Interventions to Promote Early Discharge and Avoid Inappropriate Hospital (Re)Admission: A Systematic Review

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Design
- (1)
- What type of interventions were developed and implemented to promote early discharge, prevent and manage delayed discharge, and/or avoid inappropriate hospital (re)admission?
- (2)
- What are the components of the identified interventions?
2.2. Eligibility Criteria
2.3. Information Sources
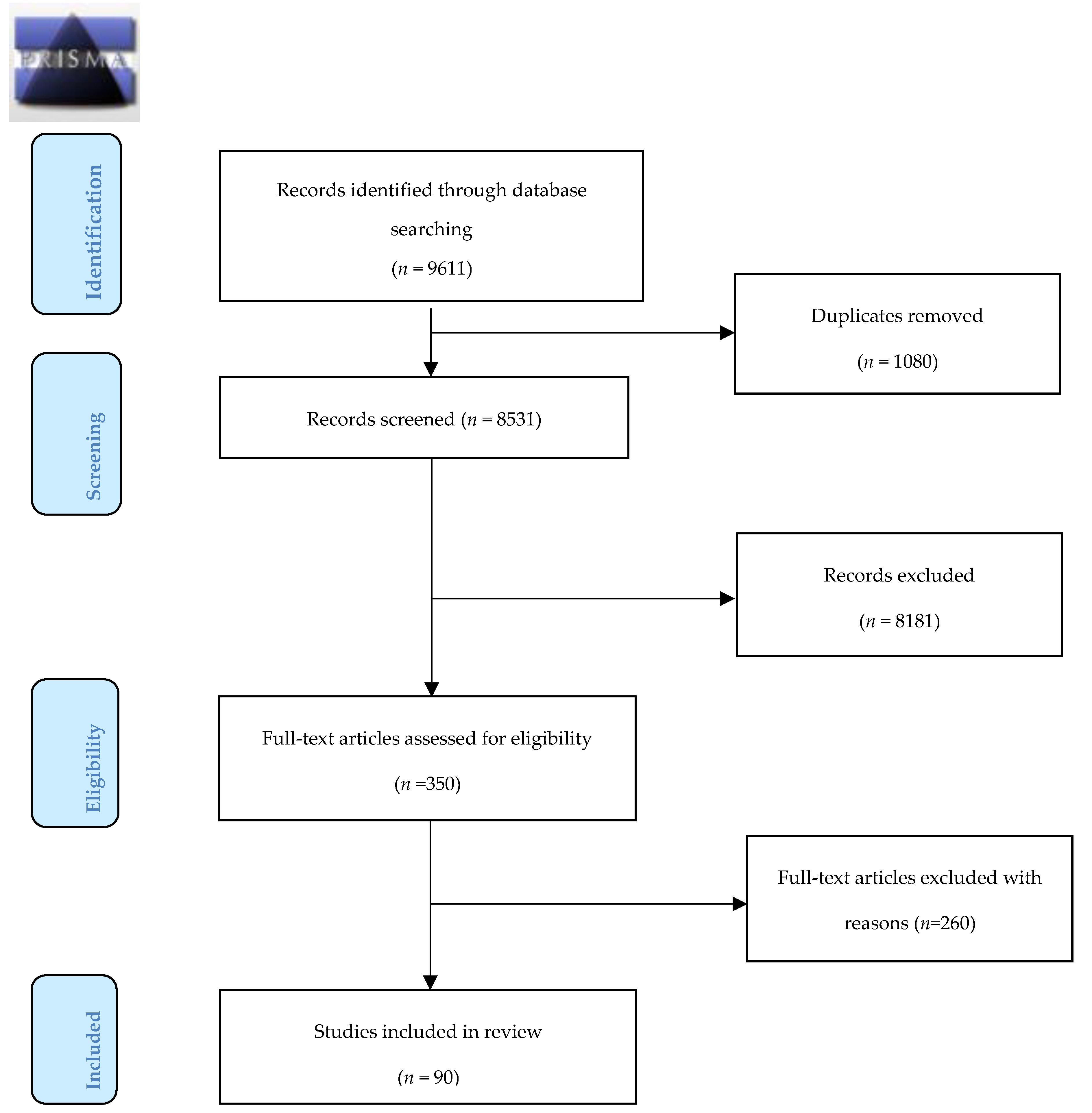
2.4. Study Selection Strategy
2.5. Data Extraction, Quality Assessment and Synthesis
3. Results
3.1. Interventions Exclusively Delivered in the Acute Hospital Pre-Discharge
3.1.1. Education
3.1.2. Multidisciplinary Clinical Management Programmes
3.1.3. Rehabilitation
3.1.4. Pharmaceutical Care
3.2. Interventions Delivered Both Pre- and Post-Discharge from Acute Care
Multidisciplinary Clinical Management
3.3. Interventions Only Delivered at Home Post-Discharge from Acute Care
Multidisciplinary Clinical Management
3.4. Interventions in Post-Acute Facility
3.4.1. Ambulatory Care
3.4.2. Transitional Care
3.4.3. Long-Term Care Interventions
3.4.4. Pharmaceutical Care
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Joint Improvement Team Scotland. Delayed Discharge. Available online: http://www.jitscotland.org.uk/action-areas/delayed-discharge/ (accessed on 14 March 2015).
- Sun, B.C.; Hsia, R.Y.; Weiss, R.E.; Zingmond, D.; Liang, L.J.; Han, W.; McCreath, H.; Asch, S.M. Effect of emergency department crowding on outcomes of admitted patients. Ann. Emerg. Med. 2013, 61, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Health Service Executive. National Rapid Discharge Guidance for Patients Who Wish to Die at Home: National Clinical Programme for Palliative Care Clinical Strategy and Programmes Directorate. Available online: https://www.hse.ie/eng/services/publications/clinical-strategy-and-programmes/national-rapid-discharge-guidance-for-patients-who-wish-to-die-at-home.pdf (accessed on 26 September 2016).
- Information Services Division Scotland Scotland. Delayed Discharges. Available online: http://www.isdscotland.org/Health-Topics/Health-and-Social-Community-Care/Delayed-Discharges/ (accessed on 26 September 2016).
- Vest, J.R.; Gamm, L.D.; Oxford, B.A.; Gonzalez, M.I.; Slawson, K.M. Determinants of preventable readmissions in the United States: A systematic review. Implement. Sci. 2010, 5, 88. [Google Scholar] [CrossRef] [PubMed]
- Bryan, K. Policies for reducing delayed discharge from hospital. Br. Med. Bull. 2010, 95, 33–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meisinger, C.; Stollenwerk, B.; Kirchberger, I.; Seidl, H.; Wende, R.; Kuch, B.; Holle, R. Effects of a nurse-based case management compared to usual care among aged patients with myocardial infarction: Results from the randomized controlled KORINNA study. BMC Geriatr. 2013, 13, 115. [Google Scholar] [CrossRef] [PubMed]
- Linertova, R.; Garcia-Perez, L.; Vazquez-Diaz, J.R.; Lorenzo-Riera, A.; Sarria-Santamera, A. Interventions to reduce hospital readmissions in the elderly: In-hospital or home care. A systematic review. J. Eval. Clin. Pract. 2011, 17, 1167–1175. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.D.; Case, L.D.; Little, W.C.; Mahler, S.A.; Burke, G.L.; Harper, E.N.; Lefebvre, C.; Hiestand, B.; Hoekstra, J.W.; Hamilton, C.A.; et al. Stress CMR reduces revascularization, hospital readmission, and recurrent cardiac testing in intermediate-risk patients with acute chest pain. JACC Cardiovasc. Imaging 2013, 6, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Kansagara, D.; Englander, H.; Salanitro, A.; Kagen, D.; Theobald, C.; Freeman, M.; Kripalani, S. Risk prediction models for hospital readmission: A systematic review. JAMA 2011, 306, 1688–1698. [Google Scholar] [CrossRef]
- Wallace, E.; Stuart, E.; Vaughan, N.; Bennett, K.; Fahey, T.; Smith, S.M. Risk prediction models to predict emergency hospital admission in community-dwelling adults: A systematic review. Med. Care 2014, 52, 751–765. [Google Scholar] [CrossRef] [PubMed]
- Weiss, M.E.; Piacentine, L.B. Psychometric properties of the Readiness for Hospital Discharge Scale. J. Nurs. Meas. 2006, 14, 163–180. [Google Scholar] [CrossRef] [PubMed]
- Weiss, M.E.; Piacentine, L.B.; Lokken, L.; Ancona, J.; Archer, J.; Gresser, S.; Holmes, S.B.; Toman, S.; Toy, A.; Vega-Stromberg, T. Perceived readiness for hospital discharge in adult medical-surgical patients. Clin. Nurse Spec. 2007, 21, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Coffey, A.; McCarthy, G.M. Older people’s perception of their readiness for discharge and postdischarge use of community support and services. Int. J. Older People Nurs. 2013, 8, 104–115. [Google Scholar] [CrossRef]
- Brent, L.; Coffey, A. Patient’s perception of their readiness for discharge following hip fracture surgery. Int. J. Orthop. Trauma Nurs. 2013, 17, 190–198. [Google Scholar] [CrossRef]
- Chapin, R.K.; Chandran, D.; Sergeant, J.F.; Koenig, T.L. Hospital to community transitions for adults: Discharge planners and community service providers’ perspectives. Soc. Work Health Care 2014, 53, 311–329. [Google Scholar] [CrossRef] [PubMed]
- Schuller, K.A.; Lin, S.H.; Gamm, L.D.; Edwardson, N. Discharge phone calls: A technique to improve patient care during the transition from hospital to home. J. Healthc. Qual. 2015, 37, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Saleh, S.S.; Freire, C.; Morris-Dickinson, G.; Shannon, T. An effectiveness and cost-benefit analysis of a hospital-based discharge transition program for elderly Medicare recipients. J. Am. Geriatr. Soc. 2012, 60, 1051–1056. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.K.; Arora, V.M.; Barach, P.R. What can artefact analysis tell us about patient transitions between the hospital and primary care? Lessons from the HANDOVER project. Eur. J. Gen. Pract. 2013, 19, 185–193. [Google Scholar] [CrossRef] [Green Version]
- Arbaje, A.I.; Wolff, J.L.; Yu, Q.; Powe, N.R.; Anderson, G.F.; Boult, C. Postdischarge environmental and socioeconomic factors and the likelihood of early hospital readmission among community-dwelling Medicare beneficiaries. Gerontologist 2008, 48, 495–504. [Google Scholar] [CrossRef]
- Dahl, U.; Steinsbekk, A.; Johnsen, R. Effectiveness of an intermediate care hospital on readmissions, mortality, activities of daily living and use of health care services among hospitalized adults aged 60 years and older—A controlled observational study. BMC Health Serv. Res. 2015, 15, 351. [Google Scholar] [CrossRef] [PubMed]
- Shepperd, S.; Lannin, N.A.; Clemson, L.M.; McCluskey, A.; Cameron, I.D.; Barras, S.L. Discharge planning from hospital to home. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Centre for Reviews and Dissemination. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Healthcare. Available online: https://www.york.ac.uk/media/crd/Systematic_Reviews.pdf (accessed on 15 September 2016).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Crowe, M. Crowe Critical Appraisal Tool (CCAT):Version 1.4. Available online: https://conchra.com.au/wp-content/uploads/2015/12/CCAT-form-v1.4.pdf (accessed on 21 August 2018).
- Crowe, M.; Sheppard, L. A review of critical appraisal tools show they lack rigor: Alternative tool structure is proposed. J. Clin. Epidemiol. 2011, 64, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Fox, M.T.; Persaud, M.; Maimets, I.; Brooks, D.; O’Brien, K.; Tregunno, D. Effectiveness of early discharge planning in acutely ill or injured hospitalized older adults: A systematic review and meta-analysis. BMC Geriatr. 2013, 13, 70. [Google Scholar] [CrossRef] [PubMed]
- Abdelaal, E.; Rao, S.V.; Gilchrist, I.C.; Bernat, I.; Shroff, A.; Caputo, R.; Costerousse, O.; Pancholy, S.B.; Bertrand, O.F. Same-day discharge compared with overnight hospitalization after uncomplicated percutaneous coronary intervention: A systematic review and meta-analysis. JACC Cardiovasc. Interv. 2013, 6, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Bradburn, M.; Goodacre, S.W.; Fitzgerald, P.; Coats, T.; Gray, A.; Hassan, T.; Humphrey, J.; Kendall, J.; Smith, J.; Collinson, P. Interhospital variation in the RATPAC trial (Randomised Assessment of Treatment using Panel Assay of Cardiac markers). Emerg. Med. J. 2012, 29, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Goldman, L.E.; Sarkar, U.; Kessell, E.; Guzman, D.; Schneidermann, M.; Pierluissi, E.; Walter, B.; Vittinghoff, E.; Critchfield, J.; Kushel, M. Support from hospital to home for elders: A randomized trial. Ann. Intern. Med. 2014, 161, 472–481. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.; Connolly, A.; Paton, F.; Corry, J. The effectiveness of protocol drive, nurse-initiated discharge in a 23-h post surgical ward: A randomized controlled trial. Int. J. Nurs. Stud. 2011, 48, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- Dawes, H.A.; Docherty, T.; Traynor, I.; Gilmore, D.H.; Jardine, A.G.; Knill-Jones, R. Specialist nurse supported discharge in gynaecology: A randomised comparison and economic evaluation. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 130, 262–270. [Google Scholar] [CrossRef]
- Wong, F.K.; Mok, M.P.; Chan, T.; Tsang, M.W. Nurse follow-up of patients with diabetes: Randomized controlled trial. J. Adv. Nurs. 2005, 50, 391–402. [Google Scholar] [CrossRef]
- Graabaek, T.; Hedegaard, U.; Christensen, M.B.; Clemmensen, M.H.; Knudsen, T.; Aagaard, L. Effect of a medicines management model on medication-related readmissions in older patients admitted to a medical acute admission unit-A randomized controlled trial. J. Eval. Clin. Pract. 2019, 25, 88–96. [Google Scholar] [CrossRef]
- Lin, R.; Gallagher, R.; Spinaze, M.; Najoumian, H.; Dennis, C.; Clifton-Bligh, R.; Tofler, G. Effect of a patient-directed discharge letter on patient understanding of their hospitalisation. Intern. Med. J. 2014, 44, 851–857. [Google Scholar] [CrossRef]
- Ogilvie, D. Hospital based alternatives to acute paediatric admission: A systematic review. Arch. Dis. Child. 2005, 90, 138. [Google Scholar] [CrossRef] [PubMed]
- Sales, V.L.; Ashraf, M.S.; Lella, L.K.; Huang, J.; Bhumireddy, G.; Lefkowitz, L.; Feinstein, M.; Kamal, M.; Caesar, R.; Cusick, E.; et al. Utilization of trained volunteers decreases 30-day readmissions for heart failure. J. Card. Fail. 2014, 20, e315–e323. [Google Scholar] [CrossRef] [PubMed]
- Jennings, J.H.; Thavarajah, K.; Mendez, M.P.; Eichenhorn, M.; Kvale, P.; Yessayan, L. Predischarge bundle for patients with acute exacerbations of COPD to reduce readmissions and ED visits: A randomized controlled trial. Chest 2015, 147, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Bonnet-Zamponi, D.; d’Arailh, L.; Konrat, C.; Delpierre, S.; Lieberherr, D.; Lemaire, A.; Tubach, F.; Lacaille, S.; Legrain, S. Drug-related readmissions to medical units of older adults discharged from acute geriatric units: Results of the Optimization of Medication in AGEd multicenter randomized controlled trial. J. Am. Geriatr. Soc. 2013, 61, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Davidson, P.M.; Cockburn, J.; Newton, P.J.; Webster, J.K.; Betihavas, V.; Howes, L.; Owensby, D.O. Can a heart failure-specific cardiac rehabilitation program decrease hospitalizations and improve outcomes in high-risk patients? Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Greening, N.J.; Williams, J.E.; Hussain, S.F.; Harvey-Dunstan, T.C.; Bankart, M.J.; Chaplin, E.J.; Vincent, E.E.; Chimera, R.; Morgan, M.D.; Singh, S.J.; et al. An early rehabilitation intervention to enhance recovery during hospital admission for an exacerbation of chronic respiratory disease: Randomised controlled trial. BMJ 2014, 349, g4315. [Google Scholar] [CrossRef] [PubMed]
- Jesudason, C.; Stiller, K.; McInnes, M.; Sullivan, T. A physiotherapy service to an emergency extended care unit does not decrease admission rates to hospital: A randomised trial. Emerg. Med. J. 2012, 29, 664–669. [Google Scholar] [CrossRef]
- Sahota, O.; Pulikottil-Jacob, R.; Marshall, F.; Montgomery, A.; Tan, W.; Sach, T.; Logan, P.; Kendrick, D.; Watson, A.; Walker, M.; et al. The Community In-reach Rehabilitation and Care Transition (CIRACT) clinical and cost-effectiveness randomisation controlled trial in older people admitted to hospital as an acute medical emergency. Age Ageing 2017, 46, 26–32. [Google Scholar] [CrossRef]
- Wu, J.; Faux, S.G.; Estell, J.; Wilson, S.; Harris, I.; Poulos, C.J.; Klein, L. Early rehabilitation after hospital admission for road trauma using an in-reach multidisciplinary team: A randomised controlled trial. Clin. Rehabil. 2017, 31, 1189–1200. [Google Scholar] [CrossRef]
- de Souza, G.S.; Vidigal, F.M.; Chebli, L.A.; da Rocha Ribeiro, T.C.; Furtado, M.C.; de Lima Pace, F.H.; de Miranda Chaves, L.D.; de Oliveira Zanini, K.A.; Gaburri, P.D.; de Azevedo Lucca, F.; et al. Effect of azathioprine or mesalazine therapy on incidence of re-hospitalization in sub-occlusive ileocecal Crohn’s disease patients. Med. Sci. Monit. 2013, 19, 716–722. [Google Scholar] [CrossRef]
- Challand, C.; Struthers, R.; Sneyd, J.R.; Erasmus, P.D.; Mellor, N.; Hosie, K.B.; Minto, G. Randomized controlled trial of intraoperative goal-directed fluid therapy in aerobically fit and unfit patients having major colorectal surgery. Br. J. Anaesth. 2012, 108, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, A.C.; Atallah, A.N.; Matos, D.; da Silva, E.M. Intravenous versus inhalational anaesthesia for paediatric outpatient surgery. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef] [PubMed]
- Shcherbakova, N.; Tereso, G. Clinical pharmacist home visits and 30-day readmissions in Medicare Advantage beneficiaries. J. Eval. Clin. Pract. 2016, 22, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Dizon, M.L.; Reinking, C. Reducing Readmissions: Nurse-Driven Interventions in the Transition of Care From the Hospital. Worldviews Evid. Based Nurs. 2017, 14, 432–439. [Google Scholar] [CrossRef]
- Alshabanat, A.; Otterstatter, M.C.; Sin, D.D.; Road, J.; Rempel, C.; Burns, J.; van Eeden, S.F.; FitzGerald, J.M. Impact of a COPD comprehensive case management program on hospital length of stay and readmission rates. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 961–971. [Google Scholar] [CrossRef] [PubMed]
- Schuller, K.A.; Kash, B.A.; Gamm, L.D. Enhanced Transitions of Care: Centralizing Discharge Phone Calls Improves Ability to Reach Patients and Reduces Hospital Readmissions. J. Healthc. Qual. 2017, 39, e10–e21. [Google Scholar] [CrossRef]
- Prvu Bettger, J.; Alexander, K.P.; Dolor, R.J.; Olson, D.M.; Kendrick, A.S.; Wing, L.; Coeytaux, R.R.; Graffagnino, C.; Duncan, P.W. Transitional care after hospitalization for acute stroke or myocardial infarction: A systematic review. Ann. Intern. Med. 2012, 157, 407–416. [Google Scholar] [CrossRef]
- Lopes, S.; Fernandes, O.B.; Marques, A.P.; Moita, B.; Sarmento, J.; Santana, R. Can Vertical Integration Reduce Hospital Readmissions? A Difference-in-Differences Approach. Med. Care 2017, 55, 506–513. [Google Scholar] [CrossRef] [Green Version]
- Martinez, A.; Everss, E.; Rojo-Alvarez, J.L.; Figal, D.P.; Garcia-Alberola, A. A systematic review of the literature on home monitoring for patients with heart failure. J. Telemed. Telecare 2006, 12, 234–241. [Google Scholar] [CrossRef]
- Li, J.; Wang, H.; Xie, H.; Mei, G.; Cai, W.; Ye, J.; Zhang, J.; Ye, G.; Zhai, H. Effects of post-discharge nurse-led telephone supportive care for patients with chronic kidney disease undergoing peritoneal dialysis in China: A randomized controlled trial. Perit. Dial. Int. 2014, 34, 278–288. [Google Scholar] [CrossRef]
- Thomas, R.; Huntley, A.L.; Mann, M.; Huws, D.; Elwyn, G.; Paranjothy, S.; Purdy, S. Pharmacist-led interventions to reduce unplanned admissions for older people: A systematic review and meta-analysis of randomised controlled trials. Age Ageing 2014, 43, 174–187. [Google Scholar] [CrossRef] [PubMed]
- Rousseaux, M.; Daveluy, W.; Kozlowski, R. Value and efficacy of early supported discharge from stroke units. Ann. Phys. Rehabil. Med. 2009, 52, 224–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huntley, A.L.; Thomas, R.; Mann, M.; Huws, D.; Elwyn, G.; Paranjothy, S.; Purdy, S. Is case management effective in reducing the risk of unplanned hospital admissions for older people? A systematic review and meta-analysis. Fam. Pract. 2013, 30, 266–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rice, K.L.; Dewan, N.; Bloomfield, H.E.; Grill, J.; Schult, T.M.; Nelson, D.B.; Kumari, S.; Thomas, M.; Geist, L.J.; Beaner, C.; et al. Disease management program for chronic obstructive pulmonary disease: A randomized controlled trial. Am. J. Respir. Crit. Care Med. 2010, 182, 890–896. [Google Scholar] [CrossRef] [PubMed]
- Ontario Health Technical Advisory Committee Ontario. Specialized community-based care: An evidence-based analysis. Ont. Health Technol. Assess. Ser. 2012, 12, 1–60. [Google Scholar]
- Ryan, S.; O’Riordan, J.M.; Tierney, S.; Conlon, K.C.; Ridgway, P.F. Impact of a new electronic handover system in surgery. Int. J. Surg. 2011, 9, 217–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stall, N.; Nowaczynski, M.; Sinha, S.K. Systematic review of outcomes from home-based primary care programs for homebound older adults. J. Am. Geriatr. Soc. 2014, 62, 2243–2251. [Google Scholar] [CrossRef]
- Holland, R.; Lenaghan, E.; Harvey, I.; Smith, R.; Shepstone, L.; Lipp, A.; Christou, M.; Evans, D.; Hand, C. Does home based medication review keep older people out of hospital? The HOMER randomised controlled trial. BMJ 2005, 330, 293. [Google Scholar] [CrossRef]
- Lainscak, M.; Kadivec, S.; Kosnik, M.; Benedik, B.; Bratkovic, M.; Jakhel, T.; Marcun, R.; Miklosa, P.; Stalc, B.; Farkas, J. Discharge coordinator intervention prevents hospitalizations in patients with COPD: A randomized controlled trial. J. Am. Med. Dir. Assoc. 2013, 14, 450. [Google Scholar] [CrossRef]
- Delgado-Passler, P.; McCaffrey, R. The influences of postdischarge management by nurse practitioners on hospital readmission for heart failure. J. Am. Acad. Nurse Pract. 2006, 18, 154–160. [Google Scholar] [CrossRef]
- Chow, S.K.; Wong, F.K.; Chan, T.M.; Chung, L.Y.; Chang, K.K.; Lee, R.P. Community nursing services for postdischarge chronically ill patients. J. Clin. Nurs. 2008, 17, 260–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crocker, J.B.; Crocker, J.T.; Greenwald, J.L. Telephone follow-up as a primary care intervention for postdischarge outcomes improvement: A systematic review. Am. J. Med. 2012, 125, 915–921. [Google Scholar] [CrossRef] [PubMed]
- Carroll, A.; Dowling, M. Discharge planning: Communication, education and patient participation. Br. J. Nurs. 2007, 16, 882–886. [Google Scholar] [CrossRef]
- Jeppesen, E.; Brurberg, K.G.; Vist, G.E.; Wedzicha, J.A.; Wright, J.J.; Greenstone, M.; Walters, J.A. Hospital at home for acute exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef] [PubMed]
- Utens, C.M.; Goossens, L.M.; Smeenk, F.W.; Rutten-van Molken, M.P.; van Vliet, M.; Braken, M.W.; van Eijsden, L.M.; van Schayck, O.C. Early assisted discharge with generic community nursing for chronic obstructive pulmonary disease exacerbations: Results of a randomised controlled trial. BMJ Open 2012, 2. [Google Scholar] [CrossRef] [PubMed]
- Parab, C.S.; Cooper, C.; Woolfenden, S.; Piper, S.M. Specialist home-based nursing services for children with acute and chronic illnesses. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, M.; Bowles, K.H.; Feldman, P.H.; St Pierre, M.; Jarrin, O.; Shah, S.; Murtaugh, C.M. Frontloading and intensity of skilled home health visits: A state of the science. Home Health Care Serv. Q. 2014, 33, 159–175. [Google Scholar] [CrossRef] [PubMed]
- Levine, S.; Steinman, B.A.; Attaway, K.; Jung, T.; Enguidanos, S. Home care program for patients at high risk of hospitalization. Am. J. Manag. Care 2012, 18, e269–e276. [Google Scholar]
- Aguado, O.; Morcillo, C.; Delas, J.; Rennie, M.; Bechich, S.; Schembari, A.; Fernandez, F.; Rosell, F. Long-term implications of a single home-based educational intervention in patients with heart failure. Heart Lung J. Crit. Care 2010, 39, S14–S22. [Google Scholar] [CrossRef] [PubMed]
- Bouman, A.; van Rossum, E.; Evers, S.; Ambergen, T.; Kempen, G.; Knipschild, P. Effects on health care use and associated cost of a home visiting program for older people with poor health status: A randomized clinical trial in the Netherlands. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 291–297. [Google Scholar] [CrossRef]
- Latour, C.H.; de Vos, R.; Huyse, F.J.; de Jonge, P.; van Gemert, L.A.; Stalman, W.A. Effectiveness of post-discharge case management in general-medical outpatients: A randomized, controlled trial. Psychosomatics 2006, 47, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Dhalla, I.A.; O’Brien, T.; Morra, D.; Thorpe, K.E.; Wong, B.M.; Mehta, R.; Frost, D.W.; Abrams, H.; Ko, F.; Van Rooyen, P.; et al. Effect of a postdischarge virtual ward on readmission or death for high-risk patients: A randomized clinical trial. Jama 2014, 312, 1305–1312. [Google Scholar] [CrossRef] [PubMed]
- Conroy, S.P.; Stevens, T.; Parker, S.G.; Gladman, J.R. A systematic review of comprehensive geriatric assessment to improve outcomes for frail older people being rapidly discharged from acute hospital: ‘interface geriatrics’. Age Ageing 2011, 40, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Adib-Hajbaghery, M.; Maghaminejad, F.; Abbasi, A. The role of continuous care in reducing readmission for patients with heart failure. J. Caring Sci. 2013, 2, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Bahr, S.J.; Solverson, S.; Schlidt, A.; Hack, D.; Smith, J.L.; Ryan, P. Integrated literature review of postdischarge telephone calls. West. J. Nurs. Res. 2014, 36, 84–104. [Google Scholar] [CrossRef] [PubMed]
- Gould, K.A. A randomized controlled trial of a discharge nursing intervention to promote self-regulation of care for early discharge interventional cardiology patients. Dimens. Crit. Care Nurs. 2011, 30, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Gellis, Z.D.; Kenaley, B.L.; Ten Have, T. Integrated telehealth care for chronic illness and depression in geriatric home care patients: The Integrated Telehealth Education and Activation of Mood (I-TEAM) study. J. Am. Geriatr. Soc. 2014, 62, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Steventon, A.; Bardsley, M.; Billings, J.; Dixon, J.; Doll, H.; Beynon, M.; Hirani, S.; Cartwright, M.; Rixon, L.; Knapp, M.; et al. Effect of telecare on use of health and social care services: Findings from the Whole Systems Demonstrator cluster randomised trial. Age Ageing 2013, 42, 501–508. [Google Scholar] [CrossRef]
- Blum, K.; Gottlieb, S.S. The effect of a randomized trial of home telemonitoring on medical costs, 30-day readmissions, mortality, and health-related quality of life in a cohort of community-dwelling heart failure patients. J. Card. Fail. 2014, 20, 513–521. [Google Scholar] [CrossRef]
- Gurwitz, J.H.; Field, T.S.; Ogarek, J.; Tjia, J.; Cutrona, S.L.; Harrold, L.R.; Gagne, S.J.; Preusse, P.; Donovan, J.L.; Kanaan, A.O.; et al. An electronic health record-based intervention to increase follow-up office visits and decrease rehospitalization in older adults. J. Am. Geriatr. Soc. 2014, 62, 865–871. [Google Scholar] [CrossRef]
- Motamedi, S.M.; Posadas-Calleja, J.; Straus, S.; Bates, D.W.; Lorenzetti, D.L.; Baylis, B.; Gilmour, J.; Kimpton, S.; Ghali, W.A. The efficacy of computer-enabled discharge communication interventions: A systematic review. BMJ Qual. Saf. 2011, 20, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Doran, K.M.; Ragins, K.T.; Gross, C.P.; Zerger, S. Medical respite programs for homeless patients: A systematic review. J. Health Care Poor Underserved 2013, 24, 499–524. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.N.; Pearce, S.E. Acute care for the elderly: A literature review. Popul. Health Manag. 2010, 13, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Scott, I.; Vaughan, L.; Bell, D. Effectiveness of acute medical units in hospitals: A systematic review. Int. J. Qual. Health Care 2009, 21, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Crotty, M.; Giles, L.C.; Halbert, J.; Harding, J.; Miller, M. Home versus day rehabilitation: A randomised controlled trial. Age Ageing 2008, 37, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Fox, M.T.; Persaud, M.; Maimets, I.; O’Brien, K.; Brooks, D.; Tregunno, D.; Schraa, E. Effectiveness of acute geriatric unit care using acute care for elders components: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2012, 60, 2237–2245. [Google Scholar] [CrossRef] [PubMed]
- Connolly, M.J.; Boyd, M.; Broad, J.B.; Kerse, N.; Lumley, T.; Whitehead, N.; Foster, S. The Aged Residential Care Healthcare Utilization Study (ARCHUS): A multidisciplinary, cluster randomized controlled trial designed to reduce acute avoidable hospitalizations from long-term care facilities. J. Am. Med Dir. Assoc. 2015, 16, 49–55. [Google Scholar] [CrossRef]
- Guerin, M.; Grimmer, K.; Kumar, S. Community services’ involvement in the discharge of older adults from hospital into the community. Int. J. Integr. Care 2013, 13, e032. [Google Scholar] [CrossRef]
- Malik, M.; Moore, Z.; Patton, D.; O’Connor, T.; Nugent, L.E. The impact of geriatric focused nurse assessment and intervention in the emergency department: A systematic review. Int. Emerg. Nurs. 2018, 37, 52–60. [Google Scholar] [CrossRef]
- Edmans, J.; Bradshaw, L.; Franklin, M.; Gladman, J.; Conroy, S. Specialist geriatric medical assessment for patients discharged from hospital acute assessment units: Randomised controlled trial. BMJ 2013, 347, f5874. [Google Scholar] [CrossRef]
- Prieto-Centurion, V.; Markos, M.A.; Ramey, N.I.; Gussin, H.A.; Nyenhuis, S.M.; Joo, M.J.; Prasad, B.; Bracken, N.; Didomenico, R.; Godwin, P.O.; et al. Interventions to reduce rehospitalizations after chronic obstructive pulmonary disease exacerbations. A systematic review. Ann. Am. Thorac. Soc. 2014, 11, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Naylor, M.D.; Aiken, L.H.; Kurtzman, E.T.; Olds, D.M.; Hirschman, K.B. The care span: The importance of transitional care in achieving health reform. Health Aff. 2011, 30, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.; Hutchinson, A.M.; Brown, R.; Livingston, P.M. Quality care outcomes following transitional care interventions for older people from hospital to home: A systematic review. BMC Health Serv. Res. 2014, 14, 346. [Google Scholar] [CrossRef] [PubMed]
- Wong, F.K.; Chow, S.K.; Chan, T.M.; Tam, S.K. Comparison of effects between home visits with telephone calls and telephone calls only for transitional discharge support: A randomised controlled trial. Age Ageing 2014, 43, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Verhaegh, K.J.; MacNeil-Vroomen, J.L.; Eslami, S.; Geerlings, S.E.; de Rooij, S.E.; Buurman, B.M. Transitional care interventions prevent hospital readmissions for adults with chronic illnesses. Health Aff. 2014, 33, 1531–1539. [Google Scholar] [CrossRef]
- Rennke, S.; Nguyen, O.K.; Shoeb, M.H.; Magan, Y.; Wachter, R.M.; Ranji, S.R. Hospital-initiated transitional care interventions as a patient safety strategy: A systematic review. Ann. Intern. Med. 2013, 158, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Feltner, C.; Jones, C.D.; Cene, C.W.; Zheng, Z.J.; Sueta, C.A.; Coker-Schwimmer, E.J.; Arvanitis, M.; Lohr, K.N.; Middleton, J.C.; Jonas, D.E. Transitional care interventions to prevent readmissions for persons with heart failure: A systematic review and meta-analysis. Ann. Intern. Med. 2014, 160, 774–784. [Google Scholar] [CrossRef]
- Reilly, S.; Miranda-Castillo, C.; Malouf, R.; Hoe, J.; Toot, S.; Challis, D.; Orrell, M. Case management approaches to home support for people with dementia. Cochrane Database Syst. Rev. 2015, 1, Cd008345. [Google Scholar] [CrossRef]
- Englander, H.; Michaels, L.; Chan, B.; Kansagara, D. The care transitions innovation (C-TraIn) for socioeconomically disadvantaged adults: Results of a cluster randomized controlled trial. J. Gen. Intern. Med. 2014, 29, 1460–1467. [Google Scholar] [CrossRef]
- Lehnbom, E.C.; Stewart, M.J.; Manias, E.; Westbrook, J.I. Impact of medication reconciliation and review on clinical outcomes. Ann. Pharmacother. 2014, 48, 1298–1312. [Google Scholar] [CrossRef]
- Herfjord, J.K.; Heggestad, T.; Ersland, H.; Ranhoff, A.H. Intermediate care in nursing home after hospital admission: A randomized controlled trial with one year follow-up. BMC Res. Notes 2014, 7, 889. [Google Scholar] [CrossRef] [PubMed]
- Tabanejad, Z.; Pazokian, M.; Ebadi, A. A Systematic Review of the Liaison Nurse Role on Patient’s Outcomes after Intensive Care Unit Discharge. Int. J. Community Based Nurs. Midwifery 2014, 2, 202–210. [Google Scholar] [PubMed]
- Boyd, M.; Armstrong, D.; Parker, J.; Pilcher, C.; Zhou, L.; McKenzie-Green, B.; Connolly, M.J. Do gerontology nurse specialists make a difference in hospitalization of long-term care residents? Results of a randomized comparison trial. J. Am. Geriatr. Soc. 2014, 62, 1962–1967. [Google Scholar] [CrossRef] [PubMed]
- Harvey, P.; Storer, M.; Berlowitz, D.J.; Jackson, B.; Hutchinson, A.; Lim, W.K. Feasibility and impact of a post-discharge geriatric evaluation and management service for patients from residential care: The Residential Care Intervention Program in the Elderly (RECIPE). BMC Geriatr. 2014, 14, 48. [Google Scholar] [CrossRef] [PubMed]
- Farris, K.B.; Carter, B.L.; Xu, Y.; Dawson, J.D.; Shelsky, C.; Weetman, D.B.; Kaboli, P.J.; James, P.A.; Christensen, A.J.; Brooks, J.M. Effect of a care transition intervention by pharmacists: An RCT. BMC Health Serv. Res. 2014, 14, 406. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Type of Study | Interventions Exclusively Delivered in the Acute Hospital Pre-Discharge | Interventions Delivered Pre- and Post-Discharge from Acute Care | Interventions only Delivered at Home (Post-Discharge from Acute Care) | Interventions only Delivered in a Post-Acute Facility |
|---|---|---|---|---|
| MR | 1 | |||
| MA | ||||
| SR & MA | 1 | 2 | 4 | |
| SR | 1 | 9 | 7 | 14 |
| RCT | 18 | 7 | 9 | 10 |
| Non-randomised trial | 2 | |||
| Pre–post-intervention study | 1 | |||
| Retrospective cohort | 2 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coffey, A.; Leahy-Warren, P.; Savage, E.; Hegarty, J.; Cornally, N.; Day, M.R.; Sahm, L.; O’Connor, K.; O’Doherty, J.; Liew, A.; et al. Interventions to Promote Early Discharge and Avoid Inappropriate Hospital (Re)Admission: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 2457. https://doi.org/10.3390/ijerph16142457
Coffey A, Leahy-Warren P, Savage E, Hegarty J, Cornally N, Day MR, Sahm L, O’Connor K, O’Doherty J, Liew A, et al. Interventions to Promote Early Discharge and Avoid Inappropriate Hospital (Re)Admission: A Systematic Review. International Journal of Environmental Research and Public Health. 2019; 16(14):2457. https://doi.org/10.3390/ijerph16142457
Chicago/Turabian StyleCoffey, Alice, Patricia Leahy-Warren, Eileen Savage, Josephine Hegarty, Nicola Cornally, Mary Rose Day, Laura Sahm, Kieran O’Connor, Jane O’Doherty, Aaron Liew, and et al. 2019. "Interventions to Promote Early Discharge and Avoid Inappropriate Hospital (Re)Admission: A Systematic Review" International Journal of Environmental Research and Public Health 16, no. 14: 2457. https://doi.org/10.3390/ijerph16142457