Seasonal and Monthly Patterns, Weekly Variations, and the Holiday Effect of Outpatient Visits for Type 2 Diabetes Mellitus Patients in China

 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Subjects
2.3. Methods
2.4. Ethical Considerations
3. Results
3.1. The Outpatient Visits of T2DM Patients in Each Season
3.2. The Seasonal Index of T2DM Outpatient Visits in Each Season and Month
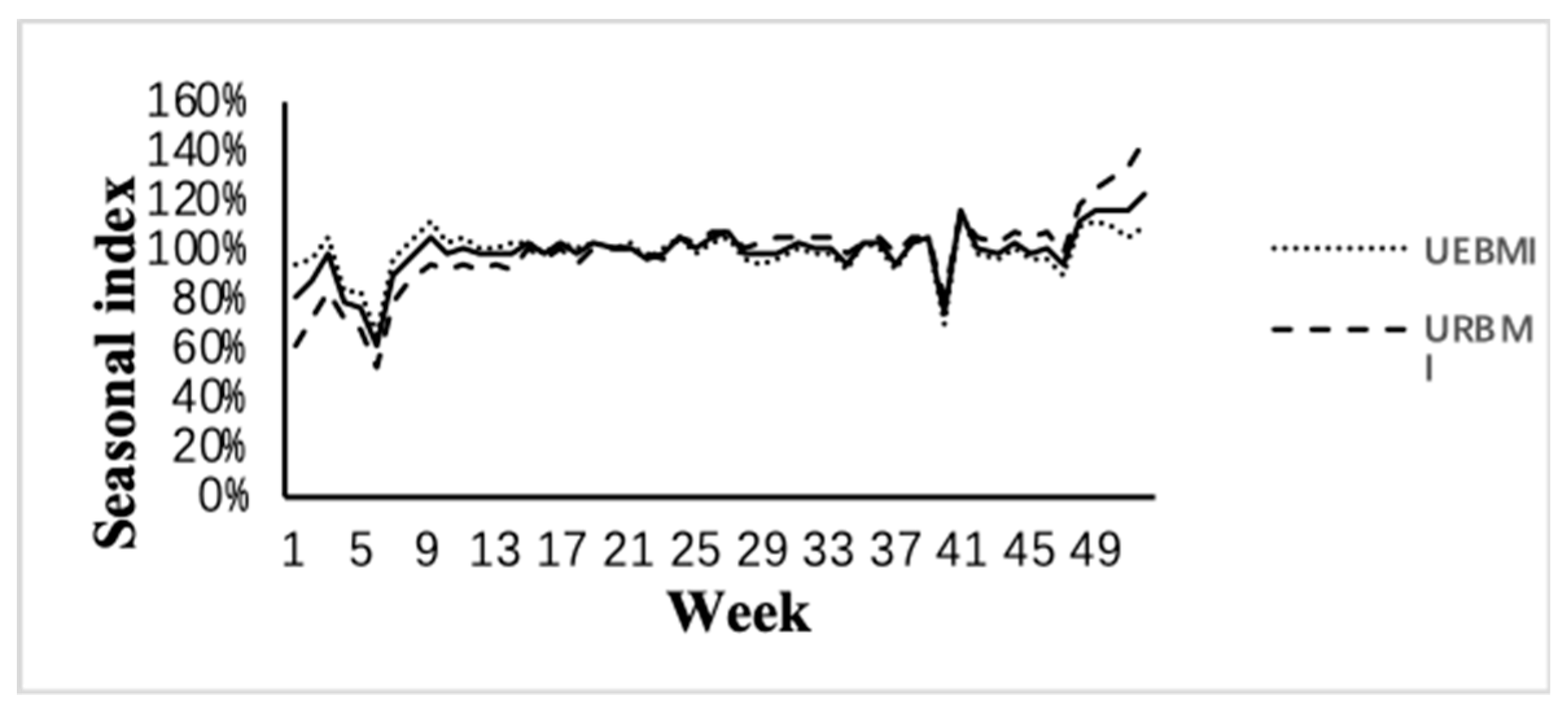
3.3. The Seasonal Index of T2DM Outpatient Visits in Each Week
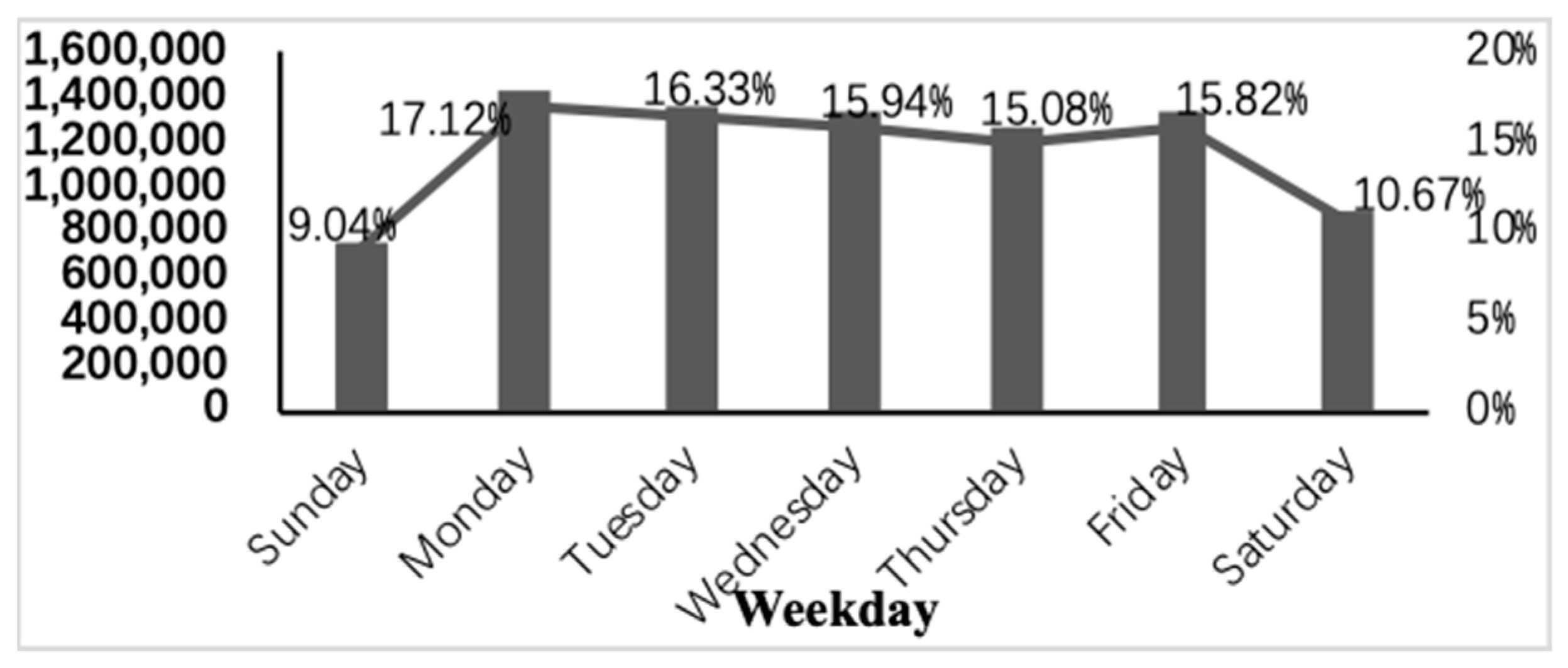
3.4. T2DM Outpatient Visits at Weekends
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hou, L.; Li, M.; Huang, X.; Wang, L.; Sun, P.; Shi, R.; Ding, L.; Pang, S. Email Seasonal variation of hemoglobin A1c levels in patients with type 2 diabetes. Int. J. Diabetes Dev. C 2017, 37, 432–436. [Google Scholar] [CrossRef]
- Ryu, O.H.; Lee, S.; Yoo, H.J.; Choi, M.G. Seasonal variations in glycemic control of type 2 diabetes in Korean women. J. Endocrinol. Investig. 2014, 37, 575–581. [Google Scholar] [CrossRef]
- Sohmiya, M.; Kanazawa, I.; Kato, Y. Seasonal changes in body composition and blood HbA1c levels without weight change in male patients with type 2 diabetes treated with insulin. Diabetes Care 2004, 27, 1238–1239. [Google Scholar] [CrossRef] [PubMed]
- Ishii, H.; Suzuki, H.; Baba, T.; Nakamura, K.; Watanabe, T. Seasonal variation of glycemic control in type 2 diabetic patients. Diabetes Care 2001, 24, 1503. [Google Scholar] [CrossRef] [PubMed]
- Hajat, S.; Haines, A.; Sarran, C.; Sharma, A.; Bates, C. Fleming the effect of ambient temperature on type-2-diabetes: Case-crossover analysis of 4+ million GP consultations across England. Environ. Health 2017, 16, 73. [Google Scholar] [CrossRef] [PubMed]
- Alba-García, J.E.G.; Salcedo-Rocha, A.L.; Ramos-Pinzon, E. The seasonality variation plays an important role for increasing the uncontrolled type 2 diabetes? Int. J. Diabetes Dev. C 2017, 37, 92–93. [Google Scholar] [CrossRef]
- Lontchi-Yimagou, E.; Tsalefac, M.; Tapinmene, L.M.T. Seasonality in diabetes in Yaounde, Cameroon: A relation with precipitation and temperature. BMC Public Health 2016, 16, 470. [Google Scholar] [CrossRef][Green Version]
- Zanobetti, A.; Luttmann-Gibson, H.; Horton, E.S. Brachial artery responses to ambient pollution, temperature, and humidity in people with type 2 diabetes: A repeated-measures study. Environ. Health Perspect. 2014, 122, 242–248. [Google Scholar] [CrossRef]
- Lindqvist, P.G.; Olsson, H.; Landin-Olsson, M. Are active sun exposure habits related to lowering risk of type 2 diabetes mellitus in women, a prospective cohort study? Diabetes Res. Clin. Pract. 2010, 90, 109–114. [Google Scholar] [CrossRef]
- Doro, P.; Grant, W.B.; Benko, R. Vitamin D and the seasonality of type 2 diabetes. Med. Hypotheses 2008, 71, 317–318. [Google Scholar] [CrossRef]
- Langer, J.; Penna-Martinez, M.; Bon, D.; Herrmann, E.; Wallasch, M.; Badenhoop, K. Insufficient Vitamin D Response to Solar Radiation in German Patients with Type 2 Diabetes or Gestational Diabetes. Horm. Metab. Res. 2016, 48, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, C.; Lu, Z.X.; Magliano, D.J.; Dunstan, D.W.; Shaw, J.E.; Zimmet, P.Z.; Sikaris, K.; Grantham, N.; Ebeling, P.R.; Daly, R.M. Serum 25-Hydroxyvitamin D, Calcium Intake, and Risk of Type 2 Diabetes After 5 Years Results from a national, population-based prospective study (the Australian Diabetes, Obesity and Lifestyle study). Diabetes Care 2011, 34, 1133–1138. [Google Scholar] [CrossRef] [PubMed]
- Si, J.; Yu, C.; Guo, Y. Season of birth and the risk of type 2 diabetes in adulthood: A prospective cohort study of 0.5 million Chinese adults. Diabetologia 2017, 60, 836–842. [Google Scholar] [CrossRef] [PubMed]
- Vaiserman, A.M.; Khalangot, M.D.; Carstensen, B. Seasonality of birth in adult type 2 diabetic patients in three Ukrainian regions. Diabetologia 2009, 52, 2665–2667. [Google Scholar] [CrossRef] [PubMed]
- Vaiserman, A.; Khalangot, M. Similar seasonality of birth in type 1 and type 2 diabetes patients: A sign for common etiology? Med. Hypotheses 2008, 71, 604–605. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.B.; Zimmermann, E.; Gamborg, M. No evidence of seasonality of birth in adult type 2 diabetes in Denmark. Diabetologia 2015, 58, 2045–2050. [Google Scholar] [CrossRef] [PubMed]
- Kostev, K.; Gläser, S.; Jacob, L. Seasonality of Insulin Use in German Outpatients with Diabetes: A Retrospective Analysis. J. Diabet. Sci. Technol. 2017, 11, 996–1000. [Google Scholar] [CrossRef]
- Scott, E.M.; Grant, P.J. Neel revisited: The adipocyte, seasonality and type 2 diabetes. Diabetologia 2006, 49, 1462–1466. [Google Scholar] [CrossRef]
- Berglund, L.; Berne, C.; Svärdsudd, K. Seasonal variations of insulin sensitivity from a euglycemic insulin clamp in elderly men. Upsala J. Med. Sci. 2012, 117, 35–40. [Google Scholar] [CrossRef]
- Holstein, A.; Wohland, T.; Patzer, O.M. Accumulation of severe hypoglycemia at weekends and in warm seasons in patients with type 1 diabetes but not with type 2 diabetes. J. Diabetes Complicat. 2016, 30, 1308–1314. [Google Scholar] [CrossRef]
- Tsujimoto, T.; Yamamoto-Honda, R.; Kajio, H. Seasonal variations of severe hypoglycemia in patients with type 1 diabetes mellitus, type 2 diabetes mellitus, and non-diabetes mellitus: Clinical analysis of 578 hypoglycemia cases. Medicine (Baltimore) 2014, 93, e148. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Jap, T.; Chen, R. A Prospective Study of Glycemic Control During Holiday Time in Type 2 Diabetic Patients. Diabetes Care 2004, 27, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.W. Seasonal Changes in Preprandial Glucose, A1C, and Blood Pressure in Diabetic Patients. Diabetes Care 2007, 30, 2501–2502. [Google Scholar] [CrossRef] [PubMed]
- Gabara, K.; Boncz, I.; Csoboth, I.; Szovak, E.; Varga, A.; De Blasio, A.; Bódi, J.; Kriszbacher, I. Variation of seasonal, weekly and daily rhythm of acute myocardial infarction in diabetic patients. Value Health 2009. [Google Scholar] [CrossRef]
- Doro, P.; Benko, R.; Matuz, M. Seasonality in the incidence of type 2 diabetes: A population-based study. Diabetes Care 2006, 29, 173. [Google Scholar] [CrossRef][Green Version]
- Fleming, D.M.; Elliot, A.J. Lessons from 40 years’ surveillance of influenza in England and Wales. Epidemiol. Infect. 2008, 136, 866–875. [Google Scholar] [CrossRef]
- Riley, P.; Cost, A.A.; Riley, S. Intra-Weekly Variations of Influenza-Like Illness in Military Populations. Mil. Med. 2016, 181, 364–368. [Google Scholar] [CrossRef][Green Version]
- Holleman, D.R.; Bowling, R.L.; Gathy, C. Predicting daily visits to a walk-in clinic and emergency department using calendar and weather data. J. Gen. Intern. Med. 1996, 11, 237–239. [Google Scholar] [CrossRef]
- Wijk, J.J.; Selow, E.R. Cluster and calendar based visualization of time series data. In Proceedings of the 1999 IEEE Symposium on Information Visualization, San Francisco, CA, USA, 24–29 October 1999; Volume 140, pp. 4–9. [Google Scholar]
- Honeyford, K.; Cecil, E.; Lo, M. The weekend effect: Does hospital mortality differ by day of the week? A systematic review and meta-analysis. BMC Health Serv. Res. 2018, 18, 870. [Google Scholar] [CrossRef]
- Mohammad, M.A.; Karlsson, S.; Haddad, J. Christmas, national holidays, sport events, and time factors as triggers of acute myocardial infarction: Swedeheart observational study 1998–2013. BMJ 2018, 363, k4811. [Google Scholar] [CrossRef]
- Buckingham-Jeffery, E.; Morbey, R.; House, T. Correcting for day of the week and public holiday effects: Improving a national daily syndromic surveillance service for detecting public health threats. BMC Public Health 2017, 17, 477. [Google Scholar] [CrossRef] [PubMed]
- Cui, S.F.; Ma, J.X.; Li, S.M. The application of time series decomposition method in predicting the incidence of shigellosis in the weekly report of chaoyang district, Beijing. China Health Stat. 2009, 6, 583–585. [Google Scholar]
- Li, X.F.; Wu, G.Z.; Gao, T.M. Methods of eliminating Spring Festival factors in the seasonal adjustment of economic indicators in China. Quant. Econ. Technol. Econ. Res. 2003, 4, 64–67. [Google Scholar]
- Deng, M. Research on the Estimation and Application of Seasonal Index; Jiangnan University: Wuxi, China, 2007. [Google Scholar]
- Liu, K.N. Problems that primary doctors should pay attention to in the treatment of type 2 diabetes. Primary Med. BBS 2006, 8, 383–384. [Google Scholar]
- Zhang, W.J. Correlation analysis of type 2 diabetes and seasonal variation in zhongtiaoshan, Shanxi Province. Chin. Med. Clin. 2012, 6, 824–826. [Google Scholar]
- Zhang, H.R. Guidelines for summer care of diabetes in community care. Pharmaco Econ. China 2014, 9, 275–276. [Google Scholar]
- Wx, Y.; Cheng, Y. “Year-end effect” of medical consumption - the effect of basic medical insurance reimbursement mechanism on medical consumption behavior of insured people. Insur. Res. 2015, 8, 16–127. [Google Scholar]
- Bao, Q.S. Research on Several Problems in Medical Insurance Data Analysis D; University of Science and Technology of China: Hefei, China, 2015. [Google Scholar]
- Chen, Y.X. Analysis of Diabetes after Holidays. In Proceedings of the first “Chinese Journal of Nursing” Paper Writing Knowledge Seminar, Kunming, China, November 2001. [Google Scholar]
- Jones, A.G.; McDonald, T.J.; Hattersley, A.T. Effect of the holiday season in patients with diabetes: Glycemia and lipids increase postholiday, but the effect is small and transient. Diabetes Care 2014, 37, e98–e99. [Google Scholar] [CrossRef][Green Version]



{kind=link}
{kind=link}
| Variables | n (%) | p-Value | |||||
|---|---|---|---|---|---|---|---|
| Spring | Summer | Autumn | Winter | Total | |||
| (n = 2,081,347) | (n = 2,208,152) | (n = 2,221,169) | (n = 1,907,246) | (n = 8,417,914) | |||
| Gender | 0.126 | ||||||
| Male | 1,097,814 | 1,144,153 | 1,141,889 | 1,012,959 | 4,396,815 | ||
| (24.97%) | (26.02%) | (25.97%) | (23.04%) | ||||
| Female | 983,533 | 1,063,999 | 1,079,280 | 894,287 | 4,021,099 | ||
| (24.46%) | (26.46%) | (26.84%) | (22.24%) | ||||
| Age (years) | 0.991 | ||||||
| ≤39 | 42,587 | 47,578 | 50,353 | 41,769 | 182,287 | ||
| (23.36%) | (26.10%) | (27.62%) | (22.91%) | ||||
| 40–49 | 184,676 | 198,453 | 204,523 | 178,179 | 765,831 | ||
| (24.11%) | (25.91%) | (26.71%) | (23.27%) | ||||
| 50–59 | 552,585 | 590,805 | 595,650 | 515,629 | 2,254,669 | ||
| (24.51%) | (26.20%) | (26.42%) | (22.87%) | ||||
| 60–69 | 773,037 | 824,329 | 829,764 | 700,552 | 3,127,682 | ||
| (24.72%) | (26.36%) | (26.53%) | (22.40%) | ||||
| 70–79 | 435,002 | 451,967 | 449,163 | 387,464 | 1,723,596 | ||
| (25.24%) | (26.22%) | (26.06%) | (22.48%) | ||||
| ≥80 | 93,460 | 95,020 | 91,716 | 83,653 | 363,849 | ||
| (25.69%) | (26.12%) | (25.21%) | (22.99%) | ||||
| Medical Insurance Types | <0.001 | ||||||
| UEBMI | 1,386,264 | 1,391,026 | 1,363,741 | 1,270,139 | 5,411,170 | ||
| (25.62%) | (25.71%) | (25.20%) | (23.47%) | ||||
| URBMI | 695,083 | 817,126 | 857,428 | 637,107 | 3,006,744 | ||
| (23.12%) | (27.18%) | (28.52%) | (21.19%) | ||||
| Season | UEBMI | URBMI | Total | Month | UEBMI | URBMI | Total |
|---|---|---|---|---|---|---|---|
| Spring | 102.60% (100.45%, 103.55%) | 102.93% (91.53%, 113.47%) | 102.67% (99.05%, 105.71%) | March | 105.36% | 87.29% | 98.98% |
| April | 109.08% | 104.18% | 107.43% | ||||
| May | 99.66% | 98.83% | 99.49% | ||||
| Summer | 96.30% (94.45%, 97.55%) | 103.65% (92.53%, 114.47%) | 99.04% (95.44%, 102.09%) | June | 99.86% | 99.10% | 99.71% |
| July | 93.31% | 100.71% | 95.24% | ||||
| August | 92.66% | 99.01% | 94.85% | ||||
| Autumn | 104.00% (102.45%, 105.55%) | 117.48% (106.03%, 127.97%) | 108.36% (104.73%, 111.38%) | September | 101.36% | 104.43% | 102.53% |
| October | 97.74% | 105.69% | 100.66% | ||||
| November | 107.28% | 114.63% | 109.95% | ||||
| Winter | 97.10% (94.95%, 98.05%) | 75.93% (65.03%, 86.97%) | 89.92% (86.34%, 93.00%) | December | 102.51% | 124.73% | 110.49% |
| January | 96.74% | 75.47% | 89.24% | ||||
| February | 94.42% | 85.93% | 91.41% | ||||
| Total | 400% | 400% | 400% | Total | 1200.00% | 1200.00% | 1200.00% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.; Li, J.; Hao, H.; Xu, L.; Nicholas, S.; Wang, J. Seasonal and Monthly Patterns, Weekly Variations, and the Holiday Effect of Outpatient Visits for Type 2 Diabetes Mellitus Patients in China. Int. J. Environ. Res. Public Health 2019, 16, 2653. https://doi.org/10.3390/ijerph16152653
Huang Y, Li J, Hao H, Xu L, Nicholas S, Wang J. Seasonal and Monthly Patterns, Weekly Variations, and the Holiday Effect of Outpatient Visits for Type 2 Diabetes Mellitus Patients in China. International Journal of Environmental Research and Public Health. 2019; 16(15):2653. https://doi.org/10.3390/ijerph16152653
Chicago/Turabian StyleHuang, Yanran, Jiajing Li, Hongying Hao, Lizheng Xu, Stephen Nicholas, and Jian Wang. 2019. "Seasonal and Monthly Patterns, Weekly Variations, and the Holiday Effect of Outpatient Visits for Type 2 Diabetes Mellitus Patients in China" International Journal of Environmental Research and Public Health 16, no. 15: 2653. https://doi.org/10.3390/ijerph16152653
APA StyleHuang, Y., Li, J., Hao, H., Xu, L., Nicholas, S., & Wang, J. (2019). Seasonal and Monthly Patterns, Weekly Variations, and the Holiday Effect of Outpatient Visits for Type 2 Diabetes Mellitus Patients in China. International Journal of Environmental Research and Public Health, 16(15), 2653. https://doi.org/10.3390/ijerph16152653