Hospitalization Costs and Financial Burden on Families with Children with Depression: A Cross-Section Study in Shandong Province, China



Abstract
:1. Introduction
2. Materials and Method
2.1. Settings and Data Source
2.2. Study Population
2.3. Statistical Analysis
3. Results
3.1. Basic Information on the Participants
3.2. Factors Associated with Total Hospitalization Costs, Length of Stay and Out-of-Pocket Expenses
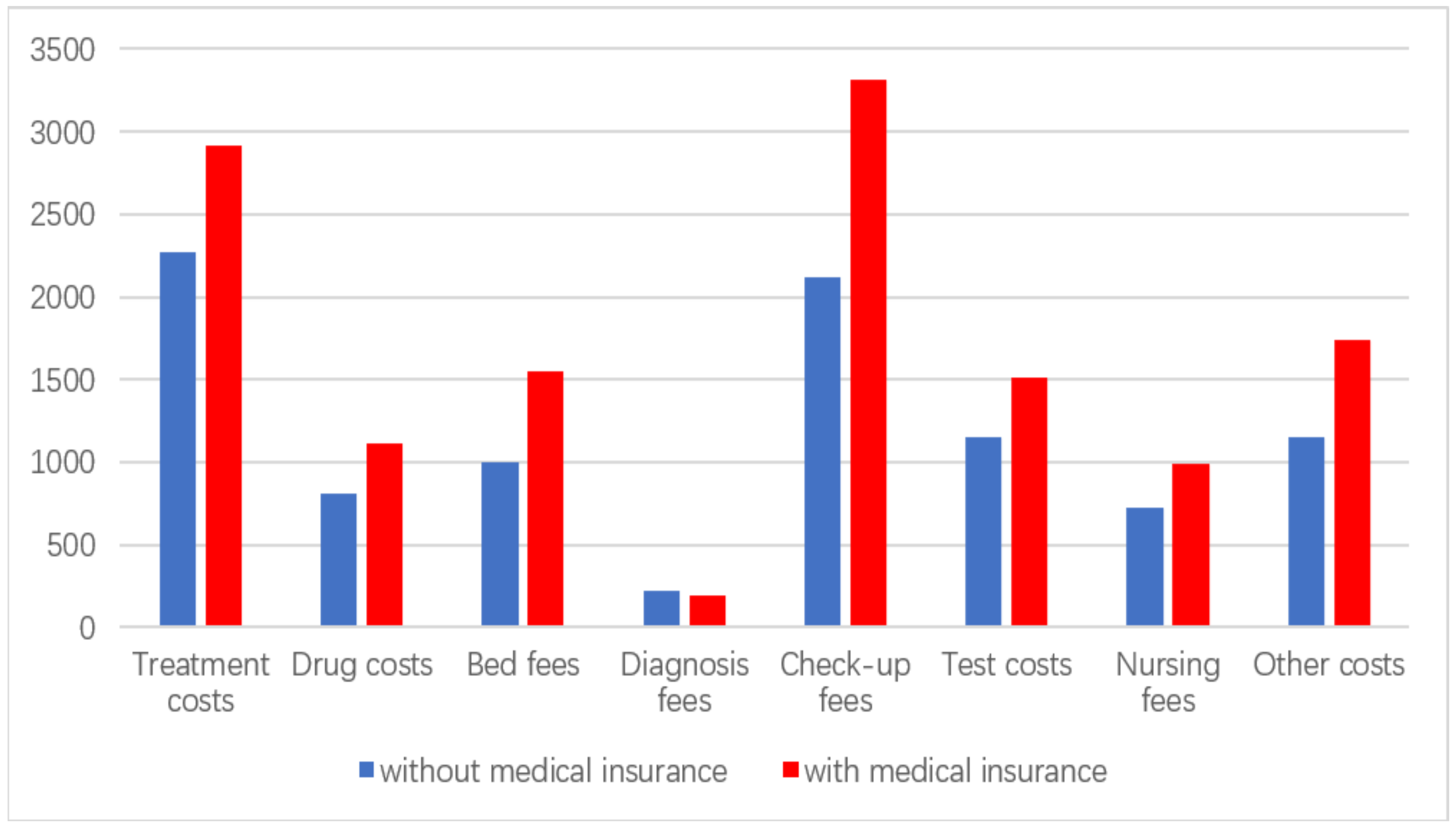
3.3. Hospitalization Costs of Children with Depression with and without Medical Insurance
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ebmeier, K.P.; Donaghey, C.; Steele, J.D. Recent developments and current controveries in depression. Lancet 2006, 367, 153–167. [Google Scholar] [CrossRef]
- Greenberg, P.E.; Birnbaum, H.G. The economic burden of depression in the US: Societal and patient perspectives. Expert Opin. Pharmacother. 2005, 6, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Holvast, F.; Massoudi, B.; Voshaar, R.C.O.; Verhaak, P.F. Non-pharmacological treatment for depressed older patients in primary care: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0184666. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Chen, Y.; Yue, L.; Liu, Q.; Montgomery, W.; Zhi, L.; Wang, W. Medication use patterns, health care resource utilization, and economic burden for patients with major depressive disorder in Beijing, People’s Republic of China. Neuropsychiatr. Dis. Treat. 2016, 12, 941. [Google Scholar] [PubMed]
- Murray, C.J.; Lopez, A.D. Evidence-based health policy--lessons from the Global Burden of Disease Study. Science 1996, 274, 740–743. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Lopez, A.D.; World Health Organization. The global burden of disease: A comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020: Summary. 1996. Available online: https://apps.who.int/iris/handle/10665/41864 (accessed on 25 July 2019).
- World Health Organization. Adolescent mental health. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health (accessed on 25 July 2019).
- Vashisht, A.; Gadi, N.A.; Singh, J.; Mukherjee, M.P.; Pathak, R.; Mishra, P. Prevalence of depression & assessment of risk factors among school going adolescents. Indian J. Community Health 2014, 26, 196–199. [Google Scholar]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yap, M.B.H.; Fowler, M.; Reavley, N.; Jorm, A.F. Parenting strategies for reducing the risk of childhood depression and anxiety disorders: A Delphi consensus study. J. Affect. Disord. 2015, 183, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Last, G.; Hansen, C.; Franco, C.; Anxious, N. Children in Adulthood: A Prospective Study of Adjustment. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Mathews, R.R.; Hall, W.D.; Vos, T.; Patton, G.C.; Degenhardt, L. What are the major drivers of prevalent disability burden in young Australians? Med. J. Aust. 2011, 194, 232–235. [Google Scholar]
- Patton, G.C.; Coffey, C.; Sawyer, S.M.; Viner, R.M.; Haller, D.M.; Bose, K.; Vos, P.T.; Ferguson, J.; Mathers, C.D. Global patterns of mortality in young people: A systematic analysis of population health data. Lancet 2009, 374, 881–892. [Google Scholar] [CrossRef]
- Phillips, M.R.; Zhang, J.; Shi, Q.; Song, Z.; Ding, Z.; Pang, S.; Li, X.; Zhang, Y.; Wang, Z. Prevalence, treatment, and associated disability of mental disorders in four provinces in China during 2001-05: An epidemiological survey. Lancet 2009, 373, 2041–2053. [Google Scholar] [CrossRef]
- Qin, X.; Wang, S.; Hsieh, C.R. The prevalence of depression and depressive symptoms among adults in China: Estimation based on a National Household Survey. China Econ. Rev. 2018, 51, 271–282. [Google Scholar] [CrossRef]
- Yang, G.; Wang, Y.; Zeng, Y.; Gao, G.F.; Liang, X.; Zhou, M.; Wan, X.; Yu, S.; Jiang, Y.; Naghavi, M. Rapid health transition in China, 1990-2010: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 381, 1987–2015. [Google Scholar] [CrossRef]
- Williams, S.B.; O’Connor, E.A.; Eder, M.; Whitlock, E.P. Screening for Child and Adolescent Depression in Primary Care Settings: A Systematic Evidence Review for the US Preventive Services Task Force. Pediatrics 2009, 123, e716–e735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roseman, M.; Saadat, N.E.; Riehm, K.; Kloda, L.A.; Boruff, J.; Lckowicz, A.; Baltzer, F.; Katz, L.Y.; Patten, S.B.; Rousseau, C. Depression Screening and Health Outcomes in Children and Adolescents: A Systematic Review. Can. J. Psychiatry 2017. [Google Scholar] [CrossRef]
- Choi, S.; Hasche, L.; Nguyen, D. Effects of Depression on the Subsequent Year’s Healthcare Expenditures Among Older Adults: Two-Year Panel Study. Psychiatr. Q. 2014, 86, 225–241. [Google Scholar] [CrossRef] [PubMed]
- Pompili, M.; Innamorati, M.; Raja, M.; Falcone, I.; Ducci, G.; Angeletti, G.; David, L.; Paolo, G.; Roberto, T.; Eleonora, D.P. Tatarelli.Suicide risk in depression and bipolar disorder: Do impulsiveness-aggressiveness and pharmacotherapy predict suicidal intent? Neuropsychiatr. Dis. Treat. 2008, 4, 247–255. [Google Scholar] [CrossRef]
- Wang, P.S.; Simon, G.; Kessler, R.C. The Economic Burden of Depression and the Cost-Effectiveness of Treatment. Int. J. Methods Psychiatr. Res. 2003, 12, 22–33. [Google Scholar] [CrossRef]
- Pirraglia, P.A.; Rosen, A.B.; Hermann, R.C.; Olchanski, N.V.; Neumann, P. Cost-Utility Analysis Studies of Depression Management: A Systematic Review. Am. J. Orthopsychiatry 2005, 161, 2155–2162. [Google Scholar] [CrossRef]
- Hsieh, C.R.; Qin, X. Depression hurts, depression costs: The medical spending attributable to depression and depressive symptoms in China. Health Econ. 2017, 27, 525–544. [Google Scholar] [CrossRef] [PubMed]
- Hu, R.; Liao, Y.; Du, Z.; Hao, Y.; Liang, H.; Shi, L. Types of health care facilities and the quality of primary care: A study of characteristics and experiences of Chinese patients in Guangdong Province, China. BMC Health Serv. Res. 2016, 16, 335. [Google Scholar] [CrossRef] [PubMed]
- Barber, S.L.; Borowitz, M.; Bekedam, H.; Ma, J. The hospital of the future in China: China’s reform of public hospitals and trends from industrialized countries. Health Policy Plan. 2013, 29, 367–378. [Google Scholar] [CrossRef] [PubMed]
- Olesen, J.; Gustavsson, A.; Svensson, M.; Wittchen, H.U.; Jönsson, B. The economic cost of brain disorders in Europe. Eur. J. Neurol. 2012, 19, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, L.; Manela, R.W.; Schiff, S. Sustaining Employment During Acute Mental Health Episodes. In Plenum Series in Rehablititation and Health; Springer: Boston, MA, USA, 2004; pp. 303–317. [Google Scholar]
- Andlin-Sobocki, P.; Jönsson, B.; Wittchen, H.U.; Olesen, J. Cost of disorders of the brain in Europe. Eur. J. Neurol. 2005. [Google Scholar] [CrossRef] [PubMed]
- Luppa, M.; Heinrich, S.; Angermeyer, M.C.; König, H.H.; Riedel-Heller, S.G. Cost-of-illness studies of depression: A systematic review. J. Affect. Disord. 2007, 98, 29–43. [Google Scholar] [CrossRef] [PubMed]
- Hawthorne, G.; Cheok, F.; Goldney, R.; Fisher, L. The Excess Cost of Depression in South Australia: A Population-Based Study. Aust. N. Z. J. Psychiatry 2003, 37, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Husaini, B.; Levine, R.; Lammers, P.; Hull, P.; Novotny, M.; Moonis, M. Smoking, depression, and hospital costs of respiratory cancers: Examining race and sex variation. Family Med. Community Health 2017, 5, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Husaini, B.A.; Levine, R.S.; Novotny, M.L.; Cain, V.A.; Sampson, U.K.; Moonis, M. Depression and race affect hospitalization costs of heart failure patients. Family Med. Community Health 2015, 3, 39–47. [Google Scholar] [CrossRef]
- Anderson, D.M.; Cesur, R.; Tekin, E. Youth Depression and Future Criminal Behavior. Econ. Inq. 2012, 53, 294–317. [Google Scholar] [CrossRef]
- Qin, X.; Pan, J. The Medical Cost Attributable to Obesity and Overweight in China: Estimation Based on Longitudinal Surveys. Health Econ. 2016, 5, 1291–1311. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.P.; Jin, A.Z.; Ho, R.; Chua, H.C.; Fones, C.S.; Lim, L. Health Beliefs and Help Seeking for Depressive and Anxiety Disorders Among Urban Singaporean Adults. Psychiatr. Serv. 2008, 59, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Tomonaga, Y.; Haettenschwiler, J.; Hatzinger, M.; Holsboer-Trachsler, E.; Rufer, M.; Hepp, U.; Szucs, T.D. The Economic Burden of Depression in Switzerland. PharmacoEconomics 2013, 31, 237–250. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, P.E.; Fournier, A.A.; Sisitsky, T.; Pike, C.T.; Kessler, R.C. The Economic Burden of Adults with Major Depressive Disorder in the United States (2005 and 2010). J. Clin. Psychiatry 2015, 76, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Hu, T. The Economic Burden of Depression and Reimbursement Policy in the Asia Pacific Region. Australas. Psychiatry 2004, 12 (Suppl. 1), s11–s15. [Google Scholar] [CrossRef] [PubMed]
- Hong, X.; Li, J.; Xu, F.; Tse, L.A.; Liang, Y.; Wang, Z.; Yu, I.T.; Griffiths, S. Physical activity inversely associated with the presence of depression among urban adolescents in regional China. BMC Public Health 2009, 9, 148. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Li, X.; Barnett, D.; Zhao, G.; Zhao, J.; Stanton, B. Risk and Protective Factors for Depression Symptoms among Children Affected by HIV/AIDS in Rural China: A Structural Equation Modeling Analysis. Soc. Sci. Med. 2012, 74, 1435–1443. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Mao, J.; Du, Y.; Morris, J.L.; Gong, G.; Xiong, X. Health-Related Quality of Life Among Pregnant Women With and Without Depression in Hubei, China. Matern. Child Health J. 2011, 16, 1355–1363. [Google Scholar] [CrossRef]
- Su, X.; Lau, J.T.; Mak, W.W.; Choi, K.C.; Chen, L.; Song, J.; Zhang, Y.; Zhao, G.; Feng, T.; Chen, X. Prevalence and associated factors of depression among people living with HIV in two cities in China. J. Affect. Disord. 2013, 149, 108–115. [Google Scholar] [CrossRef]
- Jiang, J.; Tang, Z.; Futatsuka, M. The Impact of ADL Disability on Depression Symptoms in a Community of Beijing Elderly, China. Environ. Health Prev. Med. 2002, 7, 199–204. [Google Scholar] [Green Version]
- Druss, G.B.; Rosenheck, R.; Sledge, W. Health and Disability Costs of Depressive Illness in a Major, U.S. Corporation. Am. J. Psychiat. 2000, 157, 1274–1278. [Google Scholar] [CrossRef] [PubMed]
- Sacco, P.; Unick, G.J.; Zanjani, F.; Camlin, E.A. Hospital Outcomes in Major Depression Among Older Adults: Differences by Alcohol Comorbidity. J. Dual. Diagn. 2015, 11, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Koretz, D.; Merikangas, K.R.; Rush, A.J.; Walters, E.E.; Wang, P.S. The epidemiology of major depressive disorder: Results From the National Comorbidity Survey Replication (NCS-R). Jama 2003, 289, 3095–3105. [Google Scholar] [CrossRef] [PubMed]
- Ormel, J.; Oldehinkel, A.J.; Nolen, W.A.; Vollebergh, W. Psychosocial Disability Before, During, and After a Major DepressiveEpisode: A 3-Wave Population-Based Study of State, Scar, and Trait Effects. Arch. Gen. Psychiatry 2004, 61, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Kepler, K.L.; Perlman, S.E.; Chernov, C.; Thorpe, L.E.; Hoenig, J.; Norman, C. The Burden of Depression in New York City Adults: Results from the 2013–14 NYC Health and Nutrition Examination Survey. J. Urban Health 2018, 95, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Evans, D.B.; Kawabata, K.; Zeramdini, R.; Klavus, J.; Murray, C.J. Household catastrophic health expenditure: A multicountry analysis. Lancet 2003, 362, 111–117. [Google Scholar] [CrossRef]
- Zha, B. The gap of economic development expanding between eastern China and middle, western China. China Popul. Res. Newsl. 1996, 2–3. [Google Scholar]
- Liyong, X. Shandong is a classic epitome of China in transition-visiting zhang weiguo, researcher of shandong academy of social sciences. Soc. Obs. 2006, 11. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | Observation | % |
|---|---|---|
| Age | ||
| 9–11 | 145 | 29.71 |
| 12–14 | 151 | 30.94 |
| 15–17 | 192 | 39.35 |
| Sex | ||
| males | 252 | 51.64 |
| females | 236 | 48.36 |
| Regional distribution | ||
| west | 239 | 48.98 |
| middle | 173 | 35.45 |
| east | 76 | 15.57 |
| Comorbidities | ||
| yes | 227 | 46.52 |
| no | 261 | 53.48 |
| Medical insurance | ||
| yes | 364 | 74.59 |
| no | 124 | 25.41 |
| Type of health facility | ||
| public | 438 | 89.75 |
| private | 50 | 10.25 |
| Total observations (%) | 488 | 100.00 |
| Total Costs (mean ± SD) | p-Value | Out-of-Pocket (mean ± SD) | p-Value | length of Stay (mean ± SD) | p-Value | |
|---|---|---|---|---|---|---|
| Sex | 0.5175 | 0.9206 | 0.2958 | |||
| males | 13844.46 ± 575.60 | 7637.34 ± 354.62 | 37.01 ± 1.86 | |||
| females | 13312.61 ± 584.88 | 7585.10 ± 386.79 | 34.38 ± 1.67 | |||
| Age | 0.5281 | 0.4206 | 0.4800 | |||
| 9-11 | 12905.82 ± 753.79 | 7086.04 ± 453.18 | 32.89 ± 2.21 | |||
| 12-14 | 13689.74 ± 758.79 | 7890.88 ± 486.63 | 36.22 ± 2.20 | |||
| 15-17 | 14021.27 ± 638.56 | 7790.07 ± 422.37 | 37.52 ± 2.10 | |||
| Regional distribution | 0.4710 | 0.0905 | 0.0011 | |||
| west | 14095.90 ± 620.66 | 7644.54 ± 372.81 | 37.97 ± 1.84 | |||
| middle | 13167.92 ± 682.49 | 8111.79 ± 460.93 | 37.36 ± 2.27 | |||
| east | 12942.23 ± 844.70 | 6372.50 ± 571.83 | 25.03 ± 1.80 | |||
| Comorbidities | 0.1389 | 0.0009 | 0.3367 | |||
| yes | 13021.02 ± 509.34 | 6802.17 ± 297.98 | 34.61 ± 1.65 | |||
| no | 14238.29 ± 657.51 | 8543.30 ± 438.37 | 37.04 ± 1.92 | |||
| Medical insurance | 0.0001 | 0.0000 | 0.0000 | |||
| yes | 14528.05 ± 490.26 | 6517.38 ± 239.81 | 38.87 ± 1.52 | |||
| no | 10825.55 ± 674.39 | 10825.55 ± 674.39 | 26.54 ± 1.89 | |||
| Type of health facility | 0.7908 | 0.0065 | 0.5582 | |||
| public | 13624.06 ± 428.55 | 7372.22 ± 263.69 | 36.00 ± 1.32 | |||
| private | 13264.8 ± 1400.35 | 9713.26 ± 1049.14 | 33.56 ± 4.01 | |||
| Total | 13587.25 ± 410.07 | 7612.08 ± 261.50 | 35.74 ± 1.26 |
| Factors | Unstandardized Coefficients | SE | Standardized Coefficients | t-Value | p-Value |
|---|---|---|---|---|---|
| Medical insurance | 1911.308 | 187.191 | 0.184 | 3.923 | 0.000 |
| Comorbidities | 1087.368 | 829.169 | 0.060 | 1.311 | 0.190 |
| Age | 548.816 | 490.319 | 0.050 | 1.119 | 0.264 |
| Type of health facility | 1021.604 | 1390.286 | 0.034 | 0.735 | 0.463 |
| Sex | 395.350 | 811.625 | 0.022 | 0.487 | 0.626 |
| Region | 173.562 | 571.116 | 0.014 | 0.304 | 0.761 |
| Variable | All Patients (mean ± SD) | Patients with Insurance (mean ± SD) | Patients without Insurance (mean ± SD) | t-Value | p-Value |
|---|---|---|---|---|---|
| length of stay | 35.74 ± 1.26 | 38.87 ± 1.52 | 26.54 ± 1.89 | 4.3525 | 0.0000 |
| Total costs | 13587.25 ± 410.07 | 14528.05 ± 490.26 | 10825.55 ± 674.39 | 3.9906 | 0.0001 |
| Treatment costs | 2748.97 ± 141.13 | 2913.32 ± 168.44 | 2266.54 ± 249.10 | 2.0012 | 0.0459 |
| Drug costs | 1036.58 ± 53.52 | 1112.57 ± 65.23 | 813.51 ± 85.00 | 2.4452 | 0.0148 |
| Bed fees | 1407.40 ± 55.55 | 1545.70 ± 66.73 | 1001.40 ± 87.80 | 4.3430 | 0.0000 |
| Diagnosis fees | 197.62 ± 21.44 | 188.91 ± 25.32 | 223.18 ± 42.74 | 0.6849 | 0.4937 |
| Check-up fees | 3011.26 ± 116.38 | 3314.98 ± 141.76 | 2119.70 ± 168.16 | 4.5615 | 0.0000 |
| Test costs | 1422.07 ± 48.08 | 1515.47 ± 58.68 | 1147.87 ± 73.27 | 3.3636 | 0.0008 |
| Nursing fees | 922.32 ± 44.23 | 989.24 ± 52.00 | 725.87 ± 81.45 | 2.6078 | 0.0094 |
| Other costs | 1591.54 ± 102.34 | 1740.25 ± 117.67 | 1155.00 ± 202.91 | 2.5031 | 0.0126 |
| Out-of-pocket | 7612.08 ± 261.50 | 6517.38 ± 239.81 | 10825.55 ± 674.39 | 7.5762 | 0.0000 |
| Type | RMB | Percentage Total Costs (%) | |
|---|---|---|---|
| 1 | Total hospitalization costs—age <18, depression | 6630578 | 0.016 |
| 2 | Total hospitalization costs—all ages with depression | 95236390 | 0.235 |
| 3 | Total hospitalization costs—all diseases | 40554194453 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, Y.; Sun, J.; Hu, S.; Nicholas, S.; Wang, J. Hospitalization Costs and Financial Burden on Families with Children with Depression: A Cross-Section Study in Shandong Province, China. Int. J. Environ. Res. Public Health 2019, 16, 3526. https://doi.org/10.3390/ijerph16193526
Guo Y, Sun J, Hu S, Nicholas S, Wang J. Hospitalization Costs and Financial Burden on Families with Children with Depression: A Cross-Section Study in Shandong Province, China. International Journal of Environmental Research and Public Health. 2019; 16(19):3526. https://doi.org/10.3390/ijerph16193526
Chicago/Turabian StyleGuo, Yawei, Jingjie Sun, Simeng Hu, Stephen Nicholas, and Jian Wang. 2019. "Hospitalization Costs and Financial Burden on Families with Children with Depression: A Cross-Section Study in Shandong Province, China" International Journal of Environmental Research and Public Health 16, no. 19: 3526. https://doi.org/10.3390/ijerph16193526
APA StyleGuo, Y., Sun, J., Hu, S., Nicholas, S., & Wang, J. (2019). Hospitalization Costs and Financial Burden on Families with Children with Depression: A Cross-Section Study in Shandong Province, China. International Journal of Environmental Research and Public Health, 16(19), 3526. https://doi.org/10.3390/ijerph16193526