Health-Related Quality of Life and Associated Factors in Patients with Atrial Fibrillation: An Integrative Literature Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
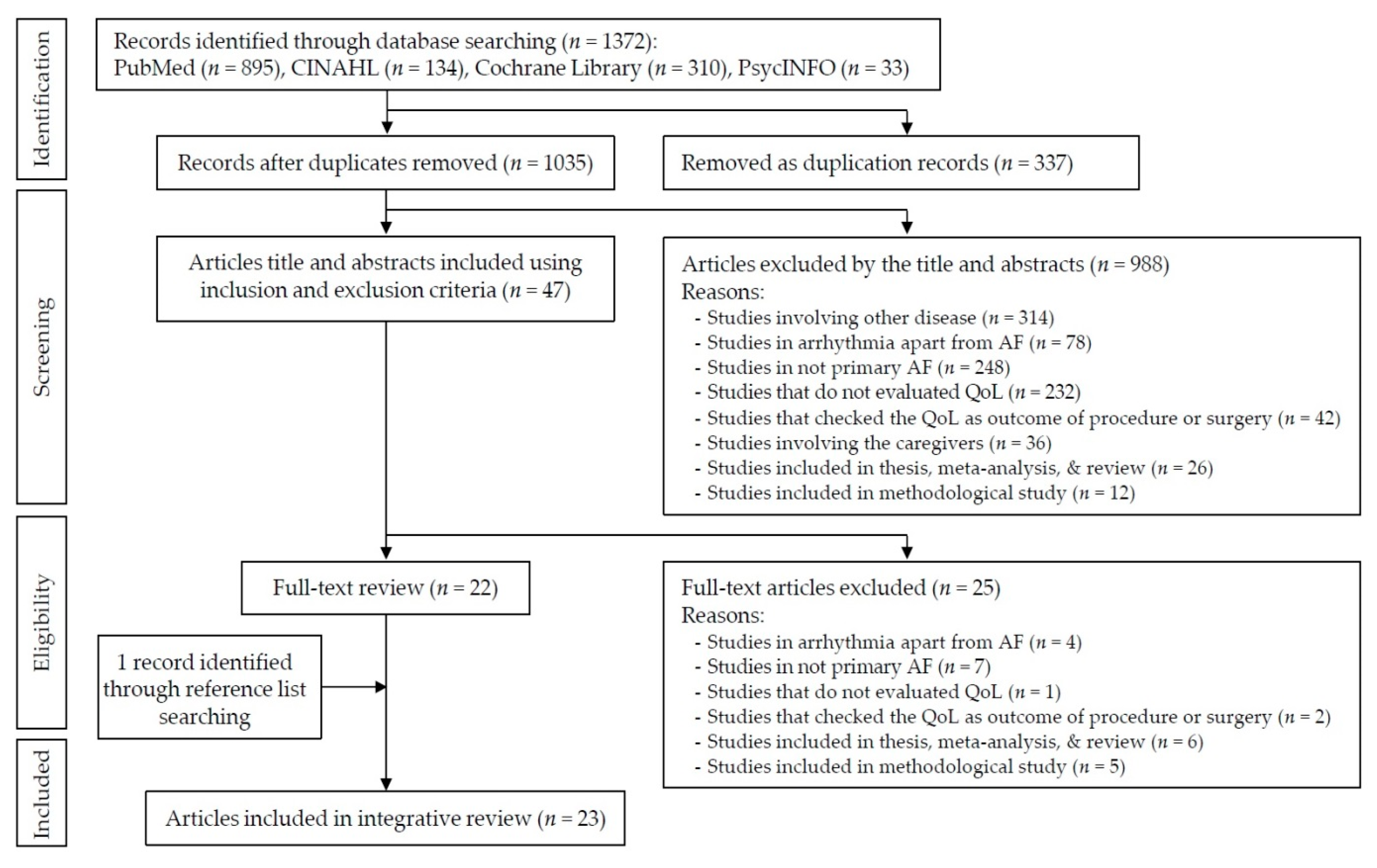
2.2. Problem Identification and Literature Search
2.3. Data Evaluation
2.4. Data Analysis
3. Results
3.1. Characteristics of Included Studies
3.2. HRQoL Scores in Patients with AF
3.3. Characteristics of the Instruments for HRQoL in Patients with AF
3.4. The Factors Influencing HRQoL in Patients with AF Based on HRQoL Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration with the Society of Thoracic Surgeons. Circulation 2019, 140, e125–e151. [Google Scholar] [CrossRef]
- Zulkifly, H.; Lip, G.Y.H.; Lane, D.A. Epidemiology of atrial fibrillation. Int. J. Clin. Pract. 2018, 72, e13070. [Google Scholar] [CrossRef]
- Rienstra, M.; Lubitz, S.A.; Mahida, S.; Magnani, J.W.; Fontes, J.D.; Sinner, M.F. Symptoms and functional status of patients with atrial fibrillation: State of the art and future research opportunities. Circulation 2012, 125, 2933–2943. [Google Scholar] [CrossRef] [PubMed]
- Pistoia, F.; Sacco, S.; Tiseo, C.; Degan, D.; Ornello, R.; Carolei, A. The epidemiology of atrial fibrillation and stroke. Cardiol. Clin. 2016, 34, 255–268. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.N.; Abdelhafiz, A. Clinical and economic implications of AF related stroke. J. Atr. Fibrillation 2016, 8, 1279. [Google Scholar] [CrossRef] [PubMed]
- Mas Dalmau, G.; Sant Arderiu, E.; Enfedaque Montes, M.B.; Solà, I.; Pequeño Saco, S.; Alonso Coello, P. Patients’ and physicians’ perceptions and attitudes about oral anticoagulation and atrial fibrillation: A qualitative systematic review. BMC Fam. Pract. 2017, 18, 3. [Google Scholar] [CrossRef]
- Thrall, G.; Lane, D.; Carroll, D.; Lip, G.Y. Quality of life in patients with atrial fibrillation: A systematic review. Am. J. Med. 2006, 119, 448.e1–448.e19. [Google Scholar] [CrossRef]
- Zhang, L.; Gallagher, R.; Neubeck, L. Health-related quality of life in atrial fibrillation patients over 65 years: A review. Eur. J. Prev. Cardiol. 2015, 22, 987–1002. [Google Scholar] [CrossRef] [PubMed]
- Gleason, K.T.; Nazarian, S.; Himmelfarb, C.D. Atrial fibrillation symptoms and sex, race, and psychological distress. J. Cardiovasc. Nurs. 2018, 33, 137–143. [Google Scholar] [CrossRef]
- Son, Y.J.; Seo, E.J. Impact of sociodemographic and clinical factors on health-related quality of life in older adults with atrial fibrillation. Res. Gerontol. Nurs. 2018, 11, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Walters, T.E.; Wick, K.; Tan, G.; Mearns, M.; Joseph, S.A.; Morton, J.B.; Sanders, P.; Bryant, C.; Kistler, P.M.; Kalman, J.M. Symptom severity and quality of life in patients with atrial fibrillation: Psychological function outweighs clinical predictors. Int. J. Cardiol. 2019, 279, 84–89. [Google Scholar] [CrossRef]
- Kotecha, D.; Ahmed, A.; Calvert, M.; Lencioni, M.; Terwee, C.B.; Lane, D.A. Patient-reported outcomes for quality of life assessment in atrial fibrillation: A systematic review of measurement properties. PLoS ONE 2016, 11, e0165790. [Google Scholar] [CrossRef]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef]
- Whittemore, R.; Chao, A.; Jang, M.; Minges, K.E.; Park, C. Methods for knowledge synthesis: An overview. Heart Lung 2014, 43, 453–461. [Google Scholar] [CrossRef]
- Ferrans, C.E.; Zerwic, J.J.; Wilbur, J.E.; Larson, J.L. Conceptual model of health-related quality of life. J. Nurs. Scholarsh. 2005, 37, 336–342. [Google Scholar] [CrossRef]
- Bakas, T.; McLennon, S.M.; Carpenter, J.S.; Buelow, J.M.; Otte, J.L.; Hanna, K.M.; Ellett, M.L.; Hadler, K.A.; Welch, J.L. Systematic review of health-related quality of life models. Health Qual. Life Outcomes 2012, 10, 134. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Luderitz, B.; Jung, W. Quality of life in patients with atrial fibrillation. Arch. Intern. Med. 2000, 160, 1749–1757. [Google Scholar] [CrossRef]
- Testa, M.A.; Simonson, D.C. Assessment of quality-of-life outcomes. N. Engl. J. Med. 1996, 334, 835–840. [Google Scholar] [CrossRef]
- Pace, R.; Pluye, P.; Bartlett, G.; Macaulay, A.C.; Salsberg, J.; Jagosh, J. Testing the reliability and efficiency of the pilot Mixed Methods Appraisal Tool (MMAT) for systematic mixed studies review. Int. J. Nurs. Stud. 2012, 49, 47–53. [Google Scholar] [CrossRef]
- Tobiano, G.; Marshall, A.; Bucknall, T.; Chaboyer, W. Patient participation in nursing care on medical wards: An integrative review. Int. J. Nurs. Stud. 2015, 52, 1107–1120. [Google Scholar] [CrossRef]
- Dorian, P.; Jung, W.; Newman, D.; Paquette, M.; Wood, K.; Ayers, G.M.; Camm, J.; Akhtar, M.; Luderitz, B. The impairment of health-related quality of life in patients with intermittent atrial fibrillation: Implications for the assessment of investigational therapy. J. Am. Coll. Cardiol. 2000, 36, 1303–1309. [Google Scholar] [CrossRef]
- Suzuki, S.; Kasanuki, H. The influences of psychosocial aspects and anxiety symptoms on quality of life of patients with arrhythmia: Investigation in paroxysmal atrial fibrillation. Int. J. Behav. Med. 2004, 11, 104–109. [Google Scholar] [CrossRef]
- van den Berg, M.P.; Ranchor, A.V.; van Sonderen, F.L.; van Gelder, I.C.; van Veldhuisen, D.J. Paroxysmal atrial fibrillation, quality of life and neuroticism. Neth. J. Med. 2005, 63, 170–174. [Google Scholar]
- Maryniak, A.; Walczak, F.; Bodalski, R.; Szumowski, L.; Derejko, P.; Urbanek, P. Atrial fibrillation onset circumstances and their relation to patients’ quality of life. Kardiol. Pol. 2006, 64, 1102–1108. [Google Scholar]
- Ong, L.; Cribbie, R.; Harris, L.; Dorian, P.; Newman, D.; Mangat, I.; Nolan, R.; Irvine, J. Psychological correlates of quality of life in atrial fibrillation. Qual. Life Res. 2006, 15, 1323–1333. [Google Scholar] [CrossRef]
- Singh, S.N.; Tang, X.C.; Singh, B.N.; Dorian, P.; Reda, D.J.; Harris, C.L.; Fletcher, R.D.; Sharma, S.C.; Atwood, J.E.; Jacobson, A.K. Quality of life and exercise performance in patients in sinus rhythm versus persistent atrial fibrillation: A Veterans Affairs Cooperative Studies Program Substudy. J. Am. Coll. Cardiol. 2006, 48, 721–730. [Google Scholar] [CrossRef]
- Hegbom, F.; Stavem, K.; Sire, S.; Heldal, M.; Orning, O.M.; Gjesdal, K. Effects of short-term exercise training on symptoms and quality of life in patients with chronic atrial fibrillation. Int. J. Cardiol. 2007, 116, 86–92. [Google Scholar] [CrossRef]
- Baek, K.H.; Son, Y.J. Relationships between symptom experience and quality of life in patients with atrial fibrillation. J. Korean Acad. Fundam. Nurs. 2008, 15, 485–494. [Google Scholar]
- Kang, Y. Gender and culture differences in the quality of life among Americans and Koreans with atrial fibrillation. Nurs. Health Sci. 2009, 11, 301–305. [Google Scholar] [CrossRef]
- Lane, D.A.; Langman, C.M.; Lip, G.Y.; Nouwen, A. Illness perceptions, affective response, and health-related quality of life in patients with atrial fibrillation. J. Psychosom. Res. 2009, 66, 203–210. [Google Scholar] [CrossRef]
- Dąbrowski, R.; Smolis-Bąk, E.; Kowalik, I.; Kazimierska, B.; Wójcicka, M.; Szwed, H. Quality of life and depression in patients with different patterns of atrial fibrillation. Kardiol. Pol. 2010, 68, 1133–1139. [Google Scholar]
- Jaber, J.; Cirenza, C.; Jaber, J.; Amaral, A.; Almeida de Sousa, J.M.; Oliveira Filho, J.A.; de Paola, A.A. Influence of heart rate on quality of life in patients with chronic atrial fibrillation. Clin. Cardiol. 2010, 33, E28–E32. [Google Scholar] [CrossRef]
- McCabe, P.J.; Schumacher, K.; Barnason, S.A. Living with atrial fibrillation: A qualitative study. J. Cardiovasc. Nurs. 2011, 26, 336–344. [Google Scholar] [CrossRef]
- Dorian, P.; Burk, C.; Mullin, C.M.; Bubien, R.; Godejohn, D.; Reynolds, M.R.; Lakkireddy, D.R.; Wimmer, A.P.; Bhandari, A.; Spertus, J. Interpreting changes in quality of life in atrial fibrillation: How much change is meaningful? Am. Heart J. 2013, 166, 381–387. [Google Scholar] [CrossRef]
- Goren, A.; Liu, X.; Gupta, S.; Simon, T.A.; Phatak, H. Quality of life, activity impairment, and healthcare resource utilization associated with atrial fibrillation in the US National Health and Wellness Survey. PLoS ONE 2013, 8, e71264. [Google Scholar] [CrossRef]
- Lakkireddy, D.; Atkins, D.; Pillarisetti, J.; Ryschon, K.; Bommana, S.; Drisko, J.; Vanga, S.; Dawn, B. Effect of yoga on arrhythmia burden, anxiety, depression, and quality of life in paroxysmal atrial fibrillation: The YOGA My Heart Study. J. Am. Coll. Cardiol. 2013, 61, 1177–1184. [Google Scholar] [CrossRef]
- Lee, S.J.; Seo, J.M. Factors influencing health-related quality of life in patients with atrial fibrillation. Korean J. Adult Nurs. 2013, 25, 13–23. [Google Scholar] [CrossRef]
- Schron, E.; Friedmann, E.; Thomas, S.A. Does health-related quality of life predict hospitalization or mortality in patients with atrial fibrillation? J. Cardiovasc. Electrophysiol. 2014, 25, 23–28. [Google Scholar] [CrossRef]
- Tsounis, D.; Ioannidis, A.; Bouras, G.; Raikou, M.; Giannopoulos, G.; Deftereos, S.; Kossyvakis, C.; Toutouzas, K.; Tousoulis, D.; Synetos, A.; et al. Assessment of health-related quality of life in a greek symptomatic population with atrial fibrillation: Correlation with functional status and echocardiographic indices. Hell. J. Cardiol. 2014, 55, 475–485. [Google Scholar]
- Yamamoto, M.; Watanabe, E.; Suzuki, T.; Yamazaki, T.; Ohtsu, H.; Ozaki, Y.; Ogawa, S.; Yamashita, T. J-RHYTHM II Investigators. Association between the quality of life and asymptomatic episodes of paroxysmal atrial fibrillation in the J-RHYTHM II study. J. Cardiol. 2014, 64, 64–69. [Google Scholar] [CrossRef]
- Altiok, M.; Yilmaz, M.; Rencüsoğullari, I. Living with atrial fibrillation: An analysis of patients’ perspectives. Asian Nurs. Res. 2015, 9, 305–311. [Google Scholar] [CrossRef]
- Freeman, J.V.; Simon, D.N.; Go, A.S.; Spertus, J.; Fonarow, G.C.; Gersh, B.J.; Hylek, E.M.; Kowey, P.R.; Mahaffey, K.W.; Thomas, L.E.; et al. Association between atrial fibrillation symptoms, quality of life, and patient outcomes: Results from the outcomes registry for better informed treatment of atrial fibrillation (ORBIT-AF). Circ. Cardiovasc. Qual. Outcomes 2015, 8, 393–402. [Google Scholar] [CrossRef]
- Bowyer, J.L.; Tully, P.J.; Ganesan, A.N.; Chahadi, F.K.; Singleton, C.B.; McGavigan, A.D. A randomised controlled trial on the effect of nurse-led educational intervention at the time of catheter ablation for atrial fibrillation on quality of life, symptom severity and rehospitalisation. Heart Lung Circ. 2017, 26, 73–81. [Google Scholar] [CrossRef]
- The Korean Society of Heart Failure. KSHF Guideline for the Management of Chronic Heart Failure 2016; The Korean Society of Heart Failure: Seoul, Korea, 2016; pp. 4–42. [Google Scholar]
- McCabe, P.J.; Barnason, S.A. Illness perceptions, coping strategies, and symptoms contribute to psychological distress in patients with recurrent symptomatic atrial fibrillation. J. Cardiovasc. Nurs. 2012, 27, 431–444. [Google Scholar] [CrossRef]
- National Institute of Nursing Research. The NINR Strategic Plan: Advancing Science, Improving Lives (2016). Available online: https://www.ninr.nih.gov/sites/www.ninr.nih.gov/files/NINR_StratPlan2016_reduced.pdf (accessed on 22 May 2019).
- Blustin, J.M.; McBane, R.D.; Ketha, S.S.; Wysokinski, W.E. Distribution of thromboembolism in valvular versus non-valvular atrial fibrillation. Expert Rev. Cardiovasc. Ther. 2014, 12, 1129–1132. [Google Scholar] [CrossRef][Green Version]
- Strømnes, L.A.; Ree, H.; Gjesdal, K.; Ariansen, I. Sex differences in quality of life in patients with atrial fibrillation: A systematic review. J. Am. Heart Assoc. 2019, 8, e010992. [Google Scholar] [CrossRef]
- Steinberg, B.A.; Piccini, J.P., Sr. Tackling patient-reported outcomes in atrial fibrillation and heart failure: Identifying disease-specific symptoms? Cardiol. Clin. 2019, 37, 139–146. [Google Scholar] [CrossRef]


{kind=link}
| Author (year), Country | Study Design | Admission Type | Sample Characteristics | Main Findings | Quality Appraisal by MMA (%) | |
|---|---|---|---|---|---|---|
| AF Type | n, male%, Mean Age (yrs) | |||||
| Dorian et al. (2000), Canada [22] | Case-control | Outpatients | Paroxysmal Persistent | AF; 152, 73%, 58.0 Healthy; 47, 45%, 54.0 PTCA; 69, 79%, 62.0 | The SF-36 subscale scores were lower in AF patients compared to the PTCA, healthy group (p < 0.05). Case group reported worse QoL than PTCA and healthy groups. | 100 |
| Suzuki et al. (2004), Japan [23] | Cross-sectional | Outpatients | Paroxysmal | 240, 69.6%, 57.9 | A significant difference was found between agoraphobic patients and nonagoraphobic patients in SDQL. Psychological stress is the main perceived inducer in daily life, and attack induced by psychological stress affects their anxiety symptoms and QoL. | 50 |
| Van den Berg et al. (2005), Netherlands [24] | Cross-sectional | Outpatients | Paroxysmal | 73, 68.5%, 55.5 | QoL in the physical domain and pain was not related to the degree of neuroticism (p = 0.81). | 50 |
| Maryniak et al. (2006), Poland [25] | Cross-sectional | Inpatients | Paroxysmal | 76, 73%, 53.2 | No significant relationship was shown among disease duration, comorbidities, and QoL. | 50 |
| Ong et al. (2006), Canada [26] | Cross-sectional | Outpatients | Paroxysmal Persistent Permanent | 93, 66%, 61.8 | PCS was 45.31 and MCS was 52.52 (SF-36: 0–100). AFSS was 7.11 (AFSS: 0–35) | 75 |
| Singh et al. (2006), USA and Canada [27] | Randomized controlled trial | Outpatients | Persistent | Con; 305, 99%, 67.3 Exp; 319, 99.7%, 66.4 | Favorable changes were seen in SF-36 subscales in SR patients at 1 year in general health (p = 0.007) and social functioning (p = 0.002). | 50 |
| Hegbom et al. (2007), Norway [28] | Randomized controlled trial | Outpatients | Chronic | Con. 15, 86.7%, 64.0 Exp. 13, 100%, 62.0 | SF-36 subscales (physical functioning, bodily pain, vitality, and role-emotional) improved significantly following Exercise Training Program. | 50 |
| Baek et al. (2008), Korea [29] | Cross-sectional | Outpatients | Persistent Permanent | 102, 55.9% | QoL measured by SF-36 (range: 0–100) had a low to moderate correlation with symptom frequency and severity. There were no significant differences in QoL according to gender, taking aspirin, or taking warfarin. | 100 |
| Kang (2009), Korea [30] | Cross-sectional | Outpatients | Not mentioned | 129, 50.3%, 63.2 | Americans’ QoL measured by SF-36 (range: 0–100); 33.53/51.43 vs. 41.46/46.12 (physical function/mental health, female vs. male) Koreans’ QoL measured by SF-36 (range: 0–100); 36.62/41.24 vs. 45.44/49.32 (physical function/mental health, female vs. male) The significant interaction effect of gender and culture on mental health was shown. | 75 |
| Lane et al. (2009), UK [31] | Prospective cohort | Outpatients | Persistent Permanent | 70, 64.3%, 71.4 | There were no significant differences in the levels of depression and perceived stress and HRQoL (except for an increase in energy and decline in general health perception) over the 12 months following diagnosis. Illness identity and beliefs about medication are significant predictors of the improvement in physical HRQoL over time. | 100 |
| Dabrowski et al. (2010), Poland [31] | Case-control | Not mentioned | Paroxysmal Persistent Permanent | AF; 95, 63.3%, 67.8 Healthy; 70, 42.9%, 55.5 | The scores of NHP (range: 0–100) were lower in paroxysmal, persistent, and permanent AF patients compared to the healthy. | 100 |
| Jaber et al. (2010), Brazil [33] | Case-control | Outpatients | Chronic | 89, 100%, 54.2 | There was a significant difference in QoL in physical and mental summary scores in patients with maximal HR ≤ 110 bpm on 6MWT in comparison with HR > 110 bpm and in the physical summary score in patients with average HR ≤ 80 bpm on Holter monitor in comparison with HR > 80 bpm. | 75 |
| McCabe et al. (2011), USA [34] | Phenomenology | Outpatients | Paroxysmal Persistent | 15, 53.3%, 59.8 | Themes included (1) finding the meaning of symptoms, (2) feeling uninformed and unsupported, (3) turning points, (4) steering clear of AF, (5) managing unpredictable and function-limiting symptoms, (6) emotional distress, and (7) accommodation to AF tempered with hope for a cure. | 100 |
| Dorian et al. (2013), Canada [35] | Prospective cohort | Inpatients | Paroxysmal Persistent Permanent | 210, 56.7%, 62.1 | AF patients’ QoL measured by AFEQT (range: 0–100). 59.5 (baseline); 72.4 (3 months) (p < 0.01) The improvement that 19 points in the AFEQT score changed can be termed a meaningful, important improvement. | 100 |
| Goren et al. (2013), USA [36] | Case-control | Outpatients | Not mentioned | 1,296, 65.1%, 64.9 | AF patients’ vs. non-AF controls’ QoL measured by SF-36 (range: 0-100); 38.6 vs. 44.8 (p < 0.001, PCS), 49.7 vs. 51.6 (p < 0.001, MCS) AF patients had lower MCS, PCS and utility scores, greater activity impairment, more traditional provider visits, and increased emergency room visits and hospitalizations. | 75 |
| Lakkireddy et al. (2013), USA [37] | Prospective cohort | Outpatients | Paroxysmal | 49, 46.9%, 60.6 | Yoga training improved the QoL parameters of physical functioning, general health, vitality, social functioning, and mental health domains on SF-36. | 100 |
| Lee et al. (2013), Korea [38] | Cross-sectional | Inpatients | Paroxysmal Persistent | 150, 51.3%, 62.4 | PCS was 38.92 and MCS was 41.49 (SF-36: 0–100). Physical and mental HRQoL had significant correlations with uncertainty, anxiety, and depression. | 100 |
| Schron et al. (2014), USA [39] | Cross-sectional | Not mentioned | Not mentioned | 693, 62.2%, 69.8 | History of stroke, heart failure, rhythm control, lower QoL (PCS and MCS in SF-36) predicted hospitalization. Diabetes, female gender, older age, CAD, hypertension, and lower PCS in SF-36 predicted mortality. | 75 |
| Tsounis et al. (2014), Greece [40] | Cross-sectional | Inpatients | Paroxysmal Persistent Permanent | 108, 64%, 65.4 | PCS was 40.28 and MCS was 40.89 (SF-36, range: 0–100). EQ-VAS (range: 3–100) was 59.63. | 50 |
| Yamamoto et al. (2014), Japan [41] | Prospective cohort | Outpatients | Paroxysmal | 233, 71%, 64.9 | Asymptomatic AF episode frequency correlates with a reduced QoL in patients with paroxysmal AF. | 100 |
| Altiok et al. (2015), Turkey [42] | Phenomenology | Outpatients | Not mentioned | 32, 50%, 66.9 | Four main themes and 15 subthemes were identified: (1) patient’s mental status regarding the disease, (2) patient’s social status regarding the disease, (3) patient’s physical condition regarding the disease, and (4) disease management and coping with the disease. | 100 |
| Freeman et al. (2015), USA [43] | Prospective cohort | Outpatients | Paroxysmal Persistent Permanent | 10,087, 57.6%, 75 | The AFEQT score decreased with increasing EHRA symptom severity class. Lower QoL was associated with a higher risk of hospitalization, but not other major adverse events, including death. | 100 |
| Bowyer et al. (2017), Australia [44] | Randomized controlled trial | Inpatients | Paroxysmal Non-paroxysmal | Con; 19, 57.9%, 62.1 Exp; 22, 76.2%, 61 | The nurse intervention group showed significant differences compared to the control with respect to higher QoL on the SF-36 score of physical functioning and vitality at six months. | 100 |
| Instrument Type | Instrument | Article Number | No. of Items | Reliability * | Validity |
|---|---|---|---|---|---|
| AF-specific | AFEQT | [35,43] | 20 | 0.88–0.95 | Reported |
| AFSS | [22,26,27] | 14 | 0.94 | Reported | |
| AFQLQ | [41] | 26 | 0.78–0.89 | Reported | |
| Cardiac-specific | NHP | [32] | 45 | 0.72 | Reported |
| IIRS | [22] | 13 | 0.88 | Reported | |
| QLI-CV | [39] | 35 | 0.94–0.95 | Reported | |
| SCL | [22,27] | 16 | 0.84–0.91 | Reported | |
| SDQL | [23] | 8 | Reported | Reported | |
| Generic | SF-12 | [36] | 12 | 0.89 (PCS) and 0.86 (MCS) | Reported |
| SF-36 | [22,24,25,26,27,28,29,30,31,33,37,38,39,40,44] | 36 | 0.89–0.93 (PCS) and 0.84–0.88 (MCS) | Reported | |
| SAS | [22,27] | 20 | 0.62 ** | Reported | |
| EQ-5D | [40] | 5 | 0.70 | Reported | |
| EQ-VAS | [40] | 1 | NA | Reported |
| Domain (No. of Predictors/Articles) | Factors (Frequency) | Article Number(s) | Significance |
|---|---|---|---|
| Biological function | Duration of illness (2) | [22,38] | –/+++ |
| (9/7) | Left ventricle ejection fraction (LVEF) (1) | [22] | – |
| Left atrial dimension (1) | [22] | – | |
| Stroke of comorbidity (1) | [29] | ++ | |
| Type of AF (1) | [32] | + | |
| Heart rate (1) | [33] | + | |
| CHADS2 score (1) | [36] | +++ | |
| Brain natriuretic peptide (BNP) level (1) | [40] | ++ | |
| LV systolic and diastolic function (1) | [40] | +++ | |
| Symptoms | Anxiety (4) | [23,26,31,38] | ++/++/++/+++ |
| (5/9) | Symptom frequency and severity (4) | [22,29,35,43] | +/+++/NA/+++ |
| Depression (2) | [32,40] | ++/+++ | |
| Perceived stress (1) | [31] | +++ | |
| Uncertainty (1) | [38] | +++ | |
| Functional status | NYHA class (3) | [22,29,38] | +/+++/+++ |
| (2/4) | Exercise performance (1) | [27] | ++ |
| General health | Fear of AF attack (1) | [23] | ++ |
| perceptions | Illness perception/identity (1) | [31] | + |
| (9/4) | Emotional distress including anxiety and fear of stroke (2) | [34,42] | Qualitative studies |
| Feeling uninformed and unsupported (2) | [34,42] | Qualitative studies | |
| Acceptance of the disease (2) | [34,42] | Qualitative studies | |
| Positive coping with living with AF (2) | [34,42] | Qualitative studies | |
| Adverse effect of social life (1) | [42] | Qualitative studies | |
| Inability to carry out daily living activities (1) | [42] | Qualitative studies | |
| Sexual problem (1) | [42] | Qualitative studies | |
| Characteristics of | Exercise intervention (2) | [28,37] | ++/+++ |
| the individual | Gender (3) | [25,30,32] | +/+/+ |
| (8/9) | Age (2) | [29,38] | ++/+++ |
| Alcohol use (1) | [29] | +++ | |
| Sleep (1) | [25] | ++ | |
| Employment (1) | [29] | + | |
| Optimism (1) | [40] | ++ | |
| Neuroticism (1) | [24] | ++ | |
| Characteristics of | Significant others (1) | [38] | +++ |
| the environment (2/1) | Financial burden (1) | [38] | +++ |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Son, Y.-J.; Baek, K.-H.; Lee, S.J.; Seo, E.J. Health-Related Quality of Life and Associated Factors in Patients with Atrial Fibrillation: An Integrative Literature Review. Int. J. Environ. Res. Public Health 2019, 16, 3042. https://doi.org/10.3390/ijerph16173042
Son Y-J, Baek K-H, Lee SJ, Seo EJ. Health-Related Quality of Life and Associated Factors in Patients with Atrial Fibrillation: An Integrative Literature Review. International Journal of Environmental Research and Public Health. 2019; 16(17):3042. https://doi.org/10.3390/ijerph16173042
Chicago/Turabian StyleSon, Youn-Jung, Kyoung-Hwa Baek, Suk Jeong Lee, and Eun Ji Seo. 2019. "Health-Related Quality of Life and Associated Factors in Patients with Atrial Fibrillation: An Integrative Literature Review" International Journal of Environmental Research and Public Health 16, no. 17: 3042. https://doi.org/10.3390/ijerph16173042
APA StyleSon, Y.-J., Baek, K.-H., Lee, S. J., & Seo, E. J. (2019). Health-Related Quality of Life and Associated Factors in Patients with Atrial Fibrillation: An Integrative Literature Review. International Journal of Environmental Research and Public Health, 16(17), 3042. https://doi.org/10.3390/ijerph16173042