A Phenomenological Account of HIV Disclosure Experiences of Children and Adolescents from Northern and Southern Ghana

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
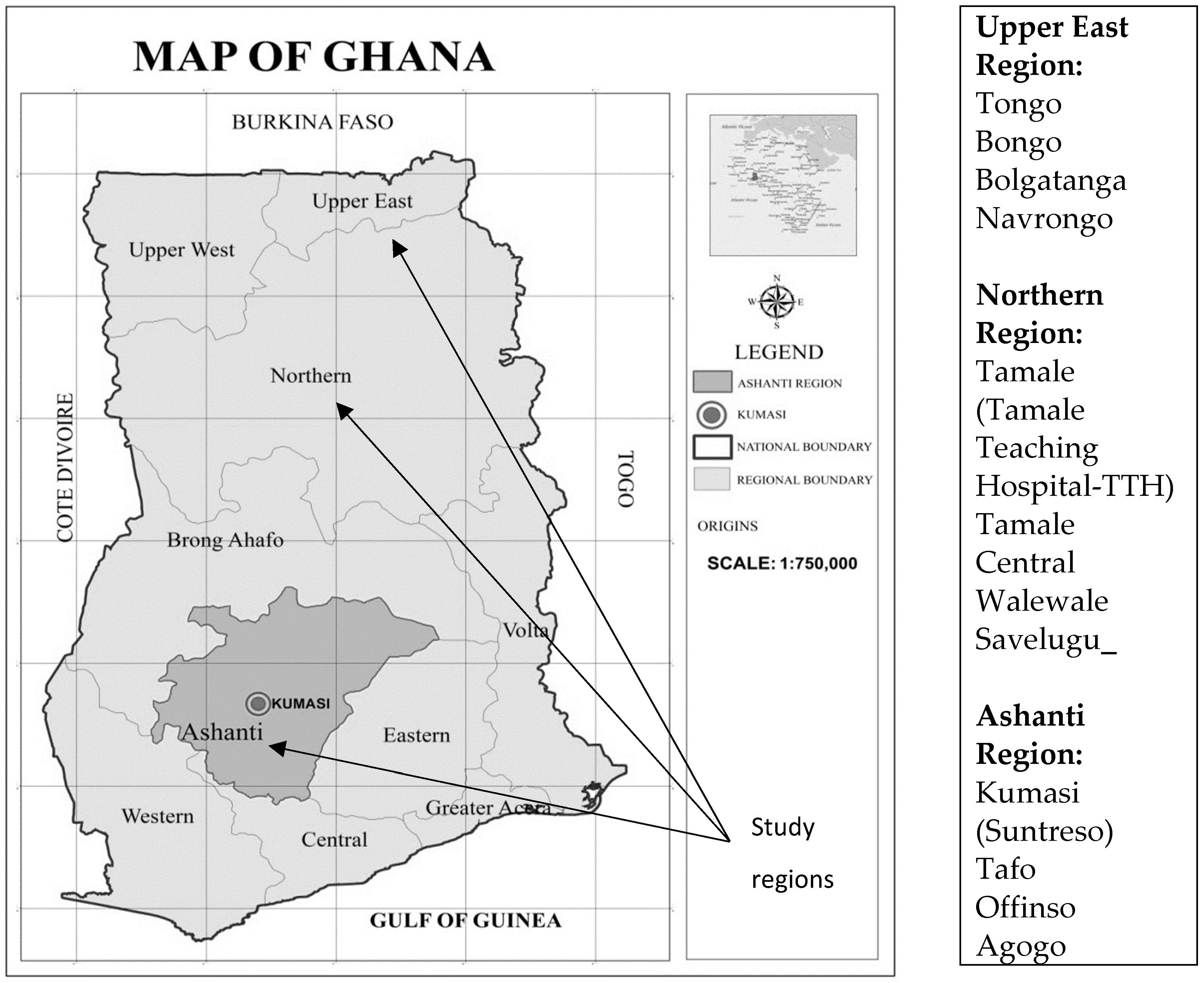
2.1. Study Setting
2.2. Study Design
2.3. Sampling and Participant Recruitment
2.4. Data Collection
2.5. Data Processing, Coding and Analysis
2.6. Quality Control and Data Rigor
2.7. Ethical Statement
3. Results
3.1. Participant’s Background Information, Current Preoccupation and Living Arrangement
“…I am 14 years … I live with my mother and siblings …I am in school and in class 4”.(Female, 14 years, Agogo, Southern Ghana)
“I am 16 years; from [ ] …I am in school; and in class 4; will be progressing to class 5”.(Female, 16 years, Agogo, Southern Ghana)
“…I am 17 years … I am in school, in junior High School Year 3”.(Female, 17 years, Tafo, Southern Ghana)
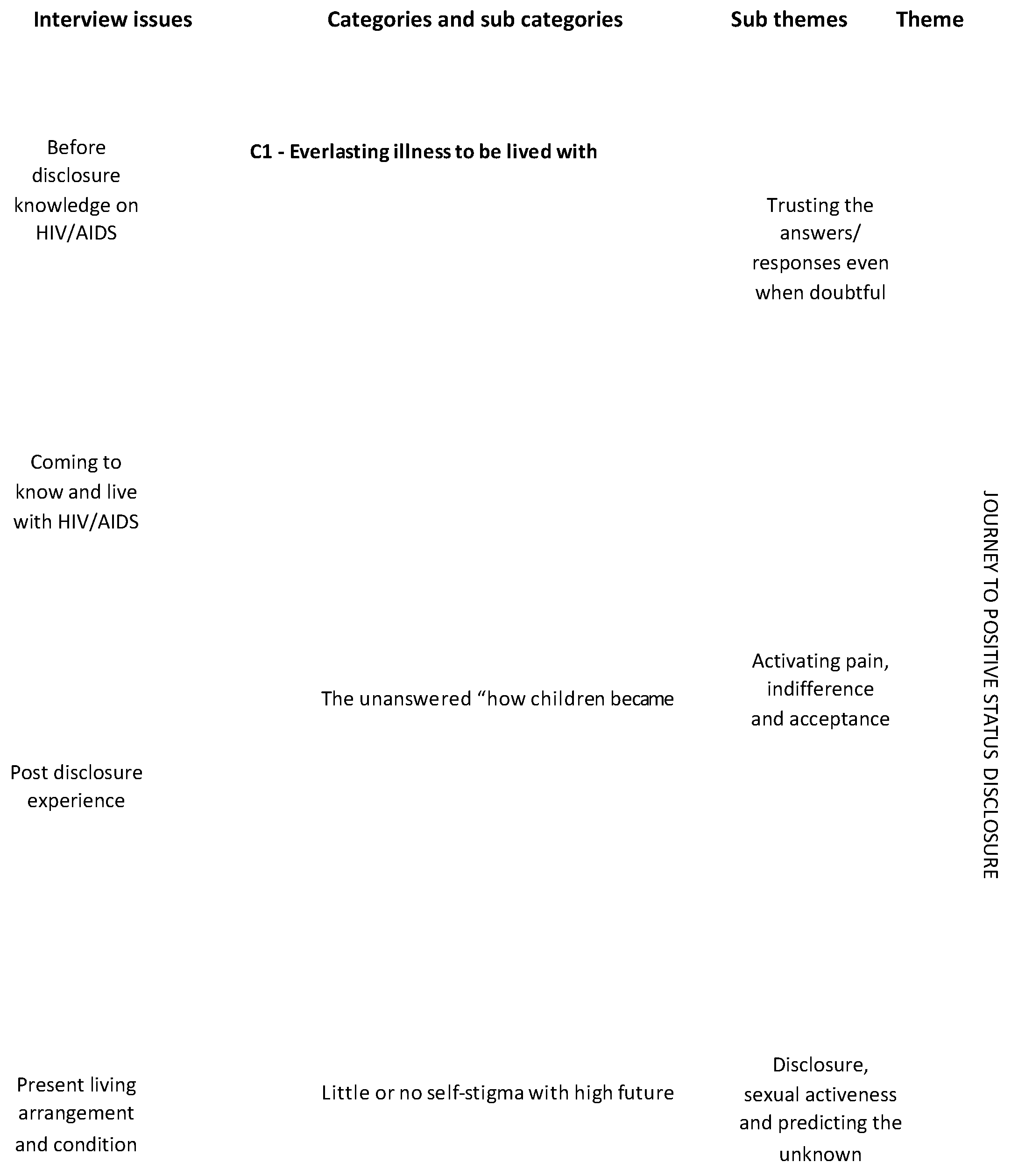
3.2. Study Emerging Themes
3.3. Pre-Disclosure Knowledge on HIV and AIDS
“My grandmother informed me after I persistently ask her why I have been taken [this] medicine every time and going to hospital almost every week. At first, she told me that my disease is scary and that if I don’t take the medicine, there will be rashes all over my body and I will die prematurely. Then I ask her the name of the disease. She calls me privately in her room and then disclose to me”.(Female, 14 years, Agogo, Southern Ghana)
“…I don’t know”.(Child 1, Child 3, Child 4, Child 7, Child 8, and Child 14)
“…actually from my step mum [was narrated to child by a step mother], they say it was through my mum and my dad”.(Female, 18 years, Tamale, Northern Ghana)
“…During the time I was in school, I felt sick and was rushed to the hospital. Then the doctor discovered it, I was about 12 years by that time”.(Female, 18 years, Tamale, Northern Ghana)
“I can’t remember. But I had a boil and came to hospital. It was then that it was discovered by the doctor”.(Male, 13 years, Tamale, Northern Ghana)
“…by having unprotected sex and secondary taking used blade, and transfer from parent to children”.(Female, 16 years, Tafo, Southern Ghana)
3.4. Disclosure Approach and Process
“The health official disclosed to my grandmother. My grandmother instructed me not to take oily foods, rice and corn related foods. I asked her why… Then she replied that it is because of my sickness. I asked what sickness?… But she refused to tell me. She then told me that if I should use razor blade and, as a result, there is a cut on me. Then if someone else uses the blade and gets a cut, the person will also be affected with my disease. So, I started thinking about it since I was taught by my science teacher that the use of infected blades or needles could cause HIV/AIDS. …Then I realized I am HIV positive, but my grandmother felt adamant and uncomfortable to disclose to me”.(Female, 17 years, Tafo, Southern Ghana)
“My mother disclosed to me privately, in the room. I was informed too late. I think I should have been informed earlier than the time I was actually informed”.(Female, 14 years, Bongo, Northern Ghana)
“When my father died, my mother came to take me away from my father’s home, my mother sent me to do the lab at the hospital and I was told… about 8 years ago [disclosure took place when the child was 7] …It was the doctor who told me at the hospital. I did not react in any way because I was young”.(Male, 15 years, Tafo, Southern Ghana)
3.5. Earliness or Lateness of Disclosure Nested in Preferred Ideal Age of Disclosure
“I think it should be above 3 years now… I feel I should have been informed earlier than the time I was informed”.(Male, 17 year, Agogo, Southern Ghana)
“When I was 17 that they informed me”.(Male, 18 years old male, Tamale, Northern Ghana)
“I was informed in 2012; which is 5 years ago…was too late. My mother should have informed me. I tried several times, but she failed to disclose to me”.(Female, 16 years, Tafo, Southern Ghana)
“I am 17 years; from Tafo Medoma. My parents are dead. I know is a dreadful disease, I can’t remember. But I had boil and came to hospital. It was then that it was discovered by the Doctor…Not long ago. Not even more than a month”.(Female, 17 years, Tafo, Southern Ghana)
“When I was in class 2, I was six years… It was normal, if they did not tell me in the earlier stage maybe I would not have been alive by now, my aunty knows about it, my aunt’s first daughter, they treat me well”.(Female, 16 year, Tafo, Southern Ghana)
“I can’t recall but it will be about 2-3 years now…I said to her its ok…Yeah, the timing was ok”.(Female,12 years, Navrongo, Northern Ghana)
“…I think disclosure should be made by examining the person’s psychological state and should not be done unexpectedly like what they did to me”.(Female, 17 years, Tafo, Southern Ghana)
“Privately like what my mother did; but the information should come early after status is known”.(Male, 14 years, Agogo, Southern Ghana)
“I think disclosure should be made immediately it is known but the patient should be made aware that HIV test is to be done. When the person gives the approval, then it can be tested and disclose to him or her”.(Female, 17 years, Agogo, Southern Ghana)
“…I think disclosure should be made by first encouraging the person, then you tell the person about the importance of the medication. After that, you can gradually unfold the information to the person. Whilst you tell the person, you still encourage the person that all is not lost”.(Male, 18 years, Offinso, Southern Ghana)
3.6. Immediate Reaction and Response to Disclosure News
“It pained me so I wept that very day…… I felt unhappy”.(Female, 14 years Bongo, Northern Ghana)
“…I felt very sorrowful. It really pained me”.(Female, 17 years, Agogo, Southern Ghana)
“…yes, what they did was paining me, getting old and telling me about it, …oh am okay with that”.(Female, 18 years, Tamale, Northern Ghana)
“So I read the label on the box and realise that it was HIV”.(Female, 14 years, Bongo, Northern Ghana)
“During the time I was in school, I felt sick and was rushed to the hospital. Then the Doctor discovered it, I was about 12 years by that time …I had ‘kooko(boils)’ and came to the hospital. Upon diagnosis by the Doctor, he disclosed to me about my HIV status. He asked me whether I am aware and I said no. I have not been informed by anyone…It really pained me. My mother then told me they shouldn’t have informed me at that very time. It should have been later. Then later, my mother approach me privately and explained everything to me concerning how I became HIV positive. She says she doesn’t know, whether it was a spiritually purchased illness for me or a blade that I might have used…Not at all. The doctor unexpectedly disclosed to me. In fact, I did not believe it but later I realized it was true. The disclosure was too instantaneous”.(Female, 18 years, Agogo, Southern Ghana)
“No, I don’t even have friends; I have somehow restricted myself from people around …and its something my mother has warned me about it…. It is sensitive situation. I have boyfriend but have never disclosed to him. My mother told me if I tell him, the relationship will break and I also don’t want to lose him. I don’t want to tell him because he will leave me”.(Female, 18 years, Agogo, Southern Ghana)
3.7. Medication Intake, Adherence and Coping Strategy
“I take every day---in the mornings and in the evenings …. it is my grandmother who encourages and ensures that I take the drugs well, sometimes I forget. I feel comfortable taking drugs at home since people do not say anything bad about the drug……It is the abdominal pains”.(Female, 16 years, Tongo, Northern Ghana)
“…one in morning and evening …it’s my life, and I have to depend on it, I just realize it’s a duty There was a day I forgot that I did not take, so they had to bring it to me, when I forgot, they had to bring it to me at work …when I forget, I quickly go and take but now I take it 7:00 in the morning …when you take the drugs, like, I don’t know how to put it, the drug is strong… No…I don’t feel anything. I don’t take the drugs at the worksite …no worse experience but when I don’t take then I have some bad experience”(Female, 18 years, Agogo, Southern Ghana)
“I take morning two…evening two. At first, I used to vomit. That was the first drugs…Yes. I used to vomit when I take that drug. But this new one, I am feeling good with it: I take every day---in the mornings and in the evenings…I know that it will strengthen my immune system and the viruses will be destroyed……Yes. Sometimes, I feel I am taking the drugs too frequently, so I pulse in some cases. Again, taking the drug is not a pleasant experience, at the work place, I take the drugs secretly so that people will not know”.(Female 18 years, Agogo, Southern Ghana)
“Sometimes, I am forced to skip my weekly visits to the hospital due to limited funds …Sometimes, I don’t eat in the afternoon due to financial problems. I have financial problem, the food we eat sometimes faces shortages; so I eat in the morning and in the evenings only. I eat twice a day. I wish that government will give positive HIV and AIDS children money to go to school. I have limited finance which affects my eating, transport and general living condition”.(Female, 18 years, Tamale, Northern Ghana)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- UNAIDS. Fact Sheet—Latest Global and Regional Statistics on the Status of the AIDS Epidemic. Available online: http://www.unaids.org/en/resources/documents/2018/UNAIDS_FactSheet (accessed on 17 February 2019).
- Kharsany, A.B.M.; Karim, Q.A. HIV infection and AIDS in Sub-Saharan Africa: Current status, challenges and opportunities. Open AIDS J. 2016, 10, 34. [Google Scholar] [CrossRef] [PubMed]
- WHO. HIV/AIDS; WHO: Geneva, Switzerland, 2017; p. 1. [Google Scholar]
- Ghana AIDS Commission. Summary of the 2016 HIV Sentinel Survey Report. 2016. Available online: http://ghanaids.gov.gh/gac1/aids_info.php (accessed on 18 February 2019).
- Unicef, National Aids Control Programe GHS. National Paediatric Acceleration Plan for HIV 2016–2020; National Aids Control Programe GHS: Accra, Ghana, 2016. [Google Scholar]
- Dako-Gyeke, P.; Dornoo, B.; Addo, S.A.; Atuahene, M.; Addo, N.A.; Yawson, A.E. Towards elimination of mother-to-child transmission of HIV in Ghana: An analysis of national programme data. Int. J. Equity Health 2016, 15, 5. [Google Scholar] [CrossRef] [PubMed]
- Progress Report: Global HIV/AIDS Response: Epidemic Update and Health Sector Progress towards Universal Access; World Health Organization: Geneva, Switzerland, 2011.
- Mutumba, M.; Bauermeister, J.A.; Harper, G.W.; Musiime, V.; Lepkowski, J.; Resnicow, K.; Snow, R.C. Psychological distress among Ugandan adolescents living with HIV: Examining stressors and the buffering role of general and religious coping strategies. Glob. Public Health 2017, 12, 1479–1491. [Google Scholar] [CrossRef]
- Wiener, L.; Mellins, C.A.; Marhefka, S.; Battles, H.B. Disclosure of an HIV diagnosis to children: History, current research, and future directions. J. Dev. Behav. Pediatr. JDBP 2007, 28, 155. [Google Scholar] [CrossRef] [PubMed]
- Watermeyer, J. ‘Are we allowed to disclose?’: A healthcare team’s experiences of talking with children and adolescents about their HIV status. Health Expect 2015, 18, 590–600. [Google Scholar] [CrossRef] [PubMed]
- Kabogo, J.; Muniu, E.; Wamunyokoli, F.; Musoke, R.; Songok, E. Evidence of reduced treatment adherence among HIV infected paediatric and adolescent populations in Nairobi at the onset of the UNAIDS Universal Test and Treat Program. BMC Res Notes 2018, 11, 134. [Google Scholar] [CrossRef]
- Dapaah, J.M. Attitudes and behaviours of health workers and the use of HIV/AIDS health care services. Nurs. Res. Pract. 2016, 2016, 5172497. [Google Scholar] [CrossRef] [PubMed]
- Appiah, S.C.Y.; Badu, E.; Dapaah, J.M.; Harriet, T.; Abubakar, M. Youth Friendliness of Sexual and Reproductive Health Service Delivery and Service Utilization in the Kwadaso Sub-Metro of the Ashanti Region, Ghana. Int. J. Innov. Appl. Stud. 2015, 10, 716–725. [Google Scholar]
- Brown, S.D.; Truog, R.D.; Johnson, J.A.; Ecker, J.L.; American Academy of Pediatrics Committee on Pediatrics AIDS. Disclosure of Illness Status to Children and Adolescents with HIV Infection. Pediatrics 1999, 103, 164–166. [Google Scholar]
- World Health Organization. Guideline on HIV Disclosure Counselling for Children up to 12 years of Age. WHO: Geneva, Switzerland, 2011. Available online: https://www.who.int/hiv/en/ (accessed on 18 February 2019).
- Paintsil, E.; Renner, L.; Antwi, S.; Dame, J.; Enimil, A.; Ofori-Atta, A.; Alhassan, A.; Ofori, I.P.; Cong, X.; Kyriakides, T.; et al. HIV knowledge, stigma, and illness beliefs among pediatric caregivers in Ghana who have not disclosed their child’s HIV status. AIDS Care 2015, 27 (Suppl. 1), 18–27. [Google Scholar] [CrossRef] [PubMed]
- Gyamfi, E.; Okyere, P.; Enoch, A.; Appiah-Brempong, E. Prevalence of, and barriers to the disclosure of HIV status to infected children and adolescents in a district of Ghana. BMC Int. Health Hum. Rights 2017, 17, 8. [Google Scholar] [CrossRef] [PubMed]
- Von Eckartsberg, R. Life-World Experience: Existential-Phenomenological Research Approaches in Psychology; University Press of America: Lanham, MD, USA, 1986. [Google Scholar]
- Creswell, J.W. Qualitative Inquiry and Research Design: Choosing among Five Traditions; Sage: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Sanders, P. Phenomenology: A new way of viewing organizational research. Acad. Manag. Rev. 1982, 7, 353–360. [Google Scholar] [CrossRef]
- Cohen, M.Z.; Kahn, D.L.; Steeves, R.H. Hermeneutic Phenomenological Research: A Practical Guide for Nurse Researchers; Sage Publications: Thousand Oaks, CA, USA, 2000. [Google Scholar]
- Davidsen, A.S. Phenomenological Approaches in Psychology and Health Sciences. Qual. Res. Psychol. 2013, 10, 318–339. [Google Scholar] [CrossRef] [PubMed]
- Paley, J. Phenomenology as Qualitative Research: A Critical Analysis of Meaning Attribution; Routledge: London, UK, 2016. [Google Scholar]
- Moustakas, C. Phenomenological Research Methods; Sage: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- Creswell, J.W.; Miller, D.L. Determining validity in qualitative inquiry. Theory Pract. 2000, 39, 124–130. [Google Scholar] [CrossRef]
- Angen, M.J. Evaluating interpretive inquiry: Reviewing the validity debate and opening the dialogue. Qual. Health Res. 2000, 10, 378–395. [Google Scholar] [CrossRef] [PubMed]
- Bryman, A. Social Research Methods; Oxford University Press: Oxford, UK, 2016. [Google Scholar]
- Okawa, S.; Mwanza-Kabaghe, S.; Mwiya, M.; Kikuchi, K.; Jimba, M.; Kankasa, C.; Ishikawa, N. Adolescents’ experiences and Their suggestions for hiV serostatus Disclosure in Zambia: A Mixed-Methods study. Front. Public Health 2017, 5, 326. [Google Scholar] [CrossRef]
- Cluver, L.D.; Hodes, R.J.; Toska, E.; Kidia, K.K.; Orkin, F.M.; Sherr, L.; Meinck, F. ‘HIV is like a tsotsi. ARVs are your guns’: Associations between HIV-disclosure and adherence to antiretroviral treatment among adolescents in South Africa. AIDS 2019, 29, S57–S65. [Google Scholar] [CrossRef]
- Moodley, K.; Myer, L.; Michaels, D.; Cotton, M. Paediatric HIV disclosure in South Africa-caregivers’ perspectives on discussing HIV with infected children. S. Afr. Med. J. 2006, 96, 201–204. [Google Scholar]
- Kallem, S.; Renner, L.; Ghebremichael, M.; Paintsil, E. Prevalence and pattern of disclosure of HIV status in HIV-infected children in Ghana. AIDS Behav. 2011, 15, 1121–1127. [Google Scholar] [CrossRef]
- Abebe, W.; Teferra, S. Disclosure of diagnosis by parents and caregivers to children infected with HIV: Prevalence associated factors and perceived barriers in Addis Ababa, Ethiopia. AIDS Care 2012, 24, 1097–1102. [Google Scholar] [CrossRef]
- Vaz, L.M.E.; Maman, S.; Eng, E.; Barbarin, O.A.; Tshikandu, T.; Behets, F. Patterns of disclosure of HIV-status to infected children in a sub-Saharan African setting. J. Dev. Behav. Pediatr. JDBP 2011, 32, 307. [Google Scholar] [CrossRef] [PubMed]
- Mburu, G.; Hodgson, I.; Kalibala, S.; Haamujompa, C.; Cataldo, F.; Lowenthal, E.D.; Ross, D. Adolescent HIV disclosure in Zambia: Barriers, facilitators and outcomes. J. Int. AIDS Soc. 2014, 17, 18866. [Google Scholar] [CrossRef] [PubMed]
- Okawa, S.; Yasuoka, J.; Ishikawa, N.; Poudel, K.C.; Ragi, A.; Jimba, M. Perceived social support and the psychological well-being of AIDS orphans in urban Kenya. AIDS Care 2011, 23, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- Mweemba, M.; Musheke, M.M.; Michelo, C.; Halwiindi, H.; Mweemba, O.; Zulu, J.M. “When am I going to stop taking the drug?” Enablers, barriers and processes of disclosure of HIV status by caregivers to adolescents in a rural district in Zambia. BMC Public Health 2015, 15, 1028. [Google Scholar] [CrossRef] [PubMed]
- Arrivé, E.; Ayaya, S.; Davies, M.A.; Chimbetete, C.; Edmonds, A.; Lelo, P.; Fong, S.M.; Razali, K.A.; Kouakou, K.; Duda, S.N.; et al. Models of support for disclosure of HIV status to HIV-infected children and adolescents in resource-limited settings. J. Int. AIDS Soc. 2018, 21, e25157. [Google Scholar] [CrossRef] [PubMed]
- UN General Assembly. UN General Assembly-Second Committee-Economic and Financial-List of Draft proposals United Nations. 2016. Available online: http://www.un.org/en/ga/second/67/proposals.shtml (accessed on 18 February 2019).
- Bettmann, J.E.; Mortensen, J.M.; Akuoko, K.O. Orphanage caregivers’ perceptions of children’s emotional needs. Child. Youth Serv. Rev. 2015, 49, 71–79. [Google Scholar] [CrossRef]
- Darkwah, E.; Daniel, M.; Asumeng, M. Caregiver perceptions of children in their care and motivations for the care work in children’s homes in Ghana: Children of God or children of white men? Child. Youth Serv. Rev. 2016, 66, 161–169. [Google Scholar] [CrossRef]
- UNICEF. The State of the World’s Children 2015:Reimagine the Future. Available online: http://sowc2015.unicef.org/ (accessed on 18 February 2019).
- Toth, G.; Mburu, G.; Tuot, S.; Khol, V.; Ngin, C.; Chhoun, P.; Yi, S. Social-support needs among adolescents living with HIV in transition from pediatric to adult care in Cambodia: Findings from a cross-sectional study. AIDS Res. Ther. 2018, 15, 8. [Google Scholar] [CrossRef]
- Wood, K.; Chase, E.; Aggleton, P. ‘Telling the truth is the best thing’: Teenage orphans’ experiences of parental AIDS-related illness and bereavement in Zimbabwe. Soc. Sci. Med. 2006, 63, 1923–1933. [Google Scholar] [CrossRef]
- Pinquart, M.; Sörensen, S. Correlates of physical health of informal caregivers: A meta-analysis. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2007, 62, 126–137. [Google Scholar] [CrossRef]
- Ke, X.; Liu, C.; Li, N. Social support and Quality of Life: A cross-sectional study on survivors eight months after the 2008 Wenchuan earthquake. BMC Public Health 2010, 10, 573. [Google Scholar] [CrossRef] [PubMed]
- Doku, P.N.; Dotse, J.E.; Mensah, K.A. Perceived social support disparities among children affected by HIV/AIDS in Ghana: A cross-sectional survey. BMC Public Health 2015, 15, 538. [Google Scholar] [CrossRef] [PubMed]
- GSS. 2010 Population and Housing Census: Summary Report of Final Results; Ghana Statistical Service: Accra, Ghana, 2012. [Google Scholar]
- Kenu, E.; Obo-Akwa, A.; Nuamah, G.B.; Brefo, A.; Sam, M.; Lartey, M. Knowledge and disclosure of HIV status among adolescents and young adults attending an adolescent HIV clinic in Accra, Ghana. BMC Res. Notes 2014, 7, 844. [Google Scholar] [CrossRef] [PubMed]
- Enimil, A.; Nugent, N.; Amoah, C.; Norman, B.; Antwi, S.; Ocran, J.; Kwara, A.; Barker, D.H. Quality of life among Ghanaian adolescents living with perinatally acquired HIV: A mixed methods study. AIDS Care 2016, 28, 460–464. [Google Scholar] [CrossRef] [PubMed]
- Aderomilehin, O.; Hanciles-Amu, A.; Ozoya, O.O. Perspectives and practice of HIV disclosure to children and adolescents by health-care providers and caregivers in sub-Saharan Africa: A systematic review. Front. Public Health 2016, 4, 166. [Google Scholar] [CrossRef] [PubMed]
- Laar, A.; Manu, A.; Laar, M.; El-Adas, A.; Amenyah, R.; Atuahene, K.; Quarshie, D.; Adjei, A.A.; Quakyi, I. Coping strategies of HIV-affected households in Ghana. BMC Public Health 2015, 15, 166. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| No | Region | Urban/Rural | Age (yrs) | Village/Town | ART Site Name | Northern/Southern Ghana |
|---|---|---|---|---|---|---|
| 1 | Upper East | Rural | 11 | Fiya | Tongo/ | Northern Ghana |
| 2 | Upper East | Urban | 11 | Bolga town | Bolgatanga RH | Northern Ghana |
| 3. | Upper East | Urban | 12 | Navrongo | Navrongo WMH | Northern Ghana |
| 4. | Upper East | Urban | 13 | Zuale | Bolgatanga RH | Northern Ghana |
| 5 | Upper East | Urban | 13 | Gambiago | Bolgatanga RH | Northern Ghana |
| 6 | Upper East | Rural | 14 | Sawla | Bongo | Northern Ghana |
| 7 | Upper East | Rural | 14 | Namong Awale | Bongo | Northern Ghana |
| 8 | Upper East | Urban | 16 | Fiya | Tongo | Northern Ghana |
| 9 | Upper East | Rural | 18 | Gamborige | Bongo | Northern Ghana |
| 10 | Northern | Rural | 10 | Savelugu | Walewale | Northern Ghana |
| 11 | Northern | Urban | 11 | Kanvin | Tamale TTH | Northern Ghana |
| 12 | Northern | Urban | 11 | Kanvin | Tamale TTH | Northern Ghana |
| 13 | Northern | Rural | 11 | Walewale | Walewale | Northern Ghana |
| 14 | Northern | Urban | 12 | Central | Tml Central | Northern Ghana |
| 15 | Northern | Rural | 13 | Savelugu | Savelugu | Northern Ghana |
| 16 | Northern | Urban | 13 | Central | Tml Central | Northern Ghana |
| 17 | Ashanti | Rural | 9 | Kyekyebiase | Agogo | Southern Ghana |
| 18 | Ashanti | Urban | 12 | Suntreso | Suntreso | Southern Ghana |
| 19 | Ashanti | Urban | 13 | Bantama | Suntreso | Southern Ghana |
| 20 | Ashanti | Rural | 14 | Agogo free Town | Agogo | Southern Ghana |
| 21 | Ashanti | Rural | 14 | Asaante Akyem Adomfe | Agogo | Southern Ghana |
| 22 | Ashanti | Urban | 15 | Atimatim | Tafo | Southern Ghana |
| 23 | Ashanti | Urban | 15 | Breman Nkontwoma | Tafo | Southern Ghana |
| 24 | Ashanti | Urban | 16 | Pankrono | Tafo | Southern Ghana |
| 25 | Ashanti | Rural | 16 | Asante Akyem | Agogo | Southern Ghana |
| 26 | Ashanti | Urban | 17 | Tafo Medoma | Tafo | Southern Ghana |
| 27 | Ashanti | Rural | 17 | Konongo Odumase | Agogo | Southern Ghana |
| 28 | Ashanti | Urban | 17 | Fawoade | Tafo | Southern Ghana |
| 29 | Ashanti | Rural | 18 | Offinso | Offinso | Southern Ghana |
| 30 | Ashanti | Rural | 18 | Konongo Zongo | Agogo | Southern Ghana |
| Theme | Sub Theme | Quotes |
|---|---|---|
| Pre-disclosure knowledge on HIV and AIDS | Knowing how children became infected with HIV and AIDS | -Male, 13 years from Gambiago:” I don’t know anything about it” -Female, 16 years from Agogo: “…HIV/AIDS is a disease which manifests in the blood; and once there is a blood contact between an infected and non-infected person, the non-infected person will be infected with the virus” - Male, 16 years from Tafo:” HIV/AIDS is a disease which manifests in the blood; and once there is a blood contact between an infected and non-infected person, the non-infected person will be infected with the virus” -Female, 13 years from Bolgatanga:” I have heard about it but no one has explained to me in details” -Female, 15 years from Nkwontwoma:” …yea, there is difference, HIV/AIDS… HIV is not very dangerous but AIDS is very dangerous…Yes, HIV is a virus…Yes, I know my status, ok, I will say HIV is a…. it looks like someone who is having a malaria parasite and went for medicine to reduce the level of malaria…but the AIDS when you get it, it’s the disease” |
| The disclosure approach and process | -Male, 18 years from Tamale:” I had ‘kooko’ and came to the hospital. Upon diagnosis by the Doctor, he disclosed to me about my HIV status. He asked me whether I am aware and I said; no. I have not been informed by anyone…When I was young, I didn’t know the reason for coming for the drugs always. Later I read about the drugs and realized that I have HIV. Again, my mother confirmed to it and some of the nurses later disclosed to me. I got ill and was admitted so was later told” -Male, 18 years from Offinso: “When I got ill and was admitted then my parents were also diagnosed” - Male, 13 years from Bolgatanga: “I was informed by a nurse” -Female 14 years from Agogo: “My grandmother disclosed to me at home. I was not happy about it at all. I came to seek medical attention and never expected to be tested for HIV/AIDS. So, when I was told about it, I could not believe it. It was later that I came for a lab test and it was confirmed” | |
| Earliness or lateness of disclosure nested in preferred ideal age of disclosure | -Male, 18 years from Tamale: “When I was 17 that they informed me, …yes, what they did was paining me, getting old and telling me about it, …oh am okay with that” -Female, 16 years from Agogo: “They waited for me to take the drugs for some time before disclosing it to me …I was pleased with the process of disclosure” -Female, 16 years from Tongo: “…Three years… I was informed too early” -Male, 17 years from Sangnerirukuku:” …months, my uncle sent me to the hospital … felt that the doctor has prescribed him the medicines so that’s all. all I know that it has been given to me by doctors, so I think that’s the right thing to do so they know what they are doing …Anytime I ask they tell me those things they always tell me, that I have something in my stomach” | |
| Reaction and response to disclosure news | - Female, 16 years from Agogo: “I felt sick and when I was sent to the hospital, it came out that I am HIV/AIDs positive…The doctor first informed my mother and she cried. When I asked her why? she failed to respond to me. Then a nurse called me and asked me whether I have had an intimacy with someone before and I said ‘No’. Then she asked my mother whether she has really found out from me concerning having intercourse with someone and she replied ‘Yes’. Later, the nurse called me and informed me privately. She told me not to feel sad…I felt sad and I still think about it… My mother should have informed me…I tried several times, but she failed to disclose to me” | |
| Medication intake and adherence | Coping strategy and food insecurity | -Male, 15 years from Tafo: “I take every day. Morning and evening…I feel healthy when I take the drugs… sometimes when I travel. I remember I went to Accra and stayed for about 8 months of which I did not take the drugs along” -Female, 16 years from Agogo:” I take every day---in the mornings and in the evenings…I know that it will strengthen my immune system and the viruses will be destroyed…Yes. Sometimes, I feel I am taking the drugs too frequently so I pulse in some cases. Again, taking the drug is not a pleasant experience, hence I sometimes take in the morning and skip the evening and vice versa…I feel comfortable taking drugs at home. At the work place, I take the drugs secretly so that people will not know” |
| Interview Issue | Southern Ghana | Northern Ghana |
|---|---|---|
| What do you know about the HIV/AIDs disease? | Child 1: “HIV/AIDs is a disease which manifests in the blood; and once there is a blood contact between an infected and non-infected person, the non-infected person will be infected with the virus” Child 3: “HIV/AIDs is a disease which affects the immune system” Child 4: “It is a disease that is very disturbing” Child 5: “HIV/AIDs is a disease which manifests in the blood; and once there is a blood contact between an infected and non-infected person, the non-infected person will be infected with the virus” Child 9: “I have heard about it before…I know difference…The difference is that if the HIV comes on you, you can have very quick treatment for it but the AIDS can easily kill you early” Child 10: “yea, there is difference, HIV/AIDS, …HIV is not very dangerous, but AIDS is very dangerous” | Child 6: “I have heard HIV lives in the body” Child 7: “I can’t tell” Child 8: “…they say it is a deadly disease but for me I don’t see it as a deadly disease” Child 11: “I know it’s a disease” Child 13: “I have heard about it but no one has explained to me in details” Child 14: “I don’t know anything about it” |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Appiah, S.C.Y.; Kroidl, I.; Hoelscher, M.; Ivanova, O.; Dapaah, J.M. A Phenomenological Account of HIV Disclosure Experiences of Children and Adolescents from Northern and Southern Ghana. Int. J. Environ. Res. Public Health 2019, 16, 595. https://doi.org/10.3390/ijerph16040595
Appiah SCY, Kroidl I, Hoelscher M, Ivanova O, Dapaah JM. A Phenomenological Account of HIV Disclosure Experiences of Children and Adolescents from Northern and Southern Ghana. International Journal of Environmental Research and Public Health. 2019; 16(4):595. https://doi.org/10.3390/ijerph16040595
Chicago/Turabian StyleAppiah, Seth Christopher Yaw, Inge Kroidl, Michael Hoelscher, Olena Ivanova, and Jonathan Mensah Dapaah. 2019. "A Phenomenological Account of HIV Disclosure Experiences of Children and Adolescents from Northern and Southern Ghana" International Journal of Environmental Research and Public Health 16, no. 4: 595. https://doi.org/10.3390/ijerph16040595