Threshold Effects of PM2.5 Exposure on Particle-Related Mortality in China


Abstract
1. Introduction
2. Research Background
2.1. Energy Consumption and
2.2. and Mortality
2.3. The Relationship between and Mortality Rate
3. Methodology
3.1. Panel Regression Model
3.2. Panel Threshold Models
3.2.1. Theoretical Model
3.2.2. Empirical Model
3.3. Data Set
4. Results
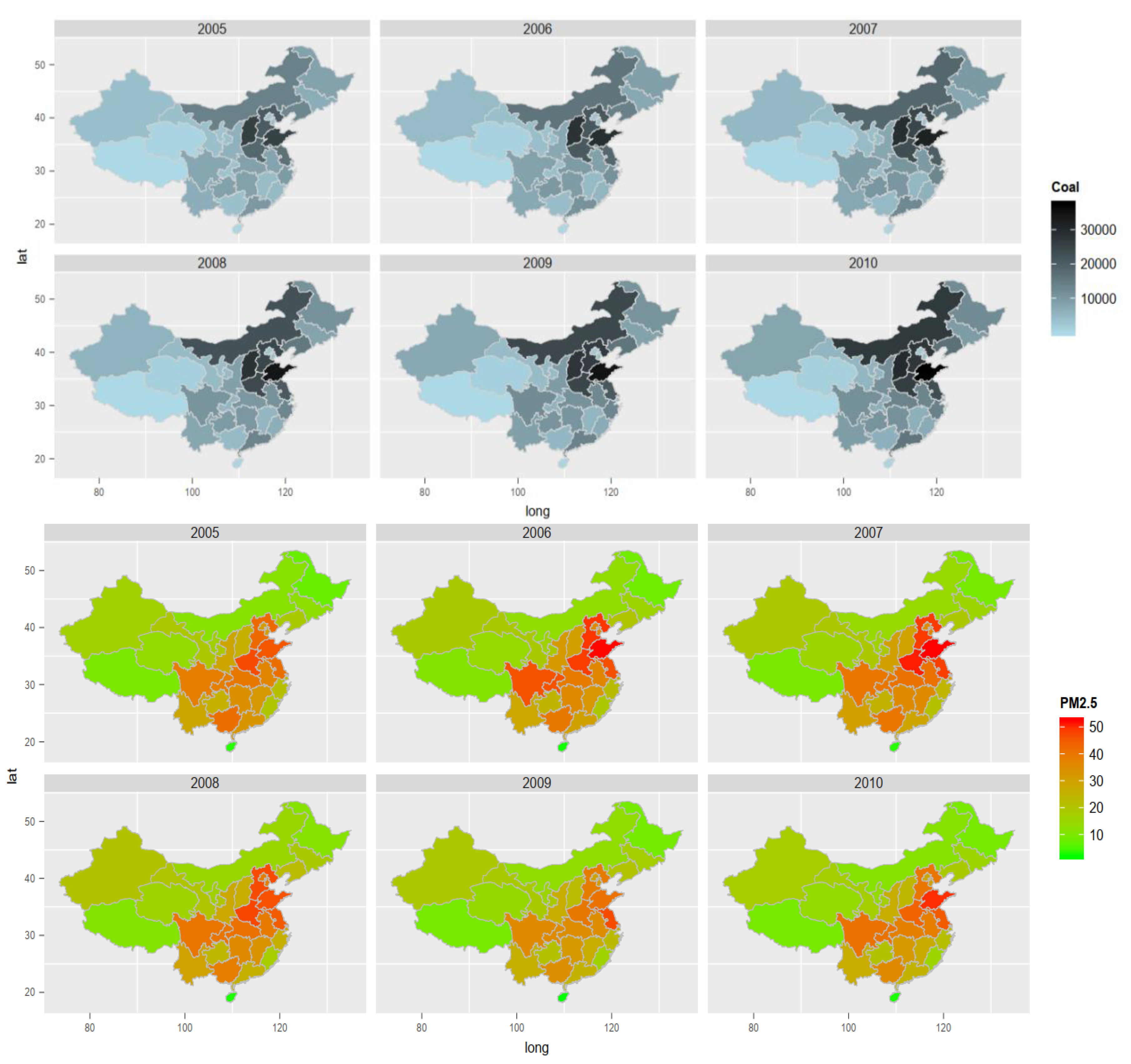
4.1. Estimating the Environmental Impacts of Fossil Fuel Consumption
4.2. Estimating Multiple Threshold Effects of on Mortality
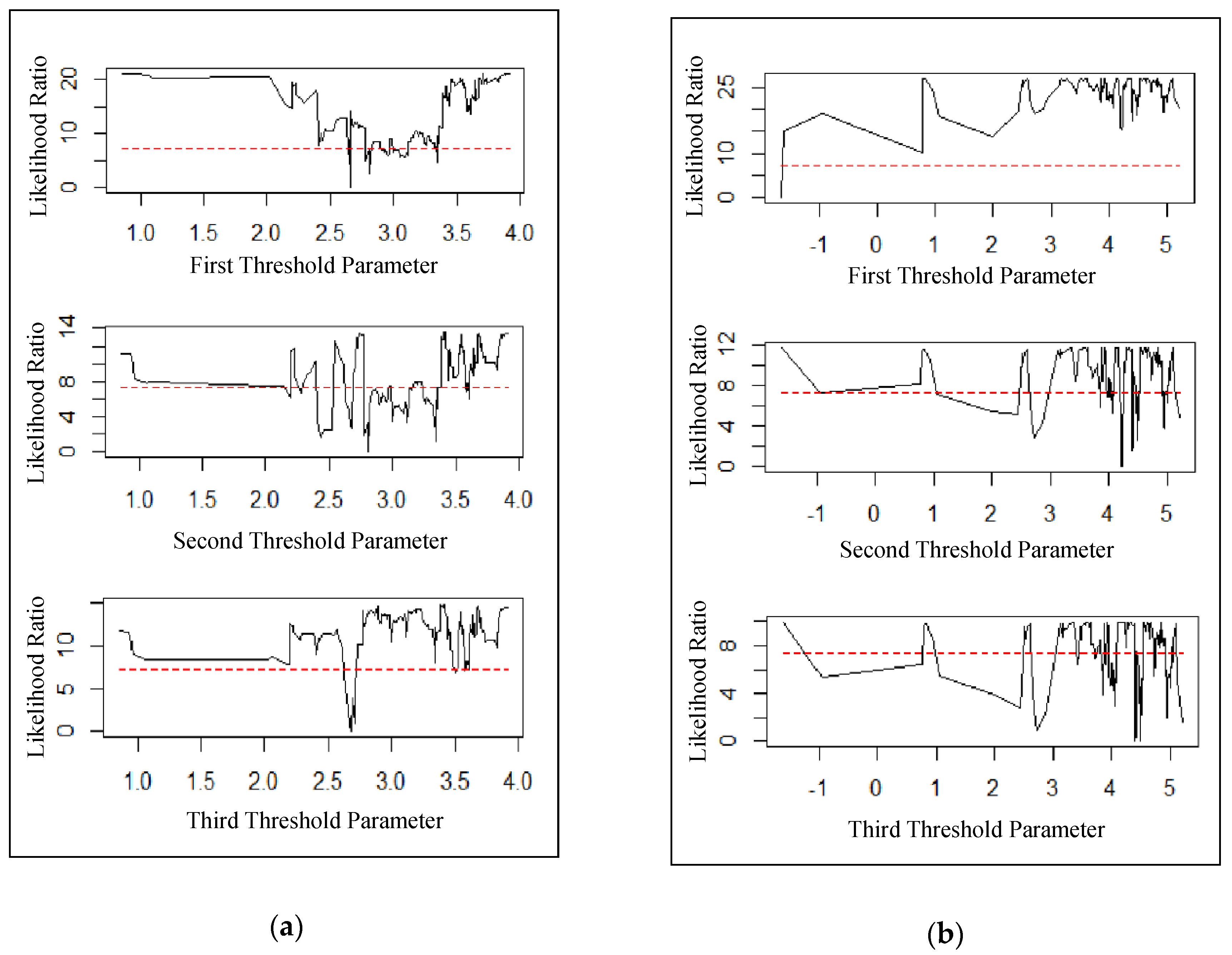
4.2.1. Testing for Multiple Thresholds
4.2.2. Estimated Effects of on Cause-Specific Mortality Rate
4.2.3. Two-stage Econometric Approach for Health Effects of Coal Consumption
5. Discussion
6. Conclusions
6.1. Contribution of the Study
6.2. Implications of the Study
6.3. Limitations of the Study
6.4. Recommendations for Further Research
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nemmar, A.; Hoet, P.M.; Vanquickenborne, B.; Dinsdale, D.; Thomeer, M.; Hoylaerts, M.; Vanbilloen, H.; Mortelmans, L.; Nemery, B. Passage of inhaled particles into the blood circulation in humans. Circulation 2002, 105, 411–414. [Google Scholar] [CrossRef]
- Oberdörster, G.; Sharp, Z.; Atudorei, V.; Elder, A.; Gelein, R.; Lunts, A.; Kreyling, W.; Cox, C. Extrapulmonary translocation of ultrafine carbon particles following whole-body inhalation exposure of rats. J. Toxicol. Environ. Health A 2002, 65, 1531–1543. [Google Scholar] [CrossRef]
- He, X.; Zhang, H.; Ma, Y.; Bai, W.; Zhang, Z.; Lu, K.; Ding, Y.; Zhao, Y.; Chai, Z. Lung deposition and extrapulmonary translocation of nano-ceria after intratracheal instillation. Nanotechnology 2010, 21, 285103. [Google Scholar] [CrossRef]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A.; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A. Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American Heart Association. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef]
- Chiu, H.-F.; Tsai, S.-S.; Weng, H.-H.; Yang, C.-Y. Short-term effects of fine particulate air pollution on emergency room visits for cardiac arrhythmias: A case-crossover study in Taipei. J. Toxicol. Environ. Health A 2013, 76, 614–623. [Google Scholar] [CrossRef]
- Franklin, M.; Zeka, A.; Schwartz, J. Association between PM2.5 and all-cause and specific-cause mortality in 27 US communities. J. Expo. Sci. Environ. Epidemiol. 2007, 17, 279–287. [Google Scholar] [CrossRef]
- Pope, C.A., III; Burnett, R.T.; Turner, M.C.; Cohen, A.; Krewski, D.; Jerrett, M.; Gapstur, S.M.; Thun, M.J. Lung cancer and cardiovascular disease mortality associated with ambient air pollution and cigarette smoke: shape of the exposure–response relationships. Environ. Health Perspect. 2011, 119, 1616–1621. [Google Scholar] [CrossRef]
- Thurston, G.D.; Burnett, R.T.; Turner, M.C.; Shi, Y.; Krewski, D.; Lall, R.; Ito, K.; Jerrett, M.; Gapstur, S.M.; Diver, W.R. Ischemic heart disease mortality and long-term exposure to source-related components of US fine particle air pollution. Environ. Health Perspect. 2016, 124, 785–794. [Google Scholar] [CrossRef]
- Anenberg, S.C.; Horowitz, L.W.; Tong, D.Q.; West, J.J. An estimate of the global burden of anthropogenic ozone and fine particulate matter on premature human mortality using atmospheric modeling. Environ. Health Perspect. 2010, 118, 1189–1195. [Google Scholar] [CrossRef]
- Ostro, B.D.; Lipsett, M.J.; Wiener, M.B.; Selner, J.C. Asthmatic responses to airborne acid aerosols. Am. J. Public Health 1991, 81, 694–702. [Google Scholar] [CrossRef]
- Shang, Y.; Sun, Z.; Cao, J.; Wang, X.; Zhong, L.; Bi, X.; Li, H.; Liu, W.; Zhu, T.; Huang, W. Systematic review of Chinese studies of short-term exposure to air pollution and daily mortality. Environ. Int. 2013, 54, 100–111. [Google Scholar] [CrossRef]
- Slaughter, J.C.; Lumley, T.; Sheppard, L.; Koenig, J.Q.; Shapiro, G.G. Effects of ambient air pollution on symptom severity and medication use in children with asthma. Ann. Allergy Asthma Immunol. 2003, 91, 346–353. [Google Scholar] [CrossRef]
- Yu, H.-L.; Chien, L.-C. Short-term population-based non-linear concentration–response associations between fine particulate matter and respiratory diseases in Taipei (Taiwan): A spatiotemporal analysis. J. Expo. Sci. Environ. Epidemiol. 2016, 26, 197–206. [Google Scholar] [CrossRef]
- Dan, M.; Zhuang, G.; Li, X.; Tao, H.; Zhuang, Y. The characteristics of carbonaceous species and their sources in PM2.5 in Beijing. Atmos. Environ. 2004, 38, 3443–3452. [Google Scholar] [CrossRef]
- Song, Y.; Zhang, Y.; Xie, S.; Zeng, L.; Zheng, M.; Salmon, L.G.; Shao, M.; Slanina, S. Source apportionment of PM2.5 in Beijing by positive matrix factorization. Atmos. Environ. 2006, 40, 1526–1537. [Google Scholar] [CrossRef]
- Ma, Q.; Cai, S.; Wang, S.; Zhao, B.; Martin, R.V.; Brauer, M.; Cohen, A.; Jiang, J.; Zhou, W.; Hao, J. Impacts of coal burning on ambient PM 2.5 pollution in China. Atmos. Chem. Phys. 2017, 17, 4477–4491. [Google Scholar] [CrossRef]
- Yang, C.; Peng, X.; Huang, W.; Chen, R.; Xu, Z.; Chen, B.; Kan, H. A time-stratified case-crossover study of fine particulate matter air pollution and mortality in Guangzhou, China. Int. Arch. Occup. Environ. Health 2012, 85, 579–585. [Google Scholar] [CrossRef]
- Ma, Y.; Chen, R.; Pan, G.; Xu, X.; Song, W.; Chen, B.; Kan, H. Fine particulate air pollution and daily mortality in Shenyang, China. Sci. Total Environ. 2011, 409, 2473–2477. [Google Scholar] [CrossRef]
- Kan, H.; London, S.J.; Chen, G.; Zhang, Y.; Song, G.; Zhao, N.; Jiang, L.; Chen, B. Differentiating the effects of fine and coarse particles on daily mortality in Shanghai, China. Environ. Int. 2007, 33, 376–384. [Google Scholar] [CrossRef]
- Daniels, M.J.; Dominici, F.; Samet, J.M.; Zeger, S.L. Estimating particulate matter-mortality dose-response curves and threshold levels: An analysis of daily time-series for the 20 largest US cities. Am. J. Epidemiol. 2000, 152, 397–406. [Google Scholar] [CrossRef]
- Samoli, E.; Analitis, A.; Touloumi, G.; Schwartz, J.; Anderson, H.R.; Sunyer, J.; Bisanti, L.; Zmirou, D.; Vonk, J.M.; Pekkanen, J. Estimating the exposure–response relationships between particulate matter and mortality within the APHEA multicity project. Environ. Health Perspect. 2005, 113, 88–95. [Google Scholar] [CrossRef]
- Schwartz, J.; Laden, F.; Zanobetti, A. The concentration-response relation between PM (2.5) and daily deaths. Environ. Health Perspect. 2002, 110, 1025–1029. [Google Scholar] [CrossRef]
- Krewski, D.; Jerrett, M.; Burnett, R.T.; Ma, R.; Hughes, E.; Shi, Y.; Turner, M.C.; Pope, C.A., III; Thurston, G.; Calle, E.E. Extended Follow-up and Spatial Analysis of the American Cancer Society Study Linking Particulate Air Pollution and Mortality; Health Effects Institute: Boston, MA, USA, 2009. [Google Scholar]
- Crouse, D.L.; Peters, P.A.; van Donkelaar, A.; Goldberg, M.S.; Villeneuve, P.J.; Brion, O.; Khan, S.; Atari, D.O.; Jerrett, M.; Pope, C.A., III. Risk of nonaccidental and cardiovascular mortality in relation to long-term exposure to low concentrations of fine particulate matter: A Canadian national-level cohort study. Environ. Health Perspect. 2012, 120, 708–714. [Google Scholar] [CrossRef]
- Burnett, R.T.; Pope, C.A., III; Ezzati, M.; Olives, C.; Lim, S.S.; Mehta, S.; Shin, H.H.; Singh, G.; Hubbell, B.; Brauer, M. An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ. Health Perspect. 2014, 122, 397–403. [Google Scholar] [CrossRef]
- Hansen, B.E. Threshold effects in non-dynamic panels: Estimation, testing, and inference. J. Econom. 1999, 93, 345–368. [Google Scholar] [CrossRef]
- Hansen, B.E. Sample splitting and threshold estimation. Econometrica 2000, 68, 575–603. [Google Scholar] [CrossRef]
- Cox, L.A.T. Effects of exposure estimation errors on estimated exposure-response relations for PM2.5. Environ. Res. 2018, 164, 636–646. [Google Scholar] [CrossRef]
- Dong, L. Capping Coal Consumption and Reduce Carbon Emission in China’s Industrial Sector. Available online: http://www.stanleyfoundation.org/climatechange/Dong-CappingCoalConsumptionReduceCarbonEmissions-China’sIndlSctr.pdf (accessed on 5 September 2018).
- GBD MAPS Working Group. Burden of Disease Attributable to Coal-Burning and Other Air Pollution Sources in China. Available online: https://www.healtheffects.org/system/files/GBDMAPS-ReportEnglishFinal1.pdf (accessed on 15 August 2018).
- Zhang, Y.-L.; Cao, F. Fine particulate matter (PM 2.5) in China at a city level. Sci. Rep. 2015, 5, 14884. [Google Scholar] [CrossRef]
- Westerdahl, D.; Wang, X.; Pan, X.; Zhang, K.M. Characterization of on-road vehicle emission factors and microenvironmental air quality in Beijing, China. Atmos. Environ. 2009, 43, 697–705. [Google Scholar] [CrossRef]
- Zheng, M.; Salmon, L.G.; Schauer, J.J.; Zeng, L.; Kiang, C.; Zhang, Y.; Cass, G.R. Seasonal trends in PM2.5 source contributions in Beijing, China. Atmos. Environ. 2005, 39, 3967–3976. [Google Scholar] [CrossRef]
- Venkatram, A.; Fitz, D.; Bumiller, K.; Du, S.; Boeck, M.; Ganguly, C. Using a dispersion model to estimate emission rates of particulate matter from paved roads. Atmos. Environ. 1999, 33, 1093–1102. [Google Scholar] [CrossRef]
- Kuhns, H.; Gillies, J.; Etyemezian, V.; Nikolich, G.; King, J.; Zhu, D.; Uppapalli, S.; Engelbrecht, J.; Kohl, S. Effect of soil type and momentum on unpaved road particulate matter emissions from wheeled and tracked vehicles. Aerosol Sci. Technol. 2010, 44, 187–196. [Google Scholar] [CrossRef]
- Dawson, J.; Adams, P.; Pandis, S. Sensitivity of PM 2.5 to climate in the Eastern US: A modeling case study. Atmos. Chem. Phys. 2007, 7, 4295–4309. [Google Scholar] [CrossRef]
- Tai, A.P.; Mickley, L.J.; Jacob, D.J. Correlations between fine particulate matter (PM2.5) and meteorological variables in the United States: Implications for the sensitivity of PM2.5 to climate change. Atmos. Environ. 2010, 44, 3976–3984. [Google Scholar] [CrossRef]
- Wang, J.; Ogawa, S. Effects of meteorological conditions on PM2.5 concentrations in Nagasaki, Japan. Int. J. Environ. Res. Public Health 2015, 12, 9089–9101. [Google Scholar] [CrossRef]
- Zhang, P.; Dong, G.; Sun, B.; Zhang, L.; Chen, X.; Ma, N.; Yu, F.; Guo, H.; Huang, H.; Lee, Y.L. Long-term exposure to ambient air pollution and mortality due to cardiovascular disease and cerebrovascular disease in Shenyang, China. PLoS ONE 2011, 6, e20827. [Google Scholar] [CrossRef]
- Dong, G.-H.; Zhang, P.; Sun, B.; Zhang, L.; Chen, X.; Ma, N.; Yu, F.; Guo, H.; Huang, H.; Lee, Y.L. Long-term exposure to ambient air pollution and respiratory disease mortality in Shenyang, China: A 12-year population-based retrospective cohort study. Respiration 2012, 84, 360–368. [Google Scholar] [CrossRef]
- Shima, M.; Adachi, M. Effect of outdoor and indoor nitrogen dioxide on respiratory symptoms in schoolchildren. Int. J. Epidemiol. 2000, 29, 862–870. [Google Scholar] [CrossRef]
- Filleul, L.; Rondeau, V.; Vandentorren, S.; Le Moual, N.; Cantagrel, A.; Annesi-Maesano, I.; Charpin, D.; Declercq, C.; Neukirch, F.; Paris, C. Twenty five year mortality and air pollution: Results from the French PAARC survey. Occup. Environ. Med. 2005, 62, 453–460. [Google Scholar] [CrossRef]
- Samoli, E.; Aga, E.; Touloumi, G.; Nisiotis, K.; Forsberg, B.; Lefranc, A.; Pekkanen, J.; Wojtyniak, B.; Schindler, C.; Niciu, E. Short-term effects of nitrogen dioxide on mortality: An analysis within the APHEA project. Eur. Respir. J. 2006, 27, 1129–1138. [Google Scholar] [CrossRef]
- Guo, Y.; Barnett, A.G.; Zhang, Y.; Tong, S.; Yu, W.; Pan, X. The short-term effect of air pollution on cardiovascular mortality in Tianjin, China: Comparison of time series and case–crossover analyses. Sci. Total Environ. 2010, 409, 300–306. [Google Scholar] [CrossRef]
- Kan, H.; London, S.J.; Chen, G.; Zhang, Y.; Song, G.; Zhao, N.; Jiang, L.; Chen, B. Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: The Public Health and Air Pollution in Asia (PAPA) Study. Environ. Health Perspect. 2008, 116, 1183–1188. [Google Scholar] [CrossRef]
- Kan, H.; Wong, C.-M.; Vichit-Vadakan, N.; Qian, Z. Short-term association between sulfur dioxide and daily mortality: The Public Health and Air Pollution in Asia (PAPA) study. Environ. Res. 2010, 110, 258–264. [Google Scholar] [CrossRef]
- Apte, J.S.; Marshall, J.D.; Cohen, A.J.; Brauer, M. Addressing global mortality from ambient PM2.5. Environ. Sci. Technol. 2015, 49, 8057–8066. [Google Scholar] [CrossRef]
- Ren, M.; Li, N.; Wang, Z.; Liu, Y.; Chen, X.; Chu, Y.; Li, X.; Zhu, Z.; Tian, L.; Xiang, H. The short-term effects of air pollutants on respiratory disease mortality in Wuhan, China: Comparison of time-series and case-crossover analyses. Sci. Rep. 2017, 7, 40482. [Google Scholar] [CrossRef]
- Mo, Z.; Fu, Q.; Zhang, L.; Lyu, D.; Mao, G.; Wu, L.; Xu, P.; Wang, Z.; Pan, X.; Chen, Z.; et al. Acute effects of air pollution on respiratory disease mortalities and outpatients in Southeastern China. Sci. Rep. 2018, 8, 3461. [Google Scholar] [CrossRef]
- Hsu, A. Seeing China’s Pollution from Space. Available online: https://www.chinadialogue.net/article/show/single/en/4775-Seeing-China-s-pollution-from-space (accessed on 5 January 2018).
- Yao, L.; Lu, N. Particulate matter pollution and population exposure assessment over mainland China in 2010 with remote sensing. Int. J. Environ. Res. Public Health 2014, 11, 5241–5250. [Google Scholar] [CrossRef]
- National Bureau of Statistics of China. Available online: http://www.stats.gov.cn/english/Statisticaldata/AnnualData/ (accessed on 26 January 2018).
- Zhou, M.; Wang, H.; Zhu, J.; Chen, W.; Wang, L.; Liu, S.; Li, Y.; Wang, L.; Liu, Y.; Yin, P. Cause-specific mortality for 240 causes in China during 1990–2013: A systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet 2016, 387, 251–272. [Google Scholar] [CrossRef]
- Pope, C.A.; Burnett, R.T.; Krewski, D.; Jerrett, M.; Shi, Y.; Calle, E.E.; Thun, M.J. Cardiovascular mortality and exposure to airborne fine particulate matter and cigarette smoke: Shape of the exposure-response relationship. Circulation 2009, 120, 941–948. [Google Scholar] [CrossRef]
- Chen, B.; Kan, H.; Chen, R.; Jiang, S.; Hong, C. Air pollution and health studies in China—Policy implications. J. Air Waste Manag. Assoc. 2011, 61, 1292–1299. [Google Scholar] [CrossRef]
- Pope, C.A., III; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 2002, 287, 1132–1141. [Google Scholar] [CrossRef]
- Beelen, R.; Hoek, G.; van Den Brandt, P.A.; Goldbohm, R.A.; Fischer, P.; Schouten, L.J.; Jerrett, M.; Hughes, E.; Armstrong, B.; Brunekreef, B. Long-term effects of traffic-related air pollution on mortality in a Dutch cohort (NLCS-AIR study). Environ. Health Perspect. 2008, 116, 196–202. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Description | Mean | Median | Max | Min | Std. Dev. |
|---|---|---|---|---|---|---|
| concentration ) | 27.26 | 26.96 | 51.91 | 2.17 | 11.71 | |
| Coal_cons | coal consumption (10,000 tons) | 10,520.76 | 8559.73 | 37,327.89 | 332.23 | 7897.92 |
| GasDie_cons | gasoline-diesel consumption (10,000 tons) | 682.03 | 568.77 | 2754.68 | 40.74 | 496.26 |
| Paved_Rd | per capita area of paved road (sq.m) | 11.41 | 11.19 | 22.23 | 4.04 | 3.31 |
| Temp | average temperature () | 14.47 | 15.1 | 25.4 | 4.5 | 5.07 |
| Humid | relative humidity (%) | 64.24 | 66 | 83 | 44 | 9.41 |
| Precp | precipitation (mm) | 867.63 | 765.6 | 2628.2 | 74.9 | 503.46 |
| Observations | 203 |
| Variables | Description | Mean | Median | Max | Min | Std. Dev. |
|---|---|---|---|---|---|---|
| cardiovascular mortality rate (deaths per 100,000 persons) | 238.84 | 239.02 | 355.85 | 152.94 | 49.04 | |
| respiratory mortality rate (deaths per 100,000 persons) | 114.39 | 104.42 | 226.05 | 55.73 | 43.25 | |
| concentration () | 26.69 | 26.72 | 51.94 | 2.17 | 11.92 | |
| concentration () | 40.86 | 41.30 | 73.00 | 11.90 | 13.69 | |
| emission () | 76.30 | 63.35 | 200.30 | 0.10 | 48.16 | |
| GRP | gross regional product (100 million yuan) | 8279.15 | 6438.74 | 35,696.71 | 229.04 | 7139.56 |
| Observations | 210 |
| Variables | Pooled OLS | FE Model | RE Model |
|---|---|---|---|
| Coefficients | |||
| Constant | −1.345 (1.228) | −1.771 ** (0.829) | −1.923 ** (0.755) |
| LnCoal_cons | 0.404 *** (0.0544) | 0.196 *** (0.056) | 0.233 *** (0.051) |
| B08 | 0.126 * (0.0704) | 0.142 *** (0.0164) | 0.145 *** (0.016) |
| LnGasDie_cons | 0.0168 (0.069) | 0.076 ** (0.038) | 0.0650 * (0.037) |
| LnPaved_Rd | −0.158 (0.106) | −0.046 (0.038) | −0.056 (0.037) |
| LnTemp | 0.689 *** (0.106) | 0.233 ** (0.110) | 0.241 ** (0.095) |
| LnHumid | 0.244 (0.365) | 0.604 *** (0.159) | 0.581 *** (0.149) |
| LnPrec | −0.260 ** (0.101) | −0.059 ** (0.027) | −0.061 ** (0.027) |
| Adj R2 | 0.481 | 0.984 | 0.376 |
| F test (Pooled vs. Fixed) | 216.96 *** | ||
| LM test (Pooled vs. Random) | 540.24 *** | ||
| Hausman Test (Random vs. Fixed) | 6.04 | ||
| Threshold | ||
|---|---|---|
| Test for single threshold | ||
| 210.329 | 51.314 | |
| p-value | 0.000 | 0.010 |
| Critical values (10, 5, 1) | 29.720, 37.778, 49.981 | 27.013, 36.152, 45.191 |
| Test for double threshold | ||
| 24.799 | 17.189 | |
| p-value | 0.080 | 0.250 |
| Critical values (10, 5, 1) | 23.274, 28.334, 34.176 | 23.340, 28.697, 36.832 |
| Test for triple threshold | ||
| 142.326 | 21.743 | |
| p-value | 0.000 | 0.013 |
| Critical values (10, 5, 1) | 20.952, 27.461, 41.740 | 13.272, 16.893, 22.610 |
| Threshold Estimates | Threshold | Estimates | 95% Confidence | |
|---|---|---|---|---|
| 2.872 | [2.717, 2.872] | 17.67 | ||
| 3.073 | [3.074, 3.074] | 21.62 | ||
| 3.534 | [2.872, 3.610] | 34.27 | ||
| Variable | Coefficient | Regime-dependent | ||
| OLS S.E. | White S.E. | |||
| 17.67 | 0.031 | 0.043 | 0.060 | |
| −0.003 | 0.020 | 0.013 | ||
| 0.196 ** | 0.073 | 0.090 | ||
| 21.62 > 17.67 | 0.806 *** | 0.245 | 0.198 | |
| −0.270 *** | 0.078 | 0.064 | ||
| −0.159 | 0.142 | 0.118 | ||
| 34.27 > 21.62 | 0.257 *** | 0.059 | 0.054 | |
| 0.054 * | 0.025 | 0.028 | ||
| −0.162 *** | 0.045 | 0.042 | ||
| > 34.27 | −0.003 | 0.070 | 0.062 | |
| 0.172 *** | 0.028 | 0.020 | ||
| −0.034 | 0.043 | 0.038 | ||
| Variable | Coefficient | Regime-independent | ||
| OLS S.E. | White S.E. | |||
| 0.0378 ** | 0.016 | 0.017 | ||
| Threshold Estimates | Threshold | Estimates | 95% Confidence | |
|---|---|---|---|---|
| r | 4.3836 | [4.3549, 4.3993] | 80.13 | |
| Variable | Coefficient | Regime-independent | ||
| OLS S.E. | White S.E. | t-statistic | ||
| ( 80.13) | 0.172 *** | 0.028 | 0.043 | 4.050 |
| 80.13) | 0.250 *** | 0.029 | 0.047 | 5.352 |
| Ln | −0.032 | 0.019 | 0.035 | −0.904 |
| Ln | 0.176 *** | 0.041 | 0.043 | 4.052 |
| LnGRP | −0.188 *** | 0.019 | 0.025 | −7.585 |
| Result of Stage 1 (Panel Data Model) | Result of Stage 2 (Panel Threshold Model) | Result of Two-Stage Approach | ||
|---|---|---|---|---|
| Estimate effect of coal consumption on | Estimate effect of on cause-specific mortality | Estimate health effect of coal consumption | ||
| 0.233 *** | Estimated threshold regimes | Coefficient | Coefficient | |
| Cardiovascular mortality | 21.62 > 17.67 | 0.806 *** | 0.188 | |
| 34.27 > 21.62 | 0.257 *** | 0.060 | ||
| Respiratory mortality | 80.13 (tons) | 0.172 *** | 0.040 | |
| 80.13 (tons) | 0.250 *** | 0.058 | ||
| Study Approach | Regions [Author] | Pollutant | Methodology (Time Period) | Health Outcomes | Estimated Coef. |
|---|---|---|---|---|---|
| Short-term Studies | Shanghai, China [19] | Time-series | Cardiovascular mortality | 0.41 [0.00, 0.82] | |
| Respiratory mortality | 0.95 [0.17, 1.73] | ||||
| Shenyang, China [18] | Time-stratified case-crossover | Cardiovascular mortality | 0.53 [0.09, 0.97] | ||
| Respiratory mortality | 0.97 [0.01, 1.94] | ||||
| Quangzhou, China [17] | Time-stratified case-crossover | Cardiovascular mortality | 1.22 [0.63, 1.68] | ||
| Respiratory mortality | 0.97 [0.16, 1.79] | ||||
| This study | China | Panel Threshold Model | Cardiovascular mortality | 30.18 (21.62 > 17.67) | |
| 9.63 (34.27 > 21.62) | |||||
| Respiratory mortality | 6.45 ( 80.13) | ||||
| 9.35 ( > 80.13) | |||||
| Long-term Studies | Shenyang, China [39] | Retrospective cohort study (1998–2009) | Cardiovascular mortality | 55 [51, 60] | |
| Shenyang, China [40] | Retrospective cohort (1998–2009) | Respiratory mortality | 67 [60, 74] | ||
| US metropolitan areas [56] | Cohort study (1979–1983) | Cardiopulmonary mortality | 6 [2, 10] | ||
| Netherlands [57] | Cohort study (1987–1996) | Respiratory mortality | 7 [−25, 52] | ||
| US metropolitan areas [56] | Cohort study (1979–1983) | Cardiopulmonary mortality | 6 [2, 10] | ||
| Canada [24] | Cohort study (1991–2001) | Cardiovascular mortality | 31 [27, 35] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, B.-L.; Chang, C.-C.; Hsu, C.-S.; Chen, C.-C.; Tseng, W.-C.; Hsu, S.-H. Threshold Effects of PM2.5 Exposure on Particle-Related Mortality in China. Int. J. Environ. Res. Public Health 2019, 16, 3549. https://doi.org/10.3390/ijerph16193549
Tran B-L, Chang C-C, Hsu C-S, Chen C-C, Tseng W-C, Hsu S-H. Threshold Effects of PM2.5 Exposure on Particle-Related Mortality in China. International Journal of Environmental Research and Public Health. 2019; 16(19):3549. https://doi.org/10.3390/ijerph16193549
Chicago/Turabian StyleTran, Bao-Linh, Ching-Cheng Chang, Chia-Sheng Hsu, Chi-Chung Chen, Wei-Chun Tseng, and Shih-Hsun Hsu. 2019. "Threshold Effects of PM2.5 Exposure on Particle-Related Mortality in China" International Journal of Environmental Research and Public Health 16, no. 19: 3549. https://doi.org/10.3390/ijerph16193549
APA StyleTran, B.-L., Chang, C.-C., Hsu, C.-S., Chen, C.-C., Tseng, W.-C., & Hsu, S.-H. (2019). Threshold Effects of PM2.5 Exposure on Particle-Related Mortality in China. International Journal of Environmental Research and Public Health, 16(19), 3549. https://doi.org/10.3390/ijerph16193549