The Effect of Mechanically-Generated Vibrations on the Efficacy of Hemodialysis; Assessment of Patients’ Safety: Preliminary Reports


Abstract
:1. Introduction
2. Materials and Methods
2.1. Measurements
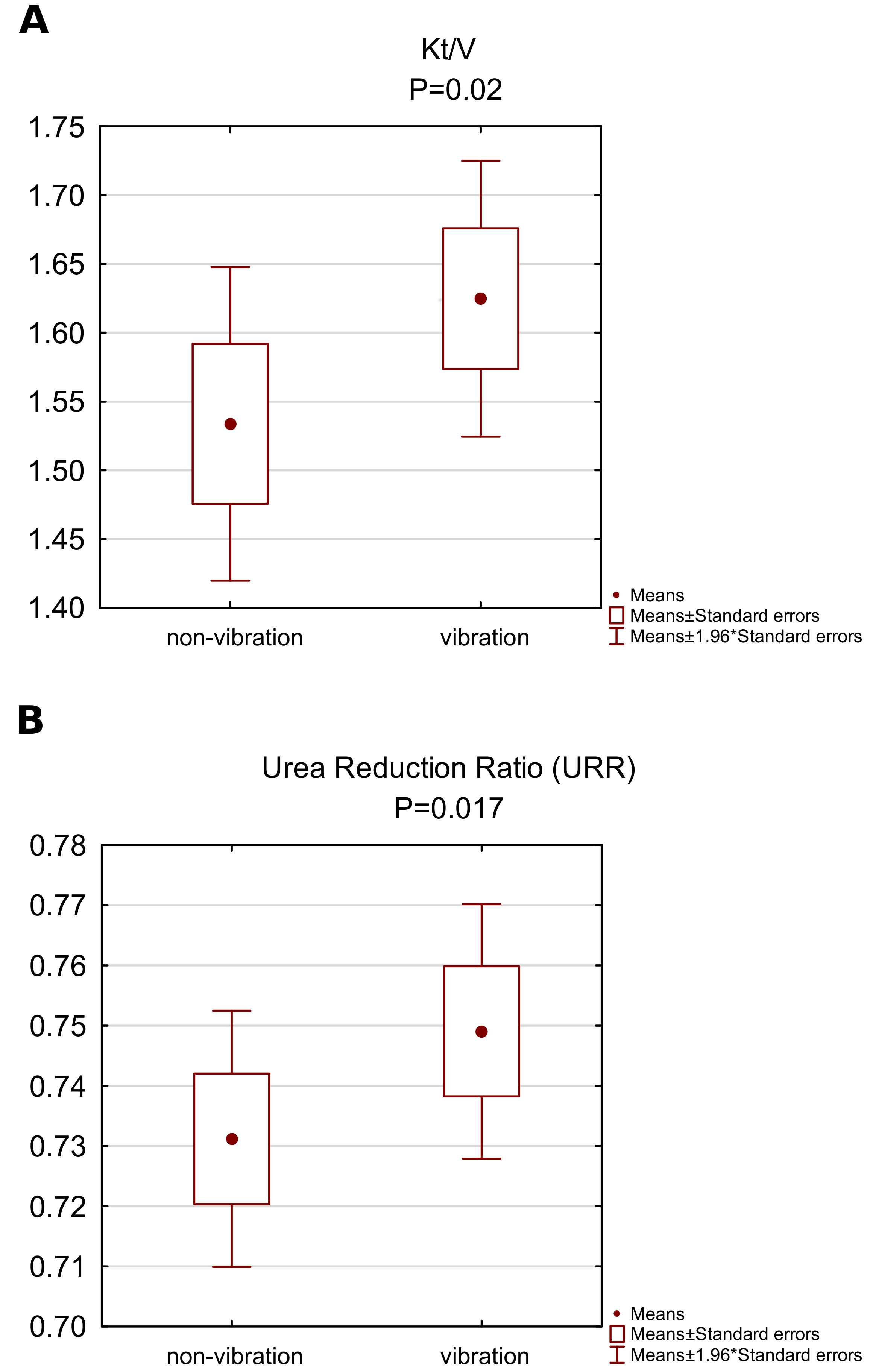
- The concentration of urea before and after the dialysis, based on which the urea reduction ratio (URR) values were calculated with the formula , where is post-dialysis blood urea nitrogen and is pre-dialysis blood urea nitrogen [13]
- The dialysis adequacy ratio () calculated using Daugirdas’ equation [14]
2.2. Description of the Intervention
2.3. Statistics
3. Results
3.1. The Influence of Vibrations on Dialysis Quality Measures
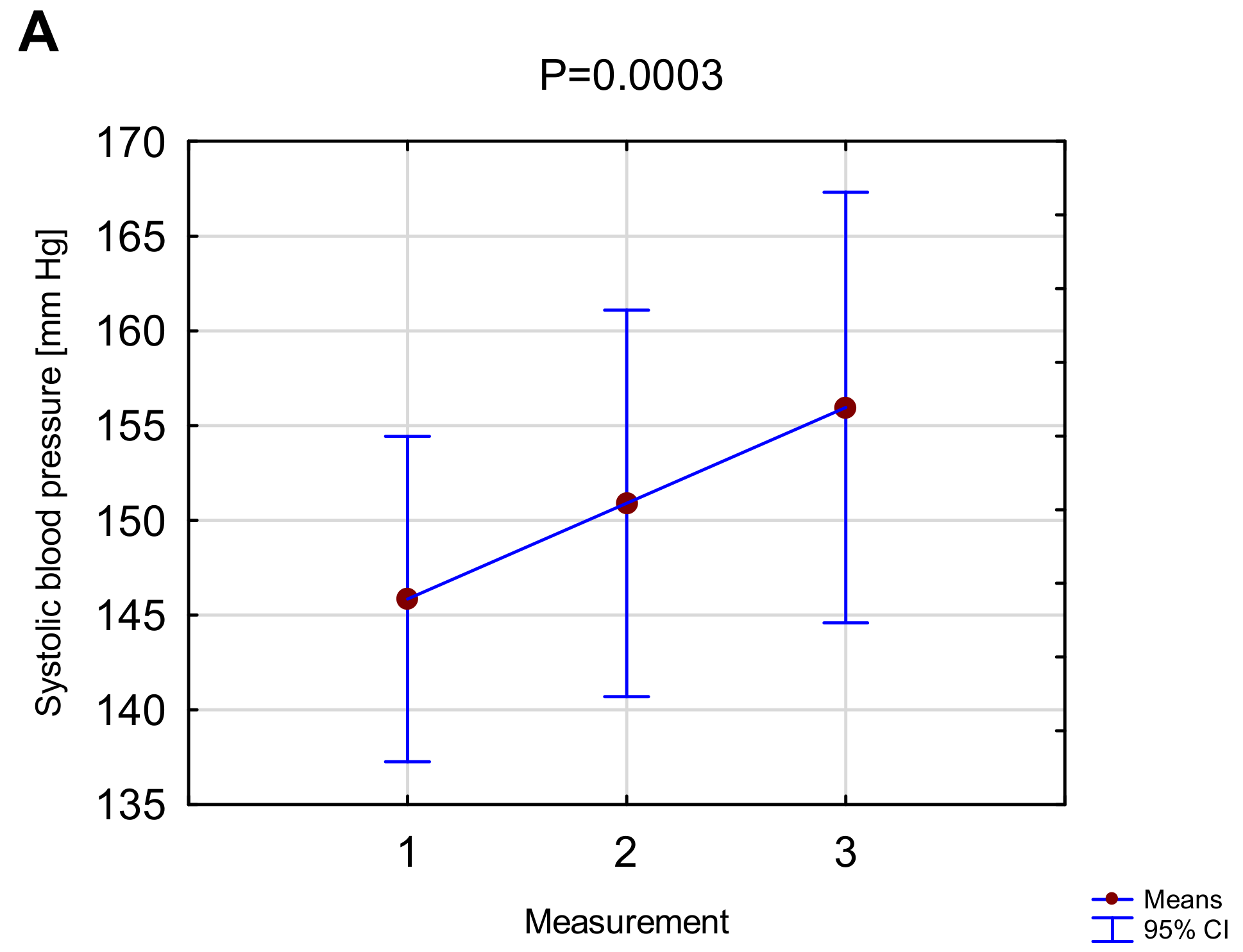
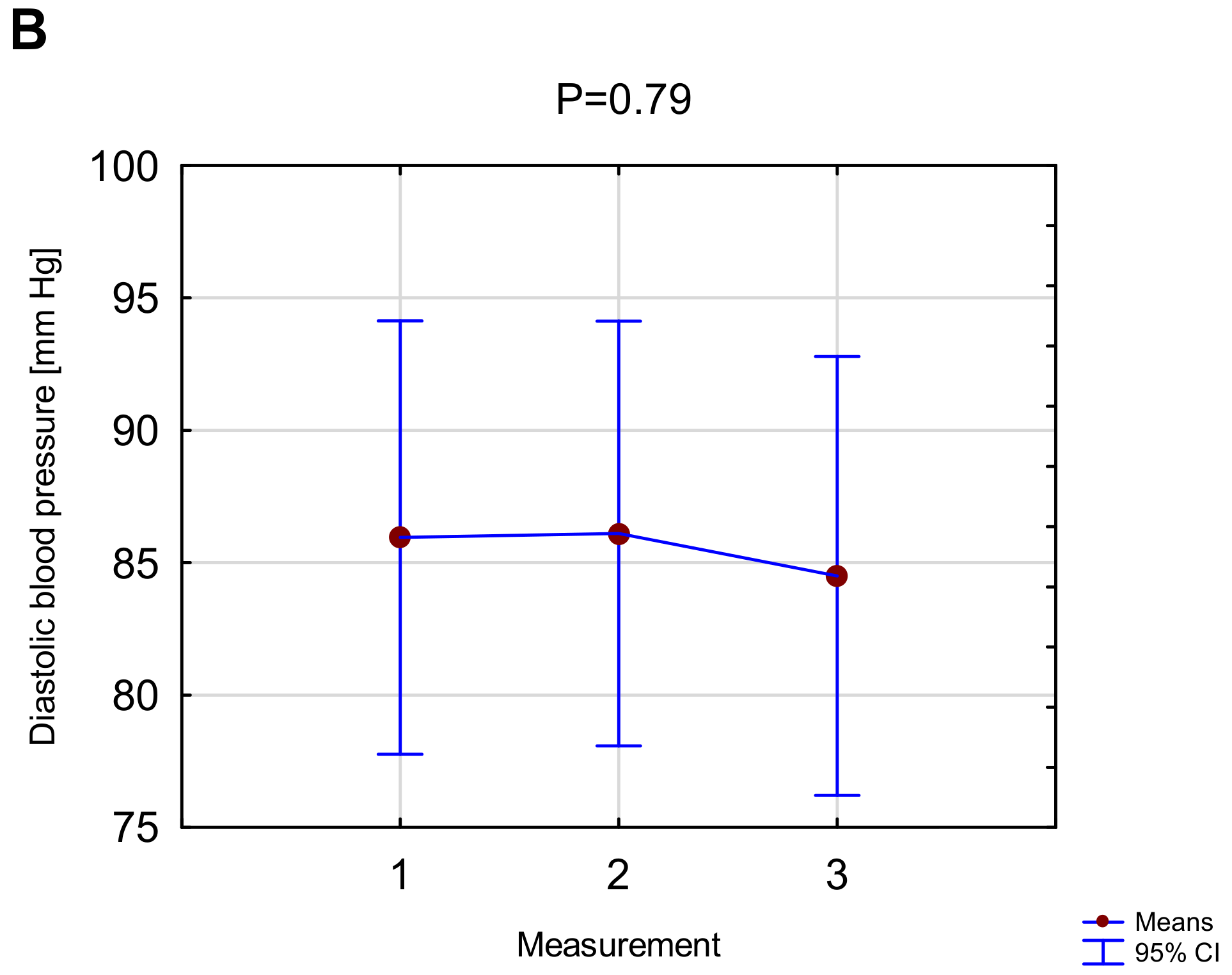
3.2. The Effect of Vibrations on Cardiovascular Function Indicators
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Glorieux, G.; Tattersall, J. Uraemic toxins and new methods to control their accumulation: Game changers for the concept of dialysis adequacy. Clin. Kidney J. 2015, 8, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Kazama, J.J.; Wakamatsu, T.; Takahashi, Y.; Kaneko, Y.; Goto, S.; Narita, I. Removal of uremic toxins by renal replacement therapies: A review of current progress and future perspectives. Ren. Replace. Ther. 2016, 2, 43. [Google Scholar] [CrossRef]
- Montgomery, L.D.; Montgomery, R.W.; Gerth, W.A.; Lew, S.Q.; Klein, M.D.; Stewart, J.M.; Medow, M.S.; Velasquez, M.T. Bioimpedance monitoring of cellular hydration during hemodialysis therapy. Hemodial. Int. 2016, 21, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Minutolo, R.; Bellizzi, V.; Cioffi, M.; Iodice, C.; Giannattasio, P.; Andreucci, M.; Terracciano, V.; Di Iorio, B.R.; Conte, G.; De Nicola, L. Postdialytic Rebound of Serum Phosphorus: Pathogenetic and Clinical Insights. J. Am. Soc. Nephrol. 2002, 13, 1046–1054. [Google Scholar] [PubMed]
- Barcellos, F.C.; Santos, I.S.; Umpierre, D.; Bohlke, M.; Hallal, P.C. Effects of exercise in the whole spectrum of chronic kidney disease: A systematic review. Clin. Kidney J. 2015, 8, 753–765. [Google Scholar] [CrossRef]
- Kirkman, D.L.; Roberts, L.D.; Kelm, M.; Wagner, J.; Jibani, M.M.; Macdonald, J.H. Interaction between Intradialytic Exercise and Hemodialysis Adequacy. Am. J. Nephrol. 2013, 38, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Giannaki, C.D.; Hadjigeorgiou, G.M.; Karatzaferi, C.; Maridaki, M.D.; Koutedakis, Y.; Founta, P.; Tsianas, N.; Stefanidis, I.; Sakkas, G.K. A single-blind randomized controlled trial to evaluate the effect of 6 months of progressive aerobic exercise training in patients with uraemic restless legs syndrome. Nephrol. Dial. Transplant. 2013, 28, 2834–2840. [Google Scholar] [CrossRef] [Green Version]
- Hazell, T.J.; Lemon, P.W.R. Synchronous whole-body vibration increases VO2 during and following acute exercise. Eur. J. Appl. Physiol. 2011, 112, 413–420. [Google Scholar] [CrossRef]
- Da Silva-Grigoletto, M.E.; Vaamonde, D.M.; Castillo, E.; Poblador, M.S.; García-Manso, J.M.; Lancho, J.L. Acute and Cumulative Effects of Different Times of Recovery From Whole Body Vibration Exposure on Muscle Performance. J. Strength Cond. Res. 2009, 23, 2073–2082. [Google Scholar] [CrossRef]
- Xie, L.; Jacobson, J.M.; Choi, E.S.; Busa, B.; Donahue, L.R.; Miller, L.M.; Rubin, C.T.; Judex, S. Low-level mechanical vibrations can influence bone resorption and bone formation in the growing skeleton. Bone 2006, 39, 1059–1066. [Google Scholar] [CrossRef]
- Von Stengel, S.; Kemmler, W.; Engelke, K.; Kalender, W.A. Effect of whole-body vibration on neuromuscular performance and body composition for females 65 years and older: A randomized-controlled trial. Scand. J. Med. Sci. Sports 2010, 22, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowrie, E. The urea reduction ratio (URR): A simple method for evaluating hemodialysis treatment. Contemp. Dial. Nephrol. 1991, 12, 11–20. [Google Scholar]
- Daugirdas, J.T. Second generation logarithmic estimates of single-pool variable volume Kt/V: An analysis of error. J. Am. Soc. Nephrol. 1993, 4, 1205–1213. [Google Scholar] [PubMed]
- Maduell, F.; Ramos, R.; Varas, J.; Martin-Malo, A.; Molina, M.; Pérez-Garcia, R.; Marcelli, D.; Moreso, F.; Aljama, P.; Merello, J.I. Hemodialysis patients receiving a greater Kt dose than recommended have reduced mortality and hospitalization risk. Kidney Int. 2016, 90, 1332–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Held, P.J.; Port, F.K.; Wolfe, R.A.; Stannard, D.C.; Carroll, C.E.; Daugirdas, J.T.; Bloembergen, W.E.; Greer, J.W.; Hakim, R.M. The dose of hemodialysis and patient mortality. Kidney Int. 1996, 50, 550–556. [Google Scholar] [CrossRef] [Green Version]
- Molina Núñez, M.; Roca Meroño, S.; de Alcorcon Jimenez, R.; Hernández, G.; Jimeno Griño, C.; Alvarez Fernandez, G.; Navarro Parreño, M.; Pérez Silva, F. Kt calculation as a quality indicator of haemodialysis adequacy. Nefrologia 2010, 30, 331–336. [Google Scholar] [PubMed]
- Locatelli, F.; Buoncristiani, U.; Canaud, B.; Kohler, H.; Petitclerc, T.; Zucchelli, P. Dialysis dose and frequency. Nephrol. Dial. Transplant. 2004, 20, 285–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daugirdas, J.T.; Depner, T.A.; Inrig, J.; Mehrotra, R.; Rocco, M.V.; Suri, R.S.; Weiner, D.E.; Greer, N.; Ishani, A.; MacDonald, R.; et al. KDOQI Clinical Practice Guideline for Hemodialysis Adequacy: 2015 update. Am. J. Kidney Dis. 2015, 66, 884–930. [Google Scholar] [CrossRef] [PubMed]
- Pérez-García, R.; Jaldo, M.; Alcázar, R.; de Sequera, P.; Albalate, M.; Puerta, M.; Ortega, M.; Ruiz, M.C.; Corchete, E. Unlike Kt, high Kt/V is associated with greater mortality: The importance of low V. Nefrologia 2019, 39, 58–66. [Google Scholar] [CrossRef]
- Oreopoulos, D.G. Beyond Kt/V: redefining adequacy of dialysis in the 21st century. Int. Urol. Nephrol. 2002, 34, 393–403. [Google Scholar] [CrossRef]
- Abbas, H.N.; Rabbani, M.A.; Safdar, N.; Murtaza, G.; Maria, Q.; Ahamd, A.; et al. Biochemical nutritional parameters and their impact on hemodialysis efficiency. Saudi J. Kidney Dis. Transpl. 2009, 20, 1105–1109. [Google Scholar] [PubMed]
- Chandrashekar, A.; Ramakrishnan, S.; Rangarajan, D. Survival analysis of patients on maintenance hemodialysis. Indian J. Nephrol. 2014, 24, 206–213. [Google Scholar] [CrossRef]
- Załuska, W.; Klinger, M.; Kusztal, M.; Lichodziejewska-Niemierko, M.; Miłkowski, A.; Stompór, T.; Sak, J.; Domański, L.; Drożdż, M.; Aksamit, D.; et al. Recommendations of the Working Group of the Polish Society of Nephrology for the criteria of quality treatment in dialysis patients with end-stage renal disease. Nefrol. Dial. Pol. 2015, 19, 6–11. [Google Scholar]
- Kosmadakis, G.; Bevington, A.; Smith, A.; Clapp, E.; Viana, J.; Bishop, N.; Feehally, J. Physical Exercise in Patients with Severe Kidney Disease. Nephron Clin. Pract. 2010, 115, c7–c16. [Google Scholar] [CrossRef] [PubMed]
- Nowicki, M.; Jagodzińska, M.; Murlikiewicz, K.; Niewodniczy, M.; et al. Physical activity in dialysed patients—A comparison of different methods of its improvement. Post. Nauk Med. 2009, 10, 799–804. [Google Scholar]
- Smart, N.; McFarlane, J.; Cornelissen, V. The Effect of Exercise Therapy on Physical Function, Biochemistry and Dialysis Adequacy in Haemodialysis Patients: A Systematic Review and Meta-Analysis. Open J. Nephrol. 2013, 3, 25–36. [Google Scholar] [CrossRef]
- Liao, M.T.; Liu, W.C.; Lin, F.H.; Huang, C.F.; Chen, S.Y.; Liu, C.C.; Lin, S.H.; Lu, K.C.; Wu, C.C. Intradialytic aerobic cycling exercise alleviates inflammation and improves endothelial progenitor cell count and bone density in hemodialysis patients. Medicine 2016, 95, e4134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, H.M.L.; March, D.S.; Graham-Brown, M.P.M.; Jones, A.W.; Curtis, F.; Grantham, C.S.; Churchward, D.R.; Highton, P.; Smith, A.C.; Singh, S.J.; et al. Effects of intradialytic cycling exercise on exercise capacity, quality of life, physical function and cardiovascular measures in adult haemodialysis patients: A systematic review and meta-analysis. Nephrol. Dial. Transplant. 2018, 33, 1436–1445. [Google Scholar] [CrossRef] [PubMed]
- Bohm, C.; Stewart, K.; Onyskie-Marcus, J.; Esliger, D.; Kriellaars, D.; Rigatto, C. Effects of intradialytic cycling compared with pedometry on physical function in chronic outpatient hemodialysis: A prospective randomized trial. Nephrol. Dial. Transplant. 2014, 29, 1947–1955. [Google Scholar] [CrossRef]
- Dungey, M.; Bishop, N.C.; Young, H.M.; Burton, J.O.; Smith, A.C. The Impact of Exercising During Haemodialysis on Blood Pressure, Markers of Cardiac Injury and Systemic Inflammation—Preliminary Results of a Pilot Study. Kidney Blood Press. Res. 2015, 40, 593–604. [Google Scholar] [CrossRef] [PubMed]
- Delgado, C.; Johansen, K.L. Barriers to exercise participation among dialysis patients. Nephrol. Dial. Transplant. 2011, 27, 1152–1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farese, S.; Budmiger, R.; Aregger, F.; Bergmann, I.; Frey, F.J.; Uehlinger, D.E. Effect of Transcutaneous Electrical Muscle Stimulation and Passive Cycling Movements on Blood Pressure and Removal of Urea and Phosphate During Hemodialysis. Am. J. Kidney Dis. 2008, 52, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Stenvinkel, P.; Carrero, J.J.; von Walden, F.; Ikizler, T.A.; Nader, G.A. Muscle wasting in end-stage renal disease promulgates premature death: Established, emerging and potential novel treatment strategies. Nephrol. Dial. Transplant. 2015, 31, 1070–1077. [Google Scholar] [CrossRef]
- Cardinale, M.; Pope, M. The effects of whole body vibration on humans: Dangerous or advantageous? Acta Physiol. Hung. 2003, 90, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Chanou, K.; Gerodimos, V.; Karatrantou, K.; Jamurtas, A. Whole-body vibration and rehabilitation of chronic diseases: a review of the literature. J. Sports Sci. Med. 2012, 11, 187–200. [Google Scholar] [PubMed]
- Donald Whedon, G.; Deitrick, J.E.; Shorr, E.; Toscani, V.; Buniak Davis, V.; Stevens, E. Modification of the effects of immobilization upon metabolic and physiologic functions of normal men by the use of an oscillating bed. Am. J. Med. 1949, 6, 684–711. [Google Scholar] [CrossRef]
- Dionello, C.; Sá-Caputo, D.; Pereira, H.; Sousa-Gonçalves, C.; Maiworm, A.; Morel, D.; Moreira-Marconi, E.; Paineiras-Domingos, L.; Bemben, D.; Bernardo-Filho, M. Effects of whole body vibration exercises on bone mineral density of women with postmenopausal osteoporosis without medications: novel findings and literature review. J. Musculoskelet. Neuronal. Interact. 2016, 16, 193–203. [Google Scholar]
- Seefried, L.; Genest, F.; Luksche, N.; Schneider, M.; Fazeli, G.; Brandl, M.; Bahner, U.; Heidland, A. Efficacy and safety of whole body vibration in maintenance hemodialysis patients—A pilot study. J. Musculoskelet. Neuronal. Interact. 2017, 17, 268–274. [Google Scholar]
- Doyle, A.; Chalmers, K.; Chinn, D.J.; McNeill, F.; Dall, N.; Grant, C.H. The utility of whole body vibration exercise in haemodialysis patients: A pilot study. Clin. Kidney J. 2017, 10, 822–829. [Google Scholar] [CrossRef]
- Sitja-Rabert, M.; Rigau, D.; Fort Vanmeerghaeghe, A.; Romero-Rodriguez, D.; Bonastre Subirana, M.; Bonfill, X. Efficacy of whole body vibration exercise in older people: a systematic review. Disabil. Rehabil. 2012, 34, 883–893. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, J.; Takeda, T.; Sato, Y.; Uzawa, M. Effect of whole-body vibration exercise on lumbar bone mineral density, bone turnover, and chronic back pain in post-menopausal osteoporotic women treated with alendronate. Aging Clin. Exp. Res. 2005, 17, 157–163. [Google Scholar] [CrossRef]
- Rees, S.S.; Murphy, A.J.; Watsford, M.L. Effects of whole body vibration on postural steadiness in an older population. J. Sci. Med. Sport 2009, 12, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Machado, A.; García-López, D.; González-Gallego, J.; Garatachea, N. Whole-body vibration training increases muscle strength and mass in older women: A randomized-controlled trial. Scand. J. Med. Sci. Sports 2009, 20, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Uehara, A.; Kurata, C.; Sugi, T.; Mikami, T.; Yamazaki, K.; Satoh, H.; Watanabe, H.; Terada, H. Peak Systolic Blood Pressure in Exercise Testing is Associated With Scintigraphic Severity of Myocardial Ischemia in Patients With Exercise-Induced ST-Segment Depression. Jpn. Circ. J. 2000, 64, 590–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henrique, D.M.N.; Reboredo, M.d.M.; Chaoubah, A.; Paula, R.B.d. Aerobic exercise improves physical capacity in patients under chronic hemodialysis. Arq. Bras. Cardiol. 2010, 94, 823–828. [Google Scholar] [CrossRef] [PubMed]
- McGuire, S.; Horton, E.J.; Renshaw, D.; Jimenez, A.; Krishnan, N.; McGregor, G. Hemodynamic Instability during Dialysis: The Potential Role of Intradialytic Exercise. BioMed Res. Int. 2018, 2018, 8276912. [Google Scholar] [CrossRef] [PubMed]
- Madhavan, G.; Cole, J.P.; Pierce, C.S.; McLeod, K.J. Reversal of Lower Limb Venous and Lymphatic Pooling by Passive Non-Invasive Calf Muscle Pump Stimulation. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 2875–2877. [Google Scholar] [CrossRef]
- Fuzari, H.K.; Dornelas de Andrade, A.; A Rodrigues, M.; I Medeiros, A.; F Pessoa, M.; Lima, A.M.; Cerqueira, M.S.; Marinho, P.E. Whole body vibration improves maximum voluntary isometric contraction of knee extensors in patients with chronic kidney disease: A randomized controlled trial. Physiother. Theory Pract. 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R. How can we prevent intradialytic hypotension? Curr. Opin. Nephrol. Hypertens. 2012, 21, 593–599. [Google Scholar] [CrossRef]
- Mueller, B.A.; Jasiak, K.D.; Thiel, S.R.; Stevenson, J.M.; Vilay, A.M.; Scoville, B.A.; Churchwell, M.D.; Pasko, D.A.; Perkins, N. Vibration Enhances Clearance of Solutes With Varying Molecular Weights During In Vitro Hemodialysis. ASAIO J. 2013, 59, 140–144. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Study Group (HD) | |
|---|---|---|
| Age (years) | (range = 27–86) | |
| Sex, female/male, n (%) | 8 (38)/13 (62) | |
| Dialysis vintage (months) | (range = 3–84) | |
| Duration of dialysis (min) | (range = 240–270) | |
| Weekly dialysis time (min) | (range = 630–980) | |
| Dialysis adequacy () | (range = 1.28–2.07) | |
| URR | (range = 0.67–0.86) | |
| Dialysis fluid flow (mL/min) | (range = 500–600) | |
| BFR during dialysis (mL/min) | (range = 280–330) | |
| Temperature of the dialysis fluid (°C) | (range = 35.0–37.0) | |
| BMI (kg/m2) | (range = 19.6–30.8) | |
| Target body weight (kg) | (range = 52–90) | |
| Residual renal function (mL) | (range = 0–2000) | |
| nPCR (g/kg per day) | (range = 0.6–1.53) | |
| Vascular access, n (%) | ||
| arteriovenous fistulas | 17 (81) | |
| central venous catheters | 4 (19) | |
| Cause of end-stage renal disease, n (%) | ||
| glomerulonephritis | 6 (28.5) | |
| diabetic renal disease | 4 (19.0) | |
| hypertension nephropathy | 4 (19.0) | |
| other | 7 (33.5) | |
| CCI (point) | (range = 2–9) | |
| Estimated GFR (mL/min/1.73 m2) | ||
| Ultrafiltration volume (L) | (range = 0.5–3.5) | |
| Hemoglobin (g/dL) | (range = 8.0–12.1) | |
| Transferrin saturation (%) | (range = 15–58) | |
| Ferritin (ng/mL) | (range = 35–1622) | |
| Creatinine (mg/dL) | (range = 3.9–10.8) | |
| Urea, predialysis (mmol/L) | (range = 8.3–28.7) | |
| Urea, postdialysis (mmol/L) | (range = 1.5–9.5) | |
| Sodium (mmol/dL) | (range = 136–141) | |
| Potassium (mmol/dL) | (range = 4.45–5.87) | |
| Albumin (g/L) | (range = 35–44) | |
| Phosphorus (inorganic) (mg/dL) | (range = 3.0–7.5) | |
| Calcium (mg/dL) | (range = 8.1–10.7) | |
| PTH (pg/mL) | (range = 152–724) |
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hornik, B.; Duława, J.; Marcisz, C.; Korchut, W.; Durmała, J. The Effect of Mechanically-Generated Vibrations on the Efficacy of Hemodialysis; Assessment of Patients’ Safety: Preliminary Reports. Int. J. Environ. Res. Public Health 2019, 16, 594. https://doi.org/10.3390/ijerph16040594
Hornik B, Duława J, Marcisz C, Korchut W, Durmała J. The Effect of Mechanically-Generated Vibrations on the Efficacy of Hemodialysis; Assessment of Patients’ Safety: Preliminary Reports. International Journal of Environmental Research and Public Health. 2019; 16(4):594. https://doi.org/10.3390/ijerph16040594
Chicago/Turabian StyleHornik, Beata, Jan Duława, Czesław Marcisz, Wojciech Korchut, and Jacek Durmała. 2019. "The Effect of Mechanically-Generated Vibrations on the Efficacy of Hemodialysis; Assessment of Patients’ Safety: Preliminary Reports" International Journal of Environmental Research and Public Health 16, no. 4: 594. https://doi.org/10.3390/ijerph16040594