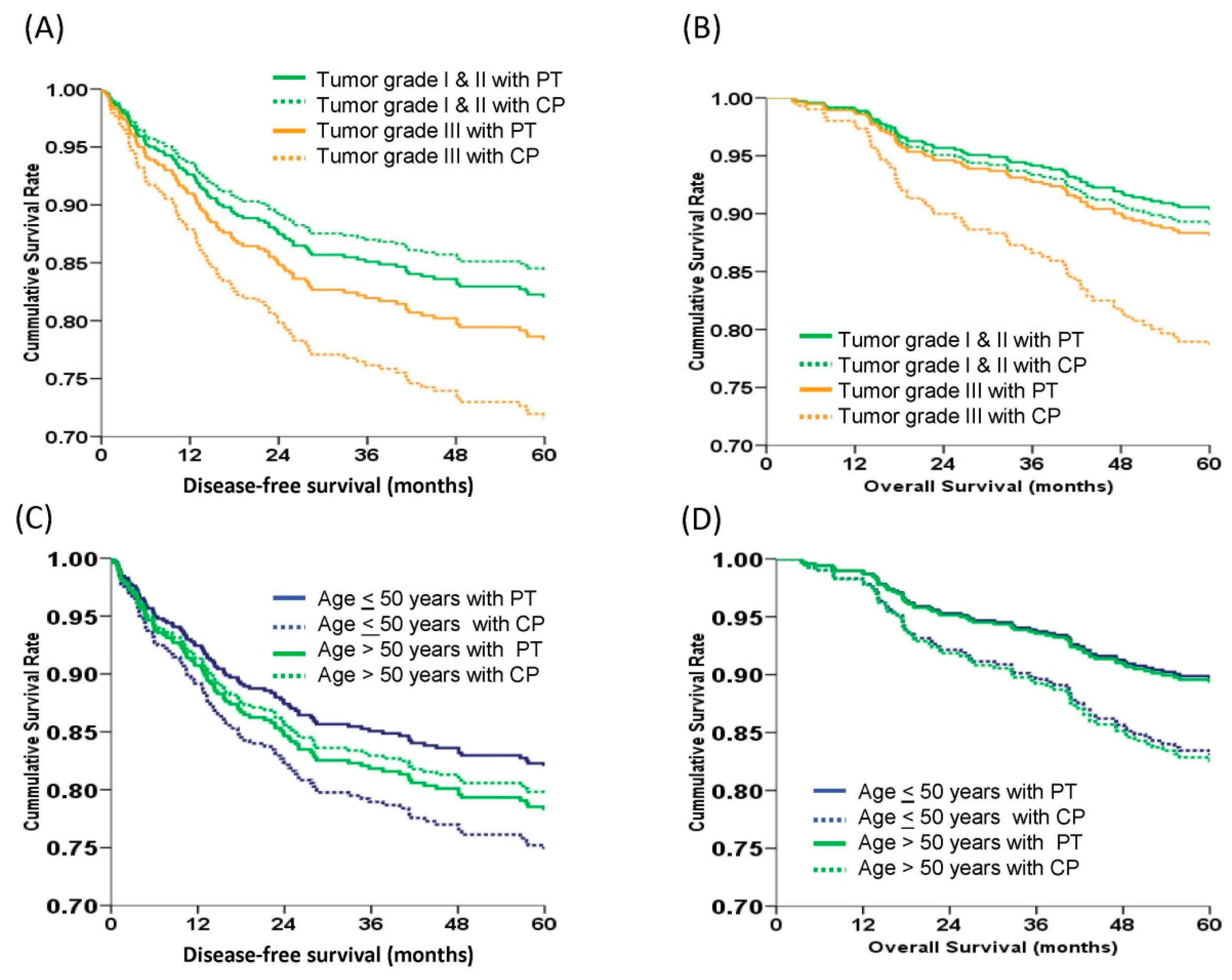
3.7. PT Regimens Had Benefit on 5-year OS in Patients with Poorly-Differentiated Tumor Cells (Grade 3)
3.8. The Patient’s Age at Diagnosis Did not Affect the 5-year DFS and OS of Patients Treated with PT and CP Regimens
4. Discussion
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviations
| CI | confidence interval |
| aHR | adjusted hazard ratio |
| FIGO | International Federation of Gynecology and Obstetrics |
| DFS | disease-free survival |
| OS | overall survival |
| EOC | epithelial ovarian carcinoma |
| PT | carboplatin + paclitaxel/cisplatin + paclitaxel/carboplatin + docetaxel |
| CP | cyclophosphamide + caboplatin/cyclophosphamide + cisplatin |
References
- Bamias, A.; Sotiropoulou, M.; Zagouri, F.; Trachana, P.; Sakellariou, K.; Kostouros, E.; Kakoyianni, K.; Rodolakis, A.; Vlahos, G.; Haidopoulos, D.; et al. Prognostic evaluation of tumour type and other histopathological characteristics in advanced epithelial ovarian cancer treated with surgery and paclitaxel/carboplatin chemotherapy: Cell type is the most useful prognostic factor. Eur. J. Cancer 2012, 48, 1476–1483. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.Y.; Kim, T.J.; Kim, M.J.; Kim, H.J.; Song, T.; Kim, M.K.; Choi, C.H.; Lee, J.W.; Bae, D.S.; Kim, B.G. Prognosis of ovarian clear cell carcinoma compared to other histological subtypes: A meta-analysis. Gynecol. Oncol. 2011, 122, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Pectasides, D.; Fountzilas, G.; Aravantinos, G.; Kalofonos, C.; Efstathiou, H.; Farmakis, D.; Skarlos, D.; Pavlidis, N.; Economopoulos, T.; Dimopoulos, M.A. Advanced stage clear-cell epithelial ovarian cancer: The Hellenic Cooperative Oncology Group experience. Gynecol. Oncol. 2006, 102, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.K.; Tian, C.; Monk, B.J.; Herzog, T.; Kapp, D.S.; Bell, J.; Young, R.C. Gynecologic Oncology Group. Prognostic factors for high-risk early-stage epithelial ovarian cancer: A Gynecologic Oncology Group study. Cancer 2008, 112, 2202–2210. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.K.; Teoh, D.; Hu, J.M.; Shin, J.Y.; Osann, K.; Kapp, D.S. Do clear cell ovarian carcinomas have poorer prognosis compared to other epithelial cell types? A study of 1411 clear cell ovarian cancers. Gynecol. Oncol. 2008, 109, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Schnack, T.H.; Høgdall, E.; Nedergaard, L.; Høgdall, C. Demographic Clinical and Prognostic Factors of Primary Ovarian Adenocarcinomas of Serous and Clear Cell Histology-A Comparative Study. Int. J. Gynecol. Cancer 2016, 26, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Timmers, P.J.; Zwinderman, A.H.; Teodorovic, I.; Vergote, I.; Trimbos, J.B. Clear cell carcinoma compared to serous carcinoma in early ovarian cancer: Same prognosis in a large randomized trial. Int. J. Gynecol. Cancer 2009, 19, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Köbel, M.; Kalloger, S.E.; Santos, J.L.; Huntsman, D.G.; Gilks, C.B.; Swenerton, K.D. Tumor type and substage predict survival in stage I and II ovarian carcinoma: Insights and implications. Gynecol. Oncol. 2010, 116, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Colombo, N.; Guthrie, D.; Chiari, S.; Parmar, M.; Qian, W.; Swart, A.M.; Torri, V.; Williams, C.; Lissoni, A.; Bonazzi, C. International Collaborative Ovarian Neoplasm, International Collaborative Ovarian Neoplasm trial 1: A randomized trial of adjuvant chemotherapy in women with early-stage ovarian cancer. J. Natl. Cancer Inst. 2003, 95, 125–132. [Google Scholar] [PubMed]
- Trimbos, J.B.; Parmar, M.; Vergote, I.; Guthrie, D.; Bolis, G.; Colombo, N.; Vermorken, J.B.; Torri, V.; Mangioni, C.; Pecorelli, S.; et al. International Collaborative Ovarian Neoplasm trial 1 and Adjuvant ChemoTherapy In Ovarian Neoplasm trial: Two parallel randomized phase III trials of adjuvant chemotherapy in patients with early-stage ovarian carcinoma. J. Natl. Cancer Inst. 2003, 95, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Trimbos, J.B.; Parmar, M.; Vergote, I.; Guthrie, D.; Bolis, G.; Colombo, N.; Vermorken, J.B.; Torri, V.; Mangioni, C.; Pecorelli, S.; et al. Treatment of Cancer-Adjuvant ChemoTherapy in Ovarian, Impact of adjuvant chemotherapy and surgical staging in early-stage ovarian carcinoma: European Organisation for Research and Treatment of Cancer-Adjuvant ChemoTherapy in Ovarian Neoplasm trial. J. Natl. Cancer Inst. 2003, 95, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Collinson, F.; Qian, W.; Fossati, R.; Lissoni, A.; Williams, C.; Parmar, M.; Ledermann, J.; Colombo, N.; Swart, A.; ICON1 Collaborators. Optimal treatment of early-stage ovarian cancer. Ann. Oncol. 2014, 25, 1165–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gershenson, D.M.; Wharton, J.T.; Copeland, L.J.; Stringer, C.A.; Edwards, C.L.; Kavanagh, J.J.; Freedman, R.S. Treatment of advanced epithelial ovarian cancer with cisplatin and cyclophosphamide. Gynecol. Oncol. 1989, 32, 336–341. [Google Scholar] [CrossRef]
- McGuire, W.P.; Hoskins, W.J.; Brady, M.F.; Kucera, P.R.; Partridge, E.E.; Look, K.Y.; Clarke-Pearson, D.L.; Davidson, M. Cyclophosphamide and cisplatin compared with paclitaxel and cisplatin in patients with stage III and stage IV ovarian cancer. N. Engl. J. Med. 1996, 334, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Piccart, M.J.; Bertelsen, K.; James, K.; Cassidy, J.; Mangioni, C.; Simonsen, E.; Stuart, G.; Kaye, S.; Vergote, I.; Blom, R.; et al. Randomized intergroup trial of cisplatin-paclitaxel versus cisplatin-cyclophosphamide in women with advanced epithelial ovarian cancer: Three-year results. J. Natl. Cancer Inst. 2000, 92, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Ozols, R.F. Update on the management of ovarian cancer. Cancer J. 2000, 8, S22–S30. [Google Scholar]
- Hennessy, B.T.; Coleman, R.L.; Markman, M. Ovarian cancer. Lancet 2009, 374, 1371–1382. [Google Scholar] [CrossRef]
- Hogberg, T.; Glimelius, B.; Nygren, P. A systematic overview of chemotherapy effects in ovarian cancer. Acta Oncol. 2001, 40, 340–360. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for the Management of Ovarian Cancer; National Health Research Institutes: Taipei, Taiwan, 2001.
- Pitakkarnkul, S.; Tangjitgamol, S.; Srijaipracharoen, S.; Manusirivithaya, S.; Pataradool, K.; Prutthiphongsit, W.; Khunnarong, J.; Thavaramara, T. Treatment outcomes of paclitaxel for refractory or recurrent epithelial ovarian cancer patients in Thailand. Asian Pac. J. Cancer Prev. 2013, 14, 2421–2427. [Google Scholar] [CrossRef] [PubMed]
- Stuart, G.C.; Kitchener, H.; Bacon, M.; duBois, A.; Friedlander, M.; Ledermann, J.; Marth, C.; Thigpen, T.; Trimble, E.; Participants of 4th Ovarian Cancer Consensus Conference (OCCC); Gynecologic Cancer Intergroup. Participants of 4th Ovarian Cancer Consensus, I Gynecologic Cancer, 2010 Gynecologic Cancer InterGroup (GCIG) consensus statement on clinical trials in ovarian cancer: Report from the Fourth Ovarian Cancer Consensus Conference. Int. J. Gynecol. Cancer 2011, 21, 750–755. [Google Scholar] [PubMed]
- Du Bois, A.; Lück, H.J.; Meier, W.; Adams, H.P.; Möbus, V.; Costa, S.; Bauknecht, T.; Richter, B.; Warm, M.; Schröder, W.; et al. Arbeitsgemeinschaft Gynakologische Onkologie Ovarian Cancer Study, A randomized clinical trial of cisplatin/paclitaxel versus carboplatin/paclitaxel as first-line treatment of ovarian cancer. J. Natl. Cancer Inst. 2003, 95, 1320–1329. [Google Scholar] [CrossRef] [PubMed]
- Gadducci, A.; Cosio, S.; Zola, P.; Sostegni, B.; Fuso, L.; Sartori, E. Prognostic factors and clinical outcome of patients with recurrent early-stage epithelial ovarian cancer: An Italian multicenter retrospective study. Int. J. Gynecol. Cancer 2013, 23, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.L.; Abu-Rustum, N.R.; Sonoda, Y.; Levine, D.A.; Poynor, E.A.; Aghajanian, C.; Jarnagin, W.R.; DeMatteo, R.P.; D’Angelica, M.I.; Barakat, R.R.; et al. The addition of extensive upper abdominal surgery to achieve optimal cytoreduction improves survival in patients with stages IIIC-IV epithelial ovarian cancer. Gynecol. Oncol. 2006, 103, 1083–1090. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, L.A.; Huang, B.; Miller, R.W.; Tucker, T.; Goodrich, S.T.; Podzielinski, I.; DeSimone, C.P.; Ueland, F.R.; van Nagell, J.R.; Seamon, L.G. Ten-year relative survival for epithelial ovarian cancer. Obstet. Gynecol. 2012, 120, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Mackay, H.J.; Brady, M.F.; Oza, A.M.; Reuss, A.; Pujade-Lauraine, E.; Swart, A.M.; Siddiqui, N.; Colombo, N.; Bookman, M.A.; Pfisterer, J.; et al. Prognostic relevance of uncommon ovarian histology in women with stage III/IV epithelial ovarian cancer. Int. J. Gynecol. Cancer 2010, 20, 945–952. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Prognostic Factors | Univariate Regression Analyses | Multivariate Regression Analyses | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | aHR | 95% CI | p | |
| Age (y/o) | ||||||
| ≤50 | 1.00 | (Reference) | 1.00 | (Reference) | ||
| >50 | 1.20 | 0.80–1.79 | 0.383 | 0.98 | 0.64–1.51 | 0.935 |
| FIGO stage | ||||||
| Ia and Ib | 1.00 | (Reference) | 1.00 | (Reference) | ||
| Ic | 1.92 | 1.00–3.69 | 0.049 | 1.98 | 1.01–3.89 | 0.043 |
| II | 3.84 | 1.94–7.63 | <0.001 | 3.26 | 1.75–8.65 | 0.002 |
| Histology | ||||||
| Serous | 1.00 | (Reference) | 1.00 | (Reference) | ||
| Mucinous | 0.50 | 0.25–1.00 | 0.049 | 0.98 | 0.45–2.12 | 0.964 |
| Endometrioid | 0.44 | 0.25–0.79 | 0.006 | 0.89 | 0.45–1.75 | 0.734 |
| Clear cell | 0.37 | 0.21–0.64 | <0.001 | 0.37 | 0.21–0.73 | 0.001 |
| Other types * | 0.67 | 0.31–1.45 | 0.311 | 0.75 | 0.33–1.69 | 0.484 |
| Tumor grade | ||||||
| 1 | 1.00 | (Reference) | 1.00 | (Reference) | ||
| 2 | 1.74 | 0.84–3.60 | 0.138 | 2.12 | 0.96–4.71 | 0.064 |
| 3 | 2.11 | 1.11–4.00 | 0.023 | 3.89 | 1.75–8.64 | 0.001 |
| Regimens and cycles | ||||||
| PT (6) | 1.00 | (Reference) | 1.00 | (Reference) | ||
| PT (3–5) | 0.51 | 0.23–1.12 | 0.093 | 0.77 | 0.33–1.79 | 0.538 |
| CP (6) | 0.77 | 0.47–1.26 | 0.297 | 0.84 | 0.49–1.43 | 0.579 |
| CP (3–5) | 1.52 | 0.86–2.68 | 0.151 | 2.22 | 1.18–4.17 | 0.013 |
| Prognostic Factors | Univariate Regression Analyses | Multivariate Regression Analyses | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | aHR | 95% CI | p | |
| Age | ||||||
| ≤50 | 1.00 | (Reference) | 1.00 | (Reference) | ||
| > 50 | 1.15 | 0.59–2.26 | 0.511 | 0.91 | 0.54–1.53 | 0.731 |
| FIGO stage | ||||||
| Ia and Ib | 1.00 | (Reference) | 1.00 | (Reference) | ||
| Ic | 1.37 | 0.62–3.02 | 0.366 | 1.53 | 0.68–3.42 | 0.302 |
| II | 3.67 | 1.65–8.17 | <0.001 | 5.97 | 2.47–14.39 | <0.001 |
| Histology | ||||||
| Serous | 1.00 | (Reference) | 1.00 | (Reference) | ||
| Mucinous | 0.79 | 0.35–1.78 | 0.570 | 2.03 | 0.79–5.21 | 0.140 |
| Endometrioid | 0.48 | 0.22–1.02 | 0.055 | 1.18 | 0.48–2.87 | 0.718 |
| Clear cell | 0.56 | 0.29–1.10 | 0.094 | 0.96 | 0.45–2.04 | 0.909 |
| Other types * | 0.79 | 0.30–2.07 | 0.635 | 1.33 | 0.49–3.56 | 0.571 |
| Tumor grade | ||||||
| 1 | 1.00 | (Reference) | 1.00 | (Reference) | ||
| 2 | 1.21 | 0.38–3.81 | 0.934 | 1.61 | 0.51–2.95 | 0.317 |
| 3 | 1.54 | 0.59–4.09 | 0.206 | 2.77 | 1.12–6.83 | 0.027 |
| Regimens and cycles | ||||||
| PT (6) | 1.00 | (Reference) | 1.00 | (Reference) | ||
| PT (3–5) | 0.81 | 0.33–1.97 | 0.645 | 1.78 | 0.70–4.61 | 0.233 |
| CP (6) | 1.24 | 0.70–2.18 | 0.465 | 1.38 | 0.74–2.58 | 0.309 |
| CP (3–5) | 1.86 | 0.92–3.77 | 0.084 | 3.29 | 1.47–7.34 | 0.004 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, S.-F.; Lau, H.-Y.; Wu, H.-H.; Hsu, H.-C.; Twu, N.-F.; Cheng, W.-F. Prognostic Factors of Early Stage Epithelial Ovarian Carcinoma. Int. J. Environ. Res. Public Health 2019, 16, 637. https://doi.org/10.3390/ijerph16040637
Hsieh S-F, Lau H-Y, Wu H-H, Hsu H-C, Twu N-F, Cheng W-F. Prognostic Factors of Early Stage Epithelial Ovarian Carcinoma. International Journal of Environmental Research and Public Health. 2019; 16(4):637. https://doi.org/10.3390/ijerph16040637
Chicago/Turabian StyleHsieh, Shu-Feng, Hei-Yu Lau, Hua-Hsi Wu, Heng-Cheng Hsu, Nae-Fang Twu, and Wen-Fang Cheng. 2019. "Prognostic Factors of Early Stage Epithelial Ovarian Carcinoma" International Journal of Environmental Research and Public Health 16, no. 4: 637. https://doi.org/10.3390/ijerph16040637