Associations Between Sub-Clinical Markers of Cardiometabolic Risk and Exposure to Residential Indoor Air Pollutants in Healthy Adults in Perth, Western Australia: A Study Protocol

 , ,
, , 
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
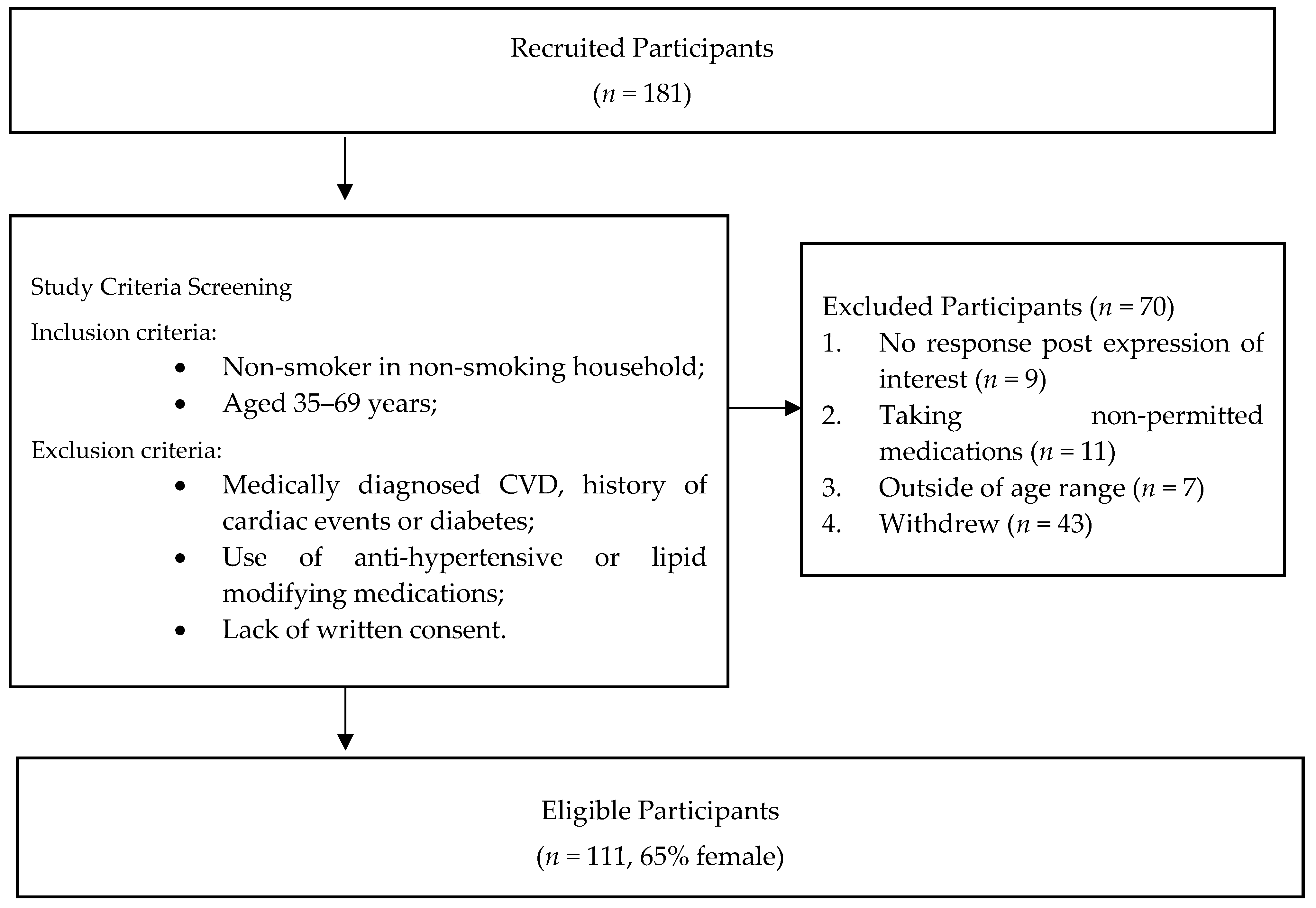
2.2. Study Location and Population
- Non-smokers living in a non-smoking household.
- Aged between 35 and 69 years.
- A history of cardiovascular events or medical diagnosis of cardiovascular disease (CVD).
- Medically diagnosed diabetes.
- Use of anti-hypertensive or lipid modifying medications.
- Lack of written consent.
2.3. Data Collection
- Stage 1: In-home equipment installation—the measurement of domestic indoor air quality in participants home and ambulatory blood pressure (ABP)/hemodynamic indices over a concurrent 24 h period. Participants were also requested to complete questionnaires related to health and domestic environment and to complete a 24 h time/activity diary during the 24 h IAQ/BP monitoring period.
- Stage 2: Clinic-based health assessment—data relating to baseline health characteristics, cardiometabolic biomarkers and measures, and pulse wave analysis were collected.
2.4. In-Home Assessment
2.4.1. Measurement of Air Quality and Instrumentation
2.4.2. Measurement of Ambulatory BP and Hemodynamic Indices
2.4.3. Questionnaires and Time-Activity Diary
2.5. Clinic Assessment
Pulse Wave Analysis and Pulse Wave Velocity
2.6. Data Management
2.7. Statistical Analysis
2.7.1. Sample Size and Effect
2.7.2. Data Analysis
2.8. Ethics and Consents
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cosselman, K.E.; Navas-Acien, A.; Kaufman, J.D. Environmental factors in cardiovascular disease. Nat. Revs. Cardiol. 2015, 12, 627–642. [Google Scholar] [CrossRef] [PubMed]
- Munzel, T.; Sorensen, M.; Gori, T.; Schmidt, F.P.; Rao, X.; Brook, F.R.; Chen, L.C.; Brook, R.D.; Rajagopalan, S. Environmental stressors and cardio-metabolic disease: Part ii-mechanistic insights. Eur. Heart J. 2017, 38, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Munzel, T.; Sorensen, M.; Gori, T.; Schmidt, F.P.; Rao, X.; Brook, J.; Chen, L.C.; Brook, R.D.; Rajagopalan, S. Environmental stressors and cardio-metabolic disease: Part i-epidemiologic evidence supporting a role for noise and air pollution and effects of mitigation strategies. Eur. Heart J. 2017, 38, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Bard, R.L.; Burnett, R.T.; Shin, H.H.; Vette, A.; Croghan, C.; Phillips, M.; Rodes, C.; Thornburg, J.; Williams, R. Differences in blood pressure and vascular responses associated with ambient fine particulate matter exposures measured at the personal versus community level. Occup. Environ. Med. 2011, 68, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Dvonch, T.J.; Kannan, J.S.; Schulz, J.A.; Keeler, L.G.; Mentz, D.G.; House, D.J.; Benjamin, D.A.; Max, D.P.; Bard, D.R.; Brook, D.R. Acute effects of ambient particulate matter on blood pressure: Differential effects across urban communities. Hypertension 2009, 53, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Lenters, V.; Uiterwaal, C.S.; Beelen, R.; Bots, M.L.; Fischer, P.; Brunekreef, B.; Hoek, G. Long-term exposure to air pollution and vascular damage in young adults. Epidemiology 2010, 21, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.J.; Zanobetti, A.; Koutrakis, P.; Mittleman, M.A.; Sparrow, D.; Vokonas, P.; Schwartz, J. Associations between short-term changes in air pollution and correlates of arterial stiffness: The veterans affairs normative aging study, 2007–2011. Am. J. Epidemiol. 2014, 179, 192–199. [Google Scholar] [CrossRef]
- Shanley, P.R.; Hayes, B.R.; Cromar, R.K.; Ito, R.K.; Gordon, R.T.; Ahn, R.J. Particulate air pollution and clinical cardiovascular disease risk factors. Epidemiology 2016, 27, 291–298. [Google Scholar] [CrossRef]
- Yang, B.-Y.; Bloom, M.S.; Markevych, I.; Qian, Z.; Vaughn, M.G.; Cummings-Vaughn, L.A.; Li, S.; Chen, G.; Bowatte, G.; Perret, J.L.; et al. Exposure to ambient air pollution and blood lipids in adults: The 33 communities chinese health study. Environ. Int. 2018, 119, 485–492. [Google Scholar] [CrossRef]
- Yang, B.-Y.; Qian, Z.; Howard, S.W.; Vaughn, M.G.; Fan, S.-J.; Liu, K.-K.; Dong, G.-H. Global association between ambient air pollution and blood pressure: A systematic review and meta-analysis. Environ. Pollut. 2018, 235, 576–588. [Google Scholar] [CrossRef]
- Brook, R.D.; Newby, D.E.; Rajagopalan, S. Air pollution and cardiometabolic disease: An update and call for clinical trials. Am. J. Hypertens. 2017, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bourdrel, T.; Bind, M.A.; Bejot, Y.; Morel, O.; Argacha, J.F. Cardiovascular effects of air pollution. Arch. Cardiovasc. Dis. 2017, 110, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Kelly, F.J.; Fussell, J.C. Air pollution and public health: Emerging hazards and improved understanding of risk. Environ. Geochem. Health 2015, 37, 631–649. [Google Scholar] [CrossRef] [PubMed]
- Uzoigwe, J.C.; Prum, T.; Bresnahan, E.; Garelnabi, M. The emerging role of outdoor and indoor air pollution in cardiovascular disease. N. Am. J. Med. Sci. 2013, 5, 445–453. [Google Scholar] [PubMed]
- Brook, R.D.; Weder, A.B.; Rajagopalan, S. “Environmental hypertensionology” the effects of environmental factors on blood pressure in clinical practice and research. J. Clin. Hypertens. 2011, 13, 836–842. [Google Scholar] [CrossRef] [PubMed]
- Giorgini, P.; Di Giosia, P.; Grassi, D.; Rubenfire, M.; Brook, R.D.; Ferri, C. Air pollution exposure and blood pressure: An updated review of the literature. Curr. Pharm. Des. 2016, 22, 28–51. [Google Scholar] [CrossRef] [PubMed]
- Auchincloss, A.; Roux, A.; Dvonch, J.; Brown, P.; Barr, R.; Daviglus, M.; Goff, D.; Kaufman, J.; O’Neill, M. Associations between recent exposure to ambient fine particulate matter and blood pressure in the multi-ethnic study of atherosclerosis (mesa). Environ. Health Perspect. 2008, 116, 486–491. [Google Scholar] [CrossRef]
- Ibald-Mulli, A.; Stieber, J.; Wichmann, H.E.; Koenig, W.; Peters, A. Effects of air pollution on blood pressure: A population-based approach. Am. J. Public Health 2001, 91, 571–577. [Google Scholar]
- Honda, T.; Pun, V.C.; Manjourides, J.; Suh, H. Associations of long-term fine particulate matter exposure with prevalent hypertension and increased blood pressure in older americans. Environ. Res. 2018, 164, 1–8. [Google Scholar] [CrossRef]
- Harrabi, I.; Rondeau, V.; Dartigues, J.-F.; Tessier, J.-F.; Filleul, L. Effects of particulate air pollution on systolic blood pressure: A population-based approach. Environ. Res. 2006, 101, 89–93. [Google Scholar] [CrossRef]
- Madsen, C.; Nafstad, P. Associations between environmental exposure and blood pressure among participants in the oslo health study (hubro). Eur. J. Epidemiol. 2006, 21, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, J.; Carter, E.; Schauer, J.J.; Ezzati, M.; Daskalopoulou, S.S.; Valois, M.F.; Shan, M.; Yang, X. Household air pollution and measures of blood pressure, arterial stiffness and central haemodynamics. Heart 2018, 104, 1515–1521. [Google Scholar] [CrossRef] [PubMed]
- Chuang, K.-J.; Yan, Y.-H.; Cheng, T.-J. Effect of air pollution on blood pressure, blood lipids, and blood sugar: A population-based approach. J. Occup. Environ. Med. 2010, 52, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Chuang, K.-J.; Yan, Y.-H.; Chiu, S.-Y.; Cheng, T.-J. Long-term air pollution exposure and risk factors for cardiovascular diseases among the elderly in taiwan. Occup. Environ. Med. 2011, 68, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, S.; Young, B.N.; Clark, M.L.; Benka-Coker, M.L.; Bachand, A.M.; Brook, R.D.; Nelson, T.L.; Volckens, J.; Reynolds, S.J.; L’orange, C.; et al. Household air pollution from biomass-burning cookstoves and metabolic syndrome, blood lipid concentrations, and waist circumference in honduran women: A cross-sectional study. Environ. Res. 2019, 170, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Yitshak Sade, F.M.; Kloog, F.I.; Liberty, F.I.; Schwartz, F.J.; Novack, F.V. The association between air pollution exposure and glucose and lipids levels. J. Clin. Endocrinol. Metab. 2016, 101, 2460–2467. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.; Liu, R.; Wei, Y.; Feng, L.; Lv, X.; Tang, F. Air pollution and blood lipid markers levels: Estimating short and long-term effects on elderly hypertension inpatients complicated with or without type 2 diabetes. Environ. Pollut. 2016, 215, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Yang, C.; Zhao, Y.; Ma, Z.; Bi, J.; Liu, Y.; Meng, X.; Wang, Y.; Cai, J.; Kan, H.; et al. Associations between long-term exposure to ambient particulate air pollution and type 2 diabetes prevalence, blood glucose and glycosylated hemoglobin levels in china. Environ. Int. 2016, 92–93, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, S.; Clark, M.L.; Young, B.N.; Benka-Coker, M.L.; Bachand, A.M.; Brook, R.D.; Nelson, T.L.; Volckens, J.; Reynolds, S.J.; L’Orange, C.; et al. Exposure to household air pollution from biomass-burning cookstoves and hba1c and diabetic status among honduran women. Indoor Air 2018, 28, 768–776. [Google Scholar] [CrossRef]
- World Health Organisation. Who: Guidelines for Indoor Air Quality: Selected Pollutants; World Health Organisation Regional Office for Europe: Copenhagen, Denmark, 2010. [Google Scholar]
- Morawska, L.; Afshari, A.; Bae, G.N.; Buonanno, G.; Chao, C.Y.H.; Hänninen, O.; Hofmann, W.; Isaxon, C.; Jayaratne, E.R.; Pasanen, P.; et al. Indoor aerosols: From personal exposure to risk assessment. Indoor Air 2013, 23, 462–487. [Google Scholar] [CrossRef]
- Bhangar, S.; Mullen, N.; Hering, S.; Kreisberg, N.; Nazaroff, W. Ultrafine particle concentrations and exposures in seven residences in northern california. Indoor Air 2011, 21, 132–144. [Google Scholar] [CrossRef] [PubMed]
- Morawska, L.; Ayoko, G.A.; Bae, G.N.; Buonanno, G.; Chao, C.Y.H.; Clifford, S.; Fu, S.C.; Hanninen, O.; He, C.; Isaxon, C.; et al. Airborne particles in indoor environment of homes, schools, offices and aged care facilities: The main routes of exposure. Environ. Int. 2017, 108, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Wallace, L. Indoor sources of ultrafine and accumulation mode particles: Size distributions, size-resolved concentrations, and source strengths. Aerosol Sci. Technol. 2006, 40, 348–360. [Google Scholar] [CrossRef]
- Clark, S.N.; Schmidt, A.M.; Carter, E.M.; Schauer, J.J.; Yang, X.; Ezzati, M.; Daskalopoulou, S.S.; Baumgartner, J. Longitudinal evaluation of a household energy package on blood pressure, central hemodynamics, and arterial stiffness in China. Environ. Res. 2019, 177, 108592. [Google Scholar] [CrossRef] [PubMed]
- Young, B.N.; Clark, M.L.; Rajkumar, S.; Benka-Coker, M.L.; Bachand, A.; Brook, R.D.; Nelson, T.L.; Volckens, J.; Reynolds, S.J.; L’Orange, C.; et al. Exposure to household air pollution from biomass cookstoves and blood pressure among women in rural honduras: A cross-sectional study. Indoor Air 2019, 29, 130–142. [Google Scholar] [CrossRef] [PubMed]
- Brasche, S.; Bischof, W. Daily time spent indoors in german homes–baseline data for the assessment of indoor exposure of german occupants. Int. J. Hyg. Environ. Health. 2005, 208, 247–253. [Google Scholar] [CrossRef]
- Lai, H.K.; Kendall, M.; Ferrier, H.; Lindup, I.; Alm, S.; Hänninen, O.; Jantunen, M.; Mathys, P.; Colvile, R.; Ashmore, M.R.; et al. Personal exposures and microenvironment concentrations of PM2.5, VOC, NO2 and CO in Oxford, UK. Atmos. Environ. 2004, 38, 6399–6410. [Google Scholar] [CrossRef]
- Leech, J.A.; Nelson, W.C.; Burnett, R.T.; Aaron, S.; Raizenne, M.E. It’s about time: A comparison of canadian and american time-activity patterns. J. Expo. Anal. Environ. Epidemiol. 2002, 12, 427–432. [Google Scholar] [CrossRef]
- Rumchev, K.; Soares, M.; Zhao, Y.; Reid, C.; Huxley, R. The association between indoor air quality and adult blood pressure levels in a high-income setting. Int. J. Environ. Res. Public Health 2018, 15, 2026. [Google Scholar] [CrossRef]
- Balmes, J.R. Household air pollution from domestic combustion of solid fuels and health. J. Allergy Clin. Immunol. 2019, 143, 1979–1987. [Google Scholar] [CrossRef]
- Reisen, F.; Meyer, C.P.; Keywood, M.D. Impact of biomass burning sources on seasonal aerosol air quality. Atmos. Environ. 2013, 67, 437–447. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Greater Perth; Western Australia. Available online: https://itt.abs.gov.au/itt/r.jsp?RegionSummary®ion=5GPER&dataset=ABS_REGIONAL_ASGS&geoconcept=REGION&measure=MEASURE&datasetASGS=ABS_REGIONAL_ASGS&datasetLGA=ABS_REGIONAL_LGA®ionLGA=REGION®ionASGS=REGION (accessed on 16 September 2019).
- Government of Western Australia; Environmental Protection Authority. Factor Guidelines and Technical Guidance: Air. Available online: http://epa.wa.gov.au/node/193 (accessed on 16 September 2019).
- Wheeler, A.J.; Xu, X.; Kulka, R.; You, H.; Wallace, L.; Mallach, G.; Ryswyk, K.V.; MacNeill, M.; Kearney, J.; Rasmussen, P.E.; et al. Windsor, ontario exposure assessment study: Design and methods validation of personal, indoor, and outdoor air pollution monitoring. J. Air Waste Manag. Assoc. 2011, 61, 324–338. [Google Scholar] [CrossRef] [PubMed]
- Yoda, Y.; Tamura, K.; Shima, M. Airborne endotoxin concentrations in indoor and outdoor particulate matter and their predictors in an urban city. Indoor Air 2017, 27, 955–964. [Google Scholar] [CrossRef] [PubMed]
- TSI. Dust Trak Aerosol Monitor-Model 8533, Operation and Service Manual. Available online: http://www.tsi.com/uploadedFiles/_Site_Root/Products/Literature/Manuals/8533-8534-DustTrak_DRX-6001898-web.pdf (accessed on 22 April 2019).
- Akbar-khanzadeh, F.; Ames, A.; Bisesi, M.; Milz, S.; Czajkowski, K.; Kumar, A. Particulate matter (pm) exposure assessment—Horizontal and vertical pm profiles in relation to agricultural activities and environmental factors in farm fields. J. Occup. Environ. Hyg. 2012, 9, 502–516. [Google Scholar] [CrossRef] [PubMed]
- TSI. P-Trak Ultrafine Particle Counter 8525-Operation and Service Manual. Available online: http://www.tsi.com/uploadedFiles/_Site_Root/Products/Literature/Manuals/Model-8525-P-Trak-1980380.pdf (accessed on 12 February 2019).
- Sun, Z.C.; Mukherjee, B.; Brook, R.D.; Gatts, G.; Yang, F.; Sun, Q.; Brook, J.R.; Fan, Z.; Rajagopalan, S. Air-pollution and cardiometabolic diseases (aircmd): A prospective study investigating the impact of air pollution exposure and propensity for type ii diabetes. Sci. Total Environ. 2013, 448, 72–78. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, E.; Parati, G.; Stergiou, G.; Asmar, R.; Beilin, L.; Bilo, G.; Clement, D.; de la Sierra, A.; de Leeuw, P.; Dolan, E.; et al. European society of hypertension position paper on ambulatory blood pressure monitoring. J. Hypertens. 2013, 31, 1731–1768. [Google Scholar] [CrossRef] [PubMed]
- Parati, G.; Stergiou, G.; O’Brien, E.; Asmar, R.; Beilin, L.; Bilo, G.; Clement, D.; de la Sierra, A.; de Leeuw, P.; Dolan, E.; et al. European society of hypertension practice guidelines for ambulatory blood pressure monitoring. J. Hypertens. 2014, 32, 1359–1366. [Google Scholar] [CrossRef] [PubMed]
- Andreadis, E.A.; Agaliotis, G.; Kollias, A.; Kolyvas, G.; Achimastos, A.; Stergiou, G.S. Night-time home versus ambulatory blood pressure in determining target organ damage. J. Hypertens. 2016, 34, 438–444, Discussion 444. [Google Scholar] [CrossRef] [PubMed]
- Rumchev, K.; Spickett, J.; Bulsara, M.; Phillips, M.; Stick, S. Association of domestic exposure to volatile organic compounds with asthma in young children. Thorax 2004, 59, 746–751. [Google Scholar] [CrossRef]
- Rumchev, K.B.; Spickett, J.T.; Bulsara, M.K.; Phillips, M.R.; Stick, S.M. Domestic exposure to formaldehyde significantly increases the risk of asthma in young children. Eur. Respir. J. 2002, 20, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Spickett, J.; Rumchev, K.; Lee, A.H.; Stick, S. Snoring in primary school children and domestic environment: A perth school based study. Respir. Res. 2004, 5, 19. [Google Scholar] [CrossRef] [PubMed]
- Australian Government. Diabetes. Available online: http://www.health.gov.au/internet/main/publishing.nsf/Content/chronic-diabetes#ris (accessed on 16 September 2019).
- Fuller, C.H.; Patton, A.P.; Lane, K.; Laws, M.B.; Marden, A.; Carrasco, E.; Spengler, J.; Mwamburi, M.; Zamore, W.; Durant, J.L.; et al. A community participatory study of cardiovascular health and exposure to near-highway air pollution: Study design and methods. Rev. Environ. Health 2013, 28, 21–35. [Google Scholar] [CrossRef] [PubMed]
- Anderson, G.L.; Manson, J.; Wallace, R.; Lund, B.; Hall, D.; Davis, S.; Shumaker, S.; Wang, C.-Y.; Stein, E.; Prentice, R.L. Implementation of the women’s health initiative study design. Ann. Epidemiol. 2003, 13, S5–S17. [Google Scholar] [CrossRef]
- Ji, H.; Xiong, J.; Yu, S.; Chi, C.; Fan, X.; Bai, B.; Zhou, Y.; Teliewubai, J.; Lu, Y.; Xu, H.; et al. Northern shanghai study: Cardiovascular risk and its associated factors in the chinese elderly—A study protocol of a prospective study design. BMJ Open 2017, 7, 1–7. [Google Scholar] [CrossRef] [PubMed]
- de Vos, L.C.; Boersema, J.; Hillebrands, J.L.; Schalkwijk, C.G.; Meerwaldt, R.; Breek, J.C.; Smit, A.J.; Zeebregts, C.J.; Lefrandt, J.D. Diverging effects of diabetes mellitus in patients with peripheral artery disease and abdominal aortic aneurysm and the role of advanced glycation end-products: Artery study—protocol for a multicentre cross-sectional study. BMJ Open 2017, 7, e012584. [Google Scholar] [CrossRef] [PubMed]
- Green, S.B. How many subjects does it take to do a regression analysis. Multivar. Behav. Res. 1991, 26, 499–510. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.; Bergen, S.; Szpiro, A.; Deroo, L.; London, S.; Marshall, J.; Kaufman, J.; Sandler, D. Long-term air pollution exposure and blood pressure in the sister study. Environ. Health Perspect. (Online) 2015, 123, 951. [Google Scholar] [CrossRef] [PubMed]
- Adar, S.D.; Chen, Y.H.; D’Souza, J.C.; O’Neill, M.S.; Szpiro, A.A.; Auchincloss, A.H.; Park, S.K.; Daviglus, M.L.; Diez Roux, A.V.; Kaufman, J.D. Longitudinal analysis of long-term air pollution levels and blood pressure: A cautionary tale from the multi-ethnic study of atherosclerosis. Environ. Health Perspect. 2018, 126, 107003. [Google Scholar] [CrossRef]
- Sanchez-Inigo, L.; Navarro-Gonzalez, D.; Pastrana-Delgado, J.; Fernandez-Montero, A.; Martinez, J.A. Association of triglycerides and new lipid markers with the incidence of hypertension in a spanish cohort. J. Hypertens. 2016, 34, 1257–1265. [Google Scholar] [CrossRef]
- Morawska, L. Indoor air quality and health. Air Qual. Clim. Chang. 2010, 44, 12–14. [Google Scholar]
- Morawska, L.; He, C.; Hitchins, J.; Mengersen, K.; Gilbert, D. Characteristics of particle number and mass concentrations in residential houses in brisbane, australia. Atmos. Environ. 2003, 37, 4195–4203. [Google Scholar] [CrossRef]
- Wilson, J.G.; Kingham, S.; Pearce, J.; Sturman, A.P. A review of intraurban variations in particulate air pollution: Implications for epidemiological research. Atmos. Environ. 2005, 39, 6444–6462. [Google Scholar] [CrossRef]
- Chang, L.-T.; Chuang, K.-J.; Yang, W.-T.; Wang, V.-S.; Chuang, H.-C.; Bao, B.-Y.; Liu, C.-S.; Chang, T.-Y. Short-term exposure to noise, fine particulate matter and nitrogen oxides on ambulatory blood pressure: A repeated-measure study. Environ. Res. 2015, 140, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Dabass, A.; Talbott, E.O.; Venkat, A.; Rager, J.; Marsh, G.M.; Sharma, R.K.; Holguin, F. Association of exposure to particulate matter (pm2.5) air pollution and biomarkers of cardiovascular disease risk in adult nhanes participants (2001–2008). Int. J. Hyg. Environ. Health. 2016, 219, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Foraster, M.; Kunzli, N.; Aguilera, I.; Rivera, M.; Agis, D.; Vila, J.; Bouso, L.; Deltell, A.; Marrugat, J.; Ramos, R.; et al. High blood pressure and long-term exposure to indoor noise and air pollution from road traffic. Environ. Health Perspect. 2014, 122, 1193–1200. [Google Scholar] [CrossRef] [PubMed]
- Zanobetti, A.; Schwartz, J. The effect of particulate air pollution on emergency admissions for myocardial infarction: A multicity case-crossover analysis. Environ. Health Perspect. 2005, 113, 978–982. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., 3rd; Turner, M.C.; Burnett, R.T.; Jerrett, M.; Gapstur, S.M.; Diver, W.R.; Krewski, D.; Brook, R.D. Relationships between fine particulate air pollution, cardiometabolic disorders, and cardiovascular mortality. Circ. Res. 2015, 116, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Brook, R.D.; Huang, W.; Fan, Z.; Xu, H.; Wu, R.; Sun, Z.; Zhao, X.; Ruan, Y.; Yan, J.; et al. Extreme levels of ambient air pollution adversely impact cardiac and central aortic hemodynamics: The aircmd-china study. J. Am. Soc. Hypertens. 2017, 11, 754–761. [Google Scholar] [CrossRef] [PubMed]
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B.; Kaufman, J.D. Long-term air pollution exposure and cardio- respiratory mortality: A review. Environ. Health 2013, 12, 43. [Google Scholar] [CrossRef] [PubMed]
- Eze, I.; Schaffner, E.; Fischer, E.; Schikowski, T.; Adam, M.; Imboden, M.; Tsai, M.; Carballo, D.; Von Eckardstein, A.; Kunzli, N.; et al. Long-term air pollution exposure and diabetes in a population-based swiss cohort. Environ. Int. 2014, 70, 95–105. [Google Scholar] [CrossRef]
- Milojevic, A.; Wilkinson, P.; Armstrong, B.; Bhaskaran, K.; Smeeth, L.; Hajat, S. Short-term effects of air pollution on a range of cardiovascular events in england and wales: Case-crossover analysis of the minap database, hospital admissions and mortality. Heart 2014, 100, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Stafoggia, M.; Samoli, E.; Alessandrini, E.; Cadum, E.; Ostro, B.; Berti, G.; Faustini, A.; Jacquemin, B.; Linares, C.; Pascal, M.; et al. Short-term associations between fine and coarse particulate matter and hospitalizations in southern europe: Results from the med-particles project. Environ. Health Perspect. 2013, 121, 1026–1033. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Cakmak, S.; Turner, M.C.; Brook, J.R.; Crouse, D.L.; Peters, P.A.; van Donkelaar, A.; Villeneuve, P.; Brion, O.; Jerrett, M.; et al. Long-term fine particulate matter exposure and mortality from diabetes in canada. Diabetes Care 2013, 36, 3313–3320. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Rajagopalan, S.; Arden Pope, C., III; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the american heart association. (aha scientific statements) (report). Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef] [PubMed]
- Pinault, L.; Tjepkema, M.; Crouse, D.L.; Weichenthal, S.; van Donkelaar, A.; Martin, R.V.; Brauer, M.; Chen, H.; Burnett, R.T. Risk estimates of mortality attributed to low concentrations of ambient fine particulate matter in the canadian community health survey cohort. Environ. Health Glob. Access Sci. Source 2016, 15, 18. [Google Scholar] [CrossRef]
- Chirinos, J.; Zambrano, J.P.; Veerani, A.; Schob, A.; Perez, G.; Mendez, A.; Chakko, S. Aortic pressure augmentation predicts adverse cardiovascular events in patients with established coronary artery disease. Eur. Heart J. 2005, 26, 696–697. [Google Scholar]
- The Internaltional Expert Committee. International expert committee report on the role of the a1c assay in the diagnosis of diabetes. Diabetes Care 2009, 32, 1327–1334. [Google Scholar] [CrossRef]

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gilbey, S.E.; Reid, C.M.; Huxley, R.R.; Soares, M.J.; Zhao, Y.; Rumchev, K. Associations Between Sub-Clinical Markers of Cardiometabolic Risk and Exposure to Residential Indoor Air Pollutants in Healthy Adults in Perth, Western Australia: A Study Protocol. Int. J. Environ. Res. Public Health 2019, 16, 3548. https://doi.org/10.3390/ijerph16193548
Gilbey SE, Reid CM, Huxley RR, Soares MJ, Zhao Y, Rumchev K. Associations Between Sub-Clinical Markers of Cardiometabolic Risk and Exposure to Residential Indoor Air Pollutants in Healthy Adults in Perth, Western Australia: A Study Protocol. International Journal of Environmental Research and Public Health. 2019; 16(19):3548. https://doi.org/10.3390/ijerph16193548
Chicago/Turabian StyleGilbey, Suzanne E., Christopher M. Reid, Rachel R. Huxley, Mario J. Soares, Yun Zhao, and Krassi Rumchev. 2019. "Associations Between Sub-Clinical Markers of Cardiometabolic Risk and Exposure to Residential Indoor Air Pollutants in Healthy Adults in Perth, Western Australia: A Study Protocol" International Journal of Environmental Research and Public Health 16, no. 19: 3548. https://doi.org/10.3390/ijerph16193548
APA StyleGilbey, S. E., Reid, C. M., Huxley, R. R., Soares, M. J., Zhao, Y., & Rumchev, K. (2019). Associations Between Sub-Clinical Markers of Cardiometabolic Risk and Exposure to Residential Indoor Air Pollutants in Healthy Adults in Perth, Western Australia: A Study Protocol. International Journal of Environmental Research and Public Health, 16(19), 3548. https://doi.org/10.3390/ijerph16193548